big pharma next generation go-to-market
TRANSCRIPT

Big Pharma
Next generation Go-to-Market

2
The Urgency for Immediate Action
In September 2021, a call for emergency action to limit global temperature increases, restore biodiversity, and protect health was published simultaneously by 227 high-impact journals (1). The statement underlined the need for society-wide changes to create a fairer and healthier world and called for all stakeholders to proactively contribute to the global prevention of further damage and the proactive action on the root causes of the crisis we face.
At the same time, Worldwide drug sales (prescription + generics + orphans) are forecast to grow 56,2% from $901bn in 2020 to $1407bn in 2026 (2), which outlines a fundamental predicament: Will the world be able to afford pharmaceuticals? And if so, what will the world require from pharmaceutical companies to justify that level of growth? The industry has the potential to take pivotal leadership in the world. The COVID-19 pandemic showcased effective vaccine development at breakneck speed, put into the world based on a not-for-profit model (3). During a 2021 conference hosted by the
American Society of Clinical Oncology, an expert panel discussed the industry’s near-future ability to develop a cure for cancer (4). On the other hand, the industry will do everything in its power to stay commercially viable and competitive for the long term, delivering robust trajectories of double-digit growth to shareholders.
So, what is the sustainable balance? The pace and urgency of modern life are undoubtedly speeding up, accelerating the accountability of pharmaceutical companies to reshape their relationship with the world. Leading CEOs point out that now is the time to shift the focus in healthcare away from just effectiveness and cost to sustainability, resiliency, and value. Now is the time for the industry to facilitate a new go-to-market (GTM) model based on deep engagement with broad coalitions of stakeholders that can supercharge efforts to combat all urgent public health challenges and revitalize disease ecosystems (5).

3
COVID-19 Aftershocks
We can’t make a change if we cannot see that one is needed. Inspiration and reorientation are at the beginning of any process of change. It relies entirely on our ability to keep a fresh perspective. We must, therefore, proactively make sure that we expose our systemic mindset to a diversity of thought. We must set up advanced monitoring systems to detect all significant developments. We must be observant of the unmet needs of our surroundings to remain relevant in the world. A future-proof GTM model will rely entirely upon our ability to understand how the landscape of health is transforming and how we can apply positive impact through action.
The pandemic outbreak was a transformational shock - an unpredictable event carrying a massive impact within weeks. Societies all over the world shut down simultaneously. By September 2021, the coronavirus cased 224 million identified cases and 4,6 million deaths (6). 2020 resulted in a staggering 4,3% reduction in GDP, a 9,0% GDP increase of global debt levels (7) and a total work-loss equivalent to 255 million full-time workers (8).
Long before COVID-19, there was clear evidence of transformational slides in the form of predictable events that will carry equally massive impact over a more extended period. The scientific reinterpretation of systems biology challenging the siloed logic of healthcare systems. The rise of consumer health accelerating the decentralization of health and putting much more emphasis on preventive lifestyles. The entry of big tech into the healthcare space introducing business models competing outside existing reimbursement schemes. The three listed slides mentioned illustrates a fraction of the moving parts that make up a health landscape undergoing fundamental change.
Before outlining a new GTM model, it is paramount to detect how the shock of the pandemic will create significant aftershocks by impacting the slides that were already ongoing. And how these aftershocks will affect the GTM model over time.
Non-communicable diseases (NCDs), notably cardiovascular diseases, cancers, diabetes, and chronic respiratory diseases, are the leading global causes of death and disability. NCDs often require repeat interactions with the healthcare system over long periods. The aftershock of the pandemic has dramatically reduced the systemic capacity to deliver NCD care. The unmet need for NCD care will lead to health and economic consequences at global, country, household and individual levels, resulting in severe disability, premature deaths, and billions of dollars in financial loss each year (9). COVID-19 has, on the other hand, made it evident that many of the tools required for fighting a pandemic are also those needed to fight NCDs (10):
• Disease surveillance• A strong civil society• Robust public health• Clear communication• Equitable access to resilient
universal healthcare systems
Therein lies the mapping of a new normal based on our ability to forecast the complex problems we will face together and identify the future solutions that can produce sustainable commercial growth. Let’s take a closer look at two major COVID-19 aftershocks that have the potential to make or break the pharmaceutical GTM model.
The Systemic Erosion of Healthcare Budgets
Angel Gurría, former Secretary-General of OECD, said, “Public health and the global economy are inextricably linked. We cannot have one without the other. Healthy global economic systems depend on healthy citizens. Strengthening the preparedness and resilience of health systems will require additional resources.” (11). The quote illustrates the trajectory that the world will run out of money to pay for the current level of healthcare and that societies must implement healthcare reform to be better prepared for future pandemics and improve the overall outcome-cost ratio of healthcare provision.
The combined effect of intensified demographic squeeze (12), growing health inequalities (13), increased prevalence of NCDs and comorbidities (14)(15)(16), and an insurmountable post-pandemic healthcare backlog (17)(18) will create an unprecedented downward spiral that will accelerate the systemic socio-economic erosion of healthcare budgets.

4
C19 AFTERSHOCKIncreased
GTMComplexity
Pharma competitivenessIncreased average price point in the market
Healthcare reformDecreased average price point in the market
C19 SHOCK
More people will live for more extended periods with multiple chronic conditions due to behavioral, physiological, environmental and genetic factors. The more severe disease state will result in social isolation, loss of jobs, income inequality, poor nutrition and lack of exercise. The added disease burden will overwhelm a healthcare system already swamped by the backlog of the pandemic. Even the most advanced preventive, diagnostic and treatment schemes can render meaningless in this scenario. Consequently, cost restraint measures will be implemented across the board, putting extreme pressure on society’s ability to spend money on pharmaceuticals.
Low-Volume High-Margin Products
Ten years ago, Severin Schwan, CEO of Roche, forecasted how the pharmaceutical industry would evolve over the next decade:
“I think what we will see over time is a segmentation of the market. We will see companies that will focus on OTC and generics - products where patents have expired (high volume, low margin
products). And then, you will have a segment of companies committed to innovation, dedicated to solutions that make a real difference to patients (low volume, high margin). Now, what will disappear is the part in the middle.” (19).
The quote illustrates that most tier 1 pharma companies have focused their portfolio on the discovery, development, manufacturing and commercialization of highly innovative products targeting a smaller population of patients, achieving higher price points in the market.
Multiple examples showcase how drug companies charge exorbitant amounts for new treatments that are often not better than older, cheaper options. Nowhere is this more the case than within oncology; it remains the largest therapy area in 2026 ($319 bn), accounting for 16,3% of worldwide drug sales (prescription + generics + orphans) that year (2). In comparison, only 9,9% of the global disease burden in 2019 measured by disability-adjusted life years (DALY) was due to cancer (14), suggesting a “premium” reflecting that cancer drug pricing does not correlate with value or clinical benefit.
Cancer has absorbed the lion’s share of R&D money for years and continues to do so (2). The new generation of treatment promises to transform the field of cancer, yielding more cures and long-term remissions than ever before. But as medicine’s ability to tackle tumors races ahead, healthcare systems worldwide struggle to accommodate the high price point (20). In recent years, financial toxicity has emerged as an essential patient-reported outcome.
Studies have demonstrated that financial toxicity - due to the high price of cancer treatments - in patients with cancer is prevalent and is seen across cancer types, countries, and health care systems (21).The aggressive low-volume high-margin competitive strategy of pharma companies is exhausting and stressing society’s willingness to spend money on innovative medicines.

5
Increased GTM Complexity
How will the pattern evolve? Societies caught in an unprecedented socio-economic downward spiral putting extreme pressure on pharmaceutical spending and tier 1 pharmaceuticals focusing on low-volume high-margin products to stay competitive by achieving a premium price point in the market? We are indeed heading for a near-future scenario where the self-interest of stakeholders grows further and further apart, potentially undermining the joint efforts to revitalize disease ecosystems and where the GTM complexity will dramatically increase.
In the US, the world’s leading pharmaceutical market, the industry and its trade associations have, during the first three months of 2021, spent more than $45 mil on lobbying, arguing in part that restrictions on the high prices charged for existing drugs would blunt incentives for future innovation (22). Several initiatives across the world are addressing the misaligned incentives within healthcare systems. If this subsequently leads to radical shifts implemented as direct price controls or a series of alternative pressures to temper unsustainable and unjustified pricing remains to be seen (2).We conducted a horizon scanning of ongoing GTM complexity trends across
Europe 2019-2021 (23) to identify a comprehensive list of initiatives to improve the pharmaceutical spending outcome/cost ratio.
Regulatory approval• Accelerated time to market for
medicine within prioritized areas• Biosimilar developers can skip
comparative efficacy trials leading to cheaper drug and faster approvals
• Demand for additional real-world evidence (RWE) post-launch
• Request for more substantial differentiation in efficacy and safety on new innovative medicines
Procurement & assessment• Adoption of health economics
and budget impact analysis• Demand to model shared
financial risk-taking• Economies of scale through
more centralized purchasing• Growth of non-retail distribution• Increased parallel trading
of medicine between EU member states
• Increased pricing transparency/ reference pricing
• Introduction of price “roof” based on QALY-type calculations
• Joint procurement and health technology assessment (HTA) process across nations
• More mature and complex procurement and HTA process
• National saving targets for pharmaceutical spending
Listings• Acceptance of lower level of
demonstrated outcomes to make more cost-efficient prioritizations
• Pharmacy-level regulations on exchanging biologics with biosimilar/generics
• Prioritization of generics and biosimilars in guideline listings
• Transfer of high-cost medicine to hospital dispensing (to better execute guidelines)
Reimbursement & fines• Both EMA/FDA and national
reimbursement bodies are restricting new indications due to a lack of convincing data
• Early access through conditional reimbursement
• Penalties for excessive and unfair pricing/price hikes
• Introduction of SMART spending • Stricter reimbursement guidelines • Pay-for-performance arrangements
which reimburse for pre-specified outcomes (value-based contracting)
• Reimbursement for digital therapeutics• Simplified reimbursement procedures
for biosimilar drugs
The GTM Discipline
GTM is associated with sales reps out in the field equipped with marketing materials trying to get a foot in the door, promoting the story of great products and science. The day-to-day front-end engagement with healthcare professionals aims to increase share of voice in relation to key competitors. In parallel, other disciplines such as market access and regulatory affairs have continuous back-end engagement with public authorities to obtain the best possible market conditions by negotiating the local requirements that pharma must adhere to. Historically the two engagement disciplines have been primarily powered by analogue activities and poorly aligned in their execution, focusing on engagement with different stakeholders for a different set of purposes. So how much and how fast will increased complexity in the market impact the efficiency of best practice GTM? Return on investment (ROI) is likely to diminish over time, demanding a much higher level of both front-end and back-end engagement activities to uphold the status quo. Return of experience (ROE) is probably going to suffer more, eroding the perception of the pharma industry as a trusted leader that can facilitate necessary change.

6
Over the last couple of years, we have conducted several download sessions with Health Care Professionals (HCPs) focusing on their role and relationship with pharma (24). We can’t disclose specific findings here (they belong to the IP of our clients) but we can highlight some high-level reoccurring trends:
Potentials:• Respondents agree that COVID-19
has changed their overall perspective of their role as HCPs
• Respondents regard continuous learning as the no. 1 priority
• Respondents rate the importance of digital health significantly higher than their digital health skills
• Respondents perceive pharma as a digital frontrunner and a competent stakeholder
Barriers:• Respondents most urgent learning
needs are highly unlikely to be related to the promotion of pharma products and science
• Respondents are highly unlikely to use an asset owned by pharma as a primary source to support their most urgent learning needs
• Respondents rate the importance of trust in healthcare significantly higher than their trust in pharma companies
• Respondents perceive pharma as pushy, biased, driven by self-interest and not good at being interested in and understanding the real-world needs of HCPs
In healthcare, the overarching goal for all 100+ stakeholders across the health value chain must be to improve social value, where ‘value’ is the health outcomes that matter most to human beings relative to the feasibility of achieving those outcomes.
As GTM complexity increases, there is no doubt that the future holds a radically different healthcare reality at the heart of which both engagement barriers and potentials grow more prominent by the day. In this new reality, existing payment and incentive models will be rendered obsolete and replaced by funding based on the holistic value provided along the entire disease journey by a coalition of health care providers (25).

7
Trust as an Opportunity
Yuval Noah Harrari, historian and futurist, proposed the following vision for a post-pandemic world:
“Humanity needs to make a choice. Will we travel down the route of disunity, or will we adopt the path of global solidarity? If we choose global solidarity, it will be a victory against all future epidemics and crises that might assail humankind in the 21st century. But to achieve such a level of cooperation, you need trust.” (26).
The quote illustrates that ROI/ROE of engagement will ultimately translate into the presence or absence of trust among stakeholders and that levels of trust can either make or break the combined efforts of front-end and back-end engagement. So, what is the status of trust in the world? According to the global reference source for measuring trust - Edelman Trust Barometer (27) - we are fast approaching a tipping point where FEAR becomes greater than TRUST. Only 1 in 4 has good information hygiene combined with trust in all information sources, which is at a record low - painting a picture of eroding trust across the board. The pandemic has added to persistent personal and societal fears combined with a widespread belief that the pandemic unfairly burdens those
less fortunate - painting a picture of fear penetrating the fabrics of society. Typically, it is difficult to restore a fundamental lack of trust overnight. But we are not living in regular times. The post-pandemic world will hold the potential for stakeholders to rebuild their image from the ground up. There is a need to combat all urgent public health challenges and revitalize disease ecosystems. Improving our healthcare systems is the most urgent foundational problem of our time, and businesses are the only societal institutions regarded as both ethical and competent enough to come to the rescue (27).
Edelman has historically recorded the trust levels within healthcare. On a scale from 1 to 100 - where 100 is the highest obtainable level of trust - pharmaceutical companies have been rated consistently around 55 for the last decade (28), making them the lowest scoring entity within the nine sub-sections of healthcare measured. In the spring of 2020, overnight pharmaceutical companies rose to a trust score of 73, making them the highest-scoring entity (29). The rapid rollout of Covid-19 vaccines has made vaccine-producers like AstraZeneca, BioNTech, Johnson & Johnson, Moderna, and Pfizer household names, and the whole industry is winning praise for cooperation. The big question then becomes; is this a trust bubble that will go away?

8
Or is it the opportunity of a lifetime for the industry to reposition itself and reshape its relationship with the world? The world’s eyes will look at every move the industry makes short-term, and that is in itself a priceless opportunity.
10-15 years ago, trust between stakeholders was a more transactional concept - a legal agreement between parties to formalize the integrity of mutual self-interest. As a post-pandemic concept, trust is shaping a more humane and just world. The 1936 edition of Carnegie Hall’s
“How to Win Friends and Influence People” stated that “the surest way to gain trust is to admit to others that you are wrong”.
Trust is, in that context, a willingness to be vulnerable to the actions of another person or group based on the feeling, judgment, belief, expectation, and confidence that the other person or group will engage based on exemplary virtues (30). As we solve complex problems and find arrays of sustainable growth, big corporations must adapt to this more human-based understanding of trust. Facilitating virtues such as being benevolent, competent, ethical, fair, honest, open and reliable will become the GTM capital of the 21st century, and no one is better positioned and equipped to take leadership than the pharmaceutical industry.
Next Practice GTM
During the pandemic, we learned that coexistence is vital for our wellbeing and that one man’s actions will have vast implications for the collective response in times of crisis. We have experienced how complex systems are interconnected and how their wholes and parts depend on each other. We have sensed that our existence is symbiotic and that individual needs and the needs of nature itself are deeply intertwined. Maybe for the first time, we have realized that nothing - no one - exists in isolation. That being human is fundamentally about transcending a purpose beyond self-interest (31).
Before the outbreak of COVID-19 in August 2019, the Business Roundtable, a group of 180 CEOs of the largest corporations, called for a new standard of corporate responsibility reflecting a fundamental commitment to all stakeholders - not just shareholders (32). At the core, the next practice GTM models will revolve around a dialogue between all accountable stakeholders to identify shared opportunity spaces and put into action a future concept of coexistence. The pharma industry must focus its engagement efforts on facilitating a dialogue based on the right questions:
• Who are “we”?• What problems do we need to solve?• Which unmet human needs do we have
to address?• When do we reach the tipping point?• Why do we have all have skin in the
game?• Where should we play together?• How do we all win?• How big can we think?• How small can we start?• How fast can we move?
In a post-pandemic world, relevance and levels of trust are no longer determined exclusively by position, scale and capabilities in producing products or delivering services. Coexistence powered by networks, platforms and partnerships will play an equally important role in becoming more relevant and trusted.
The first is an orderly approach that rests on conformity and administration. It is the realm of best practices where the focus lies on improving efficiency and developing what already exists. Inherently, change is a transactional act that modifies the systems and processes in which stakeholders already interact. The latter is an explorative approach where co-creation and co-experimentation are necessary to shape ground-breaking next practices. Essentially, change is a transformational repurposing of how stakeholders

9
NEXTPRACTICE
GTMPHARMA
BACK-END PUSH
FRONT-ENDPULL
MARKETperceive their roles, responsibilities and relationships in society at large (33). It is the facilitation of shared opportunity spaces wherein broad stakeholders can supercharge efforts to combat all urgent public health challenges and revitalize disease ecosystems from the ground up.
The best practice associated with sales reps out in the field equipped with marketing materials trying to get a foot in the door, promoting the story of great products and science, will simply render obsolete. The day-to-day front-end engagement with healthcare professionals must establish interactions around solution-led point-of-care initiatives that will respond to unmet human needs
along the disease journey. Programs above and beyond the pill enabling more resilient disease ecosystems by empowering HCPs and patients to improve the outcome/cost ratio of healthcare. In the continuous back-end engagement with public authorities, pharma companies must become much more proactive in putting forward next practice ideas. Public stakeholders are unlikely to have the surplus capacity and capabilities to bring forward necessary innovation. So, what is the sustainable balance between the industry taking leadership to solve complex problems and public authorities in return opening up long-term pockets of commercial opportunities?
What will a resilient disease ecosystem look like, and how does that enable double-digit growth? Why is next practice GTM not a one-dimensional negotiation around the average price point in the market for a given clinical effect? The evidence burden will be on the pharmaceutical industry to propose the next practice - opening up a significant innovation gap compared to how they currently operate. Both front-end and back-end engagement should focus on a return on experience around virtues of trust, enabling pharma companies to bring their next practice evidence to the table and eventually to reshape their relationship with the world.

10
Digital as an Enabler of Innovation
Coronavirus has accelerated the rise of digital health, ranging from solutions for telemedicine and teleconsultation, remote monitoring, connected devices, digital health platforms to health apps. The pandemic has also amplified the utilization of health data and application in systems based on big data, for instance, epidemiological research and AI-enabled diagnosis support (34). The discussion about whether it’s right to prioritize modern technology in healthcare systems is over. In a public survey conducted by the NHS, 77% of respondents agreed that digital health technology is essential to the NHS’s ability to respond to the pandemic, and similarly, 73% agreed it is crucial to the future of health services in the UK (35).
The pandemic has proven beyond doubt that better tech is vital for our health and the provision of health care services. We now must learn and unlearn from the digital leap of the lockdown to identify the essential capabilities that need scaling across our disease ecosystems to make them more resilient in the future. According to Douglas Rushkoff, digital theorist and host of the podcast Team Human, we can develop the cultural immune response required to face any urgent problems together by utilizing
the microlocal capacities of digital ecosystems (36). As Point of Care (PoC) shifts away from analogue and becomes more decentralized, we can use our emerging digital sensibilities to enable an out-of-system ability to create more meaningful experiences and produce better outcome/cost ratios.
All evidence points towards digital health being a COVID-19 aftershock in its own right. We would argue that it is not! It is merely an enabler and amplifier of necessary change. Ordinary life before the pandemic was already a catastrophe of desperation and exclusion for too many human beings, an environmental and climate disaster, an obscenity of inequality (37). The pandemic has dragged things out into the daylight, proving that in a few weeks, it is possible to put an economic system on hold everywhere in the world and, at the same time, a system that we thought was impossible to slow down or redirect. Putting on full display initially one by one, then as a group, what we are most attached to and what we are ready to give up (38). Digital health in a post-pandemic world is merely a practical application of our deep-rooted desire to stay alive. A transformative resilience that enables us to thrive under even the most difficult circumstances.
11
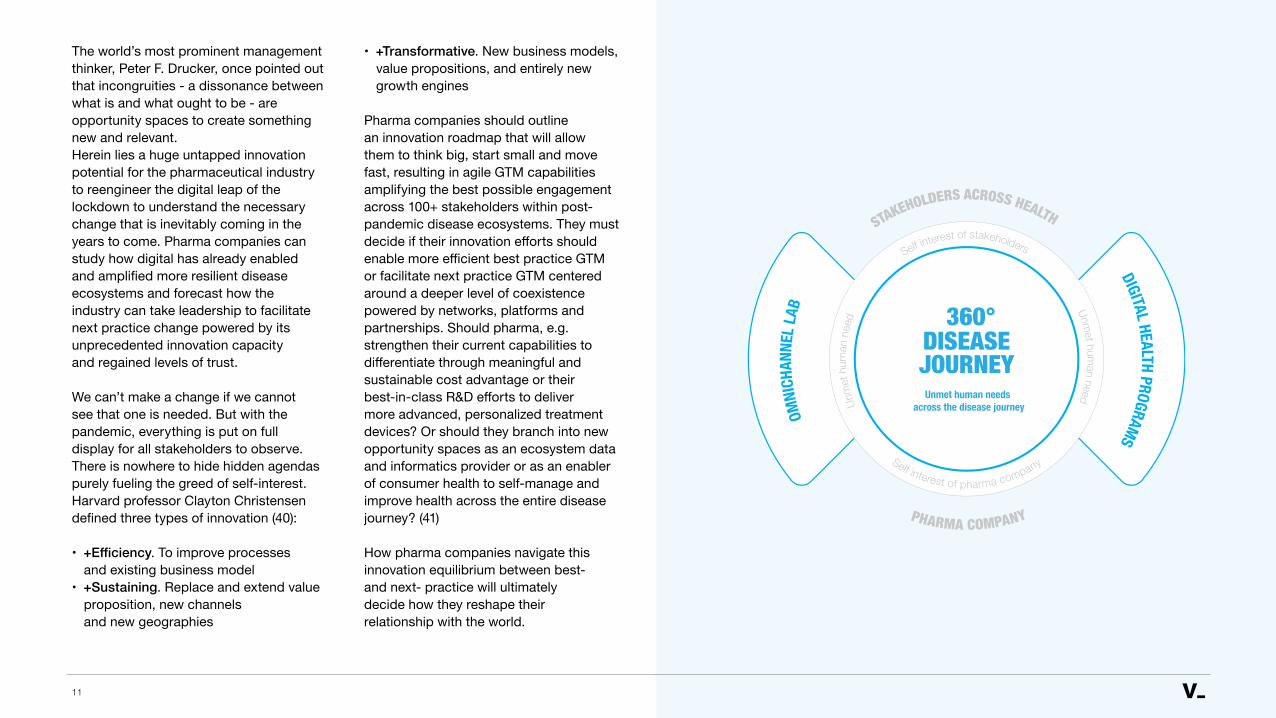
OMNI
CHAN
NEL L
AB
DIGITAL HEALTH PROGRAMS
PHARMA COMPANY
STAKEHOLDERS ACROSS HEALTH
Self interest of pharma company
Self interest of stakeholders
Unm
et h
uman
nee
d
Unmet hum
an need
360°DISEASEJOURNEY
Unmet human needs across the disease journey
The world’s most prominent management thinker, Peter F. Drucker, once pointed out that incongruities - a dissonance between what is and what ought to be - are opportunity spaces to create something new and relevant. Herein lies a huge untapped innovation potential for the pharmaceutical industry to reengineer the digital leap of the lockdown to understand the necessary change that is inevitably coming in the years to come. Pharma companies can study how digital has already enabled and amplified more resilient disease ecosystems and forecast how the industry can take leadership to facilitate next practice change powered by its unprecedented innovation capacity and regained levels of trust.
We can’t make a change if we cannot see that one is needed. But with the pandemic, everything is put on full display for all stakeholders to observe. There is nowhere to hide hidden agendas purely fueling the greed of self-interest. Harvard professor Clayton Christensen defined three types of innovation (40):
• +Efficiency. To improve processes and existing business model
• +Sustaining. Replace and extend value proposition, new channels and new geographies
• +Transformative. New business models, value propositions, and entirely new growth engines
Pharma companies should outline an innovation roadmap that will allow them to think big, start small and move fast, resulting in agile GTM capabilities amplifying the best possible engagement across 100+ stakeholders within post-pandemic disease ecosystems. They must decide if their innovation efforts should enable more efficient best practice GTM or facilitate next practice GTM centered around a deeper level of coexistence powered by networks, platforms and partnerships. Should pharma, e.g. strengthen their current capabilities to differentiate through meaningful and sustainable cost advantage or their best-in-class R&D efforts to deliver more advanced, personalized treatment devices? Or should they branch into new opportunity spaces as an ecosystem data and informatics provider or as an enabler of consumer health to self-manage and improve health across the entire disease journey? (41)
How pharma companies navigate this innovation equilibrium between best- and next- practice will ultimately decide how they reshape their relationship with the world.
12
The Innovation Equilibrium
As organizations aim to become more innovative, they often seem to start from the same assumption: “We need more or better ideas.” However, dry spells of successful innovation are more likely to be caused by the inabilities to notice and scale good ideas already on the table. It’s not an idea problem; it’s a recognition problem (42). How do we set up an organization to work better with existing ideas? How do we anchor innovation accountability within the organization? How do we unleash innovative capabilities like associating, questioning, observing, experimenting and networking within our organization? (43).
When trying to scale innovation efforts across the board, organizations face a significant challenge: the systems that enable success with today’s business model reinforce organizational behaviors and mindsets inconsistent with discovering tomorrow’s model resulting in inertia. If we give people more time in an environment stifled by inertia, we give them more time to do things the old way; if we give them new skills, those will simply go to waste if they don’t fit with existing routines (44). So, any innovation programs based on the assumption that the organizational behaviors and mindsets will be ready
for radical change is likely to come at a very high acquisition cost. Programs must carefully consider the balance between vertical innovation - more radical innovation carried out in smaller pockets of the organization - and horizontal innovation - more incremental innovation carried out across entire organizations.
By definition, a therapeutical market includes a pharmaceutical drug, a disease and a society. The level of GTM complexity can vary enormously across therapeutic markets. For example, the primary revenue driver for pharma companies can be the share of voice, the pricing, or listings. The critical customer to engage with can be GPs, hospitals/insurance, or nations/regions. Sustainable commercial growth requires that GTM models constantly adjust to the dynamics of market conditions and customer requirements (45).
We have identified a strong correlation between increased GTM complexity and the necessity to shape ground-breaking next practices, working with top ten pharma companies within the last two years. On the other hand, if GTM complexity is relatively low, we recommend that clients focus on improving the efficiency of current best practices.
We have developed an assessment tool to help clients navigate the innovation equilibrium better. Based on more than 100 parameters, the tool evaluates the innovation potential (best or next), the innovation urgency (slow or fast) and the organizational acquisition cost (high or low) associated with a specific therapeutic market. We have used the tool to map the innovation landscape across therapeutic markets and to suggest the most appropriate organizational setups, carefully considering the balance between vertical innovation and horizontal innovation.

13
Human-2-Business at the Heart of GTM
The belief system of pharma companies revolves around statements such as ‘doing now what patients need next’ (46) and ‘help people to do more, feel better, live longer’. (47). The human experience has perhaps never been as fundamental to a successful business as it is now. As we begin to emerge from the COVID-19 crisis, those companies that turn out to be most resilient in the long-term will be those that best adapt to meet new human needs, priorities, and actions (48). As pharma companies seek to reshape their relationship with the world, they will need to challenge their more traditional B2B/B2C efforts with a human-2-business (H2B) mindset.
What is H2B?
The infectious coronavirus knows no distinctions and no geographical boundaries. We have all shared the same omni experience, witnessing a system put on hold everywhere in the world from one day to the next. We have all feared for the lives of our loved ones and questioned if the system would be able to sustain us. Between March and May 2020, we conducted a meta-analysis (49) of 165 selected articles published across 30
global media outlets, representing a wide range of expert views from diverse fields such as economics, sociology, anthropology, medicine, history and philosophy. The objective was to map the human omni experience of COVID-19. We mirrored the findings with existing health behavior models (Health Action Process Approach Model, Health Belief Model, I-Change Model, Precede-Proceed Model, Cognitive Reframing, Social Cognitive Theory) to create the I-Model. The I-Model consists of 18 human-centric questions:
PERCEIVED SUPPORT: Who can I trust? Who can provide resources?Who can be on my team?
PERCEIVED SELF-ESTEEM: What do I value most? What do I hope for? What do I cope with?
PERCEIVED SELF-EFFICACY: Where do I act? Where do I participate? Where do I consume?
DETERMINANTS OF HEALTH: When do my genes impact me? When does my lifestyle impact me? When does the environment impact me?
14
SUBJECTIVE NARRATIVE: Why do I feel the way I feel? Why do I think the way I think? Why do I behave the way I behave?
OBJECTIVE NARRATIVE: How is my physical health? How is my mental health? How is my quality of life?
We have subsequently used the I-Model as a template to deconstruct the human omni experience of multiple chronic diseases. To create what we refer to as H2B maps. It is a key to unlock a deeper understanding of the things that matter most in life to people with health challenges. To understand what they need next or how they can do more, feel better, live longer. The idea is to study how the different dimensions of the I-Model evolve across the stages of a specific or intersected disease journey (everyday life, early awareness, symptoms, evaluation, diagnosis, treatment, finding the new normal, disease progression, end-stage). We have also leveraged the I-Model to create holistic health data models inspired by existing standard uestionnaires and human-centric data sets. The purpose has been to outline the H2B data points that matter the most.
Identifying Shared Opportunities
In healthcare, the overarching goal for all stakeholders must be the immediate and sometimes proactive response to unmet human needs. H2B maps and data models are crucial to identifying such shared opportunities across the disease journey wherein broad coalitions of stakeholders can engage in a relevant and trusted dialogue. A shared opportunity space holds untapped potential for stakeholders to revitalize disease ecosystems together while simultaneously serving their self-interest.
In the past, companies rarely perceived themselves as agents of social change. Yet, the connection between social progress and business success is becoming increasingly clear (50). H2B can, within a pharmaceutical organization, cultivate an ability to understand how the landscape of health transforms and how the organization can apply positive impact through action. In more than one way, it can underline the importance of nurturing an eye-opening outside-in perspective. H2B is a way to hack organizational behaviors and mindsets to accelerate the discovery of tomorrow’s GTM model. We use horizon scanning as a methodology to populate H2B maps with human-centric insights.
We monitor insights within disease ecosystems via ethnographic/anthropological research, roundtable discussions, interviews in combination with more digitally-based techniques like online questionnaires, social analytics/listening, competitor benchmarks and setting up curated news feeds. We utilize the I-Model to map the unmet needs of patients and HCPs and how they ideally want to interact. After completing H2B mapping exercises, we match the potential of social value from each identified unmet need - or patterns of unmet needs - up against the potential of commercial, market access or medical value serving the self-interest of the pharma company. Afterwards, we map - based on our deep understanding of GTM complexity within the specific therapeutic market - which stakeholders across the health value chain are most likely to have:
• Impact on the success of the pharma company (viability)
• A self-interest in contributing to the gated unmet need of patients and HCPs (desirability)
• A genuine interest to engage and collaborate (feasibility)
The result is a series of identified shared opportunities that can inform and inspire the GTM model and the day-to-day engagement with stakeholders.
There is an urgent need for commercial players within health to facilitate public-private-people coalitions (PPP coalitions) based on a shared plan of action. Local governments, markets, and cultures will determine PPP coalitions’ unique shape and potential (51). The H2B map will allow pharma companies to be more proactive in setting a human-centric agenda worth discussing and engaging into and enable them to take leadership as facilitators of PPP coalitions.
Digital engagement will hold the power to enable and amplify the necessary change dictated by the H2B agenda. To leverage the vast untapped potential of shared opportunities, pharma companies must carefully navigate the innovation equilibrium to optimize the efficiency of best practice GTM powered by omnichannel efforts and venture into next practice GTM powered by digital health programs.

15
The Omnichannel Lab
The pharmaceutical engagement strategy has traditionally focused on the personal interactions between the field force and the healthcare professional. Despite the rapid development of new digital communication channels for the last decades, companies have been slow to adapt systemically. As a result, interactions with stakeholders have primarily grown organically as siloed activation in multiple channels with limited coordination - also known as multichannel marketing (52). An integrated strategy based on omnichannel efforts is now consistently executed by first-movers across the industry.
Instead of a fragmented and siloed approach, omnichannel efforts employ the simultaneous orchestration of digital and analogue channels for customer engagement to provide a seamless and frictionless customer experience based on multiple stakeholders’ unmet needs, including consumers/patients, HCPs and payers. Whereas multichannel used to be a discipline managed solely by sales and marketing divisions within the company, it has become more of a multidisciplinary approach led by highly talented impact teams, including sales, marketing, digital execution, market access, medical affairs, and innovation excellence into the mix.
In today’s fragmented disease ecosystems, omnichannel can ultimately allow pharma companies to facilitate the critical mass of dialogue across and among stakeholders to identify and utilize shared opportunities and prevent misalignment of opposite mindsets based on cultural barriers and deep-rooted self-interest. By integrating and optimizing the experience of data, technology, content and services across the digital ecosystem, proactive first-movers can claim a space as shared disease owners and dramatically increase their brand equity while going above and beyond their products. According to a recent survey, HCPs greatly appreciate the industry’s newfound desire to diversify its communication beyond product information and find more value in providing additional support services such as education on remote support and digitized patient information. 82% of HCPs say they have seen pharma companies change what they communicate - delivering not just product information - but content and support that meets their most pressing needs (53).
More conservative companies position omnichannel as a way of migrating their obsolete mindset - of getting a foot in the door to PUSH the story of their great products and science - from an analogue to a digital platform.

16
In a post-pandemic setting, this approach will result in a much lower share of voice and a lower level of trust among stakeholders. For HCPs - to give an example - trusted digital engagement is much more likely to be based on a PULL experience of getting support based on what they need, where, when and how they want it. The expectation will be that pharma companies can deliver real value to essential tasks, freeing up more time for patients and reducing administrative costs. Sales reps’ rich and unique customer insights - formed by decades of engagement - can be leveraged to repurpose and architect even more personalized and targeted HCP experiences within the digital ecosystem of a disease.
Success will depend on pharma’s ability to do the right things right. When doing the right things, companies will facilitate an H2B agenda and subsequently impact the market by offering valued data, technology, content and services that meet the unmet needs of consumers/patients, HCPs and payers. Companies must, in parallel, acquire the 360 capabilities to do things right by capturing actionable insights on how to efficiently raise the share of voice while lowering the acquisition cost. Doing the right thing will depend entirely on the value proposition offered; doing things right will depend on delivering a personalized and frictionless customer experience. The value proposition will rely mainly on the content provided. Pharma must become the voice in the world telling the story of unmet human needs along the disease journey - inviting stakeholders to join forces in the urgent effort of building more resilient disease ecosystems.
In a recent HCP study (54), we benchmarked 60 HCP learning needs against 55 different content types. We discovered a big gap between what pharma regards as high-impact content types versus HCPs perception of relevance. In close collaboration with pharma clients, we have nurtured the HEART model (55) to propose a set of principles for curating relevant and trusted content:
• HCP-centered. Curate content according to the needs and expectations of HCPs. Being regarded as benevolent: You will protect their interests.
• Exemplary. Curate content that sets a desirable standard of quality for HCPs. Being regarded as competent: You can achieve the desired outcome.
• Always on. Curate up-to-date content continuously validated according to HCP preferences. Being regarded as reliable: You are consistent in your actions.
• Repurposable. Curate actionable content that HCPs can reuse in many different contexts together with many other people. Being regarded as fair and ethical: You increase equality for everyone involved and promote a shared code of conduct.
• Transparent. Curate content that always explicitly communicates intended use. Being regarded as open and honest: You share all information transparently, truthfully and authentically.
The 360 capabilities to do omnichannel right represents a complex channel for many pharma companies. It goes way beyond converting full-time employees (FTEs) from the field force into digital investments. Capabilities such as the creation of H2B maps, segmenting audiences, establishing an editorial line, setting up a content factory,
creating a highly modular approach to content, testing different consumption formats, establishing owned/sponsored/earned presence across digital channels, creating meaningful inward- and outward- paths for users, measuring impact and converting data point into actionable insights, must be fully integrated. Often companies only utilise a subset of the capabilities, rendering measuring pharma’s impact and influence within the ecosystem irrelevant.
We recommend setting up an omnichannel lab within a prioritised therapeutic market to discover through action what future-proof relevance and trust look like. The lab can host a vertical innovation approach where a talented impact team can conduct thousands of micro-experiments within the same digital disease ecosystem. By thinking big, starting small and scaling fast, the lab can within 4-5 months produce a robust set of actionable insights that will eventually validate use cases for best-practice omnichannel execution. Based on the lab’s learning, the pharma company can implement full omnichannel capabilities across all therapeutic markets. We have experienced how the omnichannel lab approach can increase the share of voice and dramatically reduce acquisition costs.

17
Digital Health Programs
Pharma is beginning to realize that it needs to advance beyond a sole focus on omnichannel efforts to claim their spot as shared disease owners. Engagement around content and events is not enough to attract critical attention among the stakeholders that matter most; it’s time for turning talk into action. Digital engagement strategies must become more inclusive of point of care challenges within disease ecosystems. Pharma is turning to clinical-grade digital therapeutics (DTx), directly impacting patient outcomes in specific therapeutic areas (56). DTx delivers interventions directly to patients using evidence-based, clinically evaluated software to treat, manage, and prevent a broad spectrum of diseases and disorders (57). Several trends underline the development:
• Global venture capital funding for digital health companies hit a $15 bn high in the first half of 2021, driven mainly by telehealth investment. Funding activity increased by 138% during the first half of 2021, compared to $6.3 bn raised in the first half of 2020. (58)
• Reimbursement pathways for digital health solutions are evolving at different speeds in different European markets. Germany, Sweden, and the United Kingdom are relatively mature markets where governments have introduced standardized reimbursement pathways (59)
• Most major DTx companies have attracted at least one investor or partner from the pharmaceutical sector (60)
Eddie Martucci, CEO & Co-founder of Akili Interactive, said:
“Today, patients have a limited - if any - relationship with the companies that make and distribute their medicine. The benefit of digital health is that we have a chance, through data, to deeply engage with our patients - to listen to them, and take cues from them. Digital is a new modality, and there is no well-oiled machine on how to prescribe and follow up with a software-based medication.” (61).
The quote illustrates how digital health solutions can create closer proximity to people living with health challenges.

18
The modality of digital health solutions - together with the emerging digital sensibilities of the world - can enable providers to understand better what people need next or how people can do more, feel better, and live longer.
We argue that any DTx-like initiative will only be successful if carefully positioned within the context of a more comprehensive digital health program - a portfolio of purely digital or hybrid projects facilitated by a pharma company in collaboration with a PPP coalition of stakeholders (people, public, private) to revitalize a disease ecosystem. Such programs can position the industry as shared disease owners operating based on mutual self-interest, as they promote the H2B agenda and take the role of architects of the red thread across all projects and thereby hold power to decide whom to involve. Let us illustrate the outline of a hypothetical digital health program where the mutual self-interest of stakeholders is to cut the rate of hospitalization in half, and the self-interest of the pharma company is to improve the stay-time of their product:
• Bundle treatment together with DTx solution for point of care in partnership with digital start-up
• Offer complimentary membership of virtual patient support platform in collaboration with a digital health provider
• Build a patient-to-patient forum together with a patient organization
• Set up a scaled platform for voluntary community support in partnership with an insurance company
• Create a quality of life dialogue tool for specialty nurses to use during regular check-ups
• Sponsor academics to conduct field studies investigating transitions of care
• Host a series of high-profile roundtable discussions to push urgency around the problems that need attention
• Establish a holistic health data model in collaboration with payers
• Conduct a value-based pilot in a municipality to demonstrate the outcomes
A program approach is more likely to impact hospitalization rates and stay-time than a stand-alone project simply by establishing critical mass within the disease ecosystem. We see a clear tendency towards siloed activation in multiple different setups with limited coordination. The tier one pharma companies we work with still struggle to
prioritize an integrated portfolio strategy to digital health. While waiting for reimbursement pathways to open up, investing in and creating partnerships with digital start-ups is too slow and limited. The industry must change its mindset and become first-movers. We have identified 50 categories of digital health projects that can support a modular and proactive setup when architecting a digital health program. A next-practice GTM model based on the agile execution of an ambitious digital health program together with an omnichannel lab will position pharma as a shared disease owner and a facilitator of necessary change.
Recommendations
Being who we are - determines what we do. In leadership, character matters because we view the world through a prism of identity. To be the change, we must first cultivate a deep understanding of who we are and what guides us in life. We must inspire ourselves to embark on a profound intellectual, emotional and social journey. The renewal of societies can go forward only if someone cares and decides to act. That means breaking through the rigidity and complacency of the status quo, becoming a curious and courageous pioneer of systemic change.
We must become advocates by letting our actions speak louder than our words. We have outlined a series of concrete actions pharma companies can take:
• Leverage horizon scanning to understand COVID-19 aftershocks
• Assess the GTM innovation potential of specific therapeutic markets
• Carefully navigate the innovation equilibrium between best-practice and next-practice GTM across markets
• Balance how you set up horizontal and vertical innovation efforts to optimize impact while reducing acquisition costs
• Utilize the I-Model to map unmet human needs within a disease
• Create H2B maps to identify shared opportunity spaces across the disease journey
• Broaden engagement across 100+ stakeholders based on outside-in stakeholder maps
• Become a voice in the world by producing content according to the HEART model
• Setting up an omnichannel lab to discover through action what future-proof relevance and trust look like
• Leverage a digital health program to take a position as shared disease owner

References 1. Call for emergency action to limit global tem-
perature increases, restore biodiversity, and protect health. The Lancet. 2021.
2. WORLD PREVIEW 2021. Outlook to 2026. Eval-uate Pharma. 2021.
3. AstraZeneca vaccine - was it really worth it? BBC World. 2021.
4. Is pharma ready to talk cure in cancer? Maybe with equitable access, more screening, ASCO preview panel says. Fierce Pharma. 2021.
5. To our shareholders. Johnson & Johnson Annual Report 2020. 2021.
6. Status on coronavirus. Worldometers.info. 2021.7. Global economic prospect. World bank. 2021.8. 8: World Employment and Social Outlook.
Trends 2021. International Labour Organization. 2021.
9. The impact of the COVID-19 pandemic on non-communicable disease resources and services: results of a rapid assessment. WHO. 2020.
10. COVID-19: a new lens for non-communicable diseases. The Lancet. 2020.
11. Health at a Glance. OECD. 2020.12. OECD Health Statistics. Stats.oecd.org. 2021.13. Health for everyone? OECD Report. 2019.14. Data Visualizations. vizhub.healthdata.org. 2021.15. Over 2 billion Britons risk dying early from multi-
ple illnesses. The Guardian. 2018.16. The Extra Cost of Comorbidity: multiple illnesses
and the economic burden of non-communica-ble diseases. Cortaredona & Ventelou. BMC Medicine. 2017
17. A look into the future of the COVID-19 pandemic in Europe: an expert consultation. The Lancet. 2021.
18. Sajid Javid’s warning of a 13 million NHS waiting list is well within the realms of possibility. Twitter. 2021.
19. Interview with Severin Schwan. WSJ. 2011. 20. Bringing down the cost of cancer treatment.
Nature. 2018.21. An Arm and a Leg: The Rising Cost of Cancer
Drugs and Impact on Access. American Society of Clinical Oncology Educational Book 41. 2021.
22. Making cancer treatments affordable today won’t hurt tomorrow’s innovation. Fortune. 2021.
23. Horizon scanning of ongoing GTM complexity trends across Europe 2019-2021. Valtech. 2021.
24. Download sessions with Health Care Profes-sionals (HCPs) on their role and relationship with pharma. Valtech. 2021.
25. Pathway to success in outcome-based contracting. Navigating payer needs. KPMG. 2020.
26. The world after coronavirus. Yuval Noah Harari. Financial Times. 2020.
27. Edelman Trust Barometer. Edelman. 2021.28. Edelman Trust Barometer. health Report.
Edelman. 2018.29. Pharmaceutical Market Europe. Vol June. 2020.30. Trust and Thriving Learning Eco-systems. Ross
Hall. Wise. 2021.31. Human-2-business. A podcast about the future
of health. Rasmus Rask. Valtech. 2020.32. Business Roundtable Redefines the Purpose
of a Corporation to Promote An Economy That Serves All Americans. Businessroundtable.org. 2019.
33. Where to Play next in healthcare. Valtech. 2020.34. The rise of digital health technologies during the
pandemic. European Parliament Think Tank. 2021.
35. Digital health during the COVID-19 pandemic: Learning lessons to maintain momentum. Patient Coalition for AI, Data and Digital Tech in Health. 2021.
36. Coronavirus Is Making Me Believe in the Power of the Internet Again. Douglas Rushkoff. Medium. 2020.
37. The impossible has already happened’: what coronavirus can teach us about hope. Rebecca Solnit. The Guardian. 2020.
38. What protective measures can you think of so we don’t go back to the pre-crisis production model? Bruno Latour. www.bruno-latour.fr. 2020.
39. The Discipline of Innovation. Peter F. Drucker. Harvard Business Review. 2002.
40. What type of innovation are you talking about? strategyzer.com. 2020.
41. Predicting the future of healthcare and life sciences in 2025. Deloitte. 2020.
42. Innovation Isn’t an Idea Problem. David Burkus. Harvard Business Review. 2013.
43. The Innovator’s DNA. Jeffrey H. Dyer, Hal Gregersen and Clayton M. Christensen. Harvard Business Review. 2009.
44. Breaking Down the Barriers to Innovation. An-thony et al. Harvard Business Review. 2019.
45. Case-study: Pharma go-to-market strategy. Bain & Company. 2021.
46. Annual Report 2020. Roche. 2020.47. Annual Report 2020. GSK. 2020.48. A human-first approach. Customer-led market-
ing in the Covid era. Deloitte digital. 2021.49. The human omni experience of COVID-19.
Valtech. 2020.50. The Ecosystem of Shared Value. Mark R. Kramer
and Mark W. Pfiter. Harvard Business Review. 2016.
51. Introducing Human-2-business. Valtech. 2020.52. Why Pharma Marketers Are Embracing
Omnichannel Marketing. Pete Stark. PharmaExec.com. 2021.
53. Reinventing Relevance. Accenture Healthcare Provider Survey May 2020. Accenture. 2020.
54. A benchmark of 60 HCP learning needs against 55 different content types to identify relevance. Valtech. 2020.
55. The HEART Model. Valtech. 2021.56. Shifts in pharma’s 2020 digital health landscape.
Naomi Fried. Mobilehealthnews.com. 2020.57. Understanding DTx. A New Category of
Medicine. Dtxaliance.org. 2021.58. Digital health dollars hit $15B high driven by
telehealth investment in 2021. Heather Landi. Fiercehealthcare.com. 2021.
59. The European path to reimbursement for digital health solutions. Carola Brinkmann-Sass, Laura Richter, Tobias Silberzahn, and Adam Somauroo. McKinsey & Company. 2020.
60. Digital Therapeutics: Preparing for takeoff. Mike Joyce, Olivier Leclerc, Kirsten Westhues, and Hui Xue. McKinsey & Company. 2018.
61. Building Pharma-Digital Therapeutic Alliances. Rock Health. 2020.
62. Unslpash imagery: https://unsplash.com/photos/FAQ4RE76Nvs https://unsplash.com/photos/qrdYYSLzGuY https://unsplash.com/photos/9VPtNW84vGI https://unsplash.com/photos/glpYh1cWf0o https://unsplash.com/photos/rCOWMC8qf8A https://unsplash.com/photos/kqL6CfFc664

https://www.valtech.com/en-dk/industries/health/
We are Valtech. We transform by doing and deeply care about improving the end user experience.
Conny CarlzonGlobal Lead, Valtech Health [email protected]
Rasmus RaskLead Business Designer & Futurist, Valtech Health [email protected]