bioabsorbable screws for reduction of lisfranc’s diastasis in athletes
TRANSCRIPT

Bioabsorbable Screws for Reduction ofLisfranc’s Diastasis in Athletes
Amol Saxena, DPM1
This was a study of 15 athletes who sustained Lisfranc’s diastasis and were treated with surgicalreduction and fixation with 3.5mm bioabsorbable poly-L lactic acid screws. Patients were prospectivelyevaluated for their ability to return to activity, maintenance of reduction, and need for implant removal.The average patient age was 28 years; there were 9 females and 6 males. Average followup was 36months (range: 12–62). The mean return to activity time was 4.2 months (range: 3–6), with a significantdifference between males and females (P � .02), 3.4 versus 4.7 months, respectively. The meanpreoperative American Orthopedic Foot and Ankle Society midfoot score was 35.4 � 25.0, whichincreased postoperatively to 92.7 � 7.7 (P � .00001). Overall there were 10 “excellent,” 4 “good,” and1 “poor” result. Patients were statistically more likely to have less than an excellent result when diagnosiswas delayed by more than 6 weeks (P � 0.01). One patient demonstrated a radiographic loss of reductionbut returned to full sports activities. The patient with the longest delay in diagnosis demonstratedanatomic reduction but exhibited radiographic degenerative changes and scored a poor result. Threepatients required a second surgery for screw or screw head removal. Bioabsorbable screws appearsufficient for treating Lisfranc’s diastasis but do not necessarily obviate fixation removal. (The Journal ofFoot & Ankle Surgery 44(6):445–449, 2005)
Key words: Lisfranc, tarsometatarsal, midfoot sprain, athlete, absorbable fixation
Lisfranc fracture/dislocations are a disabling injury, par-ticularly for the athlete. Return to sports takes approxi-mately 4 months after injury (1–3). Widening or diastasis ofgreater than 2mm between the first and second metatarsalsand dislocation of the tarsal-metatarsal articulations oftenrequire open reduction and internal fixation (ORIF) (1–6).A diastasis screw is placed to reduce the instability betweenthe first and second metatarsals and maintain anatomicalignment. Otherwise, arthrosis and flatfoot deformity canoccur (1–6).
Metallic screw fixation, particularly for the diastasis be-tween the medial 2 metatarsals are typically removed after10 weeks or prior to full activity (1, 3–5, 6). If metallicscrews remain in this setting, fatigue fracture of the hard-ware may occur. However, removal creates an additionalcost and surgical procedure for the patient. Metallic pins,which could be removed in an office setting and withoutadditional anesthesia, may not provide adequate stability. Inaddition, removal of both types of metallic fixation canresult in loss of alignment/reduction (1–3, 5, 6).
Address correspondence to: Amol Saxena, DPM, Dept. of Sports Med-icine, Palo Alto Medical Foundation, 795 El Camino Real, Palo Alto, CA94301. E-mail: [email protected]
1Department of Sports Medicine, Palo Alto Medical Foundation, PaloAlto, CA.
Copyright © 2005 by the American College of Foot and Ankle Surgeons
1067-2516/05/4406-0005$30.00/0doi:10.1053/j.jfas.2005.07.019VOLUME 44
Due to these problems, bioabsorbable fixation has beendescribed for Lisfranc injures (6). Thordarson and Hurvitz,in their series of Lisfranc injuries, determined that bioab-sorbable screws were able to maintain satisfactory align-ment.
It is proposed that bioabsorbable screws will maintainreduction and will degrade only after the timeframe typicalfor screw removal. However, because they may remain inthe foot longer, it is possible that bioabsorbable screws canloosen as they degrade and can cause a loss of reduction. Inaddition, sinus tracts, granulomas, or abscess formation canoccur with bioabsorbable fixation. This study evaluatedwhether bioabsorbable screws used for reduction of Lis-franc joint diastasis obviate the need for additional screwremoval surgery and adequately maintain alignment, allow-ing for return to preinjury activity levels. In addition thecomplications with bioabsorbable screws were assessed.Finally, the study evaluated whether these parameters arecomparable to the use of metallic fixation in this injury.
Materials and Methods
Patient data was accessed from a database consisting ofLisfranc injuries from a single surgeon’s practice. Duringthe study time period (1999 through 2003), 64 patients wereidentified with Lisfranc’s injuries. Sixteen patients had re-duction of a diastasis between the first and second metatar-
sals and were evaluated. Inclusion criteria were as follows:, NUMBER 6, NOVEMBER/DECEMBER 2005 445

1) an acute traumatic injury to the tarsometatarsal regionresulting in diastasis � 3mm between the first and secondrays as noted on weight-bearing AP X-rays (Fig 1), and 2)a minimum postoperative follow-up of 1 year.
Diagnosis was made from clinical examination that in-cluded a stress test that demonstrated independent motion ofthe first and second metatarsals and forefoot abductionstress resulting in pain. Weight-bearing radiographs weretaken, and computed tomography (CT) evaluation was per-formed on most patients. CT scans were ordered whenpatients were unable to bear any weight, demonstrated lossof tendon function, had significant edema and ecchymosis,clinical disruption (malalignment) of the midfoot region, orsubtle incongruities at the involved joints. Indications forsurgery were � 3mm widening (diastasis) between the firstand second metatarsal bases, and � 2mm of subluxation ofa metatarsal base from its corresponding tarsal bone.
FIGURE 1 Preoperative weight-bearing AP radiograph.
Pre- and postoperative evaluations using the American
446 THE JOURNAL OF FOOT & ANKLE SURGERY
Orthopedic Foot and Ankle Society’s (AOFAS) midfootscoring system were performed by a fellow who did notperform the surgery (7). The time from injury to diagnosiswas recorded. Note was taken of the need for any fixationremoval and any complication such as infection or abscesswith the absorbable fixation. Outcome was assessed utiliz-ing the following scale:
Excellent: Full return to activity, no pain, no degenerativechanges noted on radiographs, and no need for addi-tional fixation removal.
Good: Full return to activity, no pain, minimal degenerativechanges (joint narrowing, no lipping) noted on radio-graphs, and a potential need for fixation removal.
Fair: Limited return to activity due to pain, minimal degen-erative changes noted on radiographs, potential need forfixation removal.
Poor: Inability to return to activity due to pain, degenerativechanges noted on radiographs, and/or need for fixationremoval.
Statistical analysis, using the SyStat Package (Richmond,CA), was performed to compare return to activity times inmales versus females, and pre- versus postoperative AO-FAS scores using the Student’s t-test. Return to activity wasdefined as the time it took for patients to resume their usualdaily routine including sports. The Fisher’s exact test wasutilized to determine whether a delay in diagnosis of 6weeks or more had a significant impact on rating scores.Statistical significance was set at P � .05.
Surgical Procedure
The surgical procedure was performed under radio-graphic control. The medial cuneiform was identified, andan overlying percutaneous incision was created. The fore-foot was reduced by a squeezing maneuver with a largetowel or bone clamp, narrowing the diastasis. A 2.7 drill bitwas directed from the medial cuneiform, in the trajectory ofthe Lisfranc ligament and advanced into the second meta-tarsal base. This was verified with intraoperative imaging,and then the medial cuneiform was overdrilled with a3.5mm drill bit. Subsequently a 3.5mm bioabsorbablepoly-L Lactic Acid (PLLA) cortical screw was insertedwhile reduction was maintained. Additional bioabsorbablefixation was utilized to stabilize other joints when needed,including the first metatarsocuneiform and intercuneiformarticulations, similar to the technique used with metallicscrews (1–3, 5, 6). The protruding screw heads are reducedwith a saw, burr, or hand-held cautery.
Postoperatively, patients were kept non–weight bearingin a below-knee cast boot for 4 weeks, partial weightbearing for 2 weeks in the boot, and then were allowed to be
fully weight bearing in the boot until 10 weeks postopera-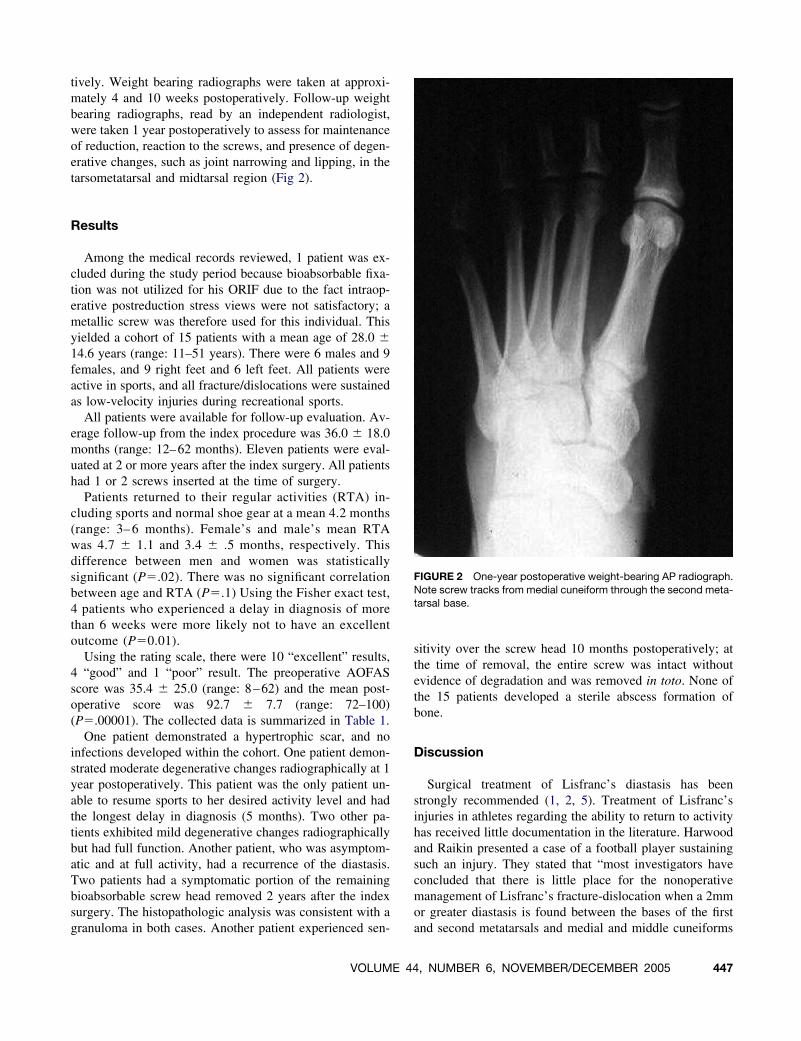
tively. Weight bearing radiographs were taken at approxi-mately 4 and 10 weeks postoperatively. Follow-up weightbearing radiographs, read by an independent radiologist,were taken 1 year postoperatively to assess for maintenanceof reduction, reaction to the screws, and presence of degen-erative changes, such as joint narrowing and lipping, in thetarsometatarsal and midtarsal region (Fig 2).
Results
Among the medical records reviewed, 1 patient was ex-cluded during the study period because bioabsorbable fixa-tion was not utilized for his ORIF due to the fact intraop-erative postreduction stress views were not satisfactory; ametallic screw was therefore used for this individual. Thisyielded a cohort of 15 patients with a mean age of 28.0 �14.6 years (range: 11–51 years). There were 6 males and 9females, and 9 right feet and 6 left feet. All patients wereactive in sports, and all fracture/dislocations were sustainedas low-velocity injuries during recreational sports.
All patients were available for follow-up evaluation. Av-erage follow-up from the index procedure was 36.0 � 18.0months (range: 12–62 months). Eleven patients were eval-uated at 2 or more years after the index surgery. All patientshad 1 or 2 screws inserted at the time of surgery.
Patients returned to their regular activities (RTA) in-cluding sports and normal shoe gear at a mean 4.2 months(range: 3– 6 months). Female’s and male’s mean RTAwas 4.7 � 1.1 and 3.4 � .5 months, respectively. Thisdifference between men and women was statisticallysignificant (P�.02). There was no significant correlationbetween age and RTA (P�.1) Using the Fisher exact test,4 patients who experienced a delay in diagnosis of morethan 6 weeks were more likely not to have an excellentoutcome (P�0.01).
Using the rating scale, there were 10 “excellent” results,4 “good” and 1 “poor” result. The preoperative AOFASscore was 35.4 � 25.0 (range: 8–62) and the mean post-operative score was 92.7 � 7.7 (range: 72–100)(P�.00001). The collected data is summarized in Table 1.
One patient demonstrated a hypertrophic scar, and noinfections developed within the cohort. One patient demon-strated moderate degenerative changes radiographically at 1year postoperatively. This patient was the only patient un-able to resume sports to her desired activity level and hadthe longest delay in diagnosis (5 months). Two other pa-tients exhibited mild degenerative changes radiographicallybut had full function. Another patient, who was asymptom-atic and at full activity, had a recurrence of the diastasis.Two patients had a symptomatic portion of the remainingbioabsorbable screw head removed 2 years after the indexsurgery. The histopathologic analysis was consistent with a
granuloma in both cases. Another patient experienced sen-VOLUME 44
sitivity over the screw head 10 months postoperatively; atthe time of removal, the entire screw was intact withoutevidence of degradation and was removed in toto. None ofthe 15 patients developed a sterile abscess formation ofbone.
Discussion
Surgical treatment of Lisfranc’s diastasis has beenstrongly recommended (1, 2, 5). Treatment of Lisfranc’sinjuries in athletes regarding the ability to return to activityhas received little documentation in the literature. Harwoodand Raikin presented a case of a football player sustainingsuch an injury. They stated that “most investigators haveconcluded that there is little place for the nonoperativemanagement of Lisfranc’s fracture-dislocation when a 2mmor greater diastasis is found between the bases of the first
FIGURE 2 One-year postoperative weight-bearing AP radiograph.Note screw tracks from medial cuneiform through the second meta-tarsal base.
and second metatarsals and medial and middle cuneiforms
, NUMBER 6, NOVEMBER/DECEMBER 2005 447

F of
because it is difficult to maintain anatomic reduction byclosed reduction and immobilization alone” (2).
Curtis et al. studied 19 athletes; 3 were unable to return tosports. On average, their patients had an RTA of 4.25months, similar to the patients in the current study (1). Theyalso found poor results in those whose diagnosis was de-layed. They utilized stress fluoroscopy to confirm the diag-nosis, but this diagnostic technique has been questioned byothers due to variability of force applied (3). Nunley andVertullo presented a retrospective study on 15 athleteswith metallic screw reduction in 8 patients. They utilizedweight-bearing radiographs and bone scans to diagnosethe Lisfranc’s injury. They reported 93% excellent resultswith a 27-month follow-up. Their entire cohort’s RTAwas just under 4 months (2). The size of the patientpopulation and results are quite similar to the findings inthe current study.
Bioabsorbable screws have been used successfully in footsurgery. Cicchinelli et al. reported the first use of PLLAscrews in foot surgery in both proximal osteotomies of thefirst metatarsal and hallux interphalangeal joint arthrodesis(8). They did not experience any untoward results. Bioab-sorbable screw fixation for Lisfranc’s injuries has also beenpreviously reported (6). The results of the current studyconcur with Thordarson and Hurvitz’s findings that bioab-sorbable fixation is acceptable for reducing Lisfranc’s inju-ries. They also utilized 2 screws with average follow-up was20 months. They found no loss of reduction, soft-tissuereaction, osteolysis, or need for screw removal (6). With themean 3-year follow-up presented here, 3 of 15 patientsdeveloped symptomatic screws/granulomas, 1 had degener-ative changes and another had a loss of reduction. Thordar-
TABLE 1 Results
Patient XRAYChange
Age Sex Diagnosis R/L Joints ORIF
1 15 F Sprain R 1 & 2, 2TMT S2 16 F Sprain R 1 & 2, 2TMT G3 DJD 17 F Sprain R 1 & 2, 1TMT S4 43 F Sprain R 1 & 2 B5 14 F Sprain L 1 & 2, 2TMT R6 16 F Sprain R 1 & 2 S7 28 F Fx/Dislocation L 1 & 2, 2TMT M8 51 F Sprain L 1 & 2 W9 DJD 50 F Fx/Dislocation R 1 & 2, 2TMT H10 24 M Fx/Dislocation L 1 & 2 M11 Widened 37 M Sprain L 1 & 2, 2TMT S12 DJD 16 M Sprain R 1 & 2, 1TMT F13 49 M Sprain R 1 & 2, 1TMT R14 11 M Dislocation L 1 & 2 M15 31 M Sprain R 1 & 2 VMean 28
RTA, return to activity; joints ORIF, open reduction internal fixation ometatarsal; 1 TMT, ORIF of first tarsal-metatarsal joint; 2 TMT, ORI
son and Hurvitz’ study on 14 patients did not have a control
448 THE JOURNAL OF FOOT & ANKLE SURGERY
group nor was it randomized, which is also a weakness ofthe current study.
All Lisfranc’s injury studies evaluating athletes requiredmetallic screw removal at 10 or more weeks postoperatively(1–3). However, the use of bioabsorbable screws in thisstudy (despite reduction of the screw heads) did not entirelyobviate the need for additional screw removal surgery.
Granulomas following bioabsorbable fixation have beendocumented previously. They often occur in a delayed fash-ion, up to 4 years’ post-implantation with PLLA screws (9,10). Bucholz et al. observed one inflammatory reaction in83 patients, with an average follow-up of 37 months afterORIF of a medial malleolar fracture (11). Rokkanen et al.reported a 0.4% incidence of sinus tract formation in afollow-up of 264 operations with the PLLA material (12).A longer postoperative follow-up of the patients in thecurrent study may reveal additional granuloma forma-tions.
The assessment tools used in this study may not be ideal.The AOFAS score can create a significantly low preopera-tive score in an acutely traumatized patient, potentiallyyielding a “0.” Even a low postoperative score can be asignificant improvement from a low preoperative score, yetthe clinical outcome is unfavorable. Also, the outcomeassessment scale created for this study is subjective andarbitrary, based on the author’s evaluation. Long-term se-quelae of the operative treatment of Lisfranc’s region re-quire further study as some authors recommend primaryarthrodesis (5, 13, 14). Further study is also needed toevaluate whether athletes undergoing ORIF are able tocontinue their activity level in the long term and if addi-
ivity RTA Outcome Pre-OpScore
Post-OpScore
FinalOutcome
er 6 Good, keloid 54 85 Goodastics 3 Excellent 8 100 Excellent
er 6 Poor, pain 59 72 Poortball 6 Good, screw removal 59 100 Good
ing 3.5 Excellent 62 100 Excellenter 5 Good, screw removal 62 90 Good
4 Excellent 8 97 Excellentng 4.5 Excellent 59 97 Excellent
4 Excellent 12 90 Excellentrcycle 3 Excellent 12 90 Excellenter 3 Excellent 54 90 Excellentall 4 Good, screw removal 54 90 Goodetball 3 Excellent 8 100 Excellent
4 Excellent 8 100 Excellentball 3.5 Excellent 12 90 Excellent
4.2 35.4 92.7
lved joints; 1 & 2, diastasis screw between first cuneiform & secondsecond tarsal-metatarsal joint.
Act
occymnoccaskeunnoccultialkiikingotooccootbaquultiolley
f invo
tional treatment is needed.

Conclusion
Fifteen athletic patients who sustained low-velocity inju-ries to the Lisfranc’s articulation underwent ORIF of thediastasis with 3.5mm bioabsorbable PLLA screws. Fourteenpatients returned to activities including sports at a mean 4.2months postoperatively. A delay in diagnosis of 6 weeks ormore was significantly more likely to yield a less-than-excellent result. Three patients necessitated screw removaldue to granuloma formation and symptomatic screw heads.Therefore, use of PLLA screws for Lisfranc’s ORIF isacceptable at maintaining reduction but does not necessarilyobviate the need for a second surgery for “hardware” re-moval.
References
1. Curtis M, Myerson M, Szura B. Tarsometatarsal joint injuries in theathlete. Am J Sports Med 21(4):497–502, 1993.
2. Harwood M, Raikin S. A Lisfranc fracture dislocaton in a footballplayer. J Am Board Fam Pract 16(1):69–72, 2003.
3. Nunley J, Vertullo C. Classification, investigation and management ofmidfoot sprains: Lisfranc injuries in the athlete. Am J Sports Med30:871–878, 2002.
4. DeLee JC. Traumatic fractures and dislocations. In: The Foot andAnkle in Sport, 1st ed, p 107, edited by Donald Baxter, Mosby, St.
Louis, 1995.VOLUME 44
5. Kuo R, Tejwani N, DiGiovanni C, Holt S, Bernischke S, Hansen S,Sangeorzan B. Outcome after open reduction and internal fixation ofLisFranc joint injuries. J Bone Joint Surg 82-A:1609–1618, 2000.
6. Thordarson DB, Hurvitz G. PLA screw fixation of Lisfranc injuries.Foot Ankle Int 23:1003–1007, 2002.
7. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS,Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot,hallux, and lesser toes. Foot Ankle Int 15:349–353, 1994.
8. Cicchinelli L, Gonzalez San Juan M, Aycart Testa J. Current conceptsof absorbable fixation in first ray surgery. Clin Podiatr Med Surg13:533–547, 1996.
9. Bergsma JE, de Bruijn WC, Rozema FR, Bos RR, Boering G. Latedegradation tissue response to poly(L-lactide) bone plates and screws.Biomaterials 16:25–31, 1995.
10. Partio EK. Absorbable screws in the fixation of cancellous bonefractures and arthrodesis. A clinical study of 318 patients (disserta-tion). Dept. of Orthopedics and Traumatology, Helsinki UniversityCentral Hospital, Helsinki, 1992.
11. Bucholz RW, Henry S, Henley MB. Fixation with bioabsorbablescrews for the treatment of fractures of the ankle. J Bone Joint SurgAm 76:319–324, 1994.
12. Rokkanen P, Bostman O, Makela M et al. Secondary infections withsinus formation when using absorbable implants in orthopedics (ab-stract). European Congress on Bone and Joint Infections, MunichOctober, 1993.
13. Mulier T, Reynders P, Dereymacker G, Broos P. Severe Lisfranc’sinjuries: primary arthrodesis or ORIF? Foot Ankle Int 23(10):902–905,2002.
14. Bonnel F, Barthelemy M. Injuries of Lisfranc’s joint: severe sprains,dislocations, fractures. Study of 39 personal cases and biomechanical
classification. J Chir 111(5-6):573–592, 1976., NUMBER 6, NOVEMBER/DECEMBER 2005 449