board of directors quality & education committee of · pdf filelee memorial health system...
TRANSCRIPT
BOARD OF DIRECTORS
QUALITY & EDUCATION Committee of the Whole
MEETING
May 13, 2010, 2:00pm Lee Memorial Hospital Boardroom
2776 Cleveland Ave, Ft. Myers, FL 33901
ELECTRONIC BOARD PACKET
ALL MEETINGS ARE OPEN TO THE PUBLIC AND THE PUBLIC IS INVITED TO ATTEND Any Public Input pertaining to an agenda item is limited to three minutes and a
“Request to Address the Board of Directors” card must be completed and submitted to the Board Assistant prior to the meeting.
P.O. BOX 2218 FORT MYERS, FLORIDA
33902
239-332-1111
CAPE CORAL HOSPITAL GULF COAST MEDICAL CENTER
HEALTHPARK MEDICAL CENTER
LEE MEMORIAL HOSPITAL
THE CHILDREN’S HOSPITAL THE REHABILITATION HOSPITAL
LEE PHYSICIAN GROUP
LEE CONVENIENT CARE
BOARD OF DIRECTORS
DISTRICT ONE
Stephen R. Brown, M.D.
Marilyn Stout
DISTRICT TWO
Richard B. Akin
Nancy M. McGovern, RN, MSM
DISTRICT THREE
Lois C. Barrett, MBA
Linda L. Brown, MSN, ARNP
DISTRICT FOUR
Frank T. La Rosa
Dawson C. McDaniel
DISTRICT FIVE
James Green
Jason Moon
Any Public input is limited to three minutes and a “Request to Address the Board of Directors” card must be completed and submitted to the Board Administrator prior to meeting.
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
QUALITY & EDUCATION COMMITTEE OF THE WHOLE MEETING
Thursday, May 13, 2010
2:00 p.m. Lee Memorial Hospital Boardroom
TENTATIVE AGENDA
1. CALL TO ORDER (Steve Brown, MD, Quality & Education Chairman) The meeting of the Quality & Education Committee of the Whole of the Lee Memorial Health System Board of Directors will be called to order. Matters concerning the business of Lee Memorial Health System consisting of Gulf Coast Medical Center & Lee Memorial Hospital/ HealthPark Medical Center and its subsidiaries (HealthPark Care Center Inc., Lee Memorial Home Health, Inc., Cape Memorial Hospital, Inc. doing business as Cape Coral Hospital, and Lee Memorial Medical Management, Inc.) may be reported, discussed and recommended by the Committee of the Whole, then referred to the Full Board of Directors for final action.
2. PUBLIC INPUT: Any public input pertaining to items on the Agenda is limited to three
minutes and a “Request to Address the Board of Directors” card must be completed and submitted to the Board Administrator prior to meeting.
3. Consent Agenda: (Approval) A. Quality & Education Committee of the Whole Minutes of April 8, 2010 B. Risk Management Report, 2nd Qtr, FY2010 C. Lee Memorial Home Health Executive Summary
4. Hospitalist Presentation (Update) (Chuck Krivenko, M.D., Chief Medical Officer/Clinical Quality Services, , Jon Burdzy, D.O., and Yanet
Rios, M.D., – 20 min)
5. Patient Safety Initiative: SafeLee (Update) (Chuck Krivenko, M.D., Chief Medical Officer/Clinical Quality Services– 20 min)
6. Pathology Dictation (Verbal Update) (Tuck Wilson, M.D., Physician Leadership Council Consultant/Quality & Education Committee – 10 min)
7. Organizational Performance Scorecard 1st Quarter FY2010 (Accept) (Chuck Krivenko, M.D., Chief Medical Officer/Clinical Quality Services & Becky Watt, System Director Decision Support-Care Management – 15 min)
8. Other Items
9. Next Regular Quality & Education Committee of the Whole Meeting: Thursday, June 10, 2010 - 1:00pm (Subject to Change)
Lee Memorial Hospital Boardroom, 2776 Cleveland Avenue, Fort Myers, FL 33901
10. ADJOURNMENT OF QUALITY & EDUCATION COMMITTEE
V:\PRESENTATIONS\2010\Quality-Education\051310 2pm\051310 Quality Tentative agenda.doc
___________________ L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
PUBLIC INPUT – AGENDA ITEMS:
Any public input
pertaining to items on the Agenda is limited to three
minutes and a “Request to Address the Board of Directors”
card must be completed and submitted to
the Board Administrator prior to meeting.
Refer to Board Policy: 10:15E: Public Addressing the Board Non-Agenda Item: Individuals wishing to address the Board on an item NOT on the Agenda, the Board office must be notified of subject matter at least seven (7) days prior to the meeting to allow staff time to prepare and to insure the matter is within the jurisdiction of the Board.

LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS QUALITY & EDUCATION COMMITTEE OF THE WHOLE MEETING MINUTES
Thursday, April 8, 2010 LOCATION: Lee Memorial Hospital Boardroom, 2776 Cleveland Avenue, Fort Myers, FL 33901 MEMBERS PRESENT: Steve Brown, M.D., Chairman, Quality & Education Committee of the Whole; Richard Akin, Board Chairman; Marilyn Stout, Board Vice Chairman; Dawson McDaniel, Board Treasurer; Linda Brown, MSN, ARNP, Board Secretary; Nancy McGovern, Director; Frank La Rosa, Director; Jason Moon, Director; Lois Barrett, MBA, Director; Denise Heinemann, DrPH, Community Representative/Quality & Education Committee; Tuck Wilson, M.D., Physician Leadership Council Consultant/Quality & Education Committee MEMBERS ABSENT: James Green, Director; David Berger, M.D., Community Representative/Quality & Education Committee; Margaret Byrnes, Community Representative/Quality & Education Committee
OTHERS PRESENT: Jim Nathan, President; Cathy Stephens, Board Administrator; John Wiest, Chief Operating Officer Business & Strategic Services; Larry Antonucci, M.D., Chief Operating Officer-Hospital & Physician Services; Jon Cecil, Chief Human Resources Officer; Mike Smith, Chief Information Officer; Chuck Krivenko, M.D., Chief Medical Officer/Clinical & Quality Services; Gaile Anthony, Chief Administrative Officer/LMH; Donna Giannuzzi, Chief Patient Care Officer; Doug Luckett, Chief Administrative Officer CCH/GCMC; Mark Greenberg, M. D., System Director Medical Staff Services; John Iacuone, Executive Director Children’s Hospital; Cindy Brown, VP Patient Care Services HP; Lisa Sgarlata, VP Patient Care Services LMH; Kevin Newingham, Vice President Strategic Services; Ann Friel, Director Utilization Management; Beth Moss, System Director Invasive Cardiovascular; Karen Krieger, System Director Public Affairs; Fred Pollier, Community Representative/Planning Committee; Jack Eikenberg, Community Representative/Planning Committee; Marliese Mooney, Community Representative/Planning Committee; Don Brown, Guest; Lee Huntley, FACHE, President/Chief Executive Officer/Central Florida Health Alliance; Frank Gluck, News Press/Reporter; Isabel Firth, Administrative Secretary/Board of Directors; Lisa Ayotte, Executive Secretary/Board of Directors
NOTE: Documents referred to in these minutes are on file by reference to this meeting date in the Office of the Board of Directors and on the Board of Directors website at www.lememorial.org/boardofdirectors, for public inspection.
SUBJECT DISCUSSION ACTION FOLLOW-UP MEETING
CALLED TO ORDER The Quality & Education Committee of the Whole meeting
was CALLED TO ORDER at 1:02p.m. by Steve Brown, M.D. Chairman, Quality & Education Committee of the Whole
The Board sits as the Lee Memorial Health System Board of Directors of Gulf Coast Medical Center, Lee Memorial Hospital, HealthPark
Medical Center and the Board of Directors of its subsidiary corporations: Cape Memorial Hospital, Inc. doing business as Cape
Coral Hospital; Lee Memorial Medical Management, Inc.; Lee Memorial Home Health, Inc.; and HealthPark Care Center, Inc.
PUBLIC INPUT None at this time.
CONSENT AGENDA Steve Brown asked for approval of the following items are on the Consent Agenda
A. Quality/Education Committee of the Whole Minutes of: January 14, 2010; February 11, 2010; March 4, 2010
B. Adoption of the following Board Policies (Exhibit 1): i. 10.18C: Quality & Performance Improvement ii. 10.41B: Governance & Reporting of System Performance Indicators iii. 30.03B: Medical Credentialing
A motion was made by Marilyn Stout to approve the Consent Agenda consisting of the following items: A. Quality/Education Committee of the Whole Minutes of:
January 14, 2010; February 11, 2010; March 4, 2010 B. Adoption of the following Board Policies (Exhibit 1):
i. 10.18C: Quality & Performance Improvement ii. 10.41B: Governance & Reporting of System
Performance Indicators iii. 30.03B: Medical Credentialing
The motion was seconded by Denise Heinemann and it carried with no opposition.
2010 UTILIZATION MANAGEMENT PLAN
Ann Friel reviewed the annual 2010 Utilization Management Plan (Exhibit 2). This plan is required by KePRO, the organization contracted by AHCA to review all inpatient Medicaid claims for medical necessity.
A motion was made by Denise Heinemann to approve the 2010 Utilization Management Plan (Exhibit 2). The motion was seconded by Marilyn Stout and it carried with no opposition.
DET NORSKE
VERITAS HEALTHCARE
(DNVHC)
Chris Crawford presented an update on the Det Norske Veritas Healthcare (DNVHC) Accreditation survey process (Exhibit 3). Highlights reviewed included the education plan, system preparation, survey interview practice session, and the survey cycle. Discussion ensued. Concerns were raised about how this new company was going to survey and also to ensure we are evaluating them also. Chris stated that Centers for Medicare/Medicaid Services is following DNV just like Joint Commission. We will be dual accredited and will have a choice between the two. We are expecting a survey any time beginning May, when the survey is complete a full review will be brought back to this Committee.
(Jason Moon arrived at 1:06pm.) (Dawson McDaniel arrived at 1:10pm.)
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS QUALITY & EDUCATION COMMITTEE OF THE WHOLE MEETING MINUTES Thursday, April 8, 2010. Page 2 of 2
SUBJECT DISCUSSION ACTION FOLLOW-UP GRADUATE MEDICAL
EDUCATION Richard Akin and John Iacuone gave a verbal update on the progress of the Graduate Medical Education (GME) initiative. Richard stated that recently John Wiest and John Iacuone visited the Florida State University Medical School. The graduates of this university are medical doctors and that is the path that Lee Memorial wants to take. The university will be responsible for the documentation and academic side of the residency program. Program directors will need to be on staff to bring this into the system for approximately a year before. A budget has already been set up for this program. We are submitting for a grant to start this program, and Florida State University has the ability to match this grant. Some graduates of this school will be medical doctors along with a Masters Degree in Business. This could be a tremendous asset to this area. A complete presentation on starting an internship program will be placed on a future Board agenda.
Future meeting: Full GME presentation
PATHOLOGY DICTATION
Chuck Krivenko gave a verbal update on issues with pathology dictation reporting. Mike Smith addressed corrected issues in Net Access and stated that changes have been put in place to label the different reports and he also confirmed patient safety is not an issue. Pathologists feel that the issues have been addressed and taken care of. Tuck Wilson will be following up with the Pathologists to verify issues have been corrected.
(Frank La Rosa arrived at 1:47pm.)
Dr. Tuck Wilson will provide a report back.
HEALTHCARE
PERFORMANCE IMPROVEMENT (HPI)
Chuck Krivenko gave a verbal update on our HPI safety initiative – SafeLee. He said tools and behavior modules are coming up, along with a group of trainers will be educated and then train staff and physicians in the numeric system. These sessions are being scheduled and facilitated by Carol Simonds. The Physician safety committee has ambassadors on each of the committees. Reporting structure is being worked on by Chuck and Legal. Marketing program and logo are underway. He said we are already seeing changes in the organization in safety and culture. Constant updates will be provided to the Board.
CARDIAC PROGRAM Steve Brown presented some concerns he has with the cardiac program. He said if a
patient is transferred from one hospital to another the catheterization -prep would be repeated. A suggestion is to have one campus situated for cardiac issues. Beth Moss stated that cardiac catheterization prep is not always repeated if the patient is transferred because the films are available at all hospitals. Data will be collected to analyze the program and decide if any changes should be made. Discussion ensued.
Data reports will be analyzed, and reported back to this committee.
OTHER ITEMS
Written Reports Steve Brown requested reports be provided in writing as opposed to verbal updates, especially on such significant topics.
NEXT REGULAR
MEETING The next REGULAR Quality & Education Committee of the Whole meeting is
May 13, 2010, 1:00pm. Lee Memorial Hospital Boardroom, 2776 Cleveland Avenue Fort Myers, FL 33901
ADJOURNMENT The Quality & Education Committee of the Whole meeting
was ADJOURNED at 2:10 p.m. by Steve Brown, M.D., Chairman, Quality & Education
Committee of the Whole.
Minutes were recorded by Lisa Ayotte, Executive Secretary/Board of Directors Office
_______________________________________________________ Linda Brown, MSN, ARNP
Board Secretary
Unless the information you submit with this form is significantly enhanced
in color (i.e. graphs), please submit in black & white,
maximum 2 slides per page.
LMHS BOARD OF DIRECTORS RECOMMENDED ACTION FOR BOARD APPROVAL
(Action includes Acceptance, Approval, Adoption, etc)
Keep form to one page, SUBMIT (thru SLC Member) ELECTRONCIALLY
to L Drive Miscellaneous BOD Presentations by Noon the Friday before the week you’re
scheduled on agenda.
DATE: May 5, 2010 LEGAL SERVICE REVIEW? YES___ NO___
SUBJECT: Quarterly Risk Management Report
REQUESTOR & TITLE: Mary McGillicuddy, Chief Legal Officer
PREVIOUS BOARD ACTION ON THIS ITEM (IF ANY) (justification and/or background for recommendations – internal groups which support the recommendation i.e. SLC, Operating Councils, PMTs, etc.) Acceptance of Quarterly Risk Management Report for the previous quarter. SPECIFIC PROPOSED MOTION: Motion to Accept Quarterly Risk Management Report Q2FY10 PROS TO RECOMMENDATION Not Applicable
CONS TO RECOMMENDATION Not Applicable
LIST AND EXPLAIN ALTERNATIVES CONSIDERED Not Applicable FINANCIAL IMPLICATIONS Budgeted ____ Non-Budgeted ____ (including cash flow statement, projected cash flow, balance sheet and income statement) No financial implications OPERATIONAL IMPLICATIONS (including FTEs, facility needs, etc.) No operational implications SUMMARY Quarterly Risk Management Report including:
• Incident Reporting per 1,000 patient days • Injury Occurrences per 1,000 patient days • Categories of incident reports • Risk Management participation in LMHS System Committees and Education • Liability Claims • Recommendations
BOD/Forms/Board (Action) Reporting Form - revised 1/9/08/cs
1
QUARTERLY RISK MANAGEMENT REPORT TO THE BOARD
January – March 2010
The disclosure of this document and the contents herein does not constitute a waiver of any and all protections afforded Patient Safety Work Product under either Florida state or federal law including but not limited to those under the Patient Safety Quality Improvement Act of 2005 and implementing regulations, 45 C.F.R. Part 3; 42 U.S.C. § 11111; §§395.0193 F.S. and 766.101 F.S.

2
REPORTING RATES
The graph below shows incident reporting rates for the system for the past 27 months. During this time range the reporting rate has increased slightly.
The graphs on page 3 reflect the reporting rates for the four facilities individually. The four graphs also show the last 27 months of activity.
Lee Memorial Health System
0
5
10
15
20
25
Jan-
08
Feb-
08
Mar
-08
Apr-
08
May
-08
Jun-
08
Jul-0
8
Aug-
08
Sep-
08
Oct
-08
Nov
-08
Dec
-08
Jan-
09
Feb-
09
Mar
-09
Apr-
09
May
-09
Jun-
09
Jul-0
9
Aug-
09
Sep-
09
Oct
-09
Nov
-09
Dec
-09
Jan-
10
Feb-
10
Mar
-10
3
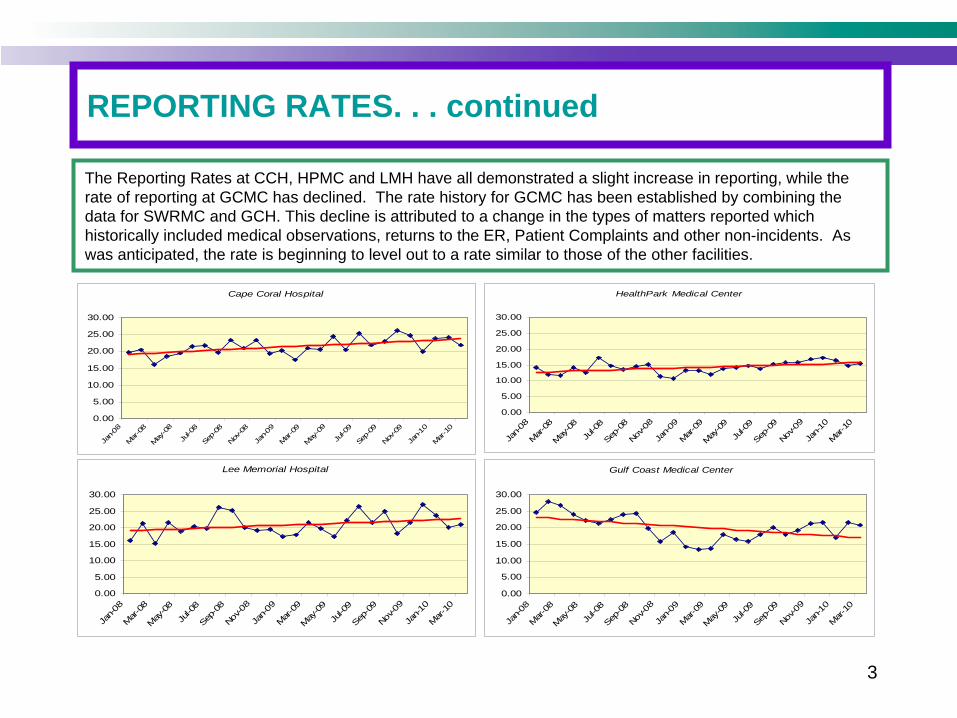
REPORTING RATES. . . continued
The Reporting Rates at CCH, HPMC and LMH have all demonstrated a slight increase in reporting, while the rate of reporting at GCMC has declined. The rate history for GCMC has been established by combining the data for SWRMC and GCH. This decline is attributed to a change in the types of matters reported which historically included medical observations, returns to the ER, Patient Complaints and other non-incidents. As was anticipated, the rate is beginning to level out to a rate similar to those of the other facilities.
Cape Coral Hospital
0.00
5.00
10.00
15.00
20.00
25.00
30.00
Jan-0
8Mar
-08
May-0
8
Jul-0
8Se
p-08
Nov-08
Jan-0
9Mar
-09
May-0
9
Jul-0
9Se
p-09
Nov-09
Jan-1
0Mar
-10
HealthPark Medical Center
0.00
5.00
10.00
15.00
20.00
25.00
30.00
Jan-
08M
ar-0
8M
ay-0
8Ju
l-08
Sep-
08Nov
-08
Jan-
09M
ar-0
9M
ay-0
9Ju
l-09
Sep-
09No
v-09
Jan-
10M
ar-1
0
Lee Memorial Hospital
0.00
5.00
10.00
15.00
20.00
25.00
30.00
Jan-
08Mar-
08M
ay-08
Jul-0
8Sep
-08
Nov-0
8Ja
n-09
Mar-
09M
ay-09
Jul-0
9Sep
-09
Nov-0
9Ja
n-10
Mar-10
Gulf Coast Medical Center
0.00
5.00
10.00
15.00
20.00
25.00
30.00
Jan-
08Mar
-08
May
-08Ju
l-08
Sep-0
8Nov
-08
Jan-
09Mar
-09
May
-09Ju
l-09
Sep-0
9Nov
-09
Jan-
10Mar
-10

4
INJURY
The first graph shows the reporting rate and the injury rate for the four facilities during the last quarter. The second graph shows the percentage of reports without injury. Reporting of no injury incidents are highly encouraged so that “near misses”
and potential areas of improvement can be identified. This information allows us to better understand where risks exist, and provides data used in our quality improvement activities throughout the system. More than 70% of the incident reports received involve no injury. During this quarter, there was one report to AHCA, as required by the Risk Management statute.
0.00
5.00
10.00
15.00
20.00
25.00
CCH HPMC LMH GCMC
Reporting Rate Injury Rate
Percent of Incidents Without Injury
0%
20%
40%
60%
80%
100%
Jan-
09
Feb-
09
Mar
-09
Apr-
09
May
-09
Jun-
09
Jul-0
9
Aug-
09
Sep-
09
Oct
-09
Nov
-09
Dec
-09
Jan-
10
Feb-
10
Mar
-10

5
CATEGORIES
The graph to the right shows the rate for the categories of reported incidents from January through March 2010 at all four facilities. Rates
are being
utilized to be consistent with other system reporting. As indicated, the vast majority of these incidents did not involve any injury.
The most reported categories are:•
Patient Falls •
Treatment & Testing category includes reports of IV infiltrates, Delays and Omissions, Patient Identification issues, etc
•
Other
category includes Exposures, Complaints, burns, skin breakdown, ER issues, AMAs, etc
•
Medication Related ReportsNearly 70% of all reported occurrences fall
within one of these four categories
0.00 1.00 2.00 3.00 4.00 5.00 6.00
Sedation for Proc
Transport Issues
Assault
Equipment
Good Catch
NonPt Fall
Inf/Mat/OB
Adverse Drug Rx
Lab Labeling
Surgical
Med Error
Other
Test/Treatment
Patient Fall
Reporting Rate per 1000 Patient Days
6
EDUCATION
Risk Management Educational Activities included:
• Risk Management Orientation for new hires• Risk management Orientation for new Nursing
hires• EMTALA Inservice• Incident Reporting Inservices• Risk Management inservices
or Neuro
Staff
• Risk Management inservice
for Surgery Staff• Risk Management Issues in the ER for HPMC
ARNPs
& PAs• Incident Report Documentation for CCH

7
LIABILITY
Malpractice ClaimsThe second fiscal quarter of 2010 was unusual, in that no claims were closed during the period. However, new claims made
against the Health System rose, with 9 claims being received during the quarter.The result has been an increase in the overall number of open claims from 40 at the end of the first fiscal quarter (October 1
– December 31, 2009), to 49 on March 31, 2010.This represents the highest number of open professional liability cases at the end of any fiscal quarter in recent memory.In keeping with prior reports, the alleged bases for professional liability claims remains quite diverse, making it difficult to
determine that a particular type of event or a particular location is involved. Prior predictions that an increase in claims against the Lee Memorial Health System would occur, due to its size and
complexity, have proven correct. Lee Memorial continues to have comparatively low numbers of malpractice claims when measured against other hospitals
and healthcare organizations in this state and nationally. That comparison, however, has not detracted from the focus of the System’s risk managers and legal staff on malpractice prevention and quality of care improvement.
As usual , the terms under which malpractice claims against the System are closed continues to be very favorable to the Health System.
05
101520253035404550
FY08Q1 FY08Q2 FY08Q3 FY08Q4 FY09Q1 FY09Q2 FY09Q3 FY09Q4 FY10Q1 FY10Q2

8
RISK MANAGEMENT ACTIVITIES
Continued participation in system committees including:• Campus Specific ADE Work Groups• Adverse Drug Event Task Force• Patient Safety Measurement Committee• Employee Safety and Wellness• Ethics Committee• Standards and Compliance• Nursing Leadership• Patient Care Service P&P Committee• Quality Safety Management Council• GCMC Patient Safety Committee• Medication Safety Committee• Serious Safety Event Rate SSER• Psychiatric Consultation Services Council• Patient Safety Evaluation System (LPSES) Steering Committee• Tobacco Free Lee Steering CommitteeParticipated in various Intense Analysis Teams

9
RECOMMENDATIONS
• Monitor the implementation of the SoftMed Risk Management Module.• Work closely with Customer Services to develop a Softmed module
which will enhance our ability to track and trend Grievance data.• Continue to track and trend incidents, provide summary data and work
closely with various departments and committees engaged in performance improvement and patient safety activities.
• Continue to work with Education and Organizational Development and management staff to assure that all employees are meeting the annual education requirement for risk management and to provide a module for the Competency activities.
• Continue to utilize pre-litigation procedures to resolve legitimate claims as quickly as the interests of the System and claimants allow.
• Continue development of specialized training materials for risk.• Collaborate with HPI with regard to patient safety initiatives.

BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS ENTITY REPORTING EXECUTIVE SUMMARYENTITY REPORTING EXECUTIVE SUMMARY
ENTITY/BUSINESS NAME: ____Home Heath___ Fiscal Year 2009___________
DIRECTOR & TITLE: Cindy Christman, Exec. Director REPORT DATE: May 2010
BUSINESS DESCRIPTION: Lee Memorial Home Health is a non-profit home health agency. The Agency provides nursing services as well as physical therapy, speech, occupational therapy, medical social work and home health aide services to residents of the community.
MISSION STATEMENT: Lee Memorial Home Health provides a comprehensive range of innovative, outcome-oriented, quality home health care services to residents of the community.
SYSTEM GOAL: Financial Performance
• Major Accomplishments • Scorecard Performance
o Revenue o Profit/Loss o Explanation of major variances
• Key Utilization Trends
Actual Budget Prior Year Admissions 3,859 3,700 3,723 Operating Revenue 9,729,508 9,005,809 8,755,562 Profit/Loss 1,269,649 745,021 665,449 Actual Profit/Loss does not include calculated charitable care of 437,089 contributing savings to the System. Increased productivity by 10% over previous year and exceeded our target this year by 18%. Total patient revenue increased by 11% over last year. Lifeline grew 29% over previous year on gain to operations CHOICES Program 20% gain to operations over previous year
SYSTEM GOAL: Quality
• Major Accomplishments • Scorecard Performance
o LOS Trends o Outcome Data
Six of twelve publicly reported clinical outcomes exceeded or equaled State and National scores. Two clinical outcomes in the top 20% of the nation. Two of our clinical staff received certifications in wound care, Carol Rothman, RN and Sharon Nottingham, RN. Carol was also awarded the Nursing Excellence Award. Established Cardiac Service Line. Successful AHCA Survey.
SYSTEM GOAL: Service
• Major Accomplishments • Scorecard Performance
o Inpatient Satisfaction o Outpatient Satisfaction
Patient Satisfaction annual score was 93.4% for Likelihood to Recommend.
SYSTEM GOAL: People
• Major Accomplishments • Scorecard Performance
o Employee Satisfaction o Vacancy Rates o Personnel Turnover
Lee Memorial Home Health exceeded the people goal by retaining newly hired staff within one year. The turnover rate was 7% while meeting the goal was targeted to be less than 22.5%. Eileen Hagenbrock, RN and Susan Killion were nominated for the Doc Coggins Award. Honey Lane nominated for the 2009 Rose of Care Award.
SYSTEM GOAL: Community
Major Accomplishments Scorecard Performance
Market Share Community Preference
Volumes increased by 4.3% from budget. Medicaid visits grew by 20% while total expenses decreased by 4% from previous year. Medicaid visits were 30.5% over budget. Charitable care increased by 14% over previous year.
Key Challenges & Opportunities
• Market Overview o Key Competitive Developments o Key Legislative or Political Developments o Key Technology Developments o Potential New Ventures and/or Businesses
Challenges/Opportunities Over 75 home health agencies in Lee County Optimize our financial performance through business development opportunities. Recruit and retain top performing staff. Improve Clinical Outcomes
Please complete with targeted information only, maximum 2 pages. Submit (thru SLC Member) ELECTRONICALLY to L Drive Miscellaneous “BOD Presentations” by Noon the Friday before the week you’re scheduled on agenda.
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
UPDATE REPORT TO THE BOARD (No Action Required)
DATE: May 3, 2010 NAME OF SERVICE LINE/ENTITY UPDATE: Hospitalist Presentations PERSON RESPONSIBLE & TITLE: Drs. Jon Burdzy, Yanet Rios and Chuck Krivenko KEY ACCOMPLISHMENTS Medical Department Standards for Inpatient Care and Hospitalist were approved by all Medical Staffs. Dr. Burdzy will review them with the Board. Dr. Rios will describe the Children’s Hospital Hospitalist Program which is functioning well with good patient satisfaction. Dr. Krivenko will review the hospitalist standards for contract hospitalist group to provide 24/7 coverage at all hospital facilities. GOALS (MET) Hospitalist standards were developed for inpatient and hospitalists care and endorsed by the Medical Staffs.
GOALS (UNMET) Contracting for 24/7 program at each of the facilities is in process.
FINANCIAL STATUS (including cash flow statement, projected cash flow, balance sheet and income statement) N/A PROBLEMS/ISSUES There is continued dissatisfaction with the present hospitalist program although there has been improvement had the LMH and HP campuses by the Cogent Hospitalist Group. ANTICIPATED NEEDS A scorecard and oversight of performance is planned and will be reviewed by the Medical Staff through the Quality Oversight Committee of the PLC. SUMMARY/COMMENTS Drs. Burdzy, Rios and Krivenko will review all inpatient and hospitalist’s standards and plans for continuing and improving service in the system.
Keep form to one page, SUBMIT (thru SLC Member) ELECTRONICALLY to L Drive – Miscellaneous - BOD Presentations by Noon the Friday before you’re scheduled on agenda.
BOD/Forms/Board UPDATE Report to the Board Form (Blue Form) – Updated 090209cs
Contracting Standards for Supported Hospitalist
LMHS Board of Directors May 13th, 2010
Chuck Krivenko, MDChief Medical Officer

Lee Memorial Health System
Hospitalist Services

Lee Memorial Health System
Physicians’ Perceptions of Hospitalist Services

Lee Memorial Health System
Aspects of Hospitalist Services(''Excellent'' Percentile Rankings)
Hospitalists' Availability to See Patients in Timely
Fashion
Communication & Feedback
Provided
Level of Competence
50th Percentile

• 24/7 in-house coverage with professional management of the Hospitalist Group.
• Designation of a lead hospitalist for each of the facility served to formally mentor other members of the hospitalist team.
• Arrange for qualified Hospitalists to staff the Facility with LMHS involvement in the selection process of new physicians.
• Board Certified in Internal Medicine or Family Practice or eligible to be admitted to the certification process and able to achieve board certification within the timeframe set forth in the Medical Staff Bylaws for the specialty of Internal Medicine or Family Practice.
• Meet all Medical Staff membership requirements.
• Orient the Hospitalists to their duties - New Hospitalist given a formal orientation to the bylaws, computer system, code of conduct, rules and regulations of the Medical Staff and Hospitalists Contracted Standard, in addition to an understanding of facility's leadership and House Supervisor Team.
Contracting Standards for Supported Hospitalist
• Mandatory use of computerized order-set or pre-printed order sets which are reviewed and acceptable to the system.
• Mandatory consultation with an intensivist on admission to the unit and limitation of clinical management to general internal medicine (no ventilator management, sedation protocols, hypotension management) unless on an interim emergency basis.
• Participate and provide leadership for the EPIC installation and the roll-out of CPOE.
• Monitor their performance to see that standard develop will be complied with in all respects with regular (monthly) participation in the review of incentive metrics in addition to other quality and services indicators with leadership of the facilities.
• Communicate with the primary care physician on admission, discharge and significant changes in a clinical condition.
• Communicate with PCP upon discharge and arrange to have the dictated discharge summary faxed to the PCP upon the patient’s discharge.
• Prepare legible standardized progress notes.
• Appropriate sign-off of clinical information between members of the group.
Contracting Standards for Supported Hospitalist
• Develop a method of handling critical values when reported from ancillary departments.
• Meet dress code appropriate to the professional duties.
• Limit the number of consultations to those necessary to achieve appropriate medical care for the patient.
• Work with consultant physicians to define clinical protocols that allow appropriate care and negate the necessity for consultations for commonly occurring conditions generally encountered by internal medicine Hospitalist physicians.
• Comply with the required telephonic communication physician to physician for all consultation requests on non-routine consults.
• Admit pregnant patient under 20 weeks with a primary medical diagnosis.
• Avoid requests for consultation prior to the hospitalist evaluating the patient, unless the situation is emergent as determined through consultation with the attending ED physician.
• Dictate the H&P as soon as possible to have a verbal transcription available.
Contracting Standards for Supported Hospitalist
• Work directly with the consulting physicians to determine the appropriate date for discharge.
• Eliminate all discharge dependency on consultants (Discharge if OK with…)
• Work directly with case management department to identify patient care options that facilitate the clinical and social recovery of the patient.
• Collaborate with the hospitalist group or groups then providing services at any other hospital facilities for appropriate communication and transfer arrangements prior to the actual transfer of the patient.
• Maintain telephone response time to departments and floors within 10 minutes.
• Maintain response time, in person when requested, to Emergency Department, Critical Care Units, and Progressive Care Units within 30 minutes of request for assistance, including overnight.
• Maintain response time, in person when requested, to Medical/Surgical units within 60 minutes of request for assistance.
Contracting Standards for Supported Hospitalist
• Maintain detailed written process for back-up coverage for situations when primary Hospitalist does not return calls and for situations when primary Hospitalist has multiple admissions pending simultaneously and inpatient services require Hospitalist attention.
• Achieving greater than ninety five percent (95%) completion of coding queries on active admissions to improve the accuracy of coding and to facilitate accurate categorization of clinical disease.
• Achieving greater than ninety five percent (95%) completion of dictations of H&Ps and/or approved Discharge Summaries within 24 hours of discharge order.
• Understand that each sections of the medical record should stand alone and should be an integral, cohesive part of the plan of care (do not copy consultant notes to the H&P).
• Maintaining a patient census that does not, on average, exceed 20 patients per Hospitalist per day.
• Adjust and reduce patient load to match the demands of critically ill patients. • Variances due to unusually high admission or discharge activity are acceptable as long
as the patient load limitations are adhered to in a good faith manner.
Contracting Standards for Supported Hospitalist

Pediatric Hospitalist GroupThe Children’s Hospital of SWFL
Background
Five years ago, due to the increasing needs of our community and under the scope of PICU services a new type of general hospital services was started to meet the unique needs of the patients, families and physicians in our environment.The newly created Pediatric Hospitalist Group evolved to become an independent and cohesive entity two years later .

Basic Principles
Voluntary Referrals
Dynamic Structure
High Qualification
Inpatient/ Outpatient Communication
Quality Indicators
Safe Transfer of CareTCH Pediatric Hospitalist group Continuity of Care
Our Group Vision
• Our Pediatric Hospitalist Program share a common vision dedicated to excellence in patient and family centered care, communication with each other and our colleagues, and a commitment to teaching and self- education.
• Our Group of Physicians are very well respected by their multidisciplinary colleagues for their attitude, work ethic, resourcefulness, and availability.
• We advocate for our individual patients and for patients globally within the health care system.
Our Current Structure
• 6 BC/BE Hospital-based Pediatricians leaded by a Medical Director who share same amount of clinical duties.
• We cover the General Pediatric Ward, Pediatric Surgical Unit, as well as Monitor Unit at HP and since last year the Pediatric Ward at CCH.
• We admit patients for ALL pediatricians and family doctors in our community and the majority of our subspecialists.
• We have presence on every committee at TCH, including The Leadership Council and THC Executive Committee.
Our Guidelines • Patient Care Timing:
1. All H&P’s dictated within 12 hours of admission. 2. A D/C Summary dictation should be completed at the
time of discharge.3. Fax to PCP to notify of discharge at the time of D/C,
verbal transferring of care( by phone conversation at the time of discharge) when necessary.
4. All patient should have a follow up physician referral at the time of discharge, no exceptions.
5. All calls should be answered within 15 minutes, no exceptions.
6. We have implemented an Action Plan for unanswered calls after 15 minutes that include Medical Director Involvement.

Our Guidelines
• Physician to Physician Communication1. All our consults are called directly to the subspecialist
and a phone conversation stating the specific concern at the time of request.
2. We discourage subspecialist making unilateral decisions in the care of our patients, so we discuss new treatment plan ideas, as well as new orders before they are written in a respectful and collegial manner.
3. The decision of discharge is ours and our discharge planning start at the time of admission.
4. Every test result that we receive after patient discharge is sent to PCPs in a timely fashion.

Our Results:
• Established protocols and evidence-based orders set to enforce standards of care on common pediatric diagnosis like Asthma, Bronchiolitis, Neonatal Sepsis and others.
• Improved families and primary care physician satisfaction scores.
• We have a voluntary referral of 100% from PCP’s in our community.
• Impressive decreased in length of stay.• Readmission rates below national standards.• Asthma Quality Indicators exceeding national expectations.• Safety initiatives implemented and overall elevation of
quality of care.

What’s next?
• Pediatric hospitalists bring a lot to the table, such as broad experience in treating acutely or chronically ill hospitalized children; the ability to coordinate care; knowledge in negotiating hospital routines and protocols; and the capacity to manage family fears.
• Implementing plans for the future of pediatric hospital medicine will require collaboration among the many specialists and groups involved in the care of children to ultimately shape it in the best benefit for them.

BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
UPDATE REPORT TO THE BOARD (No Action Required)
DATE: May 3, 2010 NAME OF SERVICE LINE/ENTITY UPDATE: Patient Safety Initiative Update PERSON RESPONSIBLE & TITLE: Chuck Krivenko, M.D., Chief Medical Officer KEY ACCOMPLISHMENTS The patient safety initiative continues in the system. This is an update of the April and May activities. GOALS (MET) Timeline and Goals to date have been met.
GOALS (UNMET)
FINANCIAL STATUS (including cash flow statement, projected cash flow, balance sheet and income statement) N/A PROBLEMS/ISSUES N/A ANTICIPATED NEEDS N/A SUMMARY/COMMENTS Status updates regarding the HPI safety initiative have been given in a verbal form. A powerpoint presentation on progress is included with a copy of the 1st SafeLee progress report. Dr. Krivenko will review progress in the following areas:
• Collegial Behavior Education • Leadership Education Completion • “Train the Trainer” Education Planning • SafeLee Progress Report completion • Physician Safety Group Planning and Recommendations. • Cultural Transformation Group activities
Keep form to one page, SUBMIT (thru SLC Member) ELECTRONICALLY to L Drive – Miscellaneous - BOD Presentations by Noon the Friday before you’re scheduled on agenda.
BOD/Forms/Board UPDATE Report to the Board Form (Blue Form) – Updated 090209cs

The disclosure of this document and the contents herein does not constitute a waiver of any and all protections afforded Patient Safety Work Product under either Florida state or federal law including but not limited to those under the Patient Safety Quality Improvement Act of 2005 and implementing regulations, 45 C.F.R. Part 3; 42 U.S.C. § 11111; §§395.0193 F.S. and 766.101 F.S.
LMHSPatient Safety Initiative Update
Board of Directors, May 13, 2010Chuck Krivenko, MD, Chief Medical Officer

Physician Education Conference Improving LMHS’ Patient Safety & Quality Care
• LMHS has partnered with Vanderbilt University School of Medicine’s Center for Patient and Professional Advocacy to present “Encouraging Collegial Relationships: Evaluating, Documenting, Treating and Monitoring Difficult Colleagues”.
– Friday Evening May 21 and Saturday May 22, 2010– The Resort At Marina Village, Tarpon Point Marina, Cape Coral
• Received RSVPs from 55 Physicians– 5 CCH MEC– 5 LMH MEC– 3 HP MEC– 4 GC MEC– 8 TCH MEC– 30 Other Physicians– 0 Special Physicians – 24 Administrators
SafeLee Educational Training• All module training of leadership will be completed
by May 14th by Dr. Morehead. • Staff training will begin with “training of the
trainers” on June 15th and 16th. This training will be done by Craig Clapper.
• Staff education will begin on August 2nd and continue to October 31st.
• Over 5,000 employees will be given a four hour course in use of tools and behaviors that improve safety.
SafeLee Communication Group
• Safety website is up and running.• Adding links for additional safety messages.• Safety Resource Center Library has been
developed in the LMH Medical Library.• The 1st SafeLee progress report will be
published in early May. It will include stories, event rates, and a graph of our progress.
Physician Safety Group• Five Nurses were added to the group.• Physician Education was planned:
1) Identifying learning objective, 2) Include hospitalists into the education and membership in the Physician
Safety Group, 3) Identify approximatley160 physicians to educate on the basis of volumes
and specialty,4) Video-tape the education session, 5) Get CME credit for the education, 6) Use Webinars to reach more physicians.
• Donna Giannuzzi and nursing members described the redesign of nursing handoffs - involving patients in a structured process of handoffs of information.
• Dave Morehead reviewed the literature regarding communications as a safety concern. The literature clearly identified that lack of hand-offs cause harm to patients.
Physician Safety Group Recommendations regarding Safe Communications
• The MEC and Physician Quality Committees should hold physicians and hospitalists accountable to the new medical department standard of using physician to physicians communication on all urgent cases. They should enforce the standard vigorously.
• Encourage the Health System to support a 24/7 in-house hospitalist program at each of the facilities.
• Encourage the use of electronic means of communication when possible.
• Encourage the Health System to develop a concierge physicians communication service which would be a single number through which a operator can locate consultants.

Cultural Transformation Group
• Group’s Purpose – Facilitate LMHS’ culture of safety transformation by ensuring the elements “tools and behaviors” of patient safety are integrated throughout LMHS.
• May 4th Organizational Meeting• Membership consist of 23 representatives throughout the system:
• Ancillary Svcs, Nursing, Trauma Svcs, Environmental Svcs, Transport, Housekeeping, IS, Spiritual Svcs, Patient Advocate, Supply Chain, Standards & Quality, Medical Staff Quality, Human Resources, Clinical Education, Risk Management, Physician Svcs.
• Group’s Goals: • Provide staff teamwork and communication training. • Implement leadership tools to hardwire safety behaviors into daily work life.• Implement physician training.• Identify, train and deploy “safety coaches”.• Prepare organization for and implement “red rules”.• Collect/analyze data to document results.
• May 13th – Educational Training by Dr. Morehead• May 18th – Group will meet on a regular basis (every 2 weeks)

Quality & Education Committee of the Whole
Pathology Dictation
(Tuck Wilson, M.D., Physician Leadership Council Consultant/Quality & Education Committee)
(Verbal Update Only)
There is no documentation for this item.
Unless the information you submit with this form is significantly enhanced
in color (i.e. graphs), please submit in black & white,
maximum 2 slides per page.
LMHS BOARD OF DIRECTORS RECOMMENDED ACTION FOR BOARD APPROVAL
(Action includes Acceptance, Approval, Adoption, etc)
Keep form to one page, SUBMIT (thru SLC Member) ELECTRONCIALLY
to L Drive Miscellaneous BOD Presentations by Noon the Friday before the week you’re
scheduled on agenda.
DATE: 5/07/10 LEGAL SERVICE REVIEW? YES___ NO_X_
SUBJECT: 1st Quarter FY 2010 Organizational Performance Measure Scorecard
REQUESTOR & TITLE: Dr. Krivenko, Chief Medical Officer/Clinical & Quality Services Dr. Greenberg, Medical Director/Medical Staff Services PREVIOUS BOARD ACTION ON THIS ITEM (IF ANY) (justification and/or background for recommendations – internal groups which support the recommendation i.e. SLC, Operating Councils, PMTs, etc.) The Quality Safety and Management Council reviewed and approved several of the indicators within the Organizational Performance Measure Scorecard on April 14, 2010. SPECIFIC PROPOSED MOTION: Approve the Organizational Performance Measure Scorecard: 1st Quarter Fiscal Year 2010. PROS TO RECOMMENDATION N/A
CONS TO RECOMMENDATION N/A
LIST AND EXPLAIN ALTERNATIVES CONSIDERED
N/A FINANCIAL IMPLICATIONS Budgeted ____ Non-Budgeted ____ (including cash flow statement, projected cash flow, balance sheet and income statement)
N/A OPERATIONAL IMPLICATIONS (including FTEs, facility needs, etc.)
N/A SUMMARY N/A
BOD/Forms/Board (Action) Reporting Form - revised 1/9/08/cs

PATIENT SAFETY WORK PRODUCT
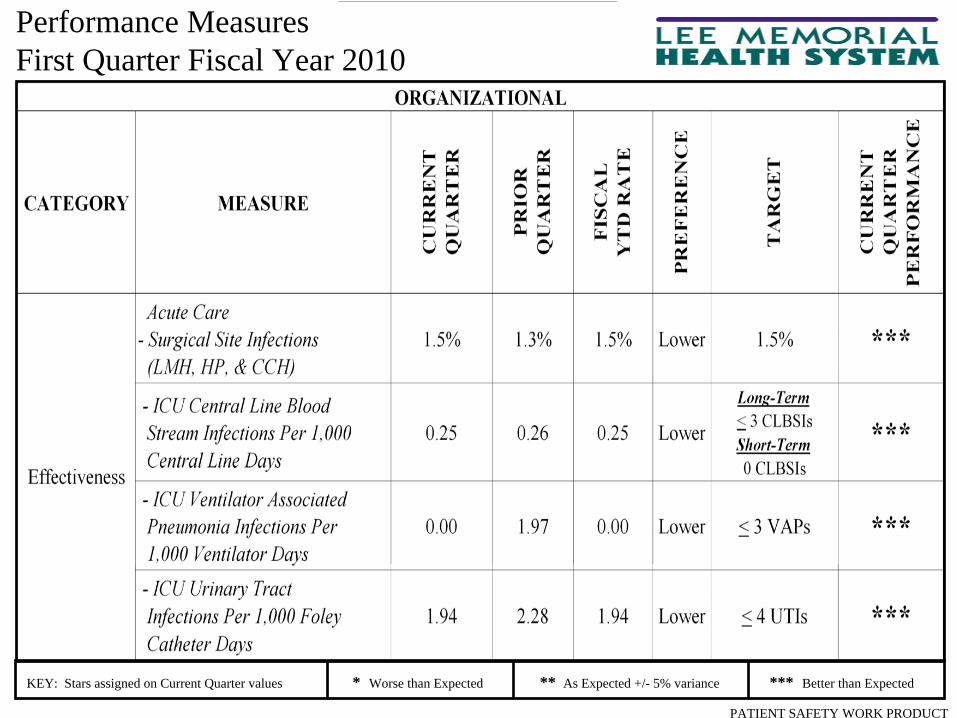
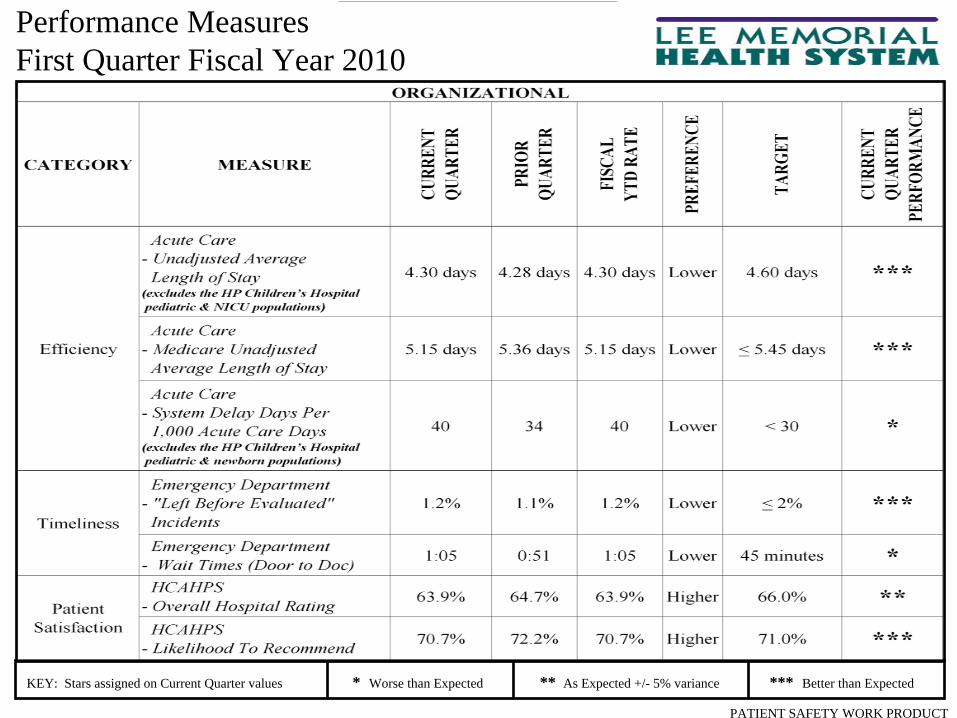
Performance Measures First Quarter Fiscal Year 2010
KEY: Stars assigned on Current Quarter values * Worse than Expected ** As Expected +/- 5% variance *** Better than Expected
PATIENT SAFETY WORK PRODUCT
Performance Measures First Quarter Fiscal Year 2010
KEY: Stars assigned on Current Quarter values * Worse than Expected ** As Expected +/- 5% variance *** Better than Expected

PATIENT SAFETY WORK PRODUCT
LongLong--Term TargetTerm Target
Data:
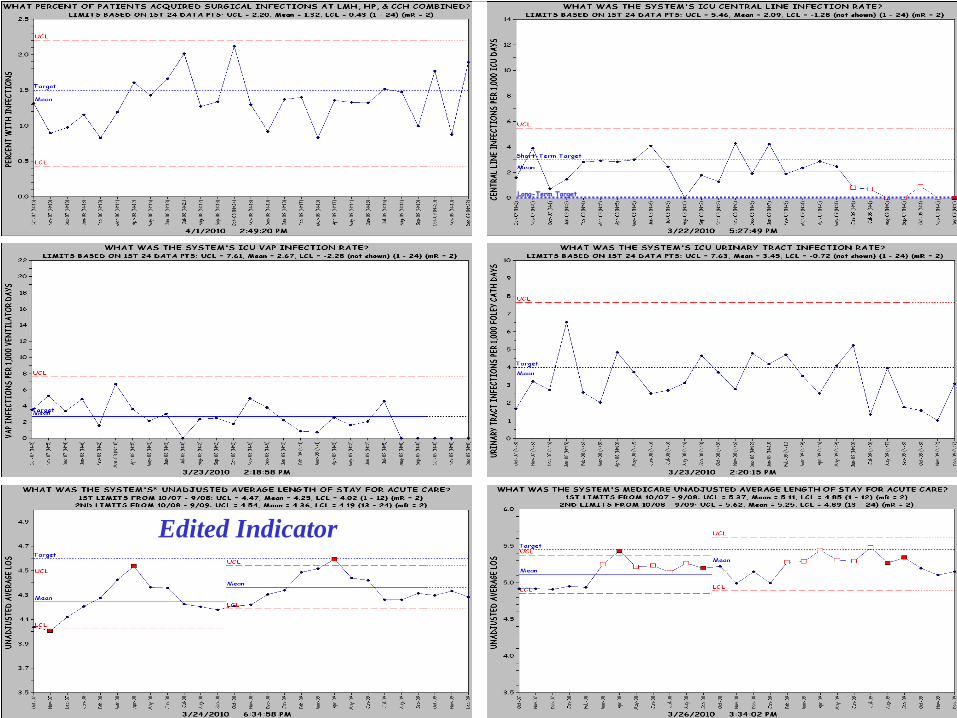
• Indicator Description: Monthly monitor of the adult ICU central line blood stream infections (CLBSIs)
• Formula: ([ICU CLBSIs / ICU central line days] * 1,000)
• Goal: < 3 CLBSIs / 1,000 central line days (internal short-term goal) 0 CLBSIs / 1,000 central line days (internal long-term goal)
• Why track: Complications cause increased risk and dissatisfaction among patient populations and increased cost to the health system and patient.
Current Status:
1st Quarter FY10
• Acute Care: 0.25 CLBSIs / 1,000 central line days (1 CLBSI / 3,965 central line days)
• Cape: 0.00 CLBSIs / 1,000 central line days (0 CLBSIs / 554 central line days)
• HealthPark: 0.00 CLBSIs / 1,000 central line days (0 CLBSIs / 977 central line days)
• Lee: 0.86 CLBSIs / 1,000 central line days (1 CLBSI / 1,165 central line days)
• Gulf Coast: 0.00 CLBSIs / 1,000 central line days (0 CLBSIs / 1,269 central line days)
Governing Body:
• Quality & Safety Management Council
Q:Q: ICU ICU –– CENTRAL LINE CENTRAL LINE BLOOD STREAM INFECTION BLOOD STREAM INFECTION
RATERATE
= = FavorableFavorable QSMC IndicatorQSMC Indicator

PATIENT SAFETY WORK PRODUCT
Data:
• Indicator Description: Monthly monitor of the adult ICU ventilator associated pneumonia infections (VAPs)
• Formula: ([ICU VAPs / ICU ventilator days] * 1,000)
• Goal: < 3 VAPs / 1,000 ventilator days (internal goal)
• Why track: Complications cause increased risk and dissatisfaction among patient populations and increased cost to the health system and patient.
Current Status:
1st Quarter FY10
• Acute Care: 0.00 VAPs / 1,000 ventilator days (0 VAPs / 2,682 ventilator days)
• Cape: 0.00 VAPs / 1,000 ventilator days (0 VAPs / 371 ventilator days)
• HealthPark: 0.00 VAPs / 1,000 ventilator days (0 VAPs / 771 ventilator days)
• Lee: 0.00 VAPs / 1,000 ventilator days (0 VAPs / 579 ventilator days)
• Gulf Coast: 0.00 VAPs / 1,000 ventilator days (0 VAPs / 961 ventilator days)
Governing Body:
• Quality & Safety Management Council
Q:Q: ICU ICU –– VENTILATOR VENTILATOR ASSOCIATED PNEUMONIA ASSOCIATED PNEUMONIA
INFECTION RATEINFECTION RATE
= = FavorableFavorable QSMC IndicatorQSMC Indicator
PATIENT SAFETY WORK PRODUCT
Performance Measures First Quarter Fiscal Year 2010
KEY: Stars assigned on Current Quarter values * Worse than Expected ** As Expected +/- 5% variance *** Better than Expected
PATIENT SAFETY WORK PRODUCT
Edited IndicatorEdited Indicator
Edited Indicator
Beginning March 2004, the Hospital Beginning March 2004, the Hospital Acquired Pressure Ulcers indicator includes Acquired Pressure Ulcers indicator includes
data from Southwest Florida Regional data from Southwest Florida Regional Medical Center and Gulf Coast Hospital / Medical Center and Gulf Coast Hospital /
Gulf Coast Medical CenterGulf Coast Medical CenterBeginning July 2008, the Patient Beginning July 2008, the Patient
Falls indicator excludes data Falls indicator excludes data from the Rehab Hospitalfrom the Rehab Hospital
Edited Indicator
PATIENT SAFETY WORK PRODUCT
Edited Indicator
LongLong--Term TargetTerm Target

PATIENT SAFETY WORK PRODUCT
WHAT % OF SYSTEM HCAHPS LIKELIHOOD TORECOMMEND RESPONSES WERE "DEFINITELY YES"?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct
-07
Nov
-07
Dec
-07
Jan-
08
Feb-
08
Mar
-08
Apr
-08
May
-08
Jun-
08
Jul-0
8
Aug
-08
Sep-
08
Oct
-08
Nov
-08
Dec
-08
Jan-
09
Feb-
09
Mar
-09
Apr
-09
May
-09
Jun-
09
Jul-0
9
Aug
-09
Sep-
09
Oct
-09
Nov
-09
Dec
-09
PERC
ENT "DEF
INIT
ELY YE
S" RES
PONSE
S
Beginning July 2008, the Delay Days Beginning July 2008, the Delay Days indicator includes data from Southwest indicator includes data from Southwest Florida Regional Medical Center and Florida Regional Medical Center and
Gulf Coast HospitalGulf Coast Hospital
Edited Indicator
WHAT % OF SYSTEM HCAHPS OVERALLHOSPITAL RATING SCORES WERE "9" & "10"?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct
-07
Nov
-07
Dec
-07
Jan-
08
Feb-
08
Mar
-08
Apr
-08
May
-08
Jun-
08
Jul-0
8
Aug
-08
Sep-
08
Oct
-08
Nov
-08
Dec
-08
Jan-
09
Feb-
09
Mar
-09
Apr
-09
May
-09
Jun-
09
Jul-0
9
Aug
-09
Sep-
09
Oct
-09
Nov
-09
Dec
-09
PERC
ENT "9" & "10" SCO
RES
TargetTarget
___________________ L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
OTHER ITEMS
___________________ L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
DATE OF THE NEXT REGULARLY SCHEDULED
MEETING
QUALITY Committee of the Whole
MEETING
Thursday, June 10, 2010
1:00pm
Lee Memorial Hospital Boardroom 2776 Cleveland Ave, Ft. Myers, FL 33901