birthing through first nations midwifery care
DESCRIPTION
This short paper was commissioned by the First Nations Centre, National Aboriginal HealthOrganization to focus exclusively on First Nations issues in midwifery, to provide a more in-depth yetinspiring background for consideration by people considering midwifery as a career, or for developmentof midwifery programs in or near First Nations communities.TRANSCRIPT
Birthing Through First Nations Midwifery Care
Book title: Birthing Through First Nations Midwifery Care
© Copyright 2009 National Aboriginal Health Organization
ISBN: 978-1-926543-24-6
Date Published: October 2009
OAAPH [now known as the National Aboriginal Health Organization (NAHO)] receivesfunding from Health Canada to assist it to undertake knowledge based activities includingeducation, research and dissemination of information to promote health issues affectingAboriginal persons. However, the contents and conclusions of this book are solely that ofthe authors and not attributable in whole or in part to Health Canada.
The National Aboriginal Health Organization, an Aboriginal-designed and -controlled body,will influence and advance the health and well-being of Aboriginal Peoples by carrying outknowledge-based strategies.
This book should be cited as:First Nations Centre (2009). Birthing Through First Nations Midwifery Care. Ottawa, ON: National Aboriginal Health Organization.
For queries or copyright requests, please contact:
National Aboriginal Health Organization220 Laurier Avenue West, Suite 1200Ottawa, ON K1P 5Z9Tel: (613) 237-9462Toll-Free: 1-877-602-4445Fax: (613) 237-1810Email: [email protected]: www.naho.ca
Birthing Through First Nations
Midwifery Care

Table of Contents
Introduction .................................................................................................................... 1
Sneak Peak at Midwifery ............................................................................................... 2
“Peacefully You Are Born” .............................................................................................. 3
Challenges & Hope ........................................................................................................ 3
Prophesized Rise of First Nations ................................................................................ 4
Longer Lives, Greater Infant Survival .......................................................................... 6
Shortage of Doctors: You Are Needed ......................................................................... 7
Shortage of Midwives: You Are Needed ...................................................................... 8
Legislative Framework for Midwifery Practice ............................................................ 8
First Nations Midwives Are Getting Organized ......................................................... 9
Becoming a Midwife ....................................................................................................... 9
Midwifery is About Genuine Caring ......................................................................... 10
Homebirth ...................................................................................................................... 12
Community Birthing Through Midwifery Care ........................................................ 13
Two First Nations Models of Care ............................................................................. 15
We Have the Right! ....................................................................................................... 18
Filling the Midwifery Gaps in Good Ways ................................................................. 20
Suggested Next Steps .................................................................................................... 21
Conclusions .................................................................................................................... 22
Citations .......................................................................................................................... 23

1
IntroductionThe National Aboriginal Health Organization launched a number of maternal health resources in February, 2009. These resources, funded by the First Nations and Inuit Health Branch of Health Canada, included the following:
Aboriginal Midwifery in Canada Paper
Midwifery and Aboriginal Midwifery in Canada Map
Exploring the Role of Social Support in Labour and Delivery for First Nations Women and Families Paper
First Nations Doulas Brochure
Inuit Midwifery DVD
“Midwifery form a First Nations Perspective” was written as a complimentary resource document to these preceding publications.
This short paper was commissioned by the First Nations Centre, National Aboriginal Health Organization to focus exclusively on First Nations issues in midwifery, to provide a more in-depth yet inspiring background for consideration by people considering midwifery as a career, or for development of midwifery programs in or near First Nations communities. Dr. Farah Shroff was contracted to write this paper because of her extensive experience as a developer and instructor in midwifery and medical education, as the author of a book on midwifery, as a strong ally for the sovereignty of First Nations people, as a strong advocate of primary care and marginalized peoples, and as a holistic health practitioner.
At first glance, the use or development of midwifery for First Nations women and their families looks challenging. Without brushing over these challenges, Dr. Shroff has found many reasons for celebration of First Nations midwifery. We hope that First Nations women and their families are inspired to see midwifery as an option for birthing their children, in or near their communities, or as a call to become a practicing midwife in their communities.
2
Sneak Peak at MidwiferyThe life of a midwife is very appealing for those who are excited by the intimate connection one can make with a woman and her family during pregnancy, childbirth and the post-partum periods. Midwives make a positive difference in the lives of mothers, babies and families, with healthy lifestyle counselling, emotional, spiritual and physical support. The possibility of using traditional First Nations health care, as part of midwifery care, also exists.
In pre-contact days, First Nations women generally had healthy pregnancies and babies—assisted by midwives. With colonization came powerlessness and poverty which had significant detrimental impact on health outcomes of both mother and baby. First Nations midwives went ‘underground’. It wasn’t until the early 20th century that high rates of maternal and infant mortality were evident. There remains to this day a widespread belief in our society as a whole that a physician run hospital birth is the best and safest way to deliver a child. Until recently medicine has been a male dominated profession with the resultant erosion of the power of midwives. Midwifery has not been viewed as a respected profession within the health care system. Many First Nations communities are isolated and lack doctors, nurses and midwives. In the 1970s nurses at nursing stations were not trained to deliver babies and hence the evacuation process began (SOGC, 2007). Laws were enacted that made midwifery illegal (NWAC, 2007). The residential school system denied an entire generation of girls and young women knowledge about childbirth and infant care. As a result there are only a few midwife elders in rural and remote communities who are able to pass on their skills, traditions and customs related to pregnancy and childbirth (Canadian National Museum of Civilization, 2005).
Currently, many doctors and nurses support the growth of midwifery. Their reasons for supporting its growth are partly altruistic and partly because the need for more maternity care providers has created a crisis. Midwives have a huge role to play in bringing birth back to local communities. There is an existing body of international work from New Zealand and Hawaii, for example, and several small projects all over Canada which have demonstrated that women in good health who have a low risk of needing a high-intervention birth can successfully give birth in their local community with the assistance of a midwife.
There have been a number of important highlights in the journey towards bringing birth back to First Nations communities in Canada. Most provinces and territories in Canada have enacted midwifery legislation, or have included the regulation of midwives within existing legislation ruling the practices of other health professionals. Health Canada has worked over the past five years to develop overarching policy pertaining to First Nations and Inuit midwives. The formation of Canada’s first national Aboriginal midwifery association in 2008 is a major milestone. These 35 midwives have shown great leadership in bringing the voices of First Nations, Inuit and Métis people to the forefront of the revitalized field of midwifery.
3
“Peacefully You Are Born”There’s a Cayuga speech to a baby that goes, “I give thanks, for peacefully you are born. I pray hopefully that peacefully your life will be ongoing, because it is that I think of you clearly, knowing you will always be loved.” When you hear that speech--it came through a family through many generations--you begin to get a sense of how babies were born before we had hospitals. And the word peace is a very potent word. Especially in relationship to a birth, it already gives me a feeling of how that birth went. (Katsi Cook, 2000)
From time immemorial, midwives have been helping to birth the next generation in ways that honour and support life. This is true all over the world. Globally midwifery has been one of the oldest and most respected professions—practiced by both men and women in First Nations communities in Canada. Sandra Jean Kioke, reflected upon the cultural meaning of pregnancy and birth within a Cree community.i She described three levels to the cultural care which women engaged in during the course of their pregnancy and childbirth. The first level was self-care or care provided to the pregnant mother or baby, which involved the basic elements of well-being and good health, survival and growth. The second level includes the infusion of cultural values, practices and understandings into the childbirthing process. Finally, the third level reflects the actualization of those cultural values through the childbirthing process. This may be expressed through five themes: journey, holistic family, interconnectedness, spiritual nature and caring/sharing.ii
Challenges & HopeWith colonization and development of a health care system based on Western science, First Nations midwifery went ‘underground’. Continuing challenges facing the practice of and positive outcomes for First Nations midwifery include Fetal Alcohol Spectrum Disorder; addictions; high birth weight babies; low numbers of First Nations peoples working in the health care field in general and midwifery specifically; remote location of some First Nations communities and their low density population; ongoing racism; access to care; treatment during care; and low levels of social justice (AFN, 2009).
Currently there are not enough midwives to handle all the requests. In Ontario, where the majority of midwives practice, 4 in 10 women are unable to get a midwife (Association of Ontario Midwives, 2006). Rural and remote areas are particularly affected by the shortage. The emphasis is on attracting and retaining foreign trained midwives to practice here. The actual goal of The Midwifery Bridging Project (2006-2010) is to fill in any gaps in their training so these foreign trained midwives can practice in Canada (Midwifery Regulators Consortium, 2006). Evidence does not show such concern
i Kioke,S.J., (1999). Revisiting the Past…Developing Traditional Care and the Cultural Meaning of Pregnancy and Birth in a Cree Community. Thesis submitted to the School of Nursing, Queen’s University: Kingston.
ii Ibid.
4
about accommodating First Nations midwives. Current maternal child health care in on-reserve communities falls far short of national and international standards (Health Canada, 2006). “There is a high turn-over of on-reserve staff complicated by a weakly supported workforce” (Health Canada, 2006). Midwives are not excluded. First Nations women have expressed a desire for Maternity Care Centres run by First Nations people where culturally based maternity care is available. Like all Canadian women they want a choice in regard to their childbirth experience (NAHO, 2007). Presently the practice is to evacuate women at 36-37 weeks of pregnancy to a tertiary care provincial hospital.
Despite these formidable challenges there is much hope, and First Nations women and midwives are enduring the difficult circumstances which they continue to experience. In the words of David Gehue, Spiritual Counsellor, Mi-kmac Nation (1993):
Heal you, the self you help heal the family, The family helps to heal the community, The community helps to heal the nation, The nations help to heal the world.
All the prophecies from other nations now coincide and complement each other.
It is time for us all to stop blaming one another, heal from our wounds and move forward, for the survival of the world, as we know it, lies in our hands. We must seek out and absorb the wisdom of our elders and use it for the betterment of others. The Great Spirit left a clear and legible path in eastern North America with petroglyphs and natural monuments. This knowledge is kept under guard by our elders and only entrusted to those native people who abide by the natural laws of the Great Spirit; respect, honesty, sharing and caring. Without each one of these, the others do not exist.
It is now time for Moms, Dads, Grandmothers, Grandfathers and children to get involved in the healing of our world. Make it your business too.
Prophesized Rise of First NationsToday, in the wake of political and social movements for social justice and the re-emergence of spiritual and holistic forms of health care, First Nations midwifery is rising out of its marginalized position. This moment in the history of Canada is very exciting for midwifery revitalization in First Nations communities and was prophesized many years ago (www.nechi.com/discover/main.php) accessed December 24, 2008:
5
There were a group of Elders who gathered for a ceremony long, long time ago. In that ceremony they were told, “Our people are in our midnight and we will come into our daylight when the Eagle lands on the Moon. When the Eagle lands on the moon we will become world leaders.”
That midnight was the government policy to outlaw our ceremonies, the Indian Act, alcoholism, death, the flu of 1918 and being removed from our families and culture and placed into residential schools.
The message the astronauts sent back to earth in 1969 when they landed on the moon was, “The Eagle Has Landed.” The old people knew the time had come. The time had come to come into our daylight.
Despite the many challenges that continue to exist, there are many reasons to celebrate. Firstly, First Nations people have continued to grow in numbers: an estimated 698,025 people identified themselves as First Nations and this population grew 29% from 1996 to 2006, now representing 2% of the Canadian population (Statistics Canada, 2006).
The birth rate is 1.9% for First Nations communities. The average Canadian population growth rate, at 0.7%, is much lower (Statistics Canada, 2005). On average, First Nations women have their babies at a younger age than other Canadian women (Statistics Canada, 2008; Wenman et al., 2004) which generally gives the mothers and babies a better chance of being in good health during pregnancy, childbirth and child-raising.
Statistics Canada (2008) notes that fertility rates amongst First Nations people have continued to be higher than the overall Canadian fertility rate. The statistical agency also notes that the overall First Nations birth rate was four times the Canadian rate in the 1960s and it is now about one-and-a-half times. In 1999, the birth rate for First Nations was 23 births per 1,000, which was two times the “comparable” rate for the Canadian population as a whole. Other indigenous populations in the United States and Australia have birth rates that are comparable to the Canadian First Nations population; First Nations birth rates are also consistent with those found among the lowest income groups in Canada (Statistics Canada, 2003).
6
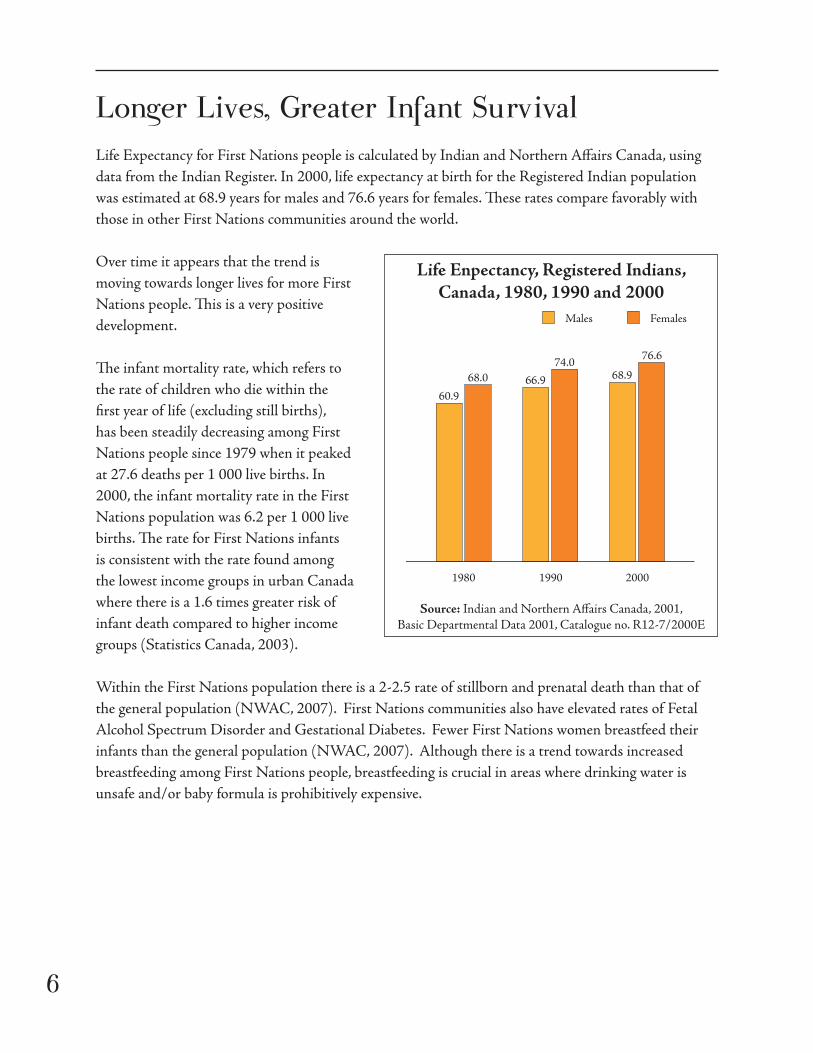
Longer Lives, Greater Infant SurvivalLife Expectancy for First Nations people is calculated by Indian and Northern Affairs Canada, using data from the Indian Register. In 2000, life expectancy at birth for the Registered Indian population was estimated at 68.9 years for males and 76.6 years for females. These rates compare favorably with those in other First Nations communities around the world.
Over time it appears that the trend is moving towards longer lives for more First Nations people. This is a very positive development.
The infant mortality rate, which refers to the rate of children who die within the first year of life (excluding still births), has been steadily decreasing among First Nations people since 1979 when it peaked at 27.6 deaths per 1 000 live births. In 2000, the infant mortality rate in the First Nations population was 6.2 per 1 000 live births. The rate for First Nations infants is consistent with the rate found among the lowest income groups in urban Canada where there is a 1.6 times greater risk of infant death compared to higher income groups (Statistics Canada, 2003).
Within the First Nations population there is a 2-2.5 rate of stillborn and prenatal death than that of the general population (NWAC, 2007). First Nations communities also have elevated rates of Fetal Alcohol Spectrum Disorder and Gestational Diabetes. Fewer First Nations women breastfeed their infants than the general population (NWAC, 2007). Although there is a trend towards increased breastfeeding among First Nations people, breastfeeding is crucial in areas where drinking water is unsafe and/or baby formula is prohibitively expensive.
Life Enpectancy, Registered Indians, Canada, 1980, 1990 and 2000
1980
60.9
68.0 66.9
74.068.9
76.6
Females
1990 2000
Males
1980
60.9
68.0 66.9
74.068.9
76.6
Females
1990 2000
Males
Source: Indian and Northern Affairs Canada, 2001, Basic Departmental Data 2001, Catalogue no. R12-7/2000E
7
Shortage of Doctors: You Are NeededIn Canada there is an “emerging crisis” (Association of Ontario Midwives, 2006) in the field of maternity care. There are not enough physicians to deliver babies. According to a 2002 study, family physicians are catching the majority of Canadian babies followed by maternal and newborn nurses, pediatricians, obstetricians/gynecologists, doulas, pediatric general surgeons and pediatric cardiologists (Canadian Institutes of Health Information (CIHI, 2004). Births are being managed mainly by doctors, but there is a current shortage of doctors who are providing services for both high and low risk pregnancies. In fact there is a maternity care crisis throughout Canada which is more acute in rural areas. With fewer family physicians delivering babies, pregnant women are turning to obstetricians and midwives for care. Due to high insurance rates, and difficulty in finding adequate on-call coverage, many family doctors no longer provide maternity care. In Canada there is also a serious shortage of family doctors. This situation impacts First Nations women in rural and urban communities. The First Nations birth rate is 1.5 times the birth rate of other population groups (NWAC, 2007).
In urban areas First Nations women often face the daunting task of finding a family physician. In Alberta payment for midwifery service is up to $3450. In non-urban areas First Nations women often have to travel potentially unsafe distances for their 10-minute prenatal visits. In areas where evacuation at 36-37 weeks is not the protocol they may make this perilous journey while in labour. Various factors are related to doctors’ declining role in maternity care: unsocial hours; limited financial remuneration; increased liability insurance costs; lack of support from colleagues; for rural doctors: lack of local resources and distance to referral centres.
Family doctors entering practice may believe that maternity care will add more stress to their already busy lives…Research on new family doctors suggests that confidence in obstetrical skills, fee structures and fear of malpractice suits are all factors that inhibit them from choosing to deliver babies as part of their practice (Whynot, 2004).
The Society of Gynecologists and Obstetricians of Canada (SOGC) have issued a policy statement on midwifery that recommended more integration of midwives into health care services for pregnant and childbearing women. They state that “midwifery care and midwifery training should be an integral part of changes in maternity care.” Midwives are now members of the SOCG.

8
Shortage of Midwives: You Are NeededCurrently there is a lack of First Nations health professional and this is reflected in the lack of First Nations midwives. There is a lack of data on the number of First Nations midwives and the current number in practice. Demographic distribution and requirements remain unclear. Data is required dealing with the percentage of First Nations children delivered by midwives, where these deliveries occur (home birthing centre, hospitals), and outcomes. Midwifery services for the Inuit, especially the Nunavik Inuulitsivik program, have been extensively researched internationally as well as in Canada. Little data for First Nations midwifery is available. Maternal and infant mortality rates for First Nations women delivered at home, in a birthing centre, and hospital settings are areas of concern. Data is required regarding economics. There is a paucity of economic literature relating to home births and birth centres (Henderson et al., 2008). It is widely believed that home births and birth centres may help decrease the cost of maternity care for uncomplicated pregnancies and deliveries (Henderson et al., 2008) but quantitative evidence is scarce. The Netherlands is often cited as an example of how advantageous midwifery is but distances are much shorter and technological help much easier to access than in remote or semi remote areas of Canada. One must also factor in the cost of insurance for midwives and the fact that highly skilled and hence costly midwives are required to provide care in remote areas. Unforeseen problems can arise quickly and help is unavailable. Consults to far away specialists don’t rescue all babies. It is also costly to set up delivery suites and build birthing stations.
In total, 800 midwives are registered with the Canadian Association of Midwives as of March 2008. Midwives are attending the births of less than 10% of Canadian families; homebirths attended by midwives make up about 1-2% of births in Canada (Martin and Lydiate, 2008). The Ontario Midwifery Education Program has received funding to increase the number of students as a result of the need for more midwives to fill the gaps in maternity care.
Legislative Framework for Midwifery PracticeLegislation governing the practices of midwives has been enacted in most provinces. In several provinces, First Nations midwives enjoy special exemptions and are recognized as distinctive from other practicing midwives with respect to their traditional approaches to and understandings of the child birthing process and the unique needs of First Nations women. Several legislative schemes make specific reference to ‘aboriginal midwifery’, which in British Columbia’s regulations is defined to include the blending of both traditional and contemporary practices. More specifically, in that province ‘aboriginal midwifery’ is defined to include the use and administration of traditional herbs and medicines, cultural and spiritual practices, contemporary practices originating from traditional practices, or a combination of both.

9
Several legislative schemes include a ‘grandfathering’ clause applicable to practicing First Nations midwives which exempts them from having to register their practices. For example, First Nations midwives on-reserve are specifically exempt in British Columbia and Ontario (Section 5(2) of the Midwives Regulation, schedule 13 of the Health Professions Act in B.C., and Section 8(3) of the Midwifery Act in Ontario) from registering as a midwife if they were practicing prior to the regulations/legislation.
In Ontario, in addition to registration exemptions, First Nations midwives are allowed to practice under the title ‘aboriginal midwife’ or the equivalent in any other language.
First Nations Midwives Are Getting OrganizedIn 2008 a group of First Nations, Inuit and Métis midwives joined the Canadian Association of Midwifery. This First Nations, Inuit and Métis midwifery group includes 35 members. This is a very exciting initiative that will develop First Nations (and other) midwives’ visions, models for practice, and wisdom. Many of the provincial models of practice include elements which reflect the five themes presented by Sandra Kioke, as described previously in this paper. For example, many of the models of practice include basic ‘fundamentals’ such as community input, informed choice, continuity of care which reflects the development of a relationship with and safe support for the pregnant woman, and a choice of birth setting.
There are many exciting steps that the larger group of First Nations midwives could be taking to support initiatives of First Nations midwives: for example, creating linkages with First Nations midwives throughout the Americas and internationally, and the creation of a college program specifically designed for training First Nations midwives.
Becoming a MidwifeNAHO’s 2009 paper, Aboriginal Midwifery in Canada, describes three options for First Nations women who wish to become midwives. They may become educated within Traditional First Nations educational institutions, non-First Nations universities, or receive a blended education (mix of First Nations and non-First Nations traditional knowledge). Carol Couchie, a First Nations midwife talks about some of these options in inspiring ways:
We need to train midwives as much as possible. We need people to have an opportunity to go and work in remote settings, to live there, to be a part of that, because we need the people who live there to be trained. So if we can put people in every two or three months, and that student midwife who is there and that is her practice and she is developing it, and she is learning
10
how to catch those babies with an experienced midwife there, in that apprenticeship model then eventually, you don’t have to send people up there any more. And even if that young woman quits, and moves to another smaller community, that knowledge goes with her. It is the democracy of knowledge. You bring back that knowledge that once belonged to our communities and give it back to them. And it stays there. Those people don’t go home. They are home. (Excerpt from Aboriginal Midwifery in Canada, 2009).
First Nations midwifery training is a very important issue when speaking of First Nations midwifery in Canada. Many communities are looking at ways of developing training that is best suited to their home communities and their current infrastructures, capacities, and community support. First Nations midwifery has the goal of safe and culturally appropriate birthing that emphasizes respect for life and the empowerment of women. In both Ontario and Québec, community based training programs exist where First Nations midwives learn from practicing midwives at local birthing centres. These centres aim to deliver culturally relevant maternal care. This process reflects ancient First Nations practices, as well as the place of older women as repositories of medical and spiritual knowledge.
It is noted that midwifery education and midwifery practice are inextricably linked, and when considering midwifery in communities, considering models of educating midwives in those communities is an integral part of this process. The following is a list of the two most prominent First Nations midwifery training programs in Canada today.
Kanaci Otinawawasowin Baccalaureate Program (KOBP; University College of the North, The Pas, Manitoba: http://is-8668.ucn.ca/webpages/xml/xml_output/2009_7_4/Program_List_1249406064437.xml)
Tsi Non:we lonnakeratstha Ona:grahsta’ First Nations Midwifery Training Program (Six Nations, Ontario: http://www.snhs.ca/midBackground.htm)
In the rest of Canada, midwifery is generally an accredited four-year program at post secondary institutions.
Midwifery is About Genuine CaringAfter years of working with women, midwives and their supporters have created a model of care that is genuinely concerned with meeting the needs of clients. This model has the potential for positively influencing the models of care that are entrenched in the mainstream health care system and most closely resembles the kinds of care raised during discussions of cultural sensitivity. Rather than placing the professional at the centre, the “woman-centred” midwifery model, puts the woman and her birthing experience at the centre. This kind of care is composed of three main elements:
11
1. Informed choice
Informed choice is providing birthing women with comprehensive information about all aspects of their care so that THEY may be the primary decision makers during the course of their midwifery care. This may include information about ultrasound tests, for example; midwives explain the results of research conducted on ultrasound technology and the most current ideas about benefits and drawbacks about it. Birthing women may then decide to undergo testing or not.
Strictly following the tenet of informed choice therefore means that midwives work with their clients under a wide variety of circumstances and that midwives continue to provide woman-centred care to all their clients regardless of the kinds of informed choices made by their clients.
2. Choice of birth place
Birthing women have the right to choose where they would like to labour and deliver their babies. Women who are deemed to be at low risk of having anything but normal and healthy deliveries (after examination), have the option of labouring and delivering in their homes, birthing centres, or hospitals. In most Canadian jurisdictions, midwives have privileges in all of these three options but generally the choice is between home and hospital, as few birthing centres exist. Pregnant women whose health conditions put them, potentially, at “high risk” are either referred or transferred to the care of a physician. In exceptional circumstances, physicians and midwives may work together to care for women who specifically request midwifery care but also need the care of physicians.
A cornerstone of midwifery care is the right of birthing women to choose to give birth in their home environment with the hospital as a back-up option. Home birth is discussed below in a separate section.
Birthing centres combine the advantages of hospitals’ technological capabilities within an environment that is more home-like than hospital-like. Birthing women who are concerned about the potential for unexpected problems arising during childbirth (e.g. live far away from hospitals) have expressed an interest in the use or creation of birthing centres in or near their communities. A few such centres exist in the country, but at present, are considered expensive, with little understanding or support for their potential benefit.
Women may also choose to give birth in a hospital with the assistance of midwives. Midwives have already, or will likely gain privileges at hospitals all around the country so their clients may plan to give birth in a hospital. In the case of a transfer of care from a

12
midwife to a physician, midwives may still be involved in some aspects of her psychosocial needs--transmitting information about the progress of a cesarean birth to the partner, advocating for the woman etc.
3. Continuity of care
Birthing women receive continuous care from two to four midwives during the course of their care. While they are pregnant, they may meet up to four midwives who practice together. In most midwifery practices, birthing women work with a primary midwife and a back-up midwife. The same midwives they have met during their pregnancies are present at their birth. In other midwifery practices, birthing women work with up to four midwives before birth, could have any of them at the birth, and for the six weeks of post-partum visits.
This continuity allows women to develop rapport - and in some cases long-term, meaningful relationships - with their care providers. Close contact, mentally, emotionally and otherwise, with midwives has catalyzed the “midwife as friend” concept which has made midwifery so popular with women. Midwives often share their own lives with birthing women and this tends to foster the egalitarian model of care that midwives uphold, for it shows that midwives are not “above” their clients and in fact may have much in common with them.
Women who have experienced medically-managed childbirth (also known as the medicalization of birth) often complain that they met several people during the course of their care. Especially during labour and delivery, this fragmentation of care can be confusing, exhausting, and even frightening. Having to repeat herself time after time, to the next person on shift or the new person involved in her care, can take away from the meaningfulness of the birth experience. Continuity of care is thus a critical component of midwifery.
HomebirthAs mentioned above, homebirth is a critical component of midwifery care and sometimes, this principle is listed separately from the principle of choice of birthplace in order to emphasize its importance. Homebirth has possibly been the most contentious aspect of midwifery care as many care providers argue that it is unsafe. They argue that unpredictable/unpredicted problems could arise in a split-second and these problems may be potentially fatal without the aid of technology.
Those who argue for the safety of homebirth cite research which shows that homebirth outcomes are equally as safe as those of hospital births. Such research includes: Tyson (1991), Sullivan and Beeman (1983); Mehl and Whitt (1977); Campbell and MacFarlane (1986) and more.
13
The home, for most women, is the place where they have power, control, comfort and love. In familiar physical and social surroundings, women report that birthing is an infinitely less difficult process than being in unfamiliar, sometimes unfriendly, hospitals. At home, many women are accustomed to being in charge and having their wishes followed. Having competent caregivers who nurture and assist birthing women in having the most positive birthing experience possible is a joy for many mothers, especially those who have supportive partners, families and communities as well as sufficient economic and social resources (eg. adequate income, maternity/paternity leave, child care etc.) to have a positive home birth.
Homebirth can only be a positive option for women for whom home is a positive environment. For women who face violence, abuse and other forms of oppression in their homes, hospital births may provide an alternative to the site of their abuse.
The College of Midwives’ 1994 Statement on Home Birth notes that most births occur in hospital and midwives must be capable of attending hospital births. It states that birth is more than a physical or medical event and that a number of expectant parents plan to have home births and that “normal birth at home must be encouraged and supported.” The statement ends by discussing safety: “Available evidence does suggest that for low-risk women, a planned birth at home with trained attendants is a safe and viable option.”
Community Birthing Through Midwifery CareWomen in rural and remote communities report that the health care they receive is satisfactory. However they are concerned that many gaps in their care exist: health services are not culturally appropriate, care is neither accessible nor holistic and is not consistent or comprehensive (Sutherns et al., 2003).
The practice of evacuating First Nations pregnant women who live in rural and remote communities to give birth in regional centres has been criticized by the women themselves, First Nations communities and organizations, health professionals, and others (Stebo, 2008; NAHO, 2008; Couchie and Sanderson, 2007; Smith, 2003). A growing body of evidence suggests that besides all the other pitfalls, this practice of evacuation contributes to higher rates of postpartum depression and increased maternal and new-born complications (Klein et al., 2002).
The crisis in maternity care across Canada acutely affects First Nations women living in rural and remote communities for various reasons. A history of colonialism has created contemporary relationships between medical institutions and First Nations communities that are marred by racism, creating poor and sometimes abusive services and barriers to accessing these services (AFN, 2009; Marsden, 2008). Throughout rural and remote communities populated by First Nations people maternity care services are fragmented and inconsistent.
14
For women with high-risk pregnancies evacuation is clearly the only option as most small communities do not have requisite equipment or the personnel to handle high-intervention childbirth. First Nations women who are required to leave their communities to deliver their babies outside of their communities ought to receive adequate funding (Kornelsen and Gryzbowski, 2005) to cover all the costs of caring for their children back home, phone calls to their family, and transportation and other costs. Women at low risk, however, ought not to have to choose between their culture or their safety (Couchie and Sanderson, 2007).
Indigenous women in rural and remote communities seek a sustainable model of maternity care for their communities that are comprehensive, collaborative, community-based continuum of care that builds on and develops local capacity (Tedford, Gold et al., 2005).
Women who have healthy pregnancies and will likely have healthy babies can be safely managed in local or regional centres (Couchie and Sanderson, 2007) as long as a system for transfer to high-intervention maternity care services exists in case of emergencies (Kornelsen and Gryzbowski, 2005). Accepting that some level of risk is inherent in the birthing process, as with most other healthy processes, is more important for families living far from emergency maternity care services. Traditionally First Nations women have accepted that birthing has risks and have been prepared to deal with the pain of labour with minimal pain relief.
First Nations midwife Aleka Stebo (2008) states:
It is my impression from this synthesis of the literature that birth centre care may be the best-suited model of care for the provision of maternity care forrural BC [First Nations] women. Birth centre care is based on family-centred, individualized, respectful care for low-risk women. This is congruent with the midwifery model of care, which is also based on continuity of care and grounded in a philosophy of respect for the social, emotional, spiritual and cultural aspects of birth. This type of care is missing in rural settings when women are being evacuated for birth. Access to birth centre facilities would enable birth to return to [First Nations] communities and families.
Aleka Stebo’s recommendations for further action have been put into the following numbered list:
1. Qualitative research initiated by rural First Nations women describing what they desire for their birth experiences.
2. Population based research regarding First Nations birth outcomes in BC.3. Research that reveals where rural First Nations women are giving birth, where do they live
permanently, what were the specifics of their pregnancy, and birth, i.e. were they low-risk? Thus revealing if local birth centre care would be applicable and where would be the most useful locations.
15
4. Recruiting and training First Nations midwives. 5. Exploration of re-opening currently closed rural hospital maternity wards as birth centre
facilities staffed in whole or in part by midwives.6. The establishment of rural birth centres with a special focus on serving First Nations
women and their families, staffed by First Nations midwives, providing culturally safe care in BC.
Two First Nations Models of CareIn March 2009, the First Nations and Inuit Health Branch of Health Canada hosted a National Aboriginal Midwifery Forum. Several models of midwifery care were presented at that forum as models which had been demonstrated as responsive to the needs of First Nations women and their families. Two of these models are presented below, as examples of best practices for midwifery services currently being delivered to First Nations women, their children and their families.
1) O’Chiese First Nation and Sunchild First Nation Collaborative Shared Care Maternity Services Program – Midwifery Pilot
There was an identified gap in prenatal care by local physicians, hospitals and nurses. In response to the call for increased and improved services, the Collaborative Shared Care Maternity Services Program was developed and implemented. The program is currently in its second year of operation and is considered to be very successful.
OVERARCHING GOALSw Optimized health and well being of mother and newborns within the context of their social networks;w Patient care provided through shared model to ensure safety, comprehensiveness, accessible care from preconception through to postpartum period;w Sustainable program capable of expansion.
PARTNERS/COLLABORATIVE NETWORKw Alberta Association of Midwives – registration and regulation of midwivesw Health Canada – access to health services, access to health information, building capacity, accountability and resourcesw Rocky Mountain Primary Care Network – access to primary care, manage ‘round-the-clock’ access to services, coordination of integrated health services including long-term care and specialty care services, address physician shortage, increase emphasis on health promotion, disease and injury prevention, care of patients with complex needs, care for patients with chronic diseases

16
w David Thompson Health Region – determine priorities in health care, allocation of resources, promote responsive services, integration of servicesw Sunchild First Nation – culture and supportw O’Chiese First Nation – culture and support
NATURE OF COLLABORATIONw Bilateral relationship amongst partiesw Common ‘line of action’ established through program elementsw Formal agreement through Memorandum of Understandingw ‘Smooth’ operations and shared resourcesw Clear understandings established amongst parties, which sets out expectations
MIDWIFERY SERVICES1) Preconception monitoring and counselling2) Education3) On-call rotation4) Pre-natal care5) Intra-partum care6) Post-partum care, including breast-feeding support
2) Transition to a Multi-disciplinary Primary Care Maternal Child Health Program (Debbie Vey, RN, RM – File Hills Qu’Appelle Tribal Council)
Through the Aboriginal Health Transition Fund, the All Nations Healing Hospital received funds which were partially used for the development of a proposal resulting in the midwifery program services.
PROGRAM GOALSw Ongoing strengthening in maternal health services; w Integrated care roles of health professionals;w Multi-disciplinary maternity health team; w Manage maternity care locally (as much as possible);w Established standards of intrapartum, postpartum and neonatal care;w Development of risk-assessment tools;w Community-based services focusing on the needs of First Nations (and other Aboriginal) people;w Improved prenatal and postnatal outcomes through increased capacity to identify childbearing clients of all risk levels and follow clients throughout childbearing period;w Addition of maternity services, including low-risk deliveries
17
COMPREHENSIVE FRAMEWORK/COLLABORATIVE NETWORKw Coordinate, integrate and improve care received by First Nations women and their children;w Women’s Health Centrew Maternal Child Health Program, Health Canada
PROJECT ELEMENTSw 2 project sitesw Moving away from ‘clinical’ care environment and providing services in group format;w Empower women to make their own decisions;w Include three key components: assessment, education, supportw Group women together by common/close due datesw Women engage in self-care activities (monitoring blood pressure, weight, urine)w Complete elements of self-care on floor mat within group spacew Complete group activities in circle.
KEY PRINCIPLES1) Women are more likely to access maternal health care offered close to their homes2) First Nations women are more likely to access health care services owned and managed by their community or Tribal Council, where there is strong First Nations community support3) Local access to prenatal care results in improved communication between women and their care providers
SERVICESw Doula carew Traditional parenting knowledgew Cultural programming and services available through Elders, ceremonial leaders and traditional healersw Outreach services, including home visitsw Ongoing communication with community governance and community members
18
We Have the Right!Over 60 years ago the United Nations declared that all people have fundamental rights. The Preamble notes that the “inherent dignity and of the equal and inalienable rights of all members of the human family is the foundation of freedom, justice and peace in the world” (United Nations, 1948).
Violence against First Nations women has a significant impact on pregnancy, childbirth and childrearing. Social justice work, counselling, healing and other excellent efforts are being made by many First Nations groups such as the Native Women’s Association of Canada (http://www.nwac-hq.org/en/background.html), Aboriginal Women Against Violence Everywhere (http://www.aboriginalwomenonthemove.org/Links.html), Warriors Against Violence Society (http://www.kiwassa.bc.ca/wav/), First Nations Child and Family Caring Society (http://www.fncfcs.com/). Racism, sexism and class prejudice are some of the challenges facing this work. Article 25 of the Universal Declaration of Human Rights
(1) Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control.
(2) Motherhood and childhood are entitled to special care and assistance. All children, whether born in or out of wedlock, shall enjoy the same social protection (United Nations, 1948).
These articles of the Universal Declaration of Human Rights are particularly relevant to the care of pregnant and childbearing women and their families. Social justice efforts of First Nations peoples require an analysis at all levels: local, provincial/territorial, national and international. Bringing international pressure to bear on Canadian governments could prove to be a powerful tool.
Besides the UN Declaration of Human Rights is the Constitution of the World Health Organization which states: “the enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being” (World Health Organization, 1948). Canada, like most countries of the world, is thus party to at least 2 international treaties that addresses health-related rights.
19
The right to positive health status is enshrined in these treaties. Discrimination based on ethnicity, sex, income or other factors has negative health consequences. So taking steps to protect human rights such as the right to clean water, nutrition, adequate housing has a positive impact on health status (World Health Organization, 2008).
The Canada Health Act, the Canadian Charter of Rights and Freedoms and other government documents are intended to provide health equity for all, including First Nations peoples. Partly because of the lack of implementation of the ideas within these and myriad other Canadian government documents, the above-mentioned international documents may be useful in arguing for the right to health, and to midwifery, for First Nations peoples.
These basic steps provide a basic framework for making health care a human right:
Principles of Human Rights for Ethical Health Care (Merali, 2001 cited in Smith, 2003)
w The right to accurate informationw The right to free and informed decision-makingw The right to privacyw The right to confidentialityw The right to choicew The right to dignityw The right to access, regardless of sex, sexual orientation, race, disability, marital status, age, socioeconomic class, location…etc.w The right to safetyw The right to express an opinionw The right to participation
Based on: Cook, R. & Dickens, J. (1998). Considerations for formulating reproductive health laws. Geneva: WHO. International Planned Parenthood Federation (IPPF), (1997). IPPF charter on sexual and reproductive rights and rights of the client. London: Author.WHO/UNICEF/UNFPA. Women friendly health services: Experience in maternal care. Mexico City workshop. January, 1999.
20
Filling the Midwifery Gaps in Good WaysCanadian midwifery education programs in Ontario, BC, and Québec are graduating fewer midwives than are required by the demands of childbearing women. Currently all the non-Native midwifery education programs produce small numbers of graduates. Although the number of graduates is increasing, there were only 19 graduates across Canada in 1996 and 34 graduates in 2004 (CIHI, 2005). This is literally a drop in the bucket, with 800 midwives in Canada serving 10% of pregnant women.
As noted in the section above, racism is a serious thorn in the side of midwifery in Canada and elsewhere. Addressing racism within the midwifery community in a straight-forward and up front manner is possible through professional development training. Non First Nations midwives can play an important role as allies and service providers if some basic cross-cultural training is provided.
Around the world, anti-racism is a priority for midwives. For example, the Seattle Midwifery School in the USA is committed to a learning environment that is free from racism and bigotry (Seattle Midwifery School, 2008). In Ireland, the Irish Nurses’ (and Midwives’) Organization created a Cultural Diversity Taskforce that recommended embracing the cultural diversity of all members and promoting cultural diversity of all health workers to prevent racism. The Equality Authority of Ireland produced an Action Plan for the Anti-Racist Workplace with the following components (http://www.equality.ie/index.asp?docID=281):
w Adapting the Minority Provide induction training for migrant workers.
w Making Cultural Allowances Implement work life balance working arrangements for Black and minority ethnic (including Traveler) employees.
w Changing Majority Attitudes Provide equality and diversity training for all employees.
w Changing Majority Behaviour Put in place anti-discrimination, sexual harassment and harassment policies and procedures.
w Changing Rules and Procedures Review all employment policies and procedures to ensure they take account of and accommodate cultural and linguistic diversity.
w Active Recruitment and Promotion Develop an equality action plan for full equality in practice.
w Mainstreaming Equality Embed an equality focus into everyday management processes and decision making.
21
In Canada, the Ontario Hospital Association produced an Anti-Racism Resource Package in collaboration with the Ontario Ministry of Health. The Package includes Anti-Racism Guidelines; Anti-Racism Organizational Change Self-Assessment Tool; a Video “No Excuse” with a discussion guide, amongst other documents (Ontario Hospital Association, 2008).
A systems approach is one that recognizes that processes, such as the integration of foreign-education midwives into the Canadian workforce, require a number of components to be working in unison for the system to be most effective. Creating a systems approach to First Nations midwifery on a federal level is challenging because many parts of the system, such as health care, are provincially governed. So in the creation of a federal systems approach, collaboration, harmonization, and innovation requires a respect for differences in jurisdictions, and differences in status as First Nations people.
Suggested Next StepsThere has been some remarkable progress made over the past several years towards bringing birthing back to communities. This progress should be both noted and built-upon. There have been a number of next steps highlighted as possible areas upon which further success can be realized. These next steps are founded on considerations which include community history, community capacity, available resources, the need for strong partnerships and supports, accountability and leadership. Next steps include:
w Gathering and synthesis of accurate, disaggregated data particularly from in a First Nations context;w Development of fact sheets reflecting programs and services, models for practice;w Tool development – for measuring such things as community readiness, barriers to program implementation and risk assessment;w Networking opportunities for midwives and students training to become midwives;w Promotion of best practices models and effective, safe/recommended ‘short-cuts’ to developing and implementing programs in communities;w Apprenticeship models;w Case management strategies and team-building;w Partnerships between associations and colleges promoting First Nations midwifery;w Creating opportunities for collaboration among First Nations midwives with opportunities to discuss best practices;w A comprehensive national strategy to recruit midwives to First Nations practices;w Promotion of the important role midwives play in First Nations communities.
22
ConclusionsThe birth rate is high in First Nations communities and promises to continue to be high. Midwives can play a great role in assisting mothers to have healthy pregnancies and healthy babies. Life expectancy is also increasing. These trends are very positive.
In the near future First Nations babies could be born in their home communities by expanding health centres and providing training for First Nations midwives. This will help to improve prenatal and birth experiences for First Nations women: The models of care offered by the Inuulitsivik Health Centre maternity ward in Puvirnituq, the Inukjjuaq maternity centre, and the Rankin Inlet birthing centre demonstrate that low-risk births can be safely managed in local or regional centres (Couchie and Sanderson, 2007).
In order to create solid plans for First Nations maternity care we need data on: what First Nations women want for their perinatal care; First Nations pregnancy and birth outcomes; maternal health data; breastfeeding rates and more. Ideally this could be collected, analyzed and presented by FN peoples.
Currently a collaborative model needs to be more formally developed given that maternity care is shared by midwives, nurses, and doctors—both family physicians and obstetricians.
More midwives are desperately needed in rural and remote communities—particularly for First Nations people. The creation of a strong association of First Nations midwives may be able to negotiate registration of traditional First Nations midwives in a respectful fashion, thereby utilizing peoples’ skills that are currently unutilized and increase the numbers of midwives able to serve First Nations communities. Besides the clear demand for local maternity care, researchers have recommended that midwives be the primary care providers for low-risk women in rural and remote communities even if there are no emergency facilities available.
Midwives make a positive difference in the lives of mothers, babies and families providing counselling, as well as emotional, spiritual and physical support. The FNC hopes that First Nations women will consider midwifery in their communities as a career option and that expecting mothers and their families will become inspired to see midwifery as an option for birthing their children. Midwives have a huge role to play in bringing back birth to First Nations communities.

23
CitationsAssembly of First Nations (2009). Backgrounder on Health Crises in First Nations communities.
http://www.afn.ca/article.asp?id=2646
Amnesty International (2004). Stolen Sisters Discrimination and violence against Indigenous women in Canada-Report Summary. http://www.amnesty.ca/stolensisters/concerns.php
Association of Radical Midwives (2000). Male Midwives. UK Midwifery Archives: A discussion group for people interested in Midwifery in the UK. http://www.radmid.demon.co.uk/malemidwife.htm
Backman, G., Hunt, P., Khosla, R., et al. (2008). Health systems and the right to health: an assessment of 194 countries. The Lancet, 372, 2047- 2085.
Benoit, C., & Carroll, D. (2004). Aboriginal Midwifery in Canada: Merging Traditional Practices and Modern Science. In. I. L. Bourgeault, C. Benoit, and R. Davis-Floyd (Eds.) Reconceiving Midwifery. Montréal, QC: McGill-Queen’sUniversity Press.
Bentham K. (2003) Maternity care for the asylum seekers. British Journal of Midwifery, 11, 73-77.
Birch, D. (2004). Aboriginal Midwifery in Canada: Reflections of A Manitoba Midwife. Proceedings of the Midwifery Way conference held in Halifax, Nova Scotia.
Canadian Institute for Health Information (2005). Giving Birth in Canada: Providers of Maternity Care. http://secure.cihi.ca/cihiweb
Canadian Institute for Health Information (2005). Midwives. http://secure.cihi.ca/cihiweb/products/Midwives.pdf
Canadian Midwifery Regulators’ Consortium (2008). A Day in the Life of a Midwife from Manitoba. http://cmrc-ccosf.ca/node/16
Canadian Midwifery Regulators’ Consortium (2008). A Week in the Life of a Midwife from Quebec. http://cmrc-ccosf.ca/node/73
Canadian Resource Centre for Victims of Crime (2009). Restorative Justice in Canada. http://www.crcvc.ca/docs/restjust.pdf
Commanda, Chief W. (2000). Seven Fires Prophecy of the Anishnabe People and the Process of Reconciliation. http://www.oneprayer.org/Seven_Fires_Prophecy.html
Cook, K. (2000). Interview with Katsi Cook. Talking Leaves, Spring Edition. http://www.talkingleaves.org/node/61
24
Couchie, C., & Sanderson, S. (2007). A Report on Best Practices for Returning Birth to Rural and Remote Aboriginal Communities. Ottawa, ON: Society of Obstetricians and Gynaecologists of Canada, 29, 250–254.
Carvel, J. (march 12, 2008). Bullying and racism claims at nursing and midwifery council. Manchester, UK: The Guardian. http://www.guardian.co.uk/society/2008/mar/12/nhs.health3
Earl, S., & Church, S. (2004). Ethnicity and Reproduction. Milton Keynes, UK: Open University.
Evehema, Chief D. (accessed December 25, 2008). Chief Dan Evehema’s Message to Mankind. http://www.think-aboutit.com/native/chief.html
Fairfax Media (2007). Midwife gives ‘street’ babies a better start. http://www.midirs.org/midirs/midszone.nsf/essart/A3A6D0AA4B85FDBB80257359005ABEA3!OpenDocument
First Nations Statistics (accessed January 13, 2009). http://www.firststats.ca
Fox, R. (1997). The antenatal education needs of Māori women (in the Tainui region) and implications for midwifery practice. Wellington, NZ: Master’s Thesis, University of Wellington.
Gehue, D. (1993). From the Eastern Door: We are in the final stages of the shaking of the earth, when the Great Spirit takes the earth in both hands and shakes it violently. http://www.thepeoplespaths.net/political/cry.html
Gerein, K. (April 3, 2008). Health care is a top human right: Robinson Former UN commissioner speaks to full house at Citadel. The Edmonton Journal.
Government of British Columbia (2004). Charting Birth Outcome in British Columbia: Determinants of Optimal Health and Ultimate Risk - An Expansion and Update http://www.vs.gov.bc.ca/stats/features/index.html
Hunt, S. C., & Richens, Y. (1999). Unwitting racism and midwifery. British Journal of Midwifery, 7, 358.
Indian and Northern Affairs Canada (2001). Basic Departmental Data 2001, Catalogue no. R12-7/2000E http://www.hc-sc.gc.ca/fniah-spnia/diseases-maladies/2005-01_health-sante_indicat-eng.php
International Work Group for Indigenous Affairs (2007). Declaration on the Rights of Indigenous Peoples. http://www.iwgia.org/sw248.asp
Irish Nurses (and Midwives) Organization (2002). Cultural Diversity Taskforce. http://www.ino.ie/DesktopModules/Articles/ArticlesView.aspx?TabID=431&ItemID=3187&mid=7569
25
Jasen, P. (1997). Race, Culture, and the Colonization of Childbirth in Northern Canada. Social History of Medicine, 10, 383-400.
Kennedy, H. P., Erickson-Owens, D., & Davis, J. (2003). Voices of Diversity in Midwifery: A Qualitative Research Study. Journal of Midwifery & Women’s Health, 51, 85 – 90.
Kirkham, M., Elizabeth, J., & Perkins, R. (Eds.) (1997). Reflections on Midwifery. London: Elsevier Health Sciences.
Klein, M. C., Christilaw J., & Johnston, S. (2002). Loss of maternity care: the cascade of unforeseen dangers. Canadian Journal of Rural Medicine, 7, 120–121.
Looking Horse, Chief A. (2008). Lakota Prophecies. http://www.crystalinks.com/lakota.html
Kornelsen, J., & Gryzbowski, S. (2005). Is Local Maternity Care an Optional Service in Rural Communities? Canadian Woman Studies Journal, April, 327-29.
Marsden, D. (2009). Personal Communications. Dr. Marsden is a former health researcher at the National Aboriginal Health Organization, Ottawa, Ontario.
Marsden, Dawn (2008). Personal Communications. Dr. Marsden is a former health researcher at the National Aboriginal Health Organization, Ottawa, Ontario.
Marsden, Dawn (2007). PhD Thesis. Vancouver, BC: University of British Columbia.
Martin, K., & Lydiate, R. (2008). Canada: closer to the goal of regulated midwifery across the country. International Midwifery. http://www.allbusiness.com/health-care/health-care-professionals-midwives/10553845-1.html
Mignone, J. (2008). Strengthening Indigenous Midwifery and Intercultural Care. Case Study Profile. Canadian Coalition for Global Health Research.
http://www.ccghr.ca/docs/GIHR_Case_Study_e.pdf
Mitchison, W. (2002).Giving Birth in Canada, 1900-1950. Toronto: University of Toronto Press.
Mothers Matter: Postnatal Depression and Families New Zealand/Whanau Trust. http://www.mothersmatter.co.nz/Culture/Maori.asp
Nasafotie G. (2008). Fulfilling The Prophecy Of Peace. http://nativeunity.blogspot.com/2008/02/fulfilling-phophecy-of-peace.html
National Aboriginal Health Organization (2008). Midwifery and Aboriginal Midwifery in Canada. Ottawa, ON: Author.
26
National Aboriginal Health Organization (2008). Podcast of Aboriginal Midwifery in Canada. Ottawa, ON: Author.
Nga Maia (Maori Midwifery Organization). http://www.ngamaia.co.nz/wawcs017243/ln-about-nga-maia.html
Nestel, S. (2006). Obstructed Labor: Race and Gender in the Re-Emergence of Midwifery. Vancouver, BC: University Of British Columbia Press.
Obomsawin, R. (2007). Cultural Competency in Primary Health Care for Canada’s Aboriginal Peoples. Ottawa, ON: Health Canada Primary Care Division of the First Nations and Inuit Health Branch.
Obomsawin, R. (2003). Aboriginal Institutional and Corporate Initiatives in Canada related to Traditional Culture and Development. Submitted to CIDA Americas Branch, InterAmerican program.
Ontario Hospital Association (2008). Anti-Racism Resource Package. http://www.oha.com/Client/OHA/OHA_LP4W_LND_WebStation.nsf/page/Knowledge+Centre+-+Guides
Price, W. A. (1938). Nutrition and Physical Degeneration. Project Gutenberg of Australia. http://gutenberg.net.au
Richens, Y. (2003) Building bridges: involving Pakistani women. The Practicing Midwife, 6, 14 - 17.
Royal College of Midwives (2000). Position Paper No. 23 RACISM AND THE MATERNITY SERVICES
http://209.85.173.132/search?q=cache:gxovUKz6v7wJ:www.rcm.org.uk/EasySite Web/GatewayLink.aspx%3FalId%3D12791+Tackling+Racism+%E2%80%93+R oyal+College+of+Midwifery+Guidelines&hl=en&ct=clnk&cd=1&gl=ca&client= firefox-a
Pomare, E., & De Boer, G. (1988). Hauora: Maori standards of health 1970-1984. Wellington, NZ: Ministry of Health.
Ramsden, I. (2002). Cultural Safety and Nursing Education in Aotearoa and Te Waipounamu. PhD Thesis, Victoria University of Wellington. http://kawawhakaruruhau.massey.ac.nz/RAMSDEN%20THESIS.pdf
Royal Commission on Aboriginal Peoples. Looking forward, looking back: report of the Royal Commission on Aboriginal peoples. Vol. 1. Ottawa, ON: Author.
Seattle Midwifery School (2008). www.seattlemidwifery.org/document/mep/09-12MEPCatalogWeb.pdf
Shroff, F. M. (1996). New Directions in Canadian Health Policy: Lessons from Holistic Medicine. PhD Thesis. Toronto: University of Toronto.
27
Shroff, F. M. (1997). Midwifery—From Rebellion to Regulation. The Rebirth of an Ancient Calling. In F. M. Shroff (Ed.) The New Midwifery. Toronto: Women’s Press.
Shroff, F. M. (2000). Ayurveda: Mother of Indigenous Health Knowledge. In G. Dei and B. Hall (Eds.) Indigenous Knowledge. Toronto: University of Toronto Press.
Shroff, F. M. (2001). Forget Reform--We Want a Revolution! Women and Holistic Care. In D. Gustafsen (Ed.) Care and Consequences. Halifax, NS: Fernwood Books.
Smith, D. (2003). Maternal-Child Health Care in Aboriginal Communities. Canadian Journal of Nursing Research, 35, 143-152.
Statistics Canada (2006). First Nations people: Diverse, fast-growing population; 2006 Census sub-module. Ottawa, ON: Author.
Stebo, A. (2008). Birth Centre Care: Relevant for Rural B.C. Aboriginal Women? Paper completed as part of the requirements for a midwifery undergraduate degree at the Vancouver, BC: University of British Columbia.
Sutherns, R., MacPhedran, M., & Margaret Haworth-Brockman (2003). Rural, Remote and Northern Women’s Health: Policy and Research Directions Final Summary and Report. Ottawa, ON: Centres of Excellence for Women’s Health. http://www.pwhce.ca/pdf/rr/RRN_ExecSummE.pdf
Society of Obstetricians and Gynecologists (2003). http://www.sogc.org/guidelines/public/126E-PS-March2003.pdf
Society of Obstetricians and Gynecologists (2007). A Report on Best Practices for Returning Birth to Rural and Remote Aboriginal Communities. Ottawa, ON: Author.
Statistics Canada (2008). Aboriginal Peoples in Canada in 2006: Inuit, Métis and First Nations, 2006 Census. Ottawa, ON: Author.
Statistics Canada (2005). Canada’s Aboriginal population in 2017. http://www.statcan.gc.ca/daily-quotidien/050628/dq050628d-eng.htm
Statistics Canada (2003). Statistics Canada 2001 census: Aboriginal share of total population on the rise. http://www12.statcan.ca/english/census01/Products/Analytic/companion/abor/canada.cfm
Tedford Gold, S., O’Neil, J., & Van Wagner, V. (2005). Examining Midwifery-based Options to Improve Continuity of Maternity Care Services in Remote Nunavut Communities. www.chrsf.ca
Tritten, J. (1998). Freedom. Paths to Becoming a Midwife: Getting an Education. Midwifery Today, 105, 67–118.

28
Turia, T. (2000). Speech to the New Zealand College of Midwives National Midwifery Conference. http://www.beehive.govt.nz/speech/speech+new+zealand+college+midwives+national+midwifery+conference
Tupara, H. N. T., & Ihimaera, L. V. (2004). In the Context of Midwifery Practice: Recognition and Management of Mental Health. Palmerston North, New Zealand: Te Rau Matatini,
UNICEF (2008). Progress for Children: a report card on maternal mortality. http://www.un.org/apps/news/story.asp?NewsID=28119&Cr=Maternal&Cr1=Mortality
United Nations (1948). The Universal Declaration of Human Rights. Adopted and proclaimed by General Assembly resolution 217 A (III) of 10 December 1948. http://www.un.org/Overview/rights.html
Wenman, W. M., Joffres, M. R., Tataryn, I. V., & The Edmonton Perinatal Infections Group (2004). A prospective cohort study of pregnancy risk factors and birth outcomes in Aboriginal women. Canadian Medical Association Journal, 171, 585–589.
Whynot, E. (2004). Fewer family doctors delivering babies: CBC News report. http://www.cbc.ca/health/story/2004/04/21/babies040421.html
World Health Organization (1948). Constitution http://www.who.int/governance/eb/constitution/en/index.html
World Health Organization (2008). Health and Human Rights. http://www.who.int/hhr/HHRETH_activities.pdf