biosimilars in rheumatoid cme arthritis: what does a changing...
TRANSCRIPT

Leonard H. Calabrese, DOCleveland Clinic Lerner College of Medicine of Case Western Reserve UniversityCleveland, Ohio
Course Director
Participate in interactive questions, download activity slides, and obtain your instant CME credit online.
This CME activity is jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
CME
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
What’s Inside
3
7
Biosimilars: A Foundational Overview
A Closer Look at the Current Biosimilar Landscape in Rheumatoid Arthritis
www.peerviewpress.com/AKG900

2 Go online to complete the post-test and evaluation for CME credit
Activity Information
Activity Description and Educational ObjectivesIn this activity, an expert in rheumatoid arthritis discusses the role of biosimilars in the management of this disease.
Upon completion of this activity, participants should be better able to:• Recognize similarities and differences of biosimilars relative to their
biological reference agents based on structure, regulation, and clinical properties
• Identify current safety and efficacy data regarding the use of biosimilars in rheumatoid arthritis
• Apply biosimilars into the management of individual patients with rheumatoid arthritis in accordance with current evidence and expert recommendations
Target AudienceThis activity has been designed to meet the educational needs of rheumatologists and other clinicians involved in the treatment of patients with rheumatoid arthritis.
Requirements for Successful CompletionIn order to receive credit, participants must view the activity and complete the post-test and evaluation form. A score of 70% or higher is needed to obtain CME credit. There are no pre-requisites and there is no fee to participate in this activity or to receive CME credit. Statements of Credit are awarded upon successful completion of the post-test and evaluation form.
Media: Enduring MaterialRelease and Expiration Dates: May 05, 2017 - May 04, 2018Time to Complete: 30 minutes
Faculty & Disclosure / Conflict of Interest Policy Before the activity, all faculty and anyone who is in a position to have control over the content of this activity and their spouse/life partner will disclose the existence of any financial interest and/or relationship(s) they might have with any commercial interest producing healthcare goods/services to be discussed during their presentation(s): honoraria, expenses, grants, consulting roles, speakers bureau membership, stock ownership, or other special relationships. Presenters will inform participants of any off-label discussions. All identified conflicts of interest are thoroughly vetted by Medical Learning Institute, Inc. for fair balance, scientific objectivity of studies mentioned in the materials or used as the basis for content, and appropriateness of patient care recommendations.
The associates of Medical Learning Institute, Inc., the accredited provider for this activity, and PVI, PeerView Institute for Medical Education do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this CME activity during the past 12 months.
Course DirectorLeonard H. Calabrese, DOProfessor of MedicineRJ Fasenmyer Chair of Clinical ImmunologyCleveland Clinic Lerner College of Medicine of Case Western Reserve UniversityCleveland, Ohio
Leonard H. Calabrese, DO, has a financial interest/relationship or affiliation in the form of:Consultant for AbbVie Inc.; Amgen Inc.; Celgene Corporation; Genentech, Inc.; GlaxoSmithKline; Janssen Pharmaceuticals, Inc.; Pfizer Inc.; Regeneron Pharmaceuticals, Inc.; and UCB, Inc.Speakers Bureau participant with AbbVie Inc.; Amgen Inc.; Celgene Corporation; Genentech, Inc.; GlaxoSmithKline; Janssen Pharmaceuticals, Inc.; Pfizer Inc.; Regeneron Pharmaceuticals, Inc.; and UCB, Inc.
Leonard H. Calabrese, DO, does intend to discuss either non-FDA-approved or investigational use for the following products/devices: biosimilars under investigation in rheumatology.
CME ReviewerRavi Acharya, MD, FACRSanford Roumm & Acharya Arthritis CenterCamp Hill, Pennsylvania
Ravi Acharya, MD, FACR, has no financial interests/relationships or affiliations in relation to this activity.
Medical DirectorKate Nelson, PhDPVI, PeerView Institute for Medical Education
Kate Nelson, PhD, has no financial interests/relationships or affiliations in relation to this activity.
DisclaimerThe information provided at this CME activity is for continuing education purposes only and is not meant to substitute for the independent medical judgment of a healthcare provider relative to diagnostic and treatment options of a specific patient's medical condition. Recommendations for the use of particular therapeutic agents are based on the best available scientific evidence and current clinical guidelines. No bias towards or promotion for any agent discussed in this program should be inferred.
Providership, Credit & SupportThis activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education. The Medical Learning Institute, Inc. is accredited by the ACCME to provide continuing medical education for physicians.
The Medical Learning Institute, Inc. designates this enduring material for a maximum of 0.5 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
ProvidershipThis CME activity is jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
SupportThis activity is supported by an independent medical education grant from Sandoz Inc., a Novartis Division.
Disclosure of Unlabeled UseThe faculty of this educational activity may include discussions of products or devices that are not currently labeled for use by the FDA. Faculty members have been advised to disclose to the audience any reference to an unlabeled or investigational use.
No endorsement of unapproved products or uses is made or implied by coverage of these products or uses in our reports. No responsibility is taken for errors or omissions in reports.
Please refer to the official prescribing information for each product for discussion of approved indications, contraindications and warnings.
The materials presented here are used with the permission of the authors and/or other sources. These materials do not necessarily reflect the views of PeerView Press or any of its partners, providers, and/or supporters.
www.peerviewpress.com/AKG900

3
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
Dr. Calabrese: Hi. This is Dr. Len Calabrese from the Cleveland Clinic Lerner College of Medicine in Cleveland, Ohio. Welcome to this educational activity focused on the role of biosimilars in rheumatoid arthritis. After completing the activity, access the post-test and evaluation form by clicking the red “Get Certificate” button.
I really encourage you to download the slides, Practice Aids and any other features that you may be interested in. You can also share what you learn in this presentation with your colleagues. To post this presentation via Twitter, Facebook, LinkedIn, or e-mail, just select “Share This Presentation” from the menu in the upper left.
Biologic drugs have made a significant impact in thetreatment of RA and other inflammatory diseases1
These therapies specifically target key modulators of the inflammatory response, such as pro-inflammatory cytokines,
lymphocytes (eg, T or B cells), and cell surface receptors2
Although biologic therapies have demonstrated clinical efficacy, availability and patient access to these treatments may be limited,
which can impact patient outcomes3
Introduction
1. Scheinberg MA, Azevedo VF. Rheumatology (Oxford). 2014;53:389-390.2. Quan LD et al. Expert Opin Ther Pat. 2008;18:723-738.3. Desai RJ et al. J Manag Care Pharm. 2014;20:1110-1120.
Biologic drugs have made a dramatic impact on rheumatoid arthritis and other immune-mediated inflammatory diseases. These therapies specifically target key modulators in the integrated immune response. It can be either cytokines or cellular elements.
And although biologic therapies have demonstrated profound efficacy, raising the bar for therapy, the availability and patient access to these therapies may be limited because they're extremely expensive, and this can affect patient outcomes.
Biosimilars: A Foundational Overview
Biosimilars have been developed to provide these treatmentsto patients at a lower cost, once patents for the originator
biopharmaceutical have expired
Several biosimilars have been approved by regulatory agencies to treat RA and other inflammatory diseases
and are commercially available in many countries
Role of Biosimilars
There's a prevailing theme of this presentation and that is to provide these treatments to patients at lower cost, once patents come off of the original biopharmaceuticals. Biosimilars have now been developed; several biosimilars have been approved by regulatory agencies as of now to treat rheumatoid arthritis and other inflammatory conditions, and these are commercially available in many countries throughout the world.
Biosimilarity…“that the biological product is highly similar to the reference product notwithstanding minordifferences in clinically inactive components” and that “there are no clinically meaningful differences between the biological product andthe reference product in terms of the safety, purity,and potency of the product” (Section 351(i)of PHS Act)1
Generic
vs
Copy of a small-molecule (chemical) drug, which can be fully defined structurally and reproduced with an identical chemical structure2
• A biosimilar cannot be identical to the originator biologic2
– Biologic drugs are made in living cells, and the proprietary manufacturing processes are specialized and never fully disclosed by the manufacturer of the originator
What Is a Biosimilar?
1. http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm291128.pdf. Accessed April 7, 2017.2. Markenson J et al. Biologics. 2017;11:13-21.

4 Go online to complete the post-test and evaluation for CME credit
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
So, to start out, what is a biosimilar? Regulatory agencies have stated that the biologic product is highly similar to the reference product, notwithstanding minor differences in clinically inactive components. That means that it's really not a carbon copy, but it's highly similar. And there is some additional wording that talks about safety, purity, and potency of the product being variables that are important to compare and contrast. This is in contrast to generics, which are literally carbon copies of an originator compound.
Cloning Into DNA Vector Transfer Into Host Cell,Expression, Screening/Selection
Different cellexpression system
PurifiedBulk Drug
Probably differentvector
Possibly samegene sequence
Target DNA
SourceDNA
Cloning and Protein Expression
Protein Production, Purification, and Validation
Cell Productionin Bioreactors
Characterizationand Stability
Recovery ThroughFiltration or
Centrifugation
PurificationThrough
Chromatography
CellExpansion
Different cell line,growth media,
bioreactor conditions
Differentoperatingconditions
Different bindingand
elution conditions
Different methods,reagents,
reference standards
Different cell line,growth media,
method of expansion
Manufacturing Process for Biologics (and Biosimilars)1
1. Mellstedt H et al. Ann Oncol. 2008;19:411-419.
So, I'd like to show you an overview here of what the process of creating a biologic looks like. It starts out by having source DNA that encodes the RNA to create a protein of a given biologic, an antibody, or an antireceptor of some sort. Then there is a long and laborious and very high-tech process of protein production, purification, and validation that actually goes into the packaging and production of a drug.
So if we compare the biosimilar process, first of all, it is possible to start out with the same genetic sequence, because this is public domain. But after that, much of this process is proprietary. The biosimilar producer will not have the exact same vector available. Even though they are grossly similar, they will be of different cell lines. And then in the manufacturing process, this all will be different, because this is proprietary. There will be different growth media, different incubators, different bioreactor conditions, all contributing to different elution, purification, and excipient addition. And finally, the packaging will be different.
Target binding;signal transduction,functional activity/
viability of cellsof relevance
EMA Guidelines
Structural analyses,functional assays
FDA Guidance
Receptor-bindingor cell-based assays
WHO Guidelines
Analytical invitro studies
Comparable PK, PD (if feasible),clinical efficacy,clinical safety
confirmation studies
PK and/or PD,immunogenicity
PK, PD, confirmatoryPK/PD, efficacy, safety
Clinicalstudies
May not requireanimal studies
(risk-based approach)a
Animal toxicityassessments,
animal PK and PDmeasures, animalimmunogenicityb
Relevant biologic/PDactivity, toxicity
Nonclinical invivo studies
Sufficient scientificevidence
(total evidence) must support
Sufficient scientificjustification required
Requires sensitive clinicaltest model, clinically relevantMOA and/or same receptor,no unique issues identified
in safety and immunogenicitystudies, and noninferiority
demonstrated in efficacy trial
Extrapolation
a If in vitro comparability is satisfactory and does not identify any factors that would block direct entry to humans. b Discussions between the FDA and the developer may potentially indicate that animal studies are not necessary.
Overview of Regulatory Requirements for Biosimilars1,2
1. Markenson J et al. Biologics. 2017;11:13-21.2. Socinski MA et al. MAbs. 2015;7:286-293.
The regulatory approval process of a biosimilar requires much, much more data than a generic small molecule. And here on this graph, we're showing three different regulatory agencies, the FDA in the middle; EMA, the European equivalent; and the WHO, all kind of providing this high-altitude guidance as to what type of analytics must be done, what type of nonclinical in vivo studies, whether or not animals studies are needed, what type of clinical studies, and then, finally, extrapolation, which has to do with the approved indications for these drugs.
Demonstration of biosimilarity
The EMA, FDA, and WHO guidelines have generally similarrequirements for approval of a biosimilar, including:
Provision that the recommendation for approval is based on the“totality of the evidence” for biosimilarity
Use of a stepwise approach to develop the evidence
Summary of Regulatory Requirements for Biosimilars1
1. Markenson J et al. Biologics. 2017;11:13-21.
So, in summary, the EMA, FDA, and WHO have laid out kind of a generally similar pathway for approval of a biosimilar. It's a stepwise approach to development, and the common threads throughout all of these is this phrase: the “totality of evidence” must demonstrate this fingerprint similarity between the biosimilar and the originator.
www.peerviewpress.com/AKG900
5
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
Physicochemicalcharacterization
Biologicalcharacterization
Preclinicalstudies
Clinicalstudies
Pharmaco-vigilance
PK, PD,safety, and
immunogenicityassessment
Phase 1 Phase 2/3
No
clin
ical
ly m
eani
ngfu
ldi
ffere
nces
dem
onst
rate
d
Efficacy, safety, and
immunogenicity assessment
No
clin
ical
ly m
eani
ngfu
ldi
ffere
nces
dem
onst
rate
d
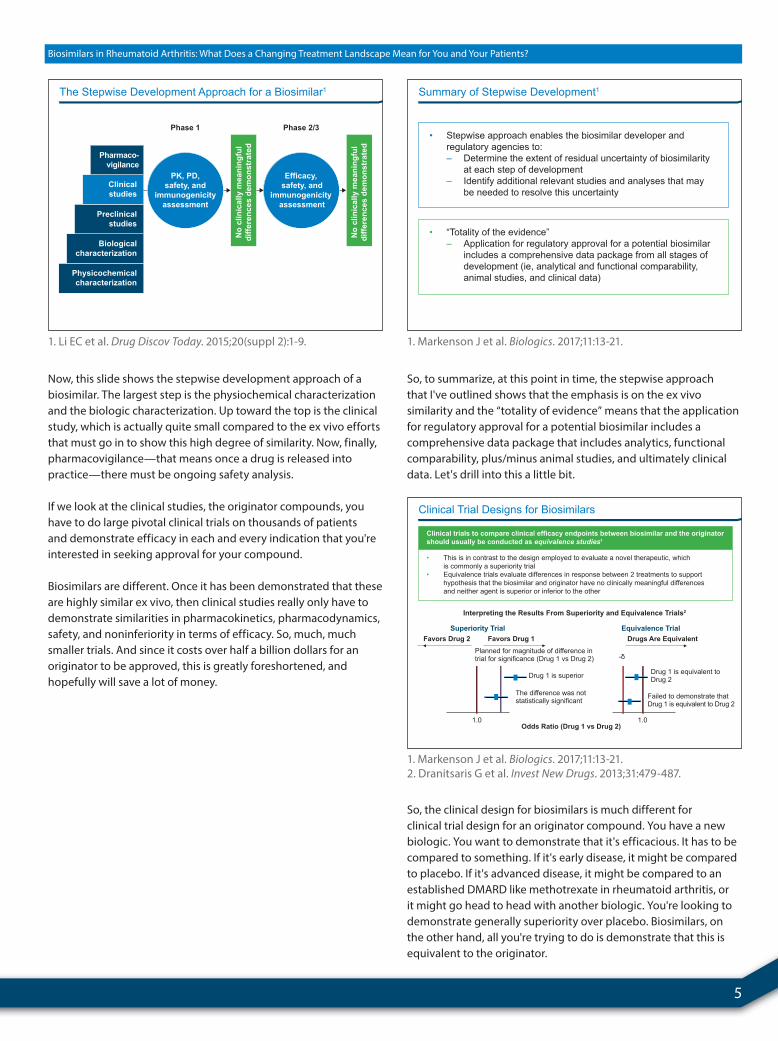
The Stepwise Development Approach for a Biosimilar1
1. Li EC et al. Drug Discov Today. 2015;20(suppl 2):1-9.
Now, this slide shows the stepwise development approach of a biosimilar. The largest step is the physiochemical characterization and the biologic characterization. Up toward the top is the clinical study, which is actually quite small compared to the ex vivo efforts that must go in to show this high degree of similarity. Now, finally, pharmacovigilance—that means once a drug is released into practice—there must be ongoing safety analysis.
If we look at the clinical studies, the originator compounds, you have to do large pivotal clinical trials on thousands of patients and demonstrate efficacy in each and every indication that you're interested in seeking approval for your compound.
Biosimilars are different. Once it has been demonstrated that these are highly similar ex vivo, then clinical studies really only have to demonstrate similarities in pharmacokinetics, pharmacodynamics, safety, and noninferiority in terms of efficacy. So, much, much smaller trials. And since it costs over half a billion dollars for an originator to be approved, this is greatly foreshortened, and hopefully will save a lot of money.
• Stepwise approach enables the biosimilar developer and regulatory agencies to: – Determine the extent of residual uncertainty of biosimilarity at each step of development – Identify additional relevant studies and analyses that may be needed to resolve this uncertainty
• “Totality of the evidence” – Application for regulatory approval for a potential biosimilar includes a comprehensive data package from all stages of development (ie, analytical and functional comparability, animal studies, and clinical data)
Summary of Stepwise Development1
1. Markenson J et al. Biologics. 2017;11:13-21.
So, to summarize, at this point in time, the stepwise approach that I've outlined shows that the emphasis is on the ex vivo similarity and the “totality of evidence” means that the application for regulatory approval for a potential biosimilar includes a comprehensive data package that includes analytics, functional comparability, plus/minus animal studies, and ultimately clinical data. Let's drill into this a little bit.
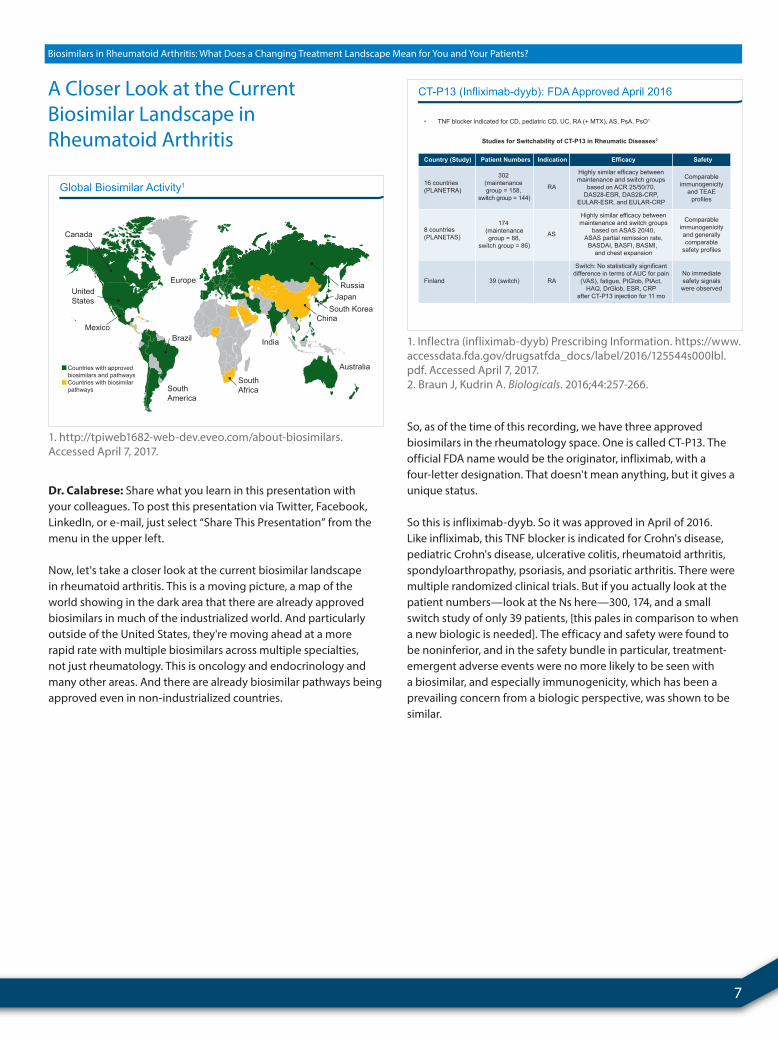
• This is in contrast to the design employed to evaluate a novel therapeutic, which is commonly a superiority trial• Equivalence trials evaluate differences in response between 2 treatments to support hypothesis that the biosimilar and originator have no clinically meaningful differences and neither agent is superior or inferior to the other
Clinical trials to compare clinical efficacy endpoints between biosimilar and the originatorshould usually be conducted as equivalence studies1
Interpreting the Results From Superiority and Equivalence Trials2
Superiority Trial Equivalence Trial
Planned for magnitude of difference in trial for significance (Drug 1 vs Drug 2)
Favors Drug 2 Favors Drug 1 Drugs Are Equivalent
Drug 1 is equivalent to Drug 2
Failed to demonstrate that Drug 1 is equivalent to Drug 2
Drug 1 is superior
The difference was not statistically significant
Odds Ratio (Drug 1 vs Drug 2)
-
1.0 1.0
Clinical Trial Designs for Biosimilars
1. Markenson J et al. Biologics. 2017;11:13-21.2. Dranitsaris G et al. Invest New Drugs. 2013;31:479-487.
So, the clinical design for biosimilars is much different for clinical trial design for an originator compound. You have a new biologic. You want to demonstrate that it's efficacious. It has to be compared to something. If it's early disease, it might be compared to placebo. If it's advanced disease, it might be compared to an established DMARD like methotrexate in rheumatoid arthritis, or it might go head to head with another biologic. You're looking to demonstrate generally superiority over placebo. Biosimilars, on the other hand, all you're trying to do is demonstrate that this is equivalent to the originator.

6 Go online to complete the post-test and evaluation for CME credit
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
You can see the design on the left of a superiority trial, where the degree of clinical improvement must be superior. On the opposite side, the equivalence trial demonstrates that you establish a preset window of therapeutic equivalence, and it must reside within that window to be deemed equivalent. And we're not looking to make this better, and we're not looking to make this worse. We're looking statistically to achieve the endpoint of equivalence.
• Noninferiority studies – Evaluate whether a biosimilar is not clinically inferior to the originator (thus, using only one margin) – May be employed for assessment of biosimilars if the study population and endpoint(s) are appropriate and sufficient scientific justification is provided1
“A sponsor should provide adequate scientific justification for thechoice of study design, study population, study endpoint(s), estimated effect size for the reference product, and margin(s)(how much difference to rule out). Sponsors should discuss theirstudy proposal(s) and overall clinical development plan with FDAbefore initiating the comparative clinical study(ies).”
Current FDA Guidance2
Clinical Trial Designs for Biosimilars (Cont’d)
1. Markenson J et al. Biologics. 2017;11:13-21.2. https://www.fda.gov/downloads/drugs/guidances/ucm291128.pdf. Accessed April 7, 2017.
So, the overall clinical design for biosimilars includes noninferiority studies, which must show that the therapeutic endpoint is not inferior to the originator.
• The FDA states that with sufficient scientific justification, the potential exists for a biosimilar to be approved for ≥1 conditions of use for which the reference product is approved based on extrapolation of data1
Biosimilarity has been clinically confirmed in a key indication
Extrapolation of efficacy and safety data to otherindications may be possible if1-3:
A shared MOA for each indication has been shown betweenthe reference product and the biosimilar
Extrapolation of Indications for Biosimilars
1. https://www.fda.gov/downloads/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/approvalapplications/therapeuticbiologicapplications/biosimilars/ucm428732.pdf. Accessed April 7, 2017.2. Weise M et al. Blood. 2012;120:5111-5117. 3. McCamish M, Woollett G. Clin Pharmacol Ther. 2012;91:405-417.
The next concept is extrapolation. Say you are making an originator compound. You have a new biologic coming out, and you think it's going to work something like a TNF inhibitor. For this to reach the marketplace, you think that your drug will be effective in psoriasis, psoriatic arthritis, rheumatoid arthritis, maybe inflammatory bowel disease. You're obligated to do clinical trials in each and every one of these diseases to apply for approval from the FDA.
Extrapolation in the biosimilar [approval] pathway is a concept that if you demonstrate equivalence to a single approved indication, then by extrapolation, you will be granted approval for use in any disease that the originator is approved for. This is of profound cost savings in drug development since you don't have to do multiple clinical trials. If I have a biosimilar TNF, and I can show it's effective in rheumatoid [arthritis], and that originator is approved for IBD, psoriasis, spondylitis, JIA, you can in one fell swoop reach by extrapolation multiple approved indications.
I would encourage you to tell your colleagues about this program. Just select “Share This Presentation” from the menu in the upper left, and they'll be able to join in this learning experience. Thank you.
www.peerviewpress.com/AKG900
7
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
Canada
UnitedStates
Mexico
SouthAfrica
India
Australia
China
JapanRussia
Countries with approvedbiosimilars and pathwaysCountries with biosimilarpathways
South Korea
Europe
Brazil
SouthAmerica
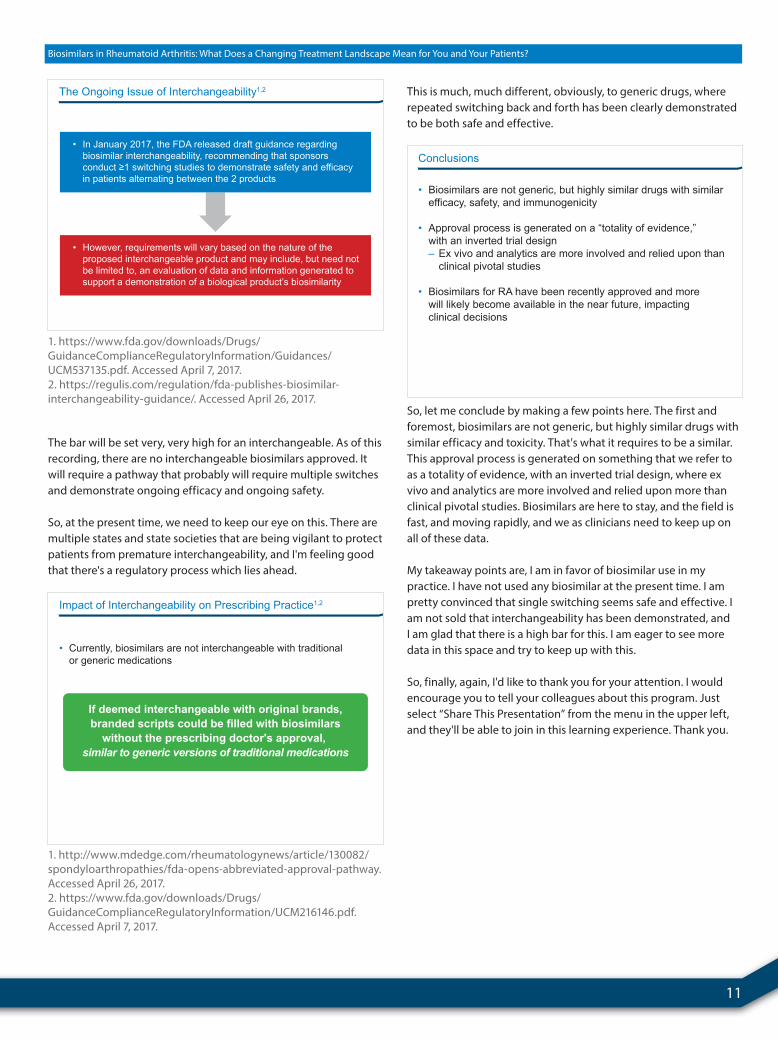
Global Biosimilar Activity1
1. http://tpiweb1682-web-dev.eveo.com/about-biosimilars. Accessed April 7, 2017.
Dr. Calabrese: Share what you learn in this presentation with your colleagues. To post this presentation via Twitter, Facebook, LinkedIn, or e-mail, just select “Share This Presentation” from the menu in the upper left.
Now, let's take a closer look at the current biosimilar landscape in rheumatoid arthritis. This is a moving picture, a map of the world showing in the dark area that there are already approved biosimilars in much of the industrialized world. And particularly outside of the United States, they're moving ahead at a more rapid rate with multiple biosimilars across multiple specialties, not just rheumatology. This is oncology and endocrinology and many other areas. And there are already biosimilar pathways being approved even in non-industrialized countries.
A Closer Look at the Current Biosimilar Landscape in Rheumatoid Arthritis
302 (maintenance group = 158,
switch group = 144)
Patient Numbers
Comparableimmunogenicity
and TEAEprofiles
SafetyCountry (Study)
RA
Indication
Studies for Switchability of CT-P13 in Rheumatic Diseases2
Highly similar efficacy betweenmaintenance and switch groups
based on ACR 25/50/70,DAS28-ESR, DAS28-CRP,
EULAR-ESR, and EULAR-CRP
Efficacy
16 countries(PLANETRA)
• TNF blocker indicated for CD, pediatric CD, UC, RA (+ MTX), AS, PsA, PsO1
174 (maintenancegroup = 88,
switch group = 86)
Comparableimmunogenicityand generallycomparable
safety profiles
AS
Highly similar efficacy betweenmaintenance and switch groups
based on ASAS 20/40,ASAS partial remission rate,
BASDAI, BASFI, BASMI, and chest expansion
8 countries(PLANETAS)
39 (switch)No immediatesafety signalswere observed
RA
Switch: No statistically significantdifference in terms of AUC for pain
(VAS), fatigue, PtGlob, PtAct,HAQ, DrGlob, ESR, CRP
after CT-P13 injection for 11 mo
Finland
CT-P13 (Infliximab-dyyb): FDA Approved April 2016
1. Inflectra (infliximab-dyyb) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/125544s000lbl.pdf. Accessed April 7, 2017.2. Braun J, Kudrin A. Biologicals. 2016;44:257-266.
So, as of the time of this recording, we have three approvedbiosimilars in the rheumatology space. One is called CT-P13. Theofficial FDA name would be the originator, infliximab, with afour-letter designation. That doesn't mean anything, but it gives aunique status.
So this is infliximab-dyyb. So it was approved in April of 2016. Like infliximab, this TNF blocker is indicated for Crohn's disease, pediatric Crohn's disease, ulcerative colitis, rheumatoid arthritis, spondyloarthropathy, psoriasis, and psoriatic arthritis. There were multiple randomized clinical trials. But if you actually look at the patient numbers—look at the Ns here—300, 174, and a small switch study of only 39 patients, [this pales in comparison to when a new biologic is needed]. The efficacy and safety were found to be noninferior, and in the safety bundle in particular, treatment-emergent adverse events were no more likely to be seen with a biosimilar, and especially immunogenicity, which has been a prevailing concern from a biologic perspective, was shown to be similar.

8 Go online to complete the post-test and evaluation for CME credit
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
Norway
Country
500
Patients, N
RA, SpA, PsA, UC, CD, and PsO
Indication
RCT (NCT02148640)
Study Type(ClinicalTrials.gov
Identifier)Study
NOR-SWITCHstudy
19 countries 214 CD RCT (NCT02096861)CD switchingstudy
Japan ~100 RA RCTRA switchingstudy
7 countries 2,450 RA RegistryRA registry inKorea, EU
9 countries — IBD (CD, UC) RegistryIBD registry inKorea, EU
5 countries — AS RegistryAS registry inKorea, EU
Korea 1,600 RA, AS, IBD, PsA, PsO Post-marketing studyPost-marketingstudy in Korea
UK 500 RA RegistryBSRBR
Germany 500 RA RegistryRABBIT
CT-P13: Ongoing Registries and Post-Marketing Studies1
1. Braun J, Kudrin A. Biologicals. 2016;44:257-266.
These are some additional ongoing registries and postmarketing studies which have added to the database of this biosimilar. In particular, the NOR-SWITCH study, which I'll mention again, is a widely quoted study. The remainder of these registration studies are basically looking at ongoing treatment-emergent issues that may be of concern, and thus far none have been found.
R, DB, 2-way
crossover
DesignStudy ID
Clinical Pharmacology Studies
Comparative Clinical StudyA cross-study comparison of studies 101 and 102
Study 101 PK, safety,immunogenicity
Objectives
57 healthysubjects
Subjects
SD 50 mg SubQ:• GP2015• EU-Etanercept
Treatments
Cmax, AUCt, andAUCinf
R, DB, 2-way
crossoverStudy 104 PK, safety,
immunogenicity54 healthy
male subjects
SD 50 mg SubQ:• GP2015• EU-Etanercept
Cmax, AUCt, andAUCinf
R, DB, 2-way
crossoverStudy 102
Report 105
PK, safety,immunogenicity
54 healthysubjects
SD 50 mg SubQ:• GP2015• US-Etanercept
Cmax, AUCt, andAUCinf
R, DB, PGTP1
(Wk 0-12)
Study 302
Efficacy, safety,immunogenicity,
PK
531 PsOpatients
50 mg SubQ twice-weekly:• GP2015• EU-Etanercept
PASI 75
R, DB, PGTP2
(switching)(Wk 12-30)
Safety,immunogenicity,
PK
PsO patientsre-randomized
50 mg SubQ QW:• GP2015 cont• GP2015 switch• EU-Etanercept cont• EU-Etanercept switch
Safety,immunogenicity
Endpoints
Key Design Features of GP2015 Clinical Studies2
• TNF blocker indicated for RA, polyarticular JIA, PsA, AS, PsO1
GP2015 (Etanercept-szzs): FDA Approved August 2016
1. Erelzi (etanercept-szzs) Prescribing Information. www.erelzi.com/globalassets/erelzi/erelzipi.pdf. Accessed April 7, 2017.2. https://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ArthritisAdvisoryCommittee/UCM510493.pdf. Accessed April 7, 2017.
A second approved biologic is a biosimilar etanercept-szzs. So it was approved in August of 2016. And similar to etanercept, it has broad approval in JIA, PsA, AS, and psoriasis, in addition to rheumatoid arthritis. There are three studies which examined basically [PK], safety, and immunogenicity—very small studies with just a few score of patients. And then a pivotal study—Study 302, with over 500 patients—done in psoriasis.
• As the 95% CI was contained within the prespecified interval (-18 to 18%), this result demonstrated therapeutic equivalence between GP2015 and ETN• Antidrug antibodies (all non-neutralizing) were limited to 5 patients on ETN during treatment period 1, and 1 patient in the switched ETN group, who had been treated with GP2015 for 12 weeks at the time of the finding• No clinically meaningful differences in safety observed up to 52 weeks of treatment• Safety profiles of GP2015 and ETN were similar to those observed in previous ETN studies
0
20
40
60
80
100
Per Protocol Set
75.773.4
-2.3% (-9.85, 5.30)
Adj
uste
d PA
SI 7
5 R
espo
nse
Rat
e at
Wee
k 12
, %
GP2015 (n = 239) ETN (n = 241)
PASI 75 (Primary Endpoint) of GP2015 in EGALITY,Phase 3 PsO Trial1
1. Griffiths C et al. Br J Dermatol. 2017;176:928-938.
And because it was noninferior in psoriasis, with an endpoint of a PASI-75, this is highly similar—not identical, but certainly noninferior by biostatistical standards—it was granted extrapolation for the other indications of etanercept. Also in this study, the safety was a major endpoint, and there was no difference in treatment-emergent adverse events leading to discontinuation.
R, PG, SD, 3-way PKbridging
DesignStudy(DatesConducted)
PK Similarity Study
20110217(07/12-10/12)
3-way PKsimilarity, safety,immunogenicity
Objectives
203 healthysubjects
Subjects
40 mg SubQ:• ABP 501• US-Adalimumab• EU-Adalimumab
26 week,R, DB, PG
Comparative Clinical Studies
Efficacy, safety,immunogenicity
in RA
526 patientswith RA
40 mg SubQ Q2W +MTX:• ABP 501• US-Adalimumab
Treatments
Key Design Features of ABP 501 Clinical Studies2
• TNF blocker indicated for RA, JIA, PsA, AS, CD, UC, PsO1
20120262(10/13-11/14)
R, DB, PGRe-randomized at week 16 to either
continue EU-adalimumab or
transition toABP 501
Efficacy, safety,immunogenicity
in PsO350 patients
with PsO
80 mg SubQ day 1,then 40 mg SubQ Q2Wfrom week 2:• ABP 501• EU-Adalimumab
20120263(10/13-03/15)
ABP 501 (Adalimumab-atto): FDA Approved September 2016
1. Amjevita (adalimumab-atto) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/761024lbl.pdf. Accessed April 7, 2017. 2. https://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ArthritisAdvisoryCommittee/UCM510293.pdf. Accessed April 7, 2017.
The third currently approved biosimilar was approved in September of 2016. This is biosimilar adalimumab, known as “-atto.” It is a TNF blocker, which has broad approval indications of RA, JIA, psoriasis, psoriatic arthritis, and a spectrum of spondyloarthritis and inflammatory bowel disease.
www.peerviewpress.com/AKG900

9
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
This is a summary of the clinical database—again, a relatively small study of healthy subjects which established PK and immunogenicity. And then the comparator clinical trials, which looked at two diseases, RA and psoriasis, [with] varying doses based upon what is used with the originator compound.
• Similar PK• Equivalent efficacy and similar safety and immunogenicity
ClinicalConfirmation
Similar efficacy• RA 6-month study• PsO 1-year study
Similar safety• RA – with MTX• PsO – without MTX
Similar immunogenicity• RA and PsO• PsO includes transition to ABP 501
ABP 501 Versus Adalimumab1-5
1. https://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ArthritisAdvisoryCommittee/UCM511900.pdf. Accessed April 7, 2017.2. Kaur P et al. Ann Rheum Dis. 2017;76:526-533. 3. Papp K et al. J Am Acad Dermatol. 2017 Mar 10 [Epub ahead of print].4. Cohen S et al. 2015 American College of Rheumatology/ Association of Rheumatology Health Professionals Annual Meeting (ACR/ARHP 2015). Abstract 2054.5. Strober B et al. J Am Acad Dermatol. 2016;74(5 suppl 1):AB249.
And again, a summary of these data showed similar PK and the clinical studies next showed similar efficacy in rheumatoid arthritis after 6 months, similar efficacy in psoriasis after 1 year. And in these larger clinical studies, similar immunogenicity and similar safety. So, equivalent efficacy, safety, and immunogenicity, leading (via extrapolation) to approval.
• Avasthagen• Biocon• BioXpress• CHS-0214 (Coherus)• LBEC010 (LG Life)• PRX-106 (Protalix)• SB4 (Samsung Bioepis)• ENIA11 (Mycenex)
• BI • Biocon • BioXpress• CHS-1420 (Coherus)• BOW050 (Epirus) • FKB327 (Kyowa Kirin)
• GP2017 (Sandoz)• Harvest Moon• LBAL (LG Life)• M923 (Momental)• Oncobiologics • PF-06410293 (Pfizer)• SB5 (Samsung)
• ABP 798 (Amgen)• AP052 (Aprogen)• BI 695500 (BI)• BioXpress• CT-P10 (Celltrion)• GP2013 (Sandoz)• Harvest Moon
• MabionCD20 (Mabion)• MK-8808 (Merck)• PF-05280586 (Pfizer)
• ABP 710 (Amgen)• BioXpress• BOW15 (Epirus)• GP2018 (Sandoz) • GP1111 (Sandoz)
Infliximab
Rituximab
Etanercept
Adalimumab
• GS071 (Aprogen) • Harvest Moon• NI-071 (Nichiiko)• PF-0643B179 (Sandoz)• SB2a
(Samsung Bioepis)
a FDA approved in April 2017 for adult and pediatric CD, adult UC, RA, AS, PsA, and adult PsO.
Biosimilars in Development1
1. http://www.imshealth.com/files/web/IMSH%20Institute/
Healthcare%20Briefs/Documents/IMS_Institute_Biosimilar_Brief_March_2016.pdf. Accessed April 7, 2017.
This is a dizzying figure, which shows biosimilars in development. You can see that there are many, many biosimilars on the way which vary from preclinical trials to those that have already been filed. So, we as clinicians will have much to keep our eye on.
Switching
Substitution
Interchangeability
Pharmacovigilance
Extrapolation of indications
Cost
Patient preference
Practical Considerations Regarding the Use of Biosimilars in RA
Finally, some practical considerations regarding this. There is some terminology that we need to understand. A lot of this is switching, substitution, interchangeability, and the rest of these, I think, have face validity, and you recognize cost and patient preference.
• 52-week randomized, double-blind, noninferiority, phase 4 study• Patients receiving infliximab for ≥6 months were randomized to continue infliximab or switch to CT-P13
• Primary outcome: Disease worsening at 12 months – 95% CI of the adjusted treatment difference (-4.4%) was -12.7 to 3.9, which was within the prespecified noninferiority margin – Frequency of AEs, including infusion reactions, were also similar• Antidrug antibodies – Infliximab: 7.1% – CT-P13: 7.9%
0 10 20 30 40 50 60 70
All
a Other conditions were studied as well (ie, IBD, PsO).
Patie
nts
With
Dis
ease
Wor
seni
ng B
y C
ondi
tion,
%a
RA PsA SpA
Infliximab (n = 241) CT-P13 (n = 240)
NOR-SWITCH1
1. Løvik Goll G et al. ACR/ARHP 2016. Abstract 19L.
I referred to the NOR-SWITCH study previously. This was a large study, 52 weeks of patients receiving infliximab. Halfway, they were randomized to stay on branded infliximab or switch to the biosimilar. And the primary outcome was disease worsening at 12 months, and then immunogenicity was a secondary endpoint. And as you can see, virtually no difference in efficacy or immunogenicity, and this has been used as one of the most impressive studies that at least a single switch is possible.

10 Go online to complete the post-test and evaluation for CME credit
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
Anti-TNF products, 21%
Long-acting insulins,15%
mAb antineoplastics,13%
Fast-actinginsulins, 11%
CSFs, 6%
IFNs, 6%
Erythropoietinproducts, 6%
Ocular antivascularproducts, 3%
Growth hormones, 3%
Miscellaneousimmunosuppressants, 2%
Miscellaneous antirheumaticagents, 2%
Bone calcium regulators, 2%
Anti-PsO products, 1%Anti-asthma and COPD, 1%
All other classes, 2%
Immunostimulants(excluding IFNs), 5%
Potential Cost Savings Across Biologic Classes1
1. https://www.rand.org/content/dam/rand/pubs/perspectives/PE100/PE127/RAND_PE127.pdf. Accessed April 7, 2017.
What about cost? The cost factor, we hope, will increase patient access, at least in the at-large community. And that's a factor of driving drug prices down. Now, in Europe, where these drugs have been used for several years, the cost savings for the centralized healthcare systems have ranged from 30% to over 70%—over 70%—this is amazing. In the United States, which has this crazy, patchwork quilt of insurance, where we seem to be phobic about single-payer systems, as one would expect, thus far the cost savings have been far less than this.
Yet, many predict that we have yet to see maximal effects until there are multiple biosimilars available for each agent. This pie-gram shows where the potential savings may come as we look at the array of biologic originators currently in use.
Setting
Insurers
Self-AdministeredFrom Retail or
Mail-OrderPharmacy
++: Significant share of savings. +: Share of savings. +/-: Ambiguous. NA: not applicable.
++
InpatientFacilitySetting
+
OutpatientFacilitySetting
Physician-Administered
++
OfficeSetting
++
Facilities NA +/- +/- NA
Physicians NA NA +/- +/-
Patients ++ + + +
Where Will Biosimilar Cost Savings Accrue?1
1. https://www.rand.org/content/dam/rand/pubs/perspectives/PE100/PE127/RAND_PE127.pdf. Accessed April 7, 2017.
Where will biosimilar cost savings accrue? This is kind of a crystal ball at the present time. Most people are putting their money that it will be insurers, outpatient facilities, office settings—so they're physician-administered. Insurance companies will do well.
Patients? This remains to be seen. If I have a patient that tells me that there is a biosimilar that they have been told that they will get a rebate on if they switch to this, and there's no medical contraindications, I would be all for it. I have yet to see this in my practice at the present time.
SEC. 7002. Approval Pathway for Biosimilar Biological Products1
(a) Licensure of biological products as biosimilar or interchangeable. —Section 351 of the Public Health Service Act (42 U.S.C. 262) is amended— “The term ‘interchangeable’ or ‘interchangeability,’ in reference to a biological product that is shown to meet the standards described in subsection (k)(4), means that the biological product may be substituted for the reference product without the intervention of the health care provider who prescribed the reference product.”
• Patient transitioned to biosimilar after initial treatment with originator
Switch = Transition
Switching vs Substitution
Substitution = Interchange
Interchangeability
1. https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/UCM216146.pdf. Accessed April 7, 2017.
Lastly, interchangeability. Interchangeability means that a biosimilar can be substituted for the reference product by [someone] other than the clinician. That could be a pharmacist, it could be an insurance company. In other words, you lose control as a clinician of doing this. We all have concerns over this because down the pike here a few years, there may be four biosimilars for etanercept; what would be the consequences of switching from biosimilar 1 to biosimilar 3 to biosimilar 2 to biosimilar 4? We don't know.
www.peerviewpress.com/AKG900
11
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
• In January 2017, the FDA released draft guidance regarding biosimilar interchangeability, recommending that sponsors conduct ≥1 switching studies to demonstrate safety and efficacy in patients alternating between the 2 products
• However, requirements will vary based on the nature of the proposed interchangeable product and may include, but need not be limited to, an evaluation of data and information generated to support a demonstration of a biological product’s biosimilarity
The Ongoing Issue of Interchangeability1,2
1. https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM537135.pdf. Accessed April 7, 2017.2. https://regulis.com/regulation/fda-publishes-biosimilar-interchangeability-guidance/. Accessed April 26, 2017.
The bar will be set very, very high for an interchangeable. As of this recording, there are no interchangeable biosimilars approved. It will require a pathway that probably will require multiple switches and demonstrate ongoing efficacy and ongoing safety.
So, at the present time, we need to keep our eye on this. There are multiple states and state societies that are being vigilant to protect patients from premature interchangeability, and I'm feeling good that there's a regulatory process which lies ahead.
• Currently, biosimilars are not interchangeable with traditional or generic medications
If deemed interchangeable with original brands,branded scripts could be filled with biosimilars
without the prescribing doctor's approval, similar to generic versions of traditional medications
Impact of Interchangeability on Prescribing Practice1,2
1. http://www.mdedge.com/rheumatologynews/article/130082/spondyloarthropathies/fda-opens-abbreviated-approval-pathway. Accessed April 26, 2017.2. https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/UCM216146.pdf. Accessed April 7, 2017.
This is much, much different, obviously, to generic drugs, where repeated switching back and forth has been clearly demonstrated to be both safe and effective.
• Biosimilars are not generic, but highly similar drugs with similar efficacy, safety, and immunogenicity
• Approval process is generated on a “totality of evidence,” with an inverted trial design – Ex vivo and analytics are more involved and relied upon than clinical pivotal studies
• Biosimilars for RA have been recently approved and more will likely become available in the near future, impacting clinical decisions
Conclusions
So, let me conclude by making a few points here. The first and foremost, biosimilars are not generic, but highly similar drugs with similar efficacy and toxicity. That's what it requires to be a similar. This approval process is generated on something that we refer to as a totality of evidence, with an inverted trial design, where ex vivo and analytics are more involved and relied upon more than clinical pivotal studies. Biosimilars are here to stay, and the field is fast, and moving rapidly, and we as clinicians need to keep up on all of these data.
My takeaway points are, I am in favor of biosimilar use in my practice. I have not used any biosimilar at the present time. I am pretty convinced that single switching seems safe and effective. I am not sold that interchangeability has been demonstrated, and I am glad that there is a high bar for this. I am eager to see more data in this space and try to keep up with this.
So, finally, again, I'd like to thank you for your attention. I would encourage you to tell your colleagues about this program. Just select “Share This Presentation” from the menu in the upper left, and they'll be able to join in this learning experience. Thank you.

CME
Biosimilars in Rheumatoid Arthritis: What Does a Changing Treatment Landscape Mean for You and Your Patients?
www.peerviewpress.com/AKG900
Sign up for e-mail alerts on new clinical advances and educational activities in your specialty: www.peerviewpress.com/signup
Copyright © 2000-2017, PeerView Press
This CME activity is jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
This activity is supported by an independent medical education grant from Sandoz Inc., a Novartis Division.
PVI, PeerView Institute for Medical Education, and Medical Learning Institute, Inc. are responsible for the selection of this activity's topics, the preparation of editorial content, and the distribution of this activity. The preparation of PeerView activities is supported by educational grants subject to written agreements that clearly stipulate and enforce the editorial independence of PVI and Medical Learning Institute, Inc. Our activities may contain references to unapproved products or uses of these products in certain jurisdictions. For approved prescribing information, please consult the manufacturer's product labeling. No endorsement of unapproved products or uses is made or implied by coverage of these products or uses in our activities. No responsibility is taken for errors or omissions in activities.
New and improved sourcefor free CME/CE