blue cross and blue shield of oklahoma - outline of
TRANSCRIPT

1
Outline of Medicare Supplement Coverage — Standard Benefits for Plan A, Plan F, High Deductible Plan F 1, Plan G, High Deductible Plan G 1, Plan N, and Blue Plan65 Select SM 2 Benefits for Plan F, Plan G, and Plan N
This chart shows the benefits included in each of the standard Medicare supplement plans. Every company must make Plan “A” available. Only applicants first eligible
for Medicare before 2020 may purchase Plans C, F, and high deductible F.
Blue Cross and Blue Shield of Oklahoma does not offer those plans shaded in gray below.
BASIC BENEFITS:• Hospitalization – Part A coinsurance plus coverage for 365 additional days after Medicare benefits end.
• Medical Expenses – Part B coinsurance (generally 20% of Medicare-approved expenses), or copayments for hospital outpatient services. Plans K, L and N require insureds to pay a portion of Part B coinsurance or copayments.
• Blood – First 3 pints of blood each year.
• Hospice – Part A coinsurance.
A Basic Benefits, including 100% Part B Coinsurance
B Basic Benefits, including 100% Part B Coinsurance
Part A Deductible
D Basic Benefits, including 100% Part B Coinsurance
Skilled Nursing Facility
Coinsurance
Part A Deductible
Foreign Travel
Emergency
G Basic Benefits, including 100% Part B Coinsurance
Skilled Nursing Facility
Coinsurance
Part A Deductible
Part B Excess (100%)
Foreign Travel
EmergencyG 1
KHospitalization and preventive
care paid at 100%; other basic benefits paid at 50%
50% Skilled Nursing Facility
Coinsurance
50% Part A
Deductible
Out-of-pocket limit $6,220; paid
at 100% after limit reached
LHospitalization and preventive
care paid at 100%; other basic benefits paid at 75%
75% Skilled Nursing Facility
Coinsurance
75% Part A
Deductible
Out-of-pocket limit $3,110; paid
at 100% after limit reached
M Basic Benefits, including 100% Part B Coinsurance
Skilled Nursing Facility
Coinsurance
50% Part A
Deductible
Foreign Travel
Emergency
NBasic Benefits, including
100% Part B coinsurance, except up to $20 copayment
for office visit, and up to $50 copayment for ER
Skilled Nursing Facility
Coinsurance
Part A Deductible
Foreign Travel
Emergency
Only available if Medicare-eligible before 2020
C Basic Benefits, including 100% Part B Coinsurance
Skilled Nursing Facility
Coinsurance
Part A Deductible
Part B Deductible
Foreign Travel
Emergency
F Basic Benefits, including 100% Part B Coinsurance 1
Skilled Nursing Facility
Coinsurance
Part A Deductible
Part B Deductible
Part B Excess (100%)
Foreign Travel
EmergencyF 1
OKMSOOC REV 01/21 607585.1220 OK
2
1 These high deductible plans pay the same benefits as Plans F and G after one has paid a calendar-year $2,370 deductible. Benefits from High Deductible Plans F and G will not begin until out-of-pocket expenses are $2,370. Out-of-pocket expenses for these deductibles are expenses that would ordinarily be paid by the policy. This includes the Medicare deductibles for Part A and Part B, but does not include the plan’s separate foreign travel emergency deductible.
2 Blue Plan65 Select Plans require that you use a Blue Plan65 Select network hospital for non-emergency admissions to receive coverage for the Medicare Part A deductible. In an emergency, the $1,484 deductible is covered at any hospital from which you receive care. Only certain hospitals are network providers under this policy. Check with your physician to determine if he or she has admitting privileges at the network hospital. If he or she does not, you may be required to use another physician at time of hospitalization or you will be required to pay for all expenses. If an insured moves out of the service area, there will be a reduction of benefit coverage and they will have the opportunity to purchase any Medicare Supplement policy with comparable or lesser benefits offered by the insurer, or Medicare Supplement/Select plans A, B, C, F, K, or L from any insurer within 63 days of termination.

3
Monthly Premium Rates effective January 1, 2021
Age 65 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $155.14 $141.04 N/A N/A $171.83 $156.22 N/A N/A
F $172.47 $156.79 $156.95 $142.68 $191.02 $173.66 $173.84 $158.04
High F 1 $39.46 $35.88 N/A N/A $43.72 $39.74 N/A N/A
G $125.80 $114.36 $110.94 $100.85 $141.03 $128.20 $124.37 $113.06
High G 1 $36.20 $32.92 N/A N/A $40.11 $36.45 N/A N/A
N $106.52 $96.84 $96.93 $88.12 $119.42 $108.56 $108.67 $98.79
Age 66 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $162.48 $147.71 N/A N/A $179.96 $163.60 N/A N/A
F $180.63 $164.21 $164.37 $149.43 $200.07 $181.88 $182.06 $165.51
High F 1 $41.33 $37.58 N/A N/A $45.79 $41.63 N/A N/A
G $132.49 $120.45 $116.84 $106.22 $148.45 $134.95 $130.90 $119.00
High G 1 $37.92 $34.47 N/A N/A $42.01 $38.19 N/A N/A
N $112.19 $101.99 $102.09 $92.81 $125.69 $114.27 $114.38 $103.99
Age 67 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $169.82 $154.39 N/A N/A $188.09 $170.99 N/A N/A
F $188.79 $171.63 $171.80 $156.18 $209.10 $190.10 $190.28 $172.99
High F 1 $43.20 $39.27 N/A N/A $47.85 $43.50 N/A N/A
G $139.20 $126.54 $122.75 $111.59 $155.86 $141.70 $137.45 $124.95
High G 1 $39.63 $36.03 N/A N/A $43.89 $39.92 N/A N/A
N $117.86 $107.15 $107.25 $97.50 $131.98 $119.98 $120.11 $109.18

4
Age 68 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $177.16 $161.06 N/A N/A $196.22 $178.39 N/A N/A
F $196.95 $179.05 $179.22 $162.93 $218.14 $198.31 $198.51 $180.47
High F 1 $45.07 $40.98 N/A N/A $49.92 $45.38 N/A N/A
G $145.89 $132.63 $128.65 $116.95 $163.28 $148.44 $143.99 $130.90
High G 1 $41.34 $37.60 N/A N/A $45.79 $41.63 N/A N/A
N $123.53 $112.30 $112.41 $102.19 $138.26 $125.69 $125.82 $114.38
Age 69 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $184.51 $167.73 N/A N/A $204.36 $185.78 N/A N/A
F $205.11 $186.47 $186.65 $169.68 $227.18 $206.53 $206.74 $187.94
High F 1 $46.93 $42.67 N/A N/A $51.99 $47.26 N/A N/A
G $152.58 $138.71 $134.56 $122.32 $170.70 $155.18 $150.53 $136.85
High G 1 $43.06 $39.15 N/A N/A $47.69 $43.36 N/A N/A
N $129.20 $117.45 $117.58 $106.89 $144.54 $131.40 $131.53 $119.57
Age 70 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $191.84 $174.40 N/A N/A $212.49 $193.17 N/A N/A
F $213.27 $193.89 $194.08 $176.44 $236.22 $214.74 $214.96 $195.42
High F 1 $48.80 $44.37 N/A N/A $54.06 $49.15 N/A N/A
G $159.28 $144.80 $140.46 $127.69 $178.11 $161.92 $157.07 $142.80
High G 1 $44.78 $40.70 N/A N/A $49.60 $45.09 N/A N/A
N $134.87 $122.61 $122.74 $111.58 $150.82 $137.11 $137.25 $124.77
5
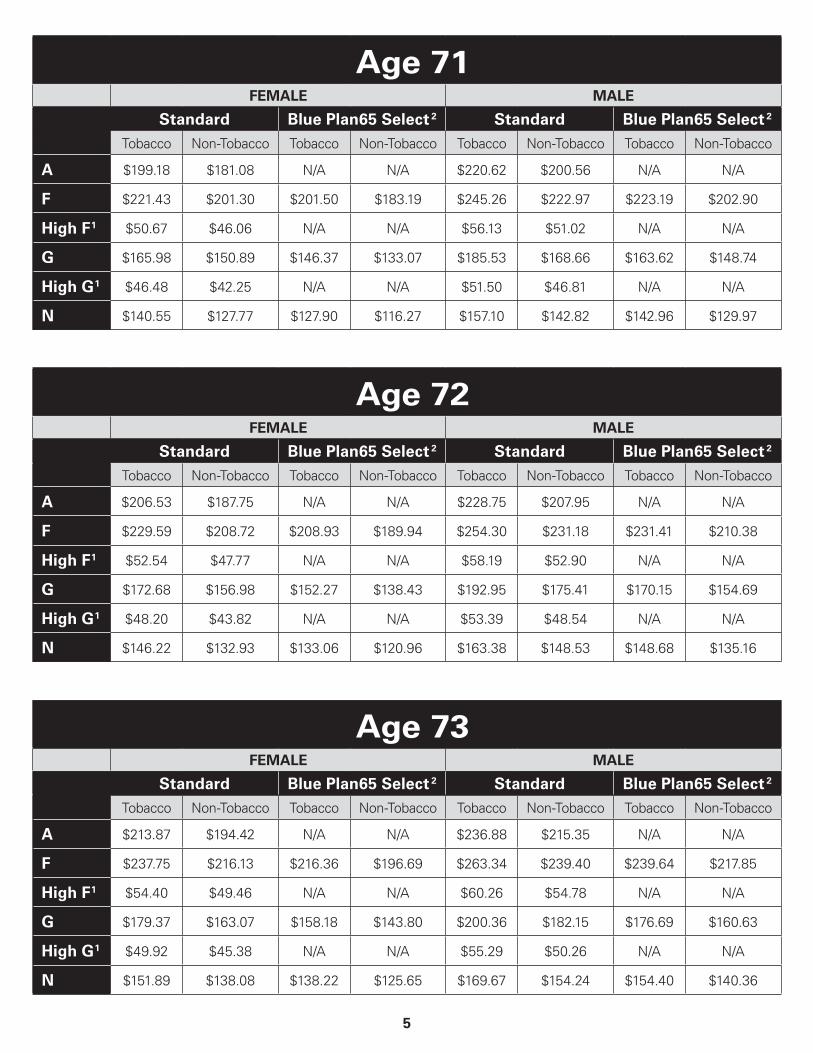
Age 71 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $199.18 $181.08 N/A N/A $220.62 $200.56 N/A N/A
F $221.43 $201.30 $201.50 $183.19 $245.26 $222.97 $223.19 $202.90
High F 1 $50.67 $46.06 N/A N/A $56.13 $51.02 N/A N/A
G $165.98 $150.89 $146.37 $133.07 $185.53 $168.66 $163.62 $148.74
High G 1 $46.48 $42.25 N/A N/A $51.50 $46.81 N/A N/A
N $140.55 $127.77 $127.90 $116.27 $157.10 $142.82 $142.96 $129.97
Age 72 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $206.53 $187.75 N/A N/A $228.75 $207.95 N/A N/A
F $229.59 $208.72 $208.93 $189.94 $254.30 $231.18 $231.41 $210.38
High F 1 $52.54 $47.77 N/A N/A $58.19 $52.90 N/A N/A
G $172.68 $156.98 $152.27 $138.43 $192.95 $175.41 $170.15 $154.69
High G 1 $48.20 $43.82 N/A N/A $53.39 $48.54 N/A N/A
N $146.22 $132.93 $133.06 $120.96 $163.38 $148.53 $148.68 $135.16
Age 73 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $213.87 $194.42 N/A N/A $236.88 $215.35 N/A N/A
F $237.75 $216.13 $216.36 $196.69 $263.34 $239.40 $239.64 $217.85
High F 1 $54.40 $49.46 N/A N/A $60.26 $54.78 N/A N/A
G $179.37 $163.07 $158.18 $143.80 $200.36 $182.15 $176.69 $160.63
High G 1 $49.92 $45.38 N/A N/A $55.29 $50.26 N/A N/A
N $151.89 $138.08 $138.22 $125.65 $169.67 $154.24 $154.40 $140.36

6
Age 74 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $221.20 $201.10 N/A N/A $245.01 $222.73 N/A N/A
F $245.91 $223.55 $223.78 $203.44 $272.38 $247.62 $247.86 $225.33
High F 1 $56.27 $51.16 N/A N/A $62.33 $56.67 N/A N/A
G $186.07 $169.15 $164.09 $149.17 $207.78 $188.90 $183.23 $166.58
High G 1 $51.62 $46.93 N/A N/A $57.18 $51.99 N/A N/A
N $157.56 $143.23 $143.37 $130.35 $175.94 $159.95 $160.11 $145.55
Age 75 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $228.55 $207.77 N/A N/A $253.14 $230.13 N/A N/A
F $254.07 $230.97 $231.21 $210.19 $281.42 $255.83 $256.08 $232.81
High F 1 $58.14 $52.86 N/A N/A $64.40 $58.55 N/A N/A
G $192.77 $175.24 $169.99 $154.54 $215.20 $195.64 $189.78 $172.53
High G 1 $53.34 $48.50 N/A N/A $59.08 $53.71 N/A N/A
N $163.23 $148.39 $148.53 $135.03 $182.22 $165.66 $165.82 $150.75
Age 76 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $235.89 $214.44 N/A N/A $261.27 $237.52 N/A N/A
F $262.24 $238.39 $238.64 $216.94 $290.45 $264.05 $264.32 $240.28
High F 1 $60.01 $54.56 N/A N/A $66.47 $60.42 N/A N/A
G $199.46 $181.33 $175.89 $159.90 $222.62 $202.38 $196.32 $178.47
High G 1 $55.06 $50.05 N/A N/A $60.98 $55.44 N/A N/A
N $168.89 $153.54 $153.69 $139.72 $188.51 $171.37 $171.54 $155.95

7
Age 77 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $243.23 $221.12 N/A N/A $269.40 $244.92 N/A N/A
F $270.40 $245.81 $246.06 $223.70 $299.50 $272.26 $272.54 $247.76
High F 1 $61.87 $56.25 N/A N/A $68.53 $62.30 N/A N/A
G $206.15 $187.41 $181.81 $165.27 $230.04 $209.12 $202.86 $184.42
High G 1 $56.76 $51.60 N/A N/A $62.88 $57.15 N/A N/A
N $174.56 $158.70 $158.85 $144.41 $194.79 $177.08 $177.26 $161.14
Age 78 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $250.57 $227.79 N/A N/A $277.53 $252.30 N/A N/A
F $278.56 $253.23 $253.49 $230.45 $308.53 $280.49 $280.77 $255.24
High F 1 $63.74 $57.95 N/A N/A $70.60 $64.19 N/A N/A
G $212.86 $193.51 $187.71 $170.64 $237.46 $215.86 $209.39 $190.36
High G 1 $58.48 $53.17 N/A N/A $64.78 $58.89 N/A N/A
N $180.23 $163.85 $164.02 $149.10 $201.06 $182.78 $182.97 $166.34
Age 79 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $257.91 $234.46 N/A N/A $285.66 $259.69 N/A N/A
F $286.72 $260.65 $260.92 $237.20 $317.57 $288.71 $288.99 $262.72
High F 1 $65.61 $59.65 N/A N/A $72.67 $66.07 N/A N/A
G $219.55 $199.59 $193.61 $176.02 $244.87 $222.61 $215.94 $196.31
High G 1 $60.19 $54.73 N/A N/A $66.68 $60.62 N/A N/A
N $185.91 $169.00 $169.18 $153.80 $207.35 $188.50 $188.69 $171.53

8
Age 80 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $265.25 $241.13 N/A N/A $293.79 $267.09 N/A N/A
F $294.88 $268.07 $268.34 $243.95 $326.61 $296.92 $297.21 $270.19
High F 1 $67.48 $61.35 N/A N/A $74.74 $67.94 N/A N/A
G $226.24 $205.68 $199.52 $181.38 $252.29 $229.36 $222.48 $202.26
High G 1 $61.91 $56.28 N/A N/A $68.57 $62.33 N/A N/A
N $191.58 $174.17 $174.34 $158.49 $213.63 $194.21 $194.40 $176.73
Age 81 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $272.60 $247.81 N/A N/A $301.92 $274.48 N/A N/A
F $303.04 $275.49 $275.77 $250.69 $335.65 $305.14 $305.44 $277.67
High F 1 $69.34 $63.04 N/A N/A $76.81 $69.83 N/A N/A
G $232.95 $211.77 $205.43 $186.75 $259.71 $236.10 $229.02 $208.20
High G 1 $63.62 $57.84 N/A N/A $70.46 $64.07 N/A N/A
N $197.25 $179.32 $179.50 $163.18 $219.91 $199.92 $200.11 $181.93
Age 82 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $279.93 $254.48 N/A N/A $310.06 $281.87 N/A N/A
F $311.20 $282.91 $283.20 $257.44 $344.68 $313.35 $313.67 $285.15
High F 1 $71.21 $64.74 N/A N/A $78.88 $71.71 N/A N/A
G $239.64 $217.85 $211.33 $192.12 $267.12 $242.84 $235.56 $214.15
High G 1 $65.33 $59.39 N/A N/A $72.36 $65.79 N/A N/A
N $202.92 $184.47 $184.66 $167.87 $226.19 $205.62 $205.84 $187.12

9
Age 83 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $287.27 $261.15 N/A N/A $318.19 $289.26 N/A N/A
F $319.36 $290.33 $290.61 $264.19 $353.73 $321.57 $321.90 $292.62
High F 1 $73.08 $66.44 N/A N/A $80.95 $73.59 N/A N/A
G $246.34 $223.94 $217.23 $197.48 $274.54 $249.58 $242.11 $220.09
High G 1 $67.05 $60.95 N/A N/A $74.26 $67.51 N/A N/A
N $208.59 $189.63 $189.81 $172.56 $232.47 $211.33 $211.55 $192.31
Age 84 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $294.62 $267.84 N/A N/A $326.32 $296.65 N/A N/A
F $327.52 $297.75 $298.04 $270.94 $362.77 $329.78 $330.12 $300.11
High F 1 $74.95 $68.14 N/A N/A $83.02 $75.47 N/A N/A
G $253.03 $230.04 $223.14 $202.85 $281.96 $256.32 $248.65 $226.04
High G 1 $68.76 $62.51 N/A N/A $76.16 $69.24 N/A N/A
N $214.26 $194.78 $194.97 $177.26 $238.75 $217.05 $217.26 $197.51
Age 85 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $301.96 $274.51 N/A N/A $334.45 $304.05 N/A N/A
F $335.68 $305.17 $305.47 $277.70 $371.80 $338.01 $338.34 $307.59
High F 1 $76.82 $69.83 N/A N/A $85.09 $77.35 N/A N/A
G $259.73 $236.12 $229.04 $208.22 $289.37 $263.06 $255.18 $231.98
High G 1 $70.47 $64.07 N/A N/A $78.07 $70.97 N/A N/A
N $219.93 $199.94 $200.13 $181.94 $245.03 $222.76 $222.98 $202.70
10
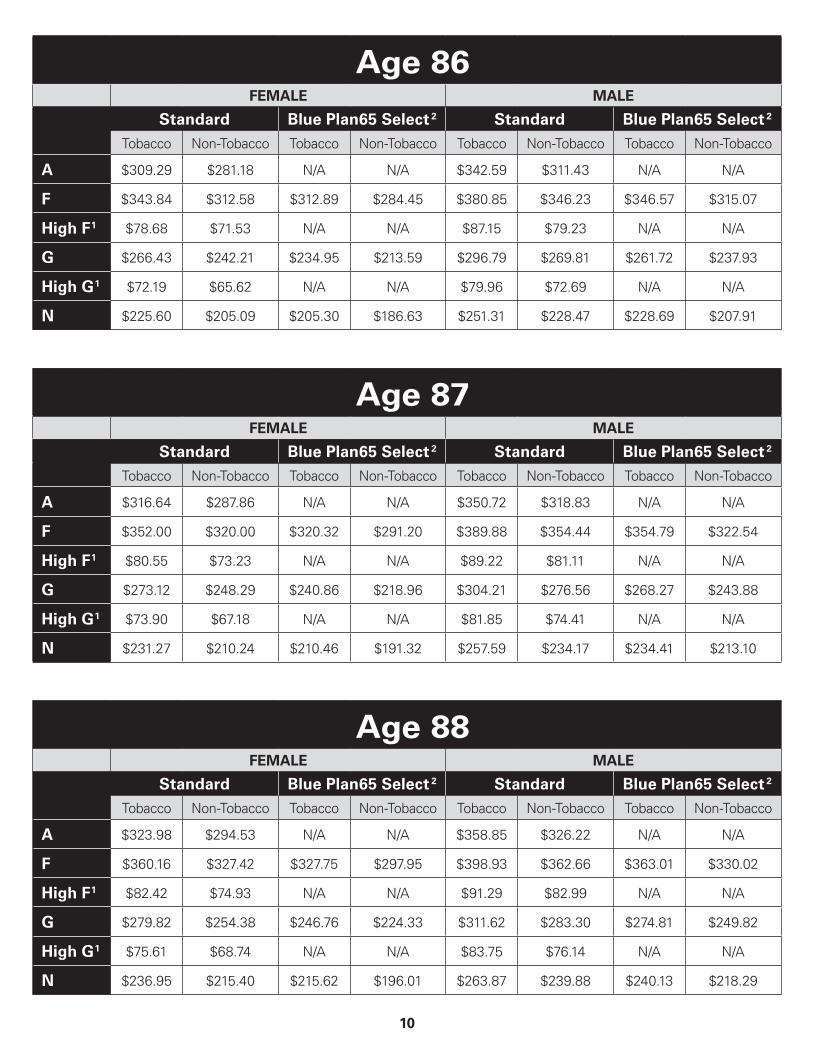
Age 86 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $309.29 $281.18 N/A N/A $342.59 $311.43 N/A N/A
F $343.84 $312.58 $312.89 $284.45 $380.85 $346.23 $346.57 $315.07
High F 1 $78.68 $71.53 N/A N/A $87.15 $79.23 N/A N/A
G $266.43 $242.21 $234.95 $213.59 $296.79 $269.81 $261.72 $237.93
High G 1 $72.19 $65.62 N/A N/A $79.96 $72.69 N/A N/A
N $225.60 $205.09 $205.30 $186.63 $251.31 $228.47 $228.69 $207.91
Age 87 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $316.64 $287.86 N/A N/A $350.72 $318.83 N/A N/A
F $352.00 $320.00 $320.32 $291.20 $389.88 $354.44 $354.79 $322.54
High F 1 $80.55 $73.23 N/A N/A $89.22 $81.11 N/A N/A
G $273.12 $248.29 $240.86 $218.96 $304.21 $276.56 $268.27 $243.88
High G 1 $73.90 $67.18 N/A N/A $81.85 $74.41 N/A N/A
N $231.27 $210.24 $210.46 $191.32 $257.59 $234.17 $234.41 $213.10
Age 88 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $323.98 $294.53 N/A N/A $358.85 $326.22 N/A N/A
F $360.16 $327.42 $327.75 $297.95 $398.93 $362.66 $363.01 $330.02
High F 1 $82.42 $74.93 N/A N/A $91.29 $82.99 N/A N/A
G $279.82 $254.38 $246.76 $224.33 $311.62 $283.30 $274.81 $249.82
High G 1 $75.61 $68.74 N/A N/A $83.75 $76.14 N/A N/A
N $236.95 $215.40 $215.62 $196.01 $263.87 $239.88 $240.13 $218.29

11
Age 89 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $331.32 $301.20 N/A N/A $366.98 $333.62 N/A N/A
F $368.32 $334.84 $335.17 $304.70 $407.96 $370.87 $371.25 $337.50
High F 1 $84.29 $76.62 N/A N/A $93.36 $84.87 N/A N/A
G $286.52 $260.47 $252.66 $229.70 $319.04 $290.04 $281.35 $255.77
High G 1 $77.33 $70.30 N/A N/A $85.65 $77.87 N/A N/A
N $242.62 $220.55 $220.78 $200.71 $270.16 $245.60 $245.84 $223.49
Age 90 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $338.66 $307.87 N/A N/A $375.11 $341.00 N/A N/A
F $376.48 $342.26 $342.60 $311.45 $417.00 $379.09 $379.47 $344.97
High F 1 $86.15 $78.33 N/A N/A $95.43 $86.75 N/A N/A
G $293.21 $266.56 $258.58 $235.07 $326.46 $296.78 $287.89 $261.71
High G 1 $79.04 $71.86 N/A N/A $87.55 $79.59 N/A N/A
N $248.28 $225.72 $225.94 $205.40 $276.43 $251.31 $251.55 $228.68
Age 91 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $346.00 $314.55 N/A N/A $383.24 $348.39 N/A N/A
F $384.64 $349.68 $350.02 $318.20 $426.04 $387.30 $387.70 $352.45
High F 1 $88.02 $80.02 N/A N/A $97.49 $88.63 N/A N/A
G $299.91 $272.65 $264.48 $240.43 $333.87 $303.52 $294.43 $267.67
High G 1 $80.75 $73.42 N/A N/A $89.44 $81.32 N/A N/A
N $253.95 $230.87 $231.10 $210.09 $282.71 $257.01 $257.27 $233.89

12
Age 92 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $353.34 $321.22 N/A N/A $391.37 $355.79 N/A N/A
F $392.81 $357.10 $357.45 $324.96 $435.08 $395.53 $395.92 $359.93
High F 1 $89.89 $81.72 N/A N/A $99.56 $90.51 N/A N/A
G $306.61 $278.73 $270.38 $245.80 $341.29 $310.26 $300.97 $273.62
High G 1 $82.47 $74.97 N/A N/A $91.34 $83.03 N/A N/A
N $259.62 $236.02 $236.25 $214.78 $289.00 $262.72 $262.99 $239.08
Age 93 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $360.69 $327.89 N/A N/A $399.50 $363.18 N/A N/A
F $400.97 $364.52 $364.88 $331.71 $444.11 $403.75 $404.14 $367.41
High F 1 $91.76 $83.41 N/A N/A $101.63 $92.40 N/A N/A
G $313.30 $284.82 $276.28 $251.17 $348.72 $317.01 $307.51 $279.56
High G 1 $84.18 $76.52 N/A N/A $93.24 $84.77 N/A N/A
N $265.29 $241.18 $241.41 $219.47 $295.28 $268.43 $268.70 $244.27
Age 94 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $368.02 $334.57 N/A N/A $407.63 $370.56 N/A N/A
F $409.13 $371.94 $372.30 $338.46 $453.16 $411.96 $412.37 $374.88
High F 1 $93.62 $85.12 N/A N/A $103.70 $94.27 N/A N/A
G $320.00 $290.91 $282.20 $256.54 $356.13 $323.76 $314.05 $285.51
High G 1 $85.89 $78.09 N/A N/A $95.14 $86.49 N/A N/A
N $270.96 $246.33 $246.57 $224.17 $301.55 $274.15 $274.42 $249.47

13
Age 95 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $375.36 $341.24 N/A N/A $415.76 $377.96 N/A N/A
F $417.29 $379.36 $379.73 $345.21 $462.19 $420.18 $420.60 $382.36
High F 1 $95.49 $86.81 N/A N/A $105.77 $96.15 N/A N/A
G $326.70 $296.99 $288.10 $261.91 $363.55 $330.50 $320.60 $291.45
High G 1 $87.61 $79.65 N/A N/A $97.04 $88.21 N/A N/A
N $276.63 $251.49 $251.74 $228.86 $307.84 $279.86 $280.13 $254.66
Age 96 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $382.71 $347.91 N/A N/A $423.89 $385.35 N/A N/A
F $425.45 $386.78 $387.16 $351.96 $471.23 $428.39 $428.83 $389.84
High F 1 $97.36 $88.51 N/A N/A $107.83 $98.04 N/A N/A
G $333.39 $303.09 $294.00 $267.28 $370.97 $337.24 $327.14 $297.40
High G 1 $89.32 $81.20 N/A N/A $98.93 $89.95 N/A N/A
N $282.31 $256.64 $256.90 $233.54 $314.12 $285.56 $285.84 $259.87
Age 97 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $390.05 $354.59 N/A N/A $432.02 $392.75 N/A N/A
F $433.61 $394.20 $394.58 $358.71 $480.28 $436.61 $437.05 $397.32
High F 1 $99.23 $90.20 N/A N/A $109.90 $99.92 N/A N/A
G $340.09 $309.17 $299.91 $272.65 $378.38 $343.98 $333.68 $303.34
High G 1 $91.03 $82.76 N/A N/A $100.83 $91.67 N/A N/A
N $287.98 $261.79 $262.06 $238.23 $320.40 $291.27 $291.57 $265.06
14
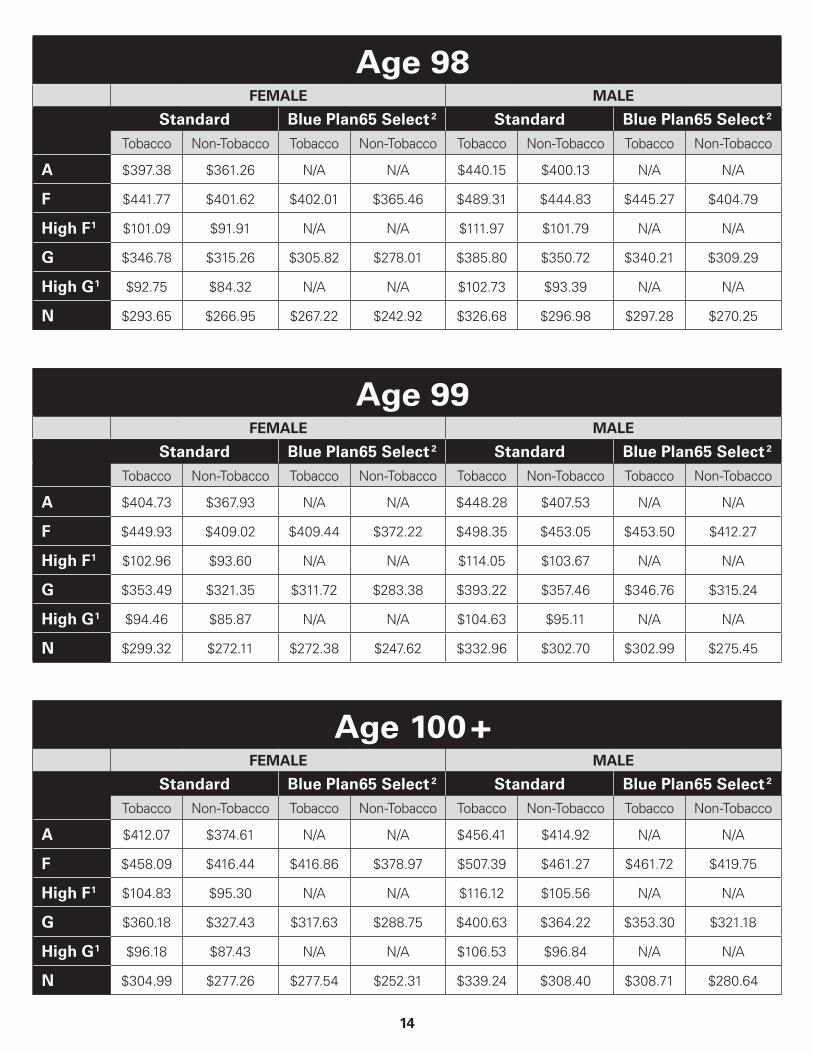
Age 98 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $397.38 $361.26 N/A N/A $440.15 $400.13 N/A N/A
F $441.77 $401.62 $402.01 $365.46 $489.31 $444.83 $445.27 $404.79
High F 1 $101.09 $91.91 N/A N/A $111.97 $101.79 N/A N/A
G $346.78 $315.26 $305.82 $278.01 $385.80 $350.72 $340.21 $309.29
High G 1 $92.75 $84.32 N/A N/A $102.73 $93.39 N/A N/A
N $293.65 $266.95 $267.22 $242.92 $326.68 $296.98 $297.28 $270.25
Age 99 FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $404.73 $367.93 N/A N/A $448.28 $407.53 N/A N/A
F $449.93 $409.02 $409.44 $372.22 $498.35 $453.05 $453.50 $412.27
High F 1 $102.96 $93.60 N/A N/A $114.05 $103.67 N/A N/A
G $353.49 $321.35 $311.72 $283.38 $393.22 $357.46 $346.76 $315.24
High G 1 $94.46 $85.87 N/A N/A $104.63 $95.11 N/A N/A
N $299.32 $272.11 $272.38 $247.62 $332.96 $302.70 $302.99 $275.45
Age 100 + FEMALE MALE
Standard Blue Plan65 Select 2 Standard Blue Plan65 Select 2
Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco Tobacco Non-Tobacco
A $412.07 $374.61 N/A N/A $456.41 $414.92 N/A N/A
F $458.09 $416.44 $416.86 $378.97 $507.39 $461.27 $461.72 $419.75
High F 1 $104.83 $95.30 N/A N/A $116.12 $105.56 N/A N/A
G $360.18 $327.43 $317.63 $288.75 $400.63 $364.22 $353.30 $321.18
High G 1 $96.18 $87.43 N/A N/A $106.53 $96.84 N/A N/A
N $304.99 $277.26 $277.54 $252.31 $339.24 $308.40 $308.71 $280.64
15
You have the option to purchase any of the Medicare Supplement benefit plans shown on the front cover in white as Standard Plans or as Blue Plan65 Select Plans, with the exception of Plan A, High Deductible Plan F 1, and High Deductible Plan G 1. Those plans are available as Standard Plans only.
Blue Plan65 Select Plans require that you use a Blue Plan65 Select network hospital for non-emergency admissions to receive coverage for the Medicare Part A deductible. In an emergency, the $1,484 deductible is covered at any hospital from which you receive care. Only certain hospitals are network providers under this policy. Check with your physician to determine if he or she has admitting privileges at the network hospital. If he or she does not, you may be required to use another physician at time of hospitalization or you will be required to pay for all expenses. If you move out of the service area, there will be a reduction of benefit coverage and you will have the opportunity to purchase any Medicare Supplement policy with comparable or lesser benefits offered by the insurer, or Medicare Supplement/Select plans A, B, C, F, K, or L from any insurer within 63 days of termination.
PREMIUM INFORMATIONBlue Cross and Blue Shield of Oklahoma can only raise your premium if we raise the premium for all policies like yours in the state. We will not change your premium or cancel your policy because of poor health. Premiums change at age 65 and every year thereafter up to age 100. If your premium changes, you will be notified at least 30 days in advance.
Gender
One factor that will determine your premium is your gender. When completing the application, you will need to make a gender selection.
Household Discount
You may be eligible for a discount if you and another individual residing in your household are both enrolled in a Blue Cross and Blue Shield of Oklahoma Medicare Supplement Insurance Plan effective on or after May 1, 2019.
Tobacco User
A Tobacco User is a person who is permitted under state and federal law to legally use Tobacco, with Tobacco use (other than religious or ceremonial use of Tobacco) occurring on average of four or more times per week that last occurred within the past six months. Tobacco products include but are not limited to: cigarettes, cigars, smokeless tobacco products, electronic cigarettes, dissolvable tobacco products, vaping, etc.
If you meet the definition of a Tobacco User, you may pay a higher premium for your health coverage.
16
DISCLOSURESUse this outline to compare benefits and premiums among policies.
READ YOUR POLICY VERY CAREFULLYThis is only an outline describing your policy’s most important features. The policy is your insurance contract. You must read the policy itself to understand all of the rights and duties of both you and your insurance company.
RIGHT TO RETURN YOUR POLICYIf you find that you are not satisfied with your policy, you may return it to Blue Medicare Supplement c/o Member Services, P.O. Box 3388 Scranton, PA 18505. If you send the policy back to us within 30 days after you receive it, we will treat the policy as if it had never been issued and will return all of your payments.
POLICY REPLACEMENTIf you are replacing another health insurance policy, do NOT cancel it until you have actually received your new policy and are sure you want to keep it.
NOTICEThis policy may not fully cover all of your medical costs. Neither Blue Cross and Blue Shield of Oklahoma nor its agents are connected with Medicare. This Outline of Coverage does not give you all the details of Medicare coverage. Contact your local Social Security Office or consult “Medicare & You” for more details.
COMPLETE ANSWERS ARE VERY IMPORTANTReview the application carefully before you sign it. Be certain that all information has been properly recorded.

17
ADDITIONAL DISCLOSURES FOR BLUE PLAN65 SELECT
YOUR BLUE PLAN65 SELECT NETWORK PROVIDERBy choosing Blue Plan65 Select as your Medicare Supplement, you are agreeing to receive services from a Blue Plan65 Select Network Provider in order to receive the highest level of benefits. For the most updated list of our Blue Plan65 Select Network Providers please visit our Web site at bcbsok.com. If you receive Covered Services from an Out-of-Network Provider, and the services were available from a Blue Plan65 Select Network Provider, those services will be reimbursed at a lower level of benefits, except for Emergency Care.
RESTRICTED BLUE PLAN65 SELECT NETWORK PROVIDER PROVISIONSIf you receive non-emergency services from a Provider other than a Blue Plan65 Select Network Provider, coverage for the supplemental portion of the Medicare services will be reduced as follows:
• No coverage will be provided for the Medicare Part A Deductible amount (the first $1,484 of the Medicare Approved Amounts). You will be responsible for this amount.
• No coverage will be provided for the Medicare Part A Coinsurance amount for the 21st through 100th days in a post-hospital Skilled Nursing Facility. You will be responsible for this amount.
• No coverage will be provided for the Medicare Part B Deductible Amount (the first $203 of the Medicare Approved Amounts). You will be responsible for this amount.
• No coverage will be provided for the difference between the actual Medicare Part B charge as billed, and the Medicare-approved Part B charge. You may be responsible for this difference if your Provider does not accept Medicare assignment.
COVERAGE FOR EMERGENCY CAREBenefits for Emergency Care, which are Medicare Eligible Expenses, will be provided at the Blue Plan65 Select Network level regardless of whether a Blue Plan65 Select Network Provider is used. This includes services which are immediately required for an unforeseen illness, injury or condition, and it is not reasonable to obtain the services through a Blue Plan65 Select Network Provider.
GRIEVANCE PROCEDURESBlue Cross and Blue Shield of Oklahoma is committed to providing quality, responsive administration of benefits and customer service to our Members. Our corporation provides dedicated customer service to Medicare Supplement Members. This service capability provides dedicated staff, dedicated telephone lines and dedicated toll-free telephone access.
Member inquiries with regard to claims payment, billing, coverage levels, benefit interpretation, network provider and other miscellaneous concerns are addressed by the dedicated customer service unit of our Customer Service Department in Tulsa, Oklahoma.
If your inquiry is not resolved through our dedicated customer service area to your satisfaction, a grievance procedure is in place to seek further review or clarification and is outlined in the Policy.
QUALITY ASSURANCEAll Blue Plan65 Select Network Providers are chosen based on specific written criteria and are periodically evaluated for quality of care provided. Processes are in place to initiate corrective action when warranted.
Blue Plan65 Select Network Providers are issued written criteria for retention in and removal from the network.
RIGHT TO PURCHASEYou have the right to apply for any Medicare Supplement Policy offered by Blue Cross and Blue Shield of Oklahoma as long as you live within 25 miles of a Blue Plan65 Select hospital. If you enroll under this Blue Plan65 Select Medicare Supplement Policy, you may change coverage to any Medicare Supplement Policy offering comparable or lesser benefits by giving 31 days written notice of exchange.
18
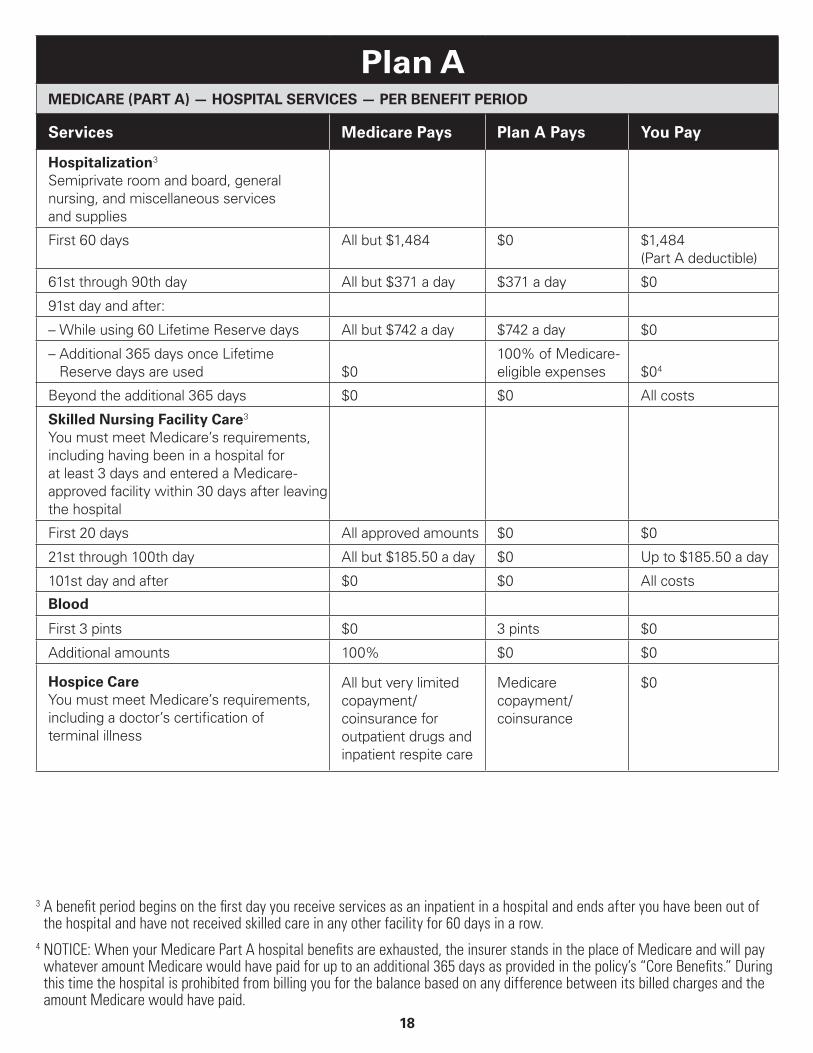
Plan AMEDICARE (PART A) — HOSPITAL SERVICES — PER BENEFIT PERIOD
Services Medicare Pays Plan A Pays You Pay
Hospitalization 3
Semiprivate room and board, general nursing, and miscellaneous services and supplies
First 60 days All but $1,484 $0 $1,484 (Part A deductible)
61st through 90th day All but $371 a day $371 a day $0
91st day and after:
– While using 60 Lifetime Reserve days All but $742 a day $742 a day $0
– Additional 365 days once Lifetime Reserve days are used $0
100% of Medicare- eligible expenses $0 4
Beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care 3
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0
21st through 100th day All but $185.50 a day $0 Up to $185.50 a day
101st day and after $0 $0 All costs
Blood
First 3 pints $0 3 pints $0
Additional amounts 100% $0 $0
Hospice CareYou must meet Medicare’s requirements, including a doctor’s certification of terminal illness
All but very limited copayment/coinsurance for outpatient drugs and inpatient respite care
Medicare copayment/ coinsurance
$0
3 A benefit period begins on the first day you receive services as an inpatient in a hospital and ends after you have been out of the hospital and have not received skilled care in any other facility for 60 days in a row.
4 NOTICE: When your Medicare Part A hospital benefits are exhausted, the insurer stands in the place of Medicare and will pay whatever amount Medicare would have paid for up to an additional 365 days as provided in the policy’s “Core Benefits.” During this time the hospital is prohibited from billing you for the balance based on any difference between its billed charges and the amount Medicare would have paid.

19
Plan AMEDICARE (PART B) — MEDICAL SERVICES — PER CALENDAR YEAR.
Services Medicare Pays Plan A Pays You Pay
Medical Expenses — In or Out of the Hospital and Outpatient Hospital Treatment, such as physicians’ services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts)
$0 $0 All costs
Blood
First 3 pints $0 All costs $0
Next $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts 80% 20% $0
Clinical Laboratory Services — Tests for Diagnostic Services
100% $0 $0
MEDICARE (PARTS A & B)
Services Medicare Pays Plan A Pays You Pay
Home Health Care Medicare-approved Services
Medically necessary skilled care services and medical supplies
100% $0 $0
Durable medical equipment
– First $203 of Medicare-approved amounts 5
$0 $0 $203 (Part B deductible)
– Remainder of Medicare-approved amounts
80% 20% $0
5 Once you have been billed $203 of Medicare-approved amounts for covered services, your Part B deductible will have been met for the calendar year.

20
Plan FMEDICARE (PART A) — HOSPITAL SERVICES — PER BENEFIT PERIOD
Services Medicare Pays Plan F Pays You Pay
Hospitalization 3
Semiprivate room and board, general nursing, and miscellaneous services and supplies
First 60 days All but $1,484 $1,484 (Part A deductible) 2
$0
61st through 90th day All but $371 a day $371 a day $0
91st day and after:
– While using 60 Lifetime Reserve days All but $742 a day $742 a day $0
– Additional 365 days once Lifetime Reserve days are used
$0 100% of Medicare- eligible expenses
$0 4
Beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care 3
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0
21st through 100th day All but $185.50 a day Up to $185.50 a day $0
101st day and after $0 $0 All costs
Blood
First 3 pints $0 3 pints $0
Additional amounts 100% $0 $0
Hospice CareYou must meet Medicare’s requirements, including a doctor’s certification of terminal illness
All but very limited copayment/coinsurance for outpatient drugs and inpatient respite care
Medicare copayment/ coinsurance
$0

21
Plan FMEDICARE (PART B) — MEDICAL SERVICES — PER CALENDAR YEAR
Services Medicare Pays Plan F Pays You Pay
Medical Expenses — In or Out of the Hospital and Outpatient Hospital Treatment, such as physicians’ services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $203 of Medicare-approved amounts 5 $0 $203 (Part B deductible) $0
Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts)
$0 100% $0
Blood
First 3 pints $0 All costs $0
Next $203 of Medicare-approved amounts 5 $0 $203 (Part B deductible) $0
Remainder of Medicare-approved amounts 80% 20% $0
Clinical Laboratory Services — Tests for Diagnostic Services
100% $0 $0
MEDICARE (PARTS A & B)
Services Medicare Pays Plan F Pays You Pay
Home Health Care Medicare-approved Services
Medically necessary skilled care services and medical supplies
100% $0 $0
Durable medical equipment
– First $203 of Medicare-approved amounts 5 $0 $203 (Part B deductible) $0
– Remainder of Medicare-approved amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
Foreign Travel — Not Covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of charges $0 80% to a lifetime maximum benefit of $50,000
20% and amounts over the $50,000 lifetime maximum

22
High Deductible Plan FMEDICARE (PART A) — HOSPITAL SERVICES — PER BENEFIT PERIOD
Services Medicare PaysAfter You Pay $2,370 Deductible1, Plan F Pays
In Addition to $2,370 Deductible1, You Pay
Hospitalization 3
Semiprivate room and board, general nursing, and miscellaneous services and supplies
First 60 days All but $1,484 $1,484 (Part A deductible)
$0
61st through 90th day All but $371 a day $371 a day $0
91st day and after:
– While using 60 Lifetime Reserve days All but $742 a day $742 a day $0
– Additional 365 days once Lifetime Reserve days are used
$0 100% of Medicare- eligible expenses
$0 4
Beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care 3
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts
$0 $0
21st through 100th day All but $185.50 a day Up to $185.50 a day $0
101st day and after $0 $0 All costs
Blood
First 3 pints $0 3 pints $0
Additional amounts 100% $0 $0
Hospice CareYou must meet Medicare’s requirements, including a doctor’s certification of terminal illness
All but very limited copayment/coinsurance for outpatient drugs and inpatient respite care
Medicare copayment/ coinsurance
$0

23
High Deductible Plan FMEDICARE (PART B) — MEDICAL SERVICES — PER CALENDAR YEAR
Services Medicare PaysAfter You Pay $2,370 Deductible1, Plan F Pays
In Addition to $2,370 Deductible1, You Pay
Medical Expenses — In or Out of the Hospital and Outpatient Hospital Treatment, such as physicians’ services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $203 of Medicare-approved amounts 5 $0 $203 (Part B deductible) $0
Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts)
$0 100% $0
Blood
First 3 pints $0 All costs $0
Next $203 of Medicare-approved amounts 5 $0 $203 (Part B deductible) $0
Remainder of Medicare-approved amounts 80% 20% $0
Clinical Laboratory Services — Tests for Diagnostic Services
100% $0 $0
MEDICARE (PARTS A & B)
Services Medicare PaysAfter You Pay $2,370 Deductible1, Plan F Pays
In Addition to $2,370 Deductible1, You Pay
Home Health Care Medicare-approved Services
Medically necessary skilled care services and medical supplies
100% $0 $0
Durable medical equipment
– First $203 of Medicare-approved amounts 5 $0 $203 (Part B deductible) $0
– Remainder of Medicare-approved amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
Foreign Travel — Not Covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of charges $0 80% to a lifetime maximum benefit of $50,000
20% and amounts over the $50,000 lifetime maximum

24
Plan GMEDICARE (PART A) — HOSPITAL SERVICES — PER BENEFIT PERIOD
Services Medicare Pays Plan G Pays You Pay
Hospitalization 3
Semiprivate room and board, general nursing, and miscellaneous services and supplies
First 60 days All but $1,484 $1,484 (Part A deductible) 2
$0
61st through 90th day All but $371 a day $371 a day $0
91st day and after:
– While using 60 Lifetime Reserve days All but $742 a day $742 a day $0
– Additional 365 days once Lifetime Reserve days are used
$0 100% of Medicare- eligible expenses
$0 4
Beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care 3
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0
21st through 100th day All but $185.50 a day Up to $185.50 a day $0
101st day and after $0 $0 All costs
Blood
First 3 pints $0 3 pints $0
Additional amounts 100% $0 $0
Hospice CareYou must meet Medicare’s requirements, including a doctor’s certification of terminal illness
All but very limited copayment/coinsurance for outpatient drugs and inpatient respite care
Medicare copayment/ coinsurance
$0

25
Plan GMEDICARE (PART B) — MEDICAL SERVICES — PER CALENDAR YEAR
Services Medicare Pays Plan G Pays You Pay
Medical Expenses — In or Out of the Hospital and Outpatient Hospital Treatment, such as physicians’ services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts)
$0 100% $0
Blood
First 3 pints $0 All costs $0
Next $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts 80% 20% $0
Clinical Laboratory Services — Tests for Diagnostic Services
100% $0 $0
MEDICARE (PARTS A & B)
Services Medicare Pays Plan G Pays You Pay
Medically necessary skilled care services and medical supplies
100% $0 $0
Durable medical equipment
– First $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
– Remainder of Medicare-approved amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
Foreign Travel — Not Covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of charges $0 80% to a lifetime maximum benefit of $50,000
20% and amounts over the $50,000 lifetime maximum

26
High Deductible Plan GMEDICARE (PART A) — HOSPITAL SERVICES — PER BENEFIT PERIOD
Services Medicare PaysAfter You Pay $2,370 Deductible1, Plan G Pays
In Addition to $2,370 Deductible1, You Pay
Hospitalization 3
Semiprivate room and board, general nursing, and miscellaneous services and supplies
First 60 days All but $1,484 $1,484 (Part A deductible)
$0
61st through 90th day All but $371 a day $371 a day $0
91st day and after:
– While using 60 Lifetime Reserve days All but $742 a day $742 a day $0
– Additional 365 days once Lifetime Reserve days are used
$0 100% of Medicare- eligible expenses
$0 4
Beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care 3
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0
21st through 100th day All but $185.50 a day Up to $185.50 a day $0
101st day and after $0 $0 All costs
Blood
First 3 pints $0 3 pints $0
Additional amounts 100% $0 $0
Hospice CareYou must meet Medicare’s requirements, including a doctor’s certification of terminal illness
All but very limited copayment/coinsurance for outpatient drugs and inpatient respite care
Medicare copayment/ coinsurance
$0

27
High Deductible Plan GMEDICARE (PART B) — MEDICAL SERVICES — PER CALENDAR YEAR
Services Medicare PaysAfter You Pay $2,370 Deductible1, Plan G Pays
In Addition to $2,370 Deductible1, You Pay
Medical Expenses — In or Out of the Hospital and Outpatient Hospital Treatment, such as physicians’ services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts Generally 80% Generally 20% $0
Part B Excess Charges (above Medicare-approved amounts)
$0 100% $0
Blood
First 3 pints $0 All costs $0
Next $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts 80% 20% $0
Clinical Laboratory Services — Tests for Diagnostic Services
100% $0 $0
MEDICARE (PARTS A & B)
Services Medicare PaysAfter You Pay $2,370 Deductible1, Plan G Pays
In Addition to $2,370 Deductible1, You Pay
Medically necessary skilled care services and medical supplies
100% $0 $0
Durable medical equipment
– First $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
– Remainder of Medicare-approved amounts 80% 20% $0
OTHER BENEFITS – NOT COVERED BY MEDICARE
Foreign Travel — Not Covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of charges $0 80% to a lifetime maximum benefit of $50,000
20% and amounts over the $50,000 lifetime maximum

28
Plan NMEDICARE (PART A) — HOSPITAL SERVICES — PER BENEFIT PERIOD
Services Medicare Pays Plan N Pays You Pay
Hospitalization 3
Semiprivate room and board, general nursing, and miscellaneous services and supplies
First 60 days All but $1,484 $1,484 (Part A deductible) 2
$0
61st through 90th day All but $371 a day $371 a day $0
91st day and after:
– While using 60 Lifetime Reserve days All but $742 a day $742 a day $0
– Additional 365 days once Lifetime Reserve days are used
$0 100% of Medicare- eligible expenses
$0 4
Beyond the additional 365 days $0 $0 All costs
Skilled Nursing Facility Care 3
You must meet Medicare’s requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital
First 20 days All approved amounts $0 $0
21st through 100th day All but $185.50 a day Up to $185.50 a day $0
101st day and after $0 $0 All costs
Blood
First 3 pints $0 3 pints $0
Additional amounts 100% $0 $0
Hospice CareYou must meet Medicare’s requirements, including a doctor’s certification of terminal illness
All but very limited copayment/coinsurance for outpatient drugs and inpatient respite care
Medicare copayment/ coinsurance
$0

29
Plan NMEDICARE (PART B) — MEDICAL SERVICES — PER CALENDAR YEAR
Services Medicare Pays Plan N Pays You Pay
Medical Expenses — In or Out of the Hospital And Outpatient Hospital Treatment, such as physicians’ services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment
First $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts Generally 80% Balance, other than up to $20 per office visit and up to $50 per emergency room visit. The copayment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
Up to $20 per office visit and up to $50 per emergency room visit. The copayment of up to $50 is waived if the insured is admitted to any hospital and the emergency visit is covered as a Medicare Part A expense.
Part B Excess Charges (above Medicare-approved amounts)
$0 $0 All costs
Blood
First 3 pints $0 All costs $0
Next $203 of Medicare-approved amounts 5 $0 $0 $203 (Part B deductible)
Remainder of Medicare-approved amounts 80% 20% $0
Clinical Laboratory Services — Tests for Diagnostic Services
100% $0 $0
MEDICARE (PARTS A & B)
Services Medicare Pays Plan N Pays You Pay
Home Health Care Medicare-approved Services
Medically necessary skilled care services and medical supplies
100% $0 $0
Durable medical equipment
– First $203 of Medicare-approved amounts 5
$0 $0 $203 (Part B deductible)
– Remainder of Medicare-approved amounts
80% 20% $0

30
Plan NOTHER BENEFITS – NOT COVERED BY MEDICARE
Services Medicare Pays Plan N Pays You Pay
Foreign Travel — Not Covered by Medicare Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA
First $250 each calendar year $0 $0 $250
Remainder of charges $0 80% to a lifetime maximum benefit of $50,000
20% and amounts over the $50,000 lifetime maximum

31
Important Information about Quotes for Medicare Supplement Quoted prices are based on the criteria specified during your search. This illustration is subject to Blue Cross and Blue Shield of Oklahoma’s rating or underwriting and approval, as appropriate, and does not guarantee rates, coverage or effective date. Furthermore, rates are subject to change if any of the information you have provided changes when and if a policy is approved. In addition, Blue Cross and Blue Shield of Oklahoma reserves the right to change rates from time to time.
Medicare Supplement insurance plans are offered by Blue Cross and Blue Shield of Oklahoma, a Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association. Not connected with or endorsed by the U.S. Government or Federal Medicare Program.