bmi classification (kg/m 2 ) underweightbmi ≤ 18.49 normal weightbmi ≥ 18.5 to 24.9...
TRANSCRIPT

Morbid ObesityPresented by Erin McLean

Overview•Patient information•Disease background•Nutrition care process•Conclusion•Review of key points•Personal impressions

Patient Profile•Gender: Male• Age: 51• Ethnic background: Hispanic•Household situation: Patient bedbound at home, cared for by brother and sister, separated from wife, no children• Education: Not disclosed•Occupation: Not disclosed• Religion: Not disclosed• Admit date/discharge date: 01/25/14, 02/17/14
Reason for Hospital Admission
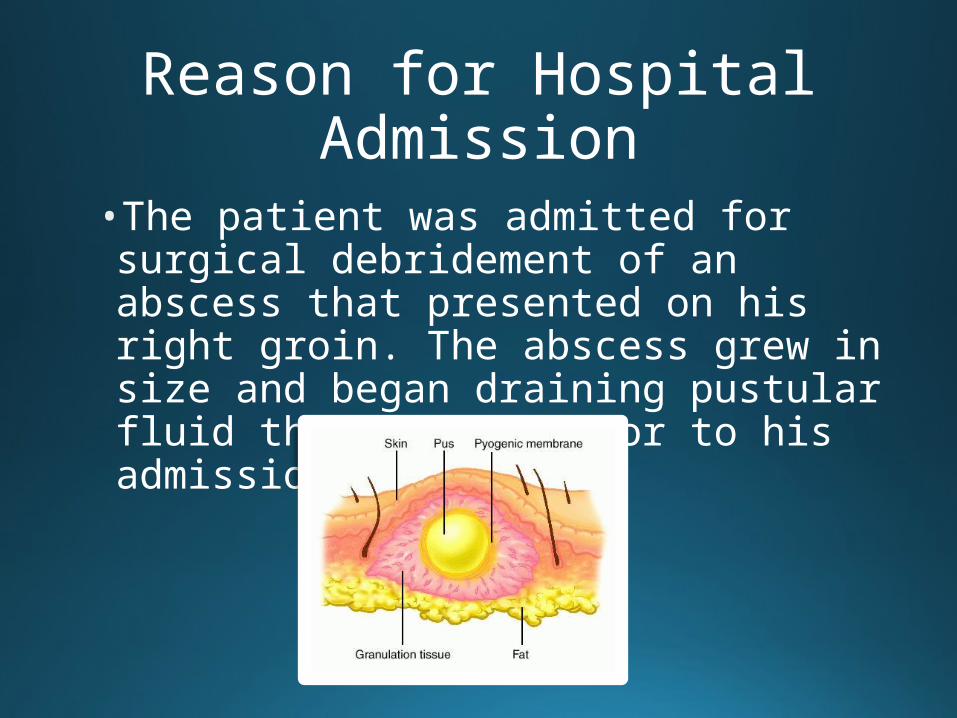
•The patient was admitted for surgical debridement of an abscess that presented on his right groin. The abscess grew in size and began draining pustular fluid three weeks prior to his admission.

Medical/Health/Family History
•Past medical history•Morbid obesity• Hypertension• Chronic lymphedema• Sleep apnea• Anxiety• Remote history of seizure disorder
•Past surgical history• Cholecystectomy• Gunshot wound repairment

Medical/Health/Family History
•Health history• Recent 91 kg weight loss PTA• Gross movement of extremities • Not using CPAP at night• No dental or swallowing issues• Some digestive issues• No eliminative issues• No history of alcohol of illicit drug abuse
• Family history• Positive for diabetes mellitus
Medical Diagnoses
•Groin abscess•Cellulitis•Morbid obesity•Diabetes mellitus•Acute respiratory failure•Urinary tract infection•Septic shock•Aspiration pneumonia•Acute kidney injury •Possible ischemic bowel
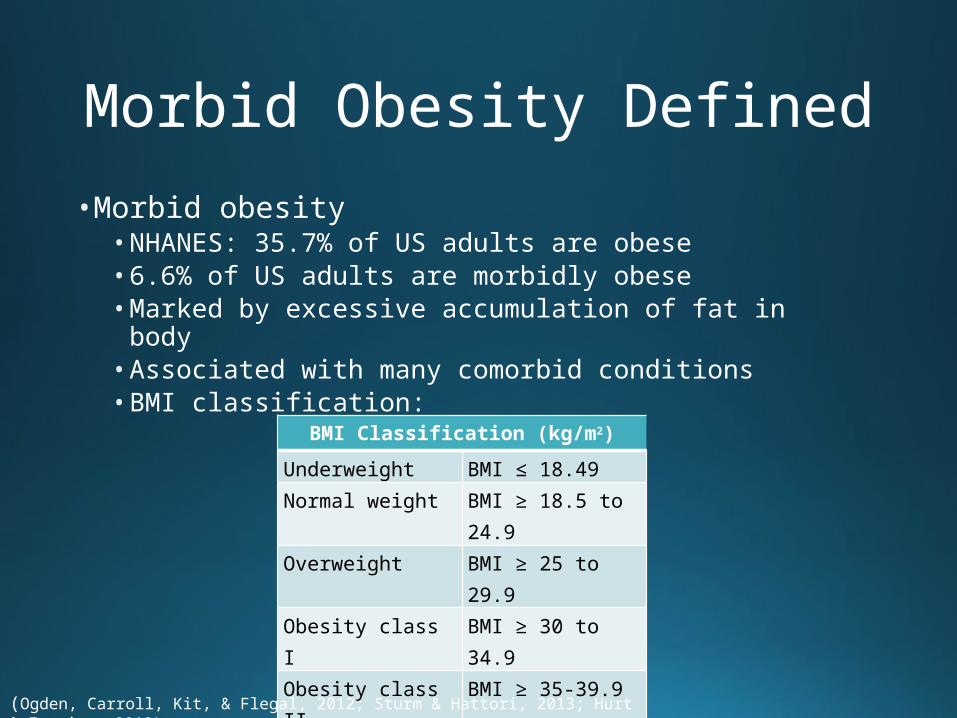
Morbid Obesity Defined•Morbid obesity• NHANES: 35.7% of US adults are obese• 6.6% of US adults are morbidly obese• Marked by excessive accumulation of fat in body• Associated with many comorbid conditions • BMI classification:
BMI Classification (kg/m2)
Underweight BMI ≤ 18.49
Normal weight BMI ≥ 18.5 to 24.9
Overweight BMI ≥ 25 to 29.9
Obesity class I BMI ≥ 30 to 34.9
Obesity class II BMI ≥ 35-39.9
Obesity class III BMI ≥ 40
(Ogden, Carroll, Kit, & Flegal, 2012; Sturm & Hattori, 2013; Hurt & Frazier, 2012)

Pathophysiology• Appetite regulation and weight management are influenced by the interplay between the CNS and hormones.• Leptin
• Simulates ↓ food intake and ↑ energy expenditure• Proportional to amount of total fat mass• Leptin resistance vs. leptin deficiency in obesity development
• Insulin• Involved in food intake regulation and production/storage of fat• Proportional to amount of total fat mass• Impaired insulin action → ↓ thermogenesis → ↑ adiposity
(Beckman, Beckman, & Earthman, 2010; Mahan, Escott-Stump, & Raymond, 2012)

Pathophysiology• Ghrelin
• Stimulates ↑ appetite• ↑ levels in normal-weight individuals, ↓ levels in obese individuals • Absent ↓ in post-prandial circulating levels in obese individuals
• Glucagon-like peptide (GLP-1)• Stimulates ↓ appetite, imparts satiety • ↑ levels in normal-weight individuals, ↓ levels in obese individuals
• Peptide YY (PYY)• Stimulates ↓ appetite, imparts satiety • ↑ levels in normal-weight individuals, ↓ levels in obese individuals
(Perry & Wang, 2012; Beckman, Beckman, & Earthman, 2010 )

Symptoms/Clinical Manifestations
• Accumulation of adipose tissue primarily in subcutaneous tissue and in abdominal region• Adipocytes increase in number and size as obesity develops.• Linked to >3o comorbidities• DM• CAD• Hypercoagulable state• Sleep apnea• NAFLD• Sex hormone disorders• Depression
(Brethauer, Kashyap, & Schauer, 2013)

Etiology•Diet• Frequent meals high in unhealthy fats, red meats,
refined grains, sugar-laden beverages• Access to energy-dense foods easier and cheaper• Disordered eating habits
• Physical activity level• Sedentary lifestyle coupled with chronic overeating• Exercise replaced with sedentary activities
(“Obesity causes,” n.d.; Hurt & Frazier, 2012; Mahan, Escott-Stump, & Raymond, 2012)
Etiology• Chronic sleep deprivation• Endocrine regulation altered• Can change composition, quantity, and timing of
food intake
•Heredity• Genes influence satiety, RMR, quantity and size of
adipose cells, distribution of fat mass• Gene activation or deactivation
(Mahan, Escott-Stump, & Raymond, 2012; Mahan, Escott-Stump, & Raymond, 2012)

Etiology•Obesogens• Alter lipid metabolism and promote fat accumulation• Act as endocrine disruptors • Pharmaceutical obesogens
• Thiazolidinediones • Selective serotonin reuptake inhibitors• Diethylstilbestrol
• Industrial obesogens• Tributyltin and triphenyltin compounds• Bisphenol A• Perfluorooctanoic acid• Diethylhexyl phthalate
• Dietary obesogens• Monosodium glutamate• Genistein• Fructose
(Holtcamp, 2012)

Etiology• Pathogens• 10 infectious agents implicated in adipogenesis• Bacteria• Viruses• Gut microflora• Prions
(Mahan, Escott-Stump, & Raymond, 2012)

Treatment• Lifestyle modification• Behavior modification• Diet intervention• Calorie restriction diets• Meal replacement diets• Commercial diet programs
• Physical activity

Treatment• Pharmaceutical management• Few drugs approved by FDA• BMI of ≥30 kg/m2 or BMI of 27-29 kg/m2 with at
least one obesity-related comorbidity to qualify• Available drugs• Orlistat/Xenical®/Alli®• Lorcaserin/Belviq®• Phentermine-topiramate/Qsymia®
(“Prescription medications,” 2013)
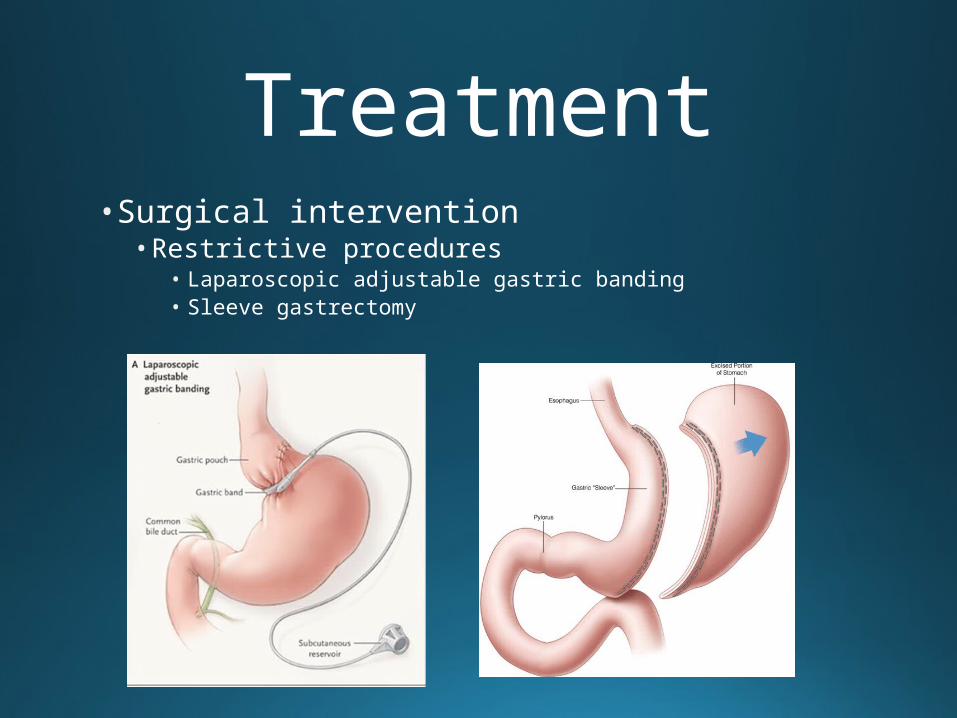
Treatment• Surgical intervention• Restrictive procedures
• Laparoscopic adjustable gastric banding• Sleeve gastrectomy
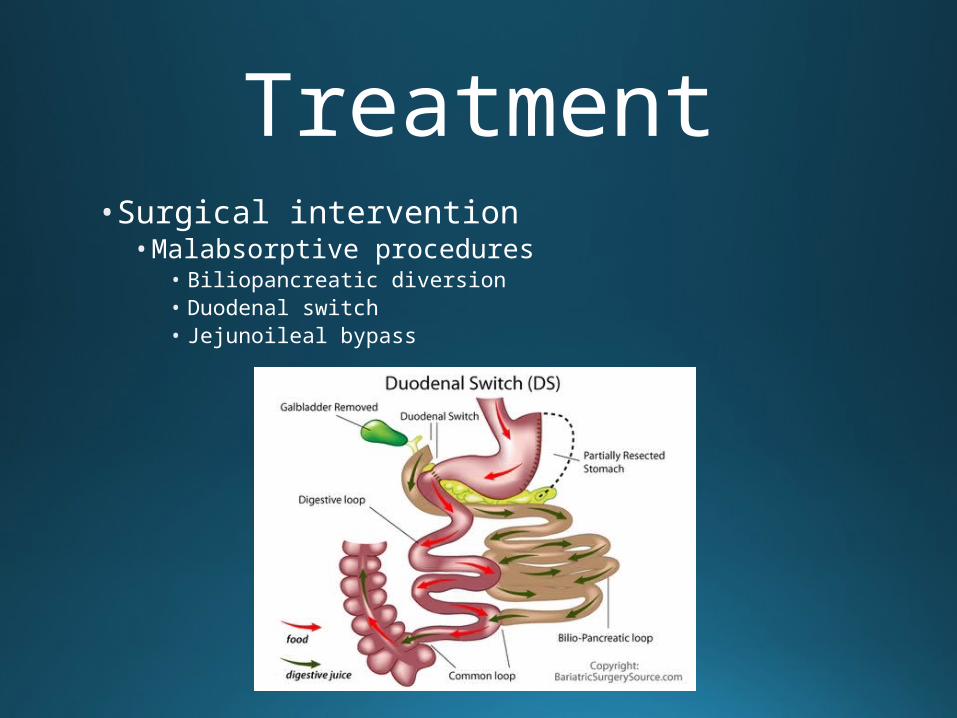
Treatment• Surgical intervention• Malabsorptive procedures
• Biliopancreatic diversion• Duodenal switch• Jejunoileal bypass

Treatment• Surgical intervention• Combined restrictive and malabsorptive procedure
• Roux-en-Y gastric bypass

The Comparative Effectiveness of Sleeve Gastrectomy, Gastric Bypass, and Adjustable
Gastric Banding Procedures for the Treatment of Morbid Obesity
• Purpose• Analyze comparative effectiveness of SG, RYGB, and
LAGB
•Methods• 2,949 SG patients matched to same number of
patients who underwent RYGB and LAGB• Matched based on 23 characteristics• Data obtained from externally audited, statewide
clinical registry • Outcomes included weight loss, complications arising
within 30 days of procedure, and quality of life
(Carlin et al., 2013)
The Comparative Effectiveness of Sleeve Gastrectomy, Gastric Bypass, and Adjustable
Gastric Banding Procedures for the Treatment of Morbid Obesity
• Results• Weight loss at 1 year for SG was 13% lower compared
to RYGB (p < 0.0001) and 77% higher compared to LAGB (p < 0.0001)• Weight loss in patients plateaued or rebounded in all three
procedure groups at years 2 and 3
• Overall complication rates in patients who underwent SG were lower compared to RYGB (p < 0.0001) and higher compared to those who underwent LAGB (p < 0.0001)• Severe complication rates for SG were similar to RYGB
(p = 0.736) but higher compared to LAGB (p < 0.0001)• Remission rates for comorbidities in patients who
underwent SG were similar to those who underwent RYGB and higher compared to LAGB patients
(Carlin et al., 2013)

• Conclusion• Due to the greater weight loss observed after SG
compared to LAGB as well as the decreased complication rates compared to RYGB, insurance carriers should provide routine coverage for this bariatric procedure.
(Carlin et al., 2013)
The Comparative Effectiveness of Sleeve Gastrectomy, Gastric Bypass, and Adjustable
Gastric Banding Procedures for the Treatment of Morbid Obesity

Treatment• Treatment specific to patient• Surgical debridement of groin abscess• Cystoscopy with Foley catheter placement• Tracheostomy placement/PEG tube placement• Dialysis catheter placement for CRRT treatment• Restricted caloric intake• Medications
• Propofol• Norepinephrine • Fentanyl• Lorazepam• Insulin lispro • Nebivolol• Pantoprazole• Furosemide• Bisacodyl• Heparin• Vancomycin

Nutrition Intervention•Decreasing caloric intake creates a negative energy balance, thereby causing a person to lose weight. • 10% ↓ in initial body weight over 6 month period for ambulatory, morbidly obese patients• For critically ill, morbidly obese patients, RMR critical to ↓ under- and overfeeding• Indirect calorimetry vs. predictive equations
(Hurt & Frazier, 2012)
Nutrition Intervention• Penn State Equation [PSU(2003b)]• Used for critically ill, mechanically ventilated, obese
adults ≤ 60 years of age• PSU(2003b): RMR (kcal/d) = Mifflin (0.96) + VE (31) +
Tmax (167) – 6212
•Modified Penn State Equation [PSU(2010)] • Used for critically ill, mechanically ventilated, obese
adults > 60 years of age• PSU(2010): RMR (kcal/d) = Mifflin (0.71) + VE (64) +
Tmax(85) – 3085
(“Critical illness,” 2013)
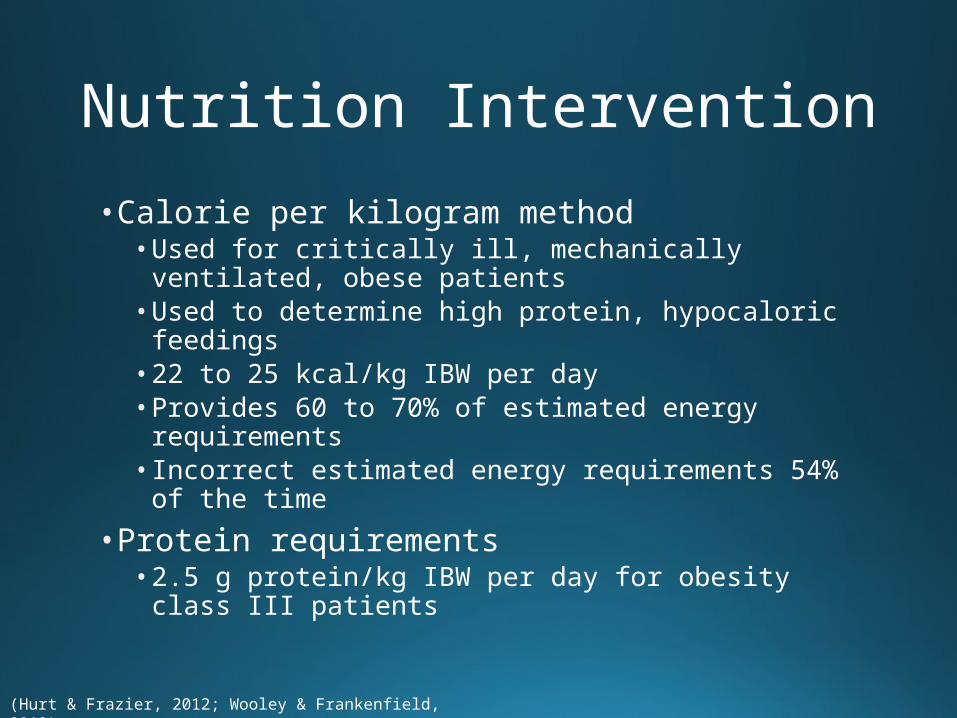
Nutrition Intervention• Calorie per kilogram method• Used for critically ill, mechanically ventilated, obese
patients• Used to determine high protein, hypocaloric feedings• 22 to 25 kcal/kg IBW per day • Provides 60 to 70% of estimated energy requirements• Incorrect estimated energy requirements 54% of the
time
• Protein requirements• 2.5 g protein/kg IBW per day for obesity class III
patients
(Hurt & Frazier, 2012; Wooley & Frankenfield, 2012)

Prediction of Resting Metabolic Rate in Critically Ill Patients at the Extremes of Body
Mass Index
• Purpose• To provide validation data on the accuracy of
predictive equations since little data currently exists
•Methods• RMR of critically ill, mechanically ventilated patients
with a BMI of ≤ 21.0 or ≥ 45.0 kg/m2 was assessed using IC• Penn State equation, Ireton-Jones equation, Faisy
equation, Harris-Benedict equation, Mifflin-St Jeor equation, and ACCP standard compared to IC measurements• Accuracy determined when energy expenditure
estimations from equations fell within 10% of IC measurement
(Frankenfield, Ashcraft, & Galvan, 2013)

Prediction of Resting Metabolic Rate in Critically Ill Patients at the Extremes of Body
Mass Index
• Results• Penn State equation had highest accuracy rate (76%)
in morbidly obese patients while ACCP standard had lowest accuracy rate when actual body weight was utilized (0%)• Penn State equation had highest accuracy rate (63%)
in underweight patients, but when BMI dropped below 20.5, accuracy rate fell to 58%
• Conclusion• For critically ill, morbidly obese patients, Penn State
equation is valid for estimating RMR• For critically ill, underweight patients, modification to
Penn State equation necessary to improve accuracy rate
(Frankenfield, Ashcraft, & Galvan, 2013)

Prognosis•Not a leading cause of death in US or world•Does increase risk for development of related comorbidities, some of which are leading causes of death•Weight loss decreases risk of developing comorbidities – all interventions, however, pose risk for weight regain• Surgical interventions provide greatest results
(“Leading causes,” 2013; “Top 10,” 2013; Stoklossa & Atwal, 2013)
• Purpose• Research on critically ill, obese adults has found
that outcomes in this patient group are not worse than in normal-weight adults. Research examining outcomes in those with morbid obesity with a BMI ≥ 40 kg/m2 has not been conducted and was the focus of this study.
(Martino et al. 2011)
Extreme Obesity and Outcomes in Critically Ill Patients

Extreme Obesity and Outcomes in Critically Ill Patients
•Methods• Data gathered and evaluated from multicenter international
observational study which examined nutrition practices in ICU• Observational study took place in 355 ICU units in 33 different
countries and included data from 2007 to 2009• Patients included in study were mechanically ventilated adults
≥ 18 years of age who received treatment in ICU for > 72 hours• 8,813 patients included in the study of which 3,490 had normal
weight while 348 had BMI of 40 to 49.9 kg/m2, 118 had BMI of 50 to 59.9 kg/m2, and 58 had BMI of 60 kg/m2 or greater• Comparison of 60-day mortality rate, DMV, LOS in ICU, and
hospital LOS conducted between morbidly obese and normal-weight patients• Potential cofounders adjusted for using logistic generalized
estimating equations and Cox proportional hazard methods with ICU clustering
(Martino et al. 2011)

Extreme Obesity and Outcomes in Critically Ill Patients
• Results• Critically ill, morbidly obese patients had improved
60-day mortality rate compared to normal-weight individuals (p = 0.04), but this was considered nonsignificant after cofounders adjusted for• Morbidly obese patients had longer DMV (p = 0.0013),
ICU LOS (p = 0.0016), and trend toward decreased hospital LOS (p = 0.17) compared to normal-weight individuals after adjustment of cofounders
• Conclusion• Morbid obesity not associated with decreased survival
rate compared to normal-weight patients during critical illness but is associated with increased DMV and ICU LOS.
(Martino et al. 2011)
Nutrition Care Process
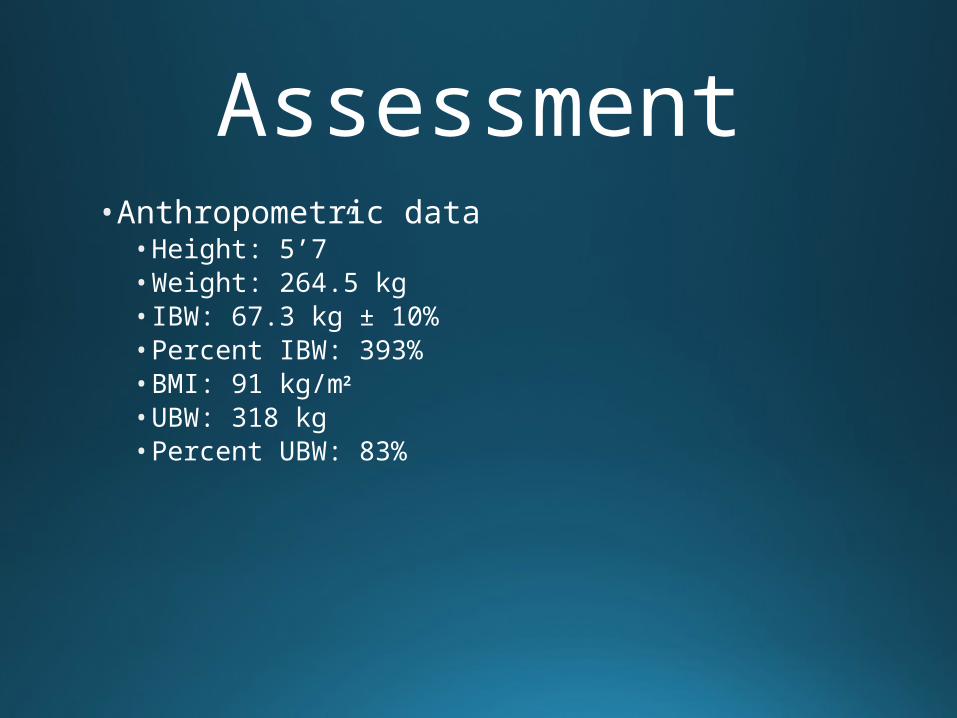
Assessment• Anthropometric data• Height: 5’7”• Weight: 264.5 kg• IBW: 67.3 kg ± 10%• Percent IBW: 393%• BMI: 91 kg/m2
• UBW: 318 kg• Percent UBW: 83%

Assessment• Biochemical labs
Basic Metabolic Panel Date 01/26 02/02 02/08 02/12Glucose(mg/dL)
372, High 205, High 280, High 124, High
BUN(mg/dL)
Normal 44, High 28, High 59, High
Creatinine (mg/dL)
Normal Normal Normal 3.43, High
Sodium(mEq/L)
131, Low Normal Normal Normal
Potassium(mEq/L)
Normal Normal Normal 6.1, High
Chloride(mEq/L)
95, Low Normal Normal Normal
CO2(mEq/L)
23, Low 32, High 34, High Normal
Calcium (mg/dL)
Normal Normal Normal Normal
GFR (mL/min/1.73 m2)
Normal Normal Normal 19, Low

Assessment• Biochemical labs
Renal ProfileDate 01/30 02/12 02/14 02/17Glucose (mg/dL)
191, High
174, High
137, High
215, High
BUN(mg/dL)
Normal 62, High 32, High 74, High
Creatinine (mg/dL)
Normal 3.81, High
2.36, High
3.52, High
Sodium (mEq/L)
133, Low Normal Normal Normal
Potassium (mEq/L)
Normal 5.9, High Normal 5.1, High
Chloride (mEq/L)
98, Low Normal Normal Normal
CO2(mEq/L)
Normal Normal Normal Normal
Calcium (mg/dL)
Normal Normal 7.9, Low Normal
Albumin (gm/dL)
1.7, Low 1.8, Low 1.8, Low 1.7, Low
Phosphorus (mg/dL)
4.5, High Normal Normal 4.4, High
GFR (mL/min/1.73 m2)
Normal 17, Low 29, Low 18, Low

Assessment• Biochemical labs
Other Labs
Date 01/26 02/13
Triglycerides (mg/dL)
228, High No lab drawn
Lactate(mmol/L )
No lab drawn 5.5, High
Complete Blood Count
Date 01/25 02/01 02/08 02/15 02/17
White Blood Cell (K/uL)
23.71, High 17.47, High Normal 13.22, High
17.29, High
Red Blood Cell (m/ul)
4.22, Low 3.99, Low 2.56, Low 2.57, Low 2.66, Low
Hemoglobin (gm/dL)
13.0, Low 12.6, Low 7.9, Low 8.0, Low 8.4, Low
Hematocrit (%)
Normal Normal 27.5, Low 26.5, Low 28.2, Low

Assessment•Diet history• Lost weight PTA• Consumed small, more frequent meals• Consumed mostly fruits and vegetables• Food shopping and preparation done by brother and
sister

Assessment• Initial dietary assessment• Consult sent by MD for tube feeding
recommendations• Patient receiving 81 mL/hr of Diprivan, providing
2,138 kcal from fat

Assessment• Calculated needs• Calories
• 3,229 kcal/d [PSU(2010)]• PSU(2003b) should have been utilized
• Protein• 170 g/d (2.5 g/kg IBW)
• Fluid• 3,300 mL/d (1 mL/kcal)
• Level 3 nutritional compromise

Nutrition Diagnosis• PES statement• Excessive fat intake related to current dose of lipids
from Diprivan as evidenced by parenteral intake of greater than 200 g/d of lipids and a high triglyceride level.

Nutrition Intervention/Monitoring & Evaluation•Nutrition intervention• Once weaned from Diprivan, Glucerna 1.5 Cal® tube
feeing at goal rate of 80 ml/hr to provide 2,880 kcal, 158 g protein, and 1,457 mL fluid
•Monitoring and evaluation• Monitor tube feeding tolerance• Promote weight loss• Promote trend of blood glucose and triglyceride levels
toward normal limits• Promote surgical wound healing
Assessment• 2nd assessment• Follow-up• Patient receiving Jevity 1.5 Cal® at 50 mL/hr which
provided 1,800 kcal, 77 g protein, and 912 mL fluid• 56% of estimated energy needs met with diet order

Nutrition Diagnosis• PES statement• Inadequate energy intake related to current tube
feeding order as evidenced by intake record.

Nutrition Intervention/Monitoring & Evaluation•Nutrition intervention• Glucerna 1.5 Cal® at 80 mL/hr to provide adequate
nutrition and better control for blood glucose levels• Phosphate binder to better control blood phosphate
levels
•Monitoring and evaluation• Maintain lean body mass while promoting weight loss• Promote trend of blood glucose and electrolyte levels
toward normal limits• Promote surgical wound healing
Assessment• 3rd, 4th, and 5th assessment• Patient still receiving Jevity 1.5 Cal® at 50 mL/hr• Later made NPO for gastrograph study• No new dietary interventions• Monitoring and evaluation of interventions remained
the same

Assessment• 6th assessment• Follow-up• Patient NPO for 2 days 2º excessive gastric residuals
and vomiting

Nutrition Diagnosis• PES statement• Altered GI function related to lack of GI motility due to
physical inactivity, possible inadequate head of bed elevation, and maximum dose of Levophed as evidenced by vomiting, excessive residuals, and a NPO diet.

Nutrition Intervention/Monitoring & Evaluation•Nutrition intervention• Bowel rest• Initiation of PPN if medically appropriate
• Clinimix 2.75/5 at 100 mL/hr
• If Levophed dose began trending below 20 mcg/min consistently, then enteral nutrition with a fiber-free formula recommended to be initiated
•Monitoring and evaluation• Remained same with addition of ensuring proper
hydration to prevent dehydration or overhydration

Assessment• 7th and final assessment• Consult sent by MD for TPN recommendations• Renal MD decided to manage TPN• Patient NPO for 4 days 2º possible ischemic bowel
Nutrition Diagnosis• PES Statement• Altered GI function related to possible ischemic bowel
disease as evidenced by a high lactate level.

Nutrition Intervention/Monitoring & Evaluation•Nutrition intervention• TPN to provide at least 70 to 80% of estimated energy
needs• TPN goal of 170 g amino acids, 350 g dextrose, and
50 g intralipids.• Monitor patient for refeeding syndrome since he had
been NPO for four days and had, before that, been underfed with tube feedings
•Monitoring and evaluation• TPN to meet at least 70% of goal nutritional needs• Promote trend of acid-base, electrolyte, and glucose
profile toward normal limits• Promote surgical wound healing

Conclusion• Admitted for surgical debridement of groin abscess•Developed multiple conditions•Nutrition diagnoses• Excessive fat intake• Inadequate energy intake• Altered GI function
•Nutrition interventions• Tube feeding recommendations• Phosphate binder• Initiation of PPN• Initiation of TPN
•Withdrawal of care •Discharge to hospice

Review of Key Points• Affects 6.6% of adult Americans• Physiological changes occur in relation to appetite regulation and weight management hormones• Associated with many comorbid conditions•Multiple factors contribute to etiology• Penn State University equations to determine RMR•Not a leading cause of death but comorbidities are
(Sturm & Hattori, 2013)
Personal Impressions

References2008 Physical Activity Guidelines for Americans Summary. (2008, October 16). Retrieved March 15, 2014, from http://www.health.gov/paguidelines/guidelines/summary.aspx Acik. (n.d.). [Plastic bottles]. Retrieved April 1, 2014, from http://www.earthtimes.org/health /map-reading-male-mice-falls-foul-bpa/1079/ [Alli function]. (n.d.). Retrieved April 1, 2014, from http://pharmamkting.blogspot.com /2011/04/little-used-drug-for-sale-gsk-says- bye.html Bearden, M. (2013, September). Ischemic bowel disease. Retrieved March 15, 2014, from
http://www.med.nyu.edu/content?ChunkIID=96868 Beckman, L. M., Beckman, T. R., & Earthman, C. P. (2010). Changes in gastrointestinal hormones and leptin after Roux-en-Y gastric bypass procedure: A review. Journal of the American Dietetic Association, 110(4), 571-584. doi: 10.1016/j.jada.2009.12.023 Brethauer, S., Kashyap, S., & Schauer, P. (2013, March). Obesity. Retrieved March 15, 2014, from http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/endocrinology/obesity/ Cellulitis. (2012, February 23). Retrieved March 15, 2014, from http://www.mayoclinic.org/ diseases-conditions /cellulitis/basics/definition/con-20023471 Charney, P., & Malone, A. (2009). ADA pocket guide to nutrition assessment (2nd ed.). Chicago, IL: American Dietetic Association. Cross section of abscess [Digital image]. (n.d.). Retrieved April 1, 2014, from http://medical- dictionary.thefreedictionary.com/_/viewer.aspx?path=dorland&name=abscess.jpg

Dugdale, D. C., III, & Lin, H. Y. (2012, September 5). Acute kidney failure: MedlinePlus medical encyclopedia. Retrieved March 15, 2014, from http://www.nlm.nih. gov/medlineplus/ency/article/000501.htm Dugdale, D. C., III. (2012, August 30). Obesity hypoventilation syndrome (OHS): MedlinePlus medical encyclopedia. Retrieved March 15, 2014, from
http://www.nlm.nih.gov/medlineplus/ency/article/000085.htm Dugdale, D. C., III. (2012, September 2). Abscess: MedlinePlus medical encyclopedia. Retrieved March 15, 2014, from http://www.nlm.nih.gov/medlineplus/ency /article/001353.htm [Duodenal switch]. (n.d.). Retrieved April 1, 2014, from http://www.bariatric-surgery- source.com/duodenal-switch.html Frankenfield, D. C., Ashcraft, C. M., & Galvan, D. A. (2013). Prediction of resting
metabolic rate in critically ill patients at the extremes of body mass index. Journal of Parenteral and Enteral Nutrition, 37(3), 361-367. doi: 10.1177/0148607112457423 Gastric banding surgery for weight loss. (2012, February 5). Retrieved March 15, 2014, from http://www.webmd.com/diet/weight-loss-surgery/gastric-banding-surgery-for-weight-loss [Glow sticks]. (n.d.). Retrieved April 1, 2014, from http://rage.officialglofx.com/the- glow-in-glow-sticks/ Holtcamp, W. (2012). Obesogens: An environmental link to obesity. Environmental Health Perspectives, 120(2), A62-A68. doi: 10.1289/ehp.120-a62 Hurt, R. T., & Frazier, T. H. (2012). Obesity. In The A.S.P.E.N. adult nutrition support core curriculum (pp. 603-619). Silver Spring, MD: American Society for Parenteral and Enteral Nutrition.
Kaynar, A. M., & Sharma, S. (2012, January 5). Respiratory failure . Retrieved March 15, 2014, from http://emedicine.medscape.com/article/167981-overview Kulick, D., Hark, L., & Deen, D. (2010). The bariatric surgery patient: A growing role for registered dietitians. Journal of the American Dietetic Association, 110(4), 593-599. doi: 10.1016/j.jada.2009.12.021 [Laparoscopic adjustable gastric banding]. (n.d.). Retrieved April 1, 2014, from http://www.bariatricexperts.com/gastric_banding.html Laparoscopic sleeve gastrectomy. (n.d.). Retrieved March 15, 2014, from
http://weightloss.clevelandclinic.org/Sleevegastrectomy.aspx Leading causes of death. (2013, December 30). Retrieved March 15, 2014, from http://www.cdc.gov/nchs/fastats/lcod.htm Louro, L. (2013, May 28). Large male patient with big belly and doctor [Digital image]. Retrieved April 1, 2014, from http://www.livescience.com/34806- obesity-bias-medical-students-doctors.html Mahan, L. K., Escott-Stump, S., & Raymond, J. L. (2012). Krause's food & the nutrition care process (13th ed.). St. Louis, MO: Saunders. Martino, J. L., Stapleton, R. D., Wang, M., Day, A. G., Cahill, N. E., Dixon, A. E., ... Heyland, D. K. (2011). Extreme Obesity and Outcomes in Critically Ill
Patients. Chest, 140(5), 1198-1206. doi: 10.1378/chest.10-3023 National Guideline Clearinghouse: Critical illness evidence-based nutrition practice guideline. (2013, March 25). Retrieved March 15, 2014, from
http://www.guideline.gov/content.aspx?id=39404

Obesity causes. (n.d.). Retrieved March 15, 2014, from http://www.hsph.harvard. edu/obesity-prevention-source/obesity-causes/ Obesity. (n.d.). Retrieved March 15, 2014, from http://www.merriam-webster.com/ dictionary/obesity Ogden, C. L., Carroll, M. D., Kit, B. K., & Flegal, K. M. (2012, January). Prevalence of obesity in the United States, 2009–2010. Retrieved March 15, 2014, from http://www.cdc.gov/nchs/data/databriefs/db82.pdf [Pathogens]. (n.d.). Retrieved April 1, 2014, from http://fellowshipoftheminds.
com/2012/12/31/do-bacteria-cause-obesity/ Perry, B., & Wang, Y. (2012). Appetite regulation and weight control: The role of gut hormones. Nutrition and Diabetes, 2(1), 1-7. doi: 10.1038/nutd.2011.21 Prescription medications for the treatment of obesity. (2013, April). Retrieved March 15, 2014, from http://www.win.niddk.nih.gov/publications/prescription.htm Pronsky, Z. M., & Crowe, J. P. (2010). Food medication interactions (16th ed.). Birchrunville, PA: Food-Medication Interactions. [Roux-en-Y gastric bypass]. (n.d.). Retrieved April 1, 2014, from http://www.
weightlosssurgery.ca/about-our-surgeries/laparoscopic-roux-en-y-gastric -bypass/
Roux-en-Y gastric bypass. (n.d.). Retrieved March 15, 2014, from http://my. clevelandclinic.org/services/procedure_treatment/gastric_bypass_surgery/roux-en-y.aspx [Scale]. (n.d.). Retrieved April 1, 2014, from http://sincerelyjenni.com/6004.html/ weight-scale-4

Seagle, H. M., Strain, G. W., Makris, A., & Reeves, R. S. (2009). Position of the American Dietetic Association: Weight management. Journal of the American Dietetic Association, 109(2), 330-346. doi: 10.1016/j.jada.2008.11.041 [Sleeve gastrectomy]. (n.d.). Retrieved April 1, 2014, from http://www.yourhealthylife.org/ procedures/sleevegastrectomy Stoklossa, C. J., & Atwal, S. (2013). Nutrition care for patients with weight regain after bariatric surgery. Gastroenterology Research and Practice, 2013, 1-7. doi: 10.1155/2013/256145 Sturm, R., & Hattori, A. (2013). Morbid obesity rates continue to rise rapidly in the US. International Journal of Obesity, 37(6), 1-6. doi: 10.1038/ijo.2012.159 The 10 leading causes of death in the world 2011 [Digital image]. (n.d.). Retrieved April 1, 2014, from http://www.who.int/mediacentre/factsheets/fs310/en/ The top 10 causes of death. (2013, July). Retrieved March 15, 2014, from http://www.who.int/ mediacentre/factsheets/fs310/en/ Venes, D. (Ed.). (2009). Sepsis. In Taber's cyclopedic medical dictionary (21st ed., p. 2101). Philadelphia, PA: F.A. Davis. [Weight Watchers]. (n.d.). Retrieved April 1, 2014, from http://www.salon.com/2010/12/06/ weight_watchers_new_points/ Wisse, B. (2013, June 18). Type 2 diabetes. Retrieved March 15, 2014, from http://www.ncbi. nlm.nih.gov/pubmedhealth/PMH0001356/ Wooley, J. A., & Frankenfield, D. (2012). Energy. In The A.S.P.E.N. adult nutrition support core curriculum (2nd ed., p. 30). Silver Spring, MD: American Society for Parenteral and Enteral Nutrition. The worlds former fattest man Paul Mason [Digital image]. (n.d.). Retrieved April 1, 2014, from http://www.mirror.co.uk/news/real-life-stories/paul-mason-former-worlds-fattest- 3023512