brain microbleeds are associated with ambulatory blood pressure
TRANSCRIPT

Brain Microbleeds Are Associated With Ambulatory BloodPressure Levels in a Hypertensive Population
Leon H.G. Henskens, Robert J. van Oostenbrugge, Abraham A. Kroon,Peter W. de Leeuw, Jan Lodder
Abstract—Brain microbleeds, indicative of cerebral small-vessel disease, may occur with increased frequency in patientswith hypertension. However, little is known about the relation of these abnormalities with blood pressure levels. Weassessed the relation between ambulatory measured blood pressure and the presence of microbleeds in a cohort ofhypertensive patients without a history of cerebrovascular disease. A total of 218 participants (110 males, age 52.5�12.6years) underwent 24-hour ambulatory blood pressure monitoring twice (off-medication) and brain MRI to detectmicrobleeds and coexisting white matter hyperintensities. We performed logistic regression analyses to relate thefollowing blood pressure components (based on both recordings) to microbleeds: the mean 24-hour, awake, and asleepblood pressures; nocturnal hypertension (asleep pressure �120/70 mm Hg); nocturnal blood pressure dipping. Modelswere adjusted for age and sex, and additionally for cardiovascular risk factors and white matter hyperintensities. Wedetected microbleeds in 35 participants (16.1%; 95% confidence interval, 11.1% to 21.0%). On average, each standarddeviation increment in blood pressure, whether 24-hour, awake, or asleep, was significantly and independentlyassociated with a 1.8- to 1.9-fold higher likelihood for microbleeds (all models P�0.05). Similarly, the adjusted oddsratio for microbleeds was 5- to 6-fold higher in subjects diagnosed with nocturnal hypertension (all models P�0.05).Microbleeds were not associated with nocturnal dipping. In conclusion, brain microbleeds are frequently found inhypertensive patients without a history of cerebrovascular disease, and are independently associated with higher daytimeas well as night-time blood pressure levels. (Hypertension. 2008;51:62-68.)
Key Words: brain microbleeds � hypertension � blood pressure � MRI� ambulatory blood pressure monitoring � target-organ damage
Brain microbleeds (BMBs) are focal accumulations of he-mosiderin-containing macrophages in the perivascular
space of small blood vessels in the brain, indicating previousextravasation of blood.1 These abnormalities, which were de-scribed in the mid-1990s for the first time,2 can be identified assmall areas of signal loss on haem-sensitive T2*-weightedgradient echo (GE) MRI and remain detectable for years.3
In Caucasian populations, the prevalence of BMBs is about5% in healthy, mostly elderly individuals, increases to around25% in ischemic stroke patients, and goes even beyond 50%in patients affected by intracerebral hemorrhage; in popula-tions of Asian descent even higher prevalences have beenreported.4,5 The presence of BMBs has been associated withcognitive impairment, independent of coexisting ischemicbrain damage (in particular white matter changes).6,7 More-over, prospective data suggest that BMBs predict the recur-rence of both ischemic and hemorrhagic stroke,8–10 empha-sizing their potential clinical relevance.
Although BMBs may occur with increased frequency inpatients with hypertension4,5 and, accordingly, in conjunction
with hypertension-related damage of the heart and the brain,11,12
little is know about their relation with blood pressure (BP) levelsper se. Some studies have reported higher BP levels in subjectsdisplaying BMBs,9,13–15 but so far no study has primarilyfocused on the BP-microbleed relationship.
It has been shown that BP obtained by ambulatory BPmonitoring (ABPM) correlates closely with hypertension-related organ damage, and that its prognostic value, whetherdaytime, night-time, or 24-hour, is superior to that of BPmeasured in the office.16–18 Therefore, the objective of thepresent study was to assess the relation between BMBs andBP measured by ABPM in a cohort of hypertensive patientswithout a history of cerebrovascular disease.
Methods
ParticipantsBetween July 2004 and September 2006, all consecutive patientsreferred to our outpatient department for the evaluation of theirhypertension have been screened for participation in the present
Received August 28, 2007; first decision September 22, 2007; revision accepted November 2, 2007.From the Department of Internal Medicine (L.H.G.H., A.A.K., P.W.d.L.), Division of General Internal Medicine, Subdivision Vascular Medicine,
University Hospital Maastricht and Cardiovascular Research Institute Maastricht (CARIM), and the Department of Neurology (R.J.v.O., J.L.), UniversityHospital Maastricht and Cardiovascular Research Institute Maastricht (CARIM), Maastricht University, The Netherlands.
Correspondence to Leon H.G. Henskens, MD, Department of Internal Medicine, University Hospital Maastricht, P. Debyelaan 25, P.O. Box 5800, 6202AZ Maastricht, The Netherlands. E-mail [email protected]
© 2007 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.107.100610
62
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
arch 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
arch 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
arch 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
arch 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
arch 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from
by guest on M
arch 17, 2018http://hyper.ahajournals.org/
Dow
nloaded from
study. As part of the routine work-up, patients underwent ABPMover a 24-hour period, standard 12-lead electrocardiography, androutine laboratory investigations. Patients who were using antihy-pertensive medication were also instructed to discontinue treatmentat least 2 weeks before the BP measurements. An experiencedinternist decided, based on the patients’ clinical information pro-vided by the referring physician and independent of the study,whether it was possible to stop temporarily the antihypertensivemedication. Accordingly, patients who continued treatment wereexcluded from participation.
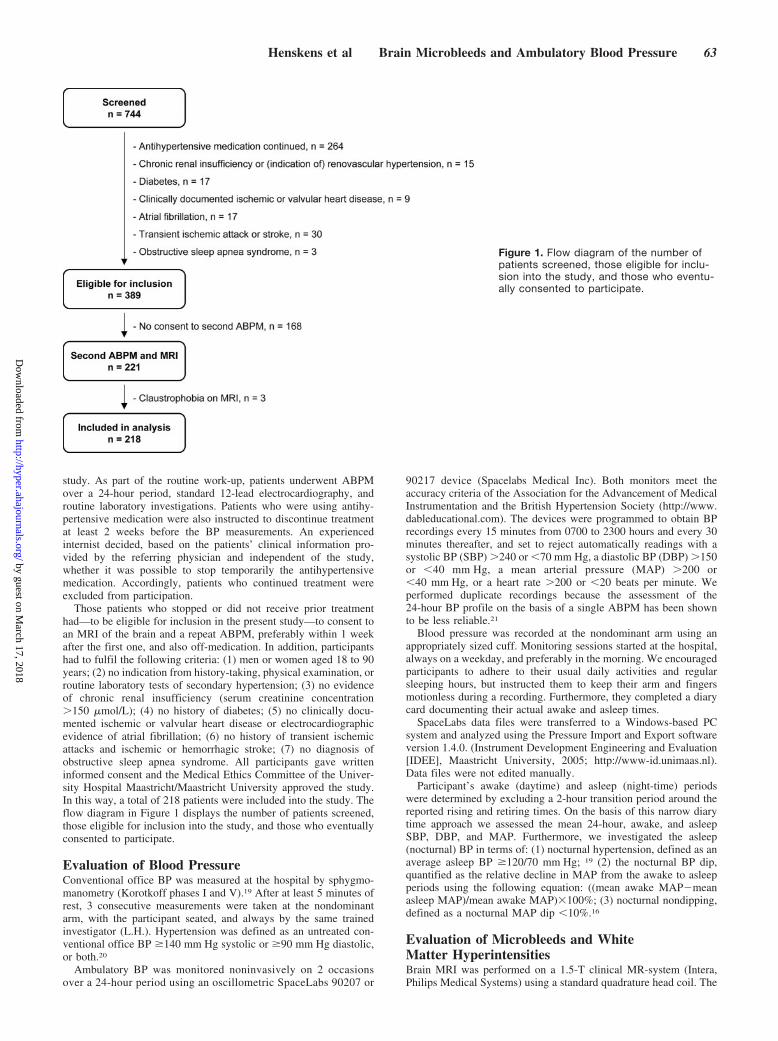
Those patients who stopped or did not receive prior treatmenthad—to be eligible for inclusion in the present study—to consent toan MRI of the brain and a repeat ABPM, preferably within 1 weekafter the first one, and also off-medication. In addition, participantshad to fulfil the following criteria: (1) men or women aged 18 to 90years; (2) no indication from history-taking, physical examination, orroutine laboratory tests of secondary hypertension; (3) no evidenceof chronic renal insufficiency (serum creatinine concentration�150 �mol/L); (4) no history of diabetes; (5) no clinically docu-mented ischemic or valvular heart disease or electrocardiographicevidence of atrial fibrillation; (6) no history of transient ischemicattacks and ischemic or hemorrhagic stroke; (7) no diagnosis ofobstructive sleep apnea syndrome. All participants gave writteninformed consent and the Medical Ethics Committee of the Univer-sity Hospital Maastricht/Maastricht University approved the study.In this way, a total of 218 patients were included into the study. Theflow diagram in Figure 1 displays the number of patients screened,those eligible for inclusion into the study, and those who eventuallyconsented to participate.
Evaluation of Blood PressureConventional office BP was measured at the hospital by sphygmo-manometry (Korotkoff phases I and V).19 After at least 5 minutes ofrest, 3 consecutive measurements were taken at the nondominantarm, with the participant seated, and always by the same trainedinvestigator (L.H.). Hypertension was defined as an untreated con-ventional office BP �140 mm Hg systolic or �90 mm Hg diastolic,or both.20
Ambulatory BP was monitored noninvasively on 2 occasionsover a 24-hour period using an oscillometric SpaceLabs 90207 or
90217 device (Spacelabs Medical Inc). Both monitors meet theaccuracy criteria of the Association for the Advancement of MedicalInstrumentation and the British Hypertension Society (http://www.dableducational.com). The devices were programmed to obtain BPrecordings every 15 minutes from 0700 to 2300 hours and every 30minutes thereafter, and set to reject automatically readings with asystolic BP (SBP) �240 or �70 mm Hg, a diastolic BP (DBP) �150or �40 mm Hg, a mean arterial pressure (MAP) �200 or�40 mm Hg, or a heart rate �200 or �20 beats per minute. Weperformed duplicate recordings because the assessment of the24-hour BP profile on the basis of a single ABPM has been shownto be less reliable.21
Blood pressure was recorded at the nondominant arm using anappropriately sized cuff. Monitoring sessions started at the hospital,always on a weekday, and preferably in the morning. We encouragedparticipants to adhere to their usual daily activities and regularsleeping hours, but instructed them to keep their arm and fingersmotionless during a recording. Furthermore, they completed a diarycard documenting their actual awake and asleep times.
SpaceLabs data files were transferred to a Windows-based PCsystem and analyzed using the Pressure Import and Export softwareversion 1.4.0. (Instrument Development Engineering and Evaluation[IDEE], Maastricht University, 2005; http://www-id.unimaas.nl).Data files were not edited manually.
Participant’s awake (daytime) and asleep (night-time) periodswere determined by excluding a 2-hour transition period around thereported rising and retiring times. On the basis of this narrow diarytime approach we assessed the mean 24-hour, awake, and asleepSBP, DBP, and MAP. Furthermore, we investigated the asleep(nocturnal) BP in terms of: (1) nocturnal hypertension, defined as anaverage asleep BP �120/70 mm Hg; 19 (2) the nocturnal BP dip,quantified as the relative decline in MAP from the awake to asleepperiods using the following equation: ((mean awake MAP�meanasleep MAP)/mean awake MAP)�100%; (3) nocturnal nondipping,defined as a nocturnal MAP dip �10%.16
Evaluation of Microbleeds and WhiteMatter HyperintensitiesBrain MRI was performed on a 1.5-T clinical MR-system (Intera,Philips Medical Systems) using a standard quadrature head coil. The
Figure 1. Flow diagram of the number ofpatients screened, those eligible for inclu-sion into the study, and those who eventu-ally consented to participate.
Henskens et al Brain Microbleeds and Ambulatory Blood Pressure 63
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from

standardized imaging protocol consisted of T2-weighted fast spinecho (repetition time [TR] 4820 ms; echo time [TE] 100 ms; flipangle 90°; field of view [FOV] 230 mm; acquisition matrix512�512), fluid-attenuated inversion recovery (FLAIR) (TR 8000ms; TE 120 ms; inversion time 2000 ms; FOV 230 mm; acquisitionmatrix 256�256 [reconstructed to 512X512]) and T2*-weighted GE(TR 736 ms; TE 23 ms; flip angle 15°; FOV 230 mm; acquisitionmatrix 256�256; in-plane spatial resolution 0.9�0.9 mm/pixel[resolution may be actually higher because of the T2*-effect3])sequences in the axial plane, producing 24 slices with a thickness of5 mm and a 0.5-mm interslice gap.
We defined BMBs as punctate (diameter �5 mm), homogeneousfoci of low signal intensity on T2*-weighted GE images.22 Thepresence of BMBs was assessed throughout the brain, eg, brain stem,cerebellum, basal ganglia, corona radiata, and cortico-subcorticalgray and white matter. Symmetric hypointensities in the globipallidi, likely to represent calcification or iron deposition, and sulcalflow voids from cortical vessels were disregarded.
White matter hyperintensities (WMH) were identified on T2-weighted and FLAIR images and classified according to Fazekas etal into hyperintensities of the deep and subcortical white matter(DWMH) and periventricular hyperintensities (PVH).23 We consid-ered WMH to be advanced in case of DWMH grades 2 or 3 (ie,beginning confluence of foci or large confluent areas) or PVH grade3 (ie, irregular hyperintensities extending into the deep white matter).Histopathologic and clinical data indicate that these advanced lesionsreflect ischemic brain damage related to a cerebral small-vesseldisease.24,25
Figure 2 illustrates, as an example, BMBs and advanced WMH inone of the participants.
Two independent raters (R.v.O. and J.L.), blinded to the partici-pants’ age, sex, and clinical status (including BP data), rated allscans. The inter-rater reliability, expressed as Cohen’s kappa, was0.68 for the presence of BMBs and 0.76 for advanced WMH.According to Landis and Koch, kappa values between 0.60 to 0.79indicate substantial agreement.26 In case of disagreement, lesionswere ascertained by consensus.
Evaluation of Risk FactorsInformation on lifestyle habits, past and current morbidity (includingcurrent treatment), and hypertension history (including the self-reported age of diagnosis and previous use of antihypertensivemedication), were obtained by interview and verified by inspectionof recently started medical records. The duration of hypertension wasestimated as the time (in months) passed since the self-reported ageof diagnosis until inclusion into the study. Smoking was classified asnever, past, or current. Height and weight were measured todetermine the body mass index (BMI, kg/m2). Venous blood sam-ples, routinely drawn after an overnight fast, were analyzed forserum total and high-density lipoprotein (HDL) cholesterol andserum creatinine using standard laboratory procedures. Hypercholes-terolemia was considered to be present in subjects who either usedlipid-lowering drugs or had untreated total cholesterol levels�6.5 mmol/L.
Statistical AnalysisBefore analyzing the relation between ambulatory BP and BMBswe tested the reproducibility of the duplicate ambulatory BPrecordings. A detailed description is given in the online supple-ment to this paper (please see the expanded Methods section athttp://hyper.ahajournals.org).
To detect group differences between unpaired data we applied theindependent samples t test for normally distributed variables, theMann–Whitney U test for variables with skewed distributions, andthe Pearson �2 statistic or Fisher’s exact test for categorical variables.
We performed logistic regression analyses to evaluate the relationbetween the aforementioned ambulatory BP components and thepresence of BMBs. Models were adjusted for age and sex (model 1),and additionally (ie, exploratory analyses) for cardiovascular riskfactors, ie, the duration of hypertension, previous antihypertensivetreatment, smoking status,5 and the ratio of total/HDL cholesterol27
(model 2). Finally, we also adjusted for the presence of advancedWMH (model 3).28 All covariates were forced into the modelsimultaneously (enter procedure).
Normally distributed variables are presented as mean�SD, vari-ables with skewed distributions as median with interquartile ranges(IQR), and categorical variables as frequencies. Odds ratios arepresented with corresponding 95% confidence intervals. A 2-tailedprobability value �0.05 was considered statistically significant.Analyses were performed using the statistical software packageSPSS (version 11.0.4 for Macintosh, SPSS Inc).
ResultsOf the 389 patients eligible for inclusion into the study, 218consented to participate (Figure 1). The remainder (n�171)did not differ significantly from the participants in terms ofage (50.4�14.4 versus 52.5�12.6 years, P�0.283) and sex
Figure 2. Example of brain MRI, showing both brain microb-leeds (BMBs) and advanced white matter hyperintensities(WMH) in one of the participants. A, T2*-GE images showingmultiple BMBs (white arrows) in the cerebellum (first image),one microbleed in the basal ganglia (second image), and onemicrobleed in the subcortical white matter (third image). B,FLAIR images (corresponding to the images of A) showingadvanced deep and periventricular WMH.
64 Hypertension January 2008
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from
(45.0% male versus 50.5%, P�0.287). The daytime MAPand DBP levels were slightly, yet significantly, higher inparticipants than in those who were not included into thestudy (MAP: 117�13 versus 114�13 mm Hg, P�0.045;DBP: 97�12 versus 94�12 mm Hg, P�0.016). However,refusal to participate was neither associated with the daytimesystolic pressure (156�18 versus 153�17 mm Hg, P�0.336)nor with the SBP, MAP as well as DBP levels during sleep(132/97/80�20/15/13 versus 131/95/77�19/14/12 mm Hg,P�0.460/0.143/0.056).
Characteristics According to Microbleed StatusMicrobleeds were observed in 35 of 218 participants (16.1%;95% confidence interval [CI], 11.1% to 21.0%). Twenty-twopatients displayed a single microbleed, 6 patients had 2, and7 patients showed 3 or more BMBs. The characteristics of thestudy population are summarized in Table 1. Participants withBMBs were older and had higher office BP levels than thosewithout (P�0.05). Based on the office pressures 207 (94.9%)patients were diagnosed with hypertension. Eleven (5.1%)participants had normal BP levels, and none of them dis-played BMBs on MRI. We observed no differences in theduration of hypertension or cardiovascular treatment, ie,previous antihypertensive treatment, or current use of anti-thrombotic and cholesterol lowering medication.
Advanced WMH were present in 46 of 218 participants(21.1%; 95% CI, 15.6% to 26.6%), being more prevalent insubjects with BMBs than in those without (48.6% versus15.8%, respectively; P�0.001).
Reproducibility of Ambulatory Blood PressureOf the 218 participants who underwent ABPM, duplicaterecordings were available in 213 (97.7%). Monitoring ses-sions were repeated with a median interval of 7 (IQR 5, 9)days. Detailed reproducibility data are given in the onlinesupplement to this paper (please see expanded results section,Table S1 and Figure S1A and S1B). Briefly, the reproduc-ibility of the mean 24-hour, awake, and asleep BPs wasacceptable (concordance ranging between 22.4 and 27.7% ofnearly maximal variation)29 and higher than that of therelative nocturnal BP dip (40.8%). The nocturnal BP status aswell as the dipping pattern were moderately reproducible(Cohen’s kappa 0.48 and 0.43, respectively).26 Therefore, andbecause an increasing number of BP readings improves thereliability of ambulatory BP components,30 all further analy-ses have been performed on the basis of both ABPMs(n�213). That is, we calculated the mean for continuous BPdata and classified participants as nocturnal hypertensive ornondipper when they confirmed their initial status on thesecond ABPM, otherwise subjects were labeled as normoten-sive or dipper, respectively (please see Table S1).
Ambulatory Blood Pressure andBrain MicrobleedsBrain MRI was performed with a median interval of 10 (IQR,7, 16) days after the first ABPM. Odds ratios quantifying therelation between the different ambulatory BP componentsand BMBs are summarized in Table 2. Higher 24-hour,awake, and asleep BP levels, and nocturnal hypertensionwere significantly associated with the presence of BMBs,independent of age and sex (Table 2, model 1; all P�0.01).For every SD increase in SBP, MAP, or DBP, the odds ratiosranged between 1.84 and 2.01 for the 24-hour period, be-tween 1.75 and 1.87 for the awake period, and between 1.80and 1.90 for the asleep period; a diagnosis of nocturnalhypertension was associated with a 5.45-fold higher likeli-hood for BMBs (Table 2, model 1). Additional adjustments(exploratory analyses) for cardiovascular risk factors, ie, theduration of hypertension, previous antihypertensive treat-ment, smoking, and the ratio of total/HDL cholesterol, did notaffect the associations substantially (Table 2, model 2). Finaladjustments for coexisting advanced WMH modified theresults of model 2 only slightly (Table 2, model 3).
DiscussionThe present study demonstrated that, in this hypertensivepopulation without a history of cerebrovascular disease, theprevalence of microbleeds in the brain was 16.1% (95% CI,11.1% to 21.0%), and that the daytime, nighttime, and24-hour BP levels and a diagnosis of nocturnal hypertensionwere associated with the presence of BMBs, independent ofage and sex, other cardiovascular risk factors, and coexistingischemic brain damage.
Table 1. Characteristics of the Study Population According toMicrobleed Status
Characteristics All (218)
Brain Microbleeds
Absent (183) Present (35)
Sex, n (%) male 110 (50.5) 90 (49.2) 20 (57.1)
Age, years 52.5�12.6 51.0�12.3 60.0�11.9†
BMI, kg/m2 28.2�4.9 28.3�5.1 27.4�3.3
Office BP, mm Hg
SBP 174�24 166�22 187�27†
DBP 104�13 103�12 108�14*
Heart rate, bpm 75�12 75�12 74�12
Smoking of cigarettes, n (%)
Never 87 (39.9) 72 (39.3) 15 (42.9)
Past 93 (42.7) 83 (45.4) 10 (28.6)
Current 38 (17.4) 28 (15.3) 10 (28.6)
Cholesterol, mmol/L
Total 5.9�1.2 5.9�1.2 5.7�0.9
HDL 1.4�0.4 1.4�0.4 1.4�0.4
Ratio total/HDL cholesterol 4.6�1.5 4.6�1.5 4.5�1.2
Hypercholesterolemia, n (%) 73 (33.6) 65 (35.7) 8 (22.9)
Creatinine, mmol/L 82 (71, 94) 82 (71, 93) 84 (72, 105)
Hypertension history
Duration of hypertension,months
44 (13, 134) 39 (13, 126) 60 (12, 164)
Previous antihypertensivetreatment, n (%)
178 (81.7) 149 (81.4) 29 (82.9)
n indicates number; BMI, body mass index; BP, blood pressure; SBP, systolicBP; DBP, diastolic BP; bpm, beats per minute; HDL, high-density lipoprotein.
*P�0.05; †P�0.001 vs brain microbleeds absent.
Henskens et al Brain Microbleeds and Ambulatory Blood Pressure 65
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from

The prevalence of BMBs in our hypertensive cohort isapproximately 3 times higher than that reported in the generalpopulation.4 Importantly, in our study the microbleed-countcould not have been influenced by a history of symptomaticcerebrovascular disease as this was an exclusion criterion.31,32
This, together with the observed associations between ambu-latory BP and BMBs, suggests that hypertension is a substan-tial and independent risk factor for the development ofBMBs.
The associations between the various ambulatory BP com-ponents and the presence of BMBs were robust and indepen-dent of age and sex, other cardiovascular risk factors, andadvanced WMH. On average, every SD increment in BP,whether 24-hour, daytime, or night-time, was associated witha 1.8- to 1.9-fold higher likelihood for BMBs. In the adjustedmodels the asleep BP, in addition to the awake pressure,remained significantly related to the presence of BMBs.Moreover, the associations were even stronger, confirmingearlier observations supporting the importance of a highnighttime BP.17,18 The finding that the likelihood for BMBswas 5- to 6-fold higher in subjects who were diagnosed withnocturnal hypertension further supports this.
Contrary, the nondipping status, in general considered tobe a strong determinant of hypertension-related organ dam-
age,33 was not related to the presence of BMBs. Also whenwe analyzed the day-to-night BP decline as a continuousvariable, adjusted associations were not significant. However,the prevalence of nondippers was small (n�15, 7.0%). This,along with the narrow and nearly significant 95% confidenceintervals of the odds ratios for BMBs associated with therelative nocturnal BP dip, reflects the low statistical power ofthese analyses to detect associations with BP dipping.
The mechanism behind hypertension-related BMBs re-mains speculative. Histopathologic studies have shown thatBMBs consist of macrophages containing hemosiderin—ablood breakdown product—adjacent to small blood vesselsaffected by moderate to severe fibrohyalinosis or arteriolo-sclerosis.1,34 Hence, a high BP during the day and additionallyat night, ie, a higher cumulative 24-hour BP load, couldinduce structural changes of the brain microvasculature withsubsequent extravasation of blood. A similar concept, ie,blood-brain barrier leakage of plasma components with hy-pertension as a major risk factor, has been proposed previ-ously as a cause of other types of small-vessel disease in thebrain, namely WMH and lacunar stroke.35 The associationsbetween BMBs and ambulatory BP in our study were notexplained by coexisting WMH, suggesting that the occur-
Table 2. Ambulatory BP Components in Relation to Brain Microbleeds (n�213)
BP Component
Brain Microbleeds
Unadjusted* Model 1* Model 2* Model 3*Absent (179) Present (34)
24-hour BP, mm Hg
SBP 148�17 161�19 2.02 (1.37–2.97)§ 1.84 (1.25–2.72)‡ 1.95 (1.27–2.97)‡ 1.84 (1.17–2.92)‡
MAP 111�12 119�14 1.82 (1.24–2.66)‡ 1.94 (1.29–2.92)‡ 2.07 (1.34–3.19)‡ 1.94 (1.23–3.07)‡
DBP 92�11 98�14 1.58 (1.08–2.30)† 2.01 (1.31–3.06)‡ 2.13 (1.33–3.41)‡ 1.98 (1.24–3.17)‡
Awake BP, mm Hg
SBP 154�17 166�21 1.91 (1.30–2.81)§ 1.75 (1.19–2.58)‡ 1.81 (1.19–2.77)‡ 1.72 (1.12–2.62)†
MAP 116�12 123�16 1.68 (1.18–2.40)‡ 1.81 (1.24–2.66)‡ 1.92 (1.24–2.95)‡ 1.79 (1.16–2.77)‡
DBP 97�11 101�15 1.45 (1.00–2.11)† 1.87 (1.22–2.85)‡ 1.95 (1.25–3.06)‡ 1.82 (1.14–2.92)†
Asleep BP, mm Hg
SBP 129�19 142�16 1.98 (1.37–2.86)§ 1.80 (1.24–2.62)‡ 1.91 (1.27–2.87)‡ 1.80 (1.15–2.82)‡
MAP 95�13 104�12 1.88 (1.28–2.76)‡ 1.90 (1.30–2.80)‡ 2.01 (1.30–3.12)‡ 1.90 (1.23–2.95)‡
DBP 78�12 84�12 1.68 (1.15–2.44)‡ 1.89 (1.27–2.82)‡ 2.01 (1.28–3.14)‡ 1.89 (1.21–2.95)‡
Nocturnalhypertension, n (%)
Yes 123 (68.7) 31 (91.2) 4.71 (1.38–16.04)† 5.45 (1.54–19.27)‡ 6.03 (1.62–22.54)† 5.35 (1.42–20.24)†
No 56 (31.3) 3 (8.8)
Nocturnal BP dipping
Relative BP dip, % 18�7 15�7 1.48 (1.02–2.14)† 1.35 (0.93–1.96) 1.41 (0.95–2.10) 1.36 (0.92–2.03)
Non-dipper, n (%) 11 (6.1) 4 (11.8) 2.04 (0.61–6.82) 1.71 (0.49–5.96) 1.49 (0.40–5.49) 1.43 (0.38–5.44)
Dipper, n (%) 168 (93.9) 30 (88.2)
BP indicates blood pressure; SBP, systolic BP; MAP, mean arterial pressure; DBP, diastolic BP; n, No.*Data are presented as the odds ratios (95% confidence interval) associated with a 1 SD increase in 24-hour, awake, or asleep BPs; a 1 SD decrease in the relative
nocturnal BP dip; or the presence of the nocturnal hypertension status or the nondipping pattern. The SDs of the respective SBP, MAP, and DBP were 18, 13, and12 mm Hg for the 24-hour period, 18, 13, and 12 mm Hg for the awake period, and 19, 14, and 12 mm Hg for the asleep period; the SD of the relative nocturnalBP dip was 7%.
Model 1: adjusted for age and sex.Model 2: additionally adjusted for duration of hypertension, previous antihypertensive treatment, smoking and ratio of total/HDL cholesterol.Model 3: additionally adjusted for advanced white matter hyperintensities.†P�0.05; ‡P�0.01; §P�0.001.
66 Hypertension January 2008
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from

rence and mechanisms of both abnormalities are, at least inpart, independent.
The present study has limitations, such as the cross-sectional design and the relatively small number of partici-pants displaying BMBs. Although the group size was suffi-cient to carry out the logistic regression analyses corrected forage and sex, the additional adjustments (models 2 and 3),having an exploratory nature, need to be interpreted withinthe context of their statistical limitations. Hence, our findingsrequire confirmation in longitudinal and adequately poweredstudies. Another limitation is the lack of a local, preferablycommunity based, control population. Such a control groupwould have enabled us to assess whether the prevalence ofBMBs in our hypertensive cohort was really increased.Furthermore, it is possible that we failed to include patientswith more severe hypertension, because they were not al-lowed to stop their antihypertensive medication. However,we would expect an even higher prevalence of BMBs andmore robust associations with ambulatory BP when partici-pants with more severe hypertension had been included.
On the other hand, we performed our study in a largecohort of well-defined hypertensive patients whose data werecollected prospectively. Moreover, demographic and BP dataof the participants were similar to those who did not consentto the study. Another strength of the study is that the BP wasmeasured by ABPM and, importantly, on two occasions.Based on the reproducibility analyses we used the data ofboth recordings. Other investigators previously have shownthat this improves the reliability of the calculated BP com-ponents.21,30 Finally, the observed associations were notbiased by concurrent antihypertensive treatment36 or a historyof symptomatic stroke.31,32 The latter implies that the detectedBMBs in our participants were all silent.
PerspectivesOur study showed that BMBs are a frequent finding inhypertensive patients without a history of cerebrovasculardisease. Moreover, the data suggest that participants with ahigh daytime and especially nighttime BP, ie, a high 24-hourBP load, were more likely to display BMBs on MRI. Incontrast to the general belief that BMBs are clinically silent,recently reported associations with cognitive impairment6,7
and an increased risk of stroke recurrence8,9—processes thatmay be accelerated in the face of a persistently high BP—illustrate the potential clinical relevance of these smalllesions. Considering all this, we postulate that BMBs shouldbe considered as an additional (besides WMH and lacunarinfarcts) and independent marker of hypertensive target-organ damage of the brain. Our findings need, however,confirmation in adequately powered and preferably long-termfollow-up studies, which also should address the role ofBMBs in risk estimation and prevention of both future strokeand impairment of brain function.
DisclosuresNone.
References1. Fazekas F, Kleinert R, Roob G, Kleinert G, Kapeller P, Schmidt R,
Hartung HP. Histopathologic analysis of foci of signal loss on
gradient-echo T2*-weighted MR images in patients with spontaneousintracerebral hemorrhage: evidence of microangiopathy-relatedmicrobleeds. AJNR. 1999;20:637–642.
2. Offenbacher H, Fazekas F, Schmidt R, Koch M, Fazekas G, Kapeller P.MR of cerebral abnormalities concomitant with primary intracerebralhematomas. AJNR. 1996;17:573–578.
3. Roob G, Fazekas F. Magnetic resonance imaging of cerebral microbleeds.Curr Opin Neurol. 2000;13:69–73.
4. Koennecke HC. Cerebral microbleeds on MRI: prevalence, associations,and potential clinical implications. Neurology. 2006;66:165–171.
5. Cordonnier C, Al-Shahi Salman R, Wardlaw J. Spontaneous brainmicrobleeds: systematic review, subgroup analyses and standards forstudy design and reporting. Brain. 2007;130:1988–2003.
6. Werring DJ, Frazer DW, Coward LJ, Losseff NA, Watt H, Cipolotti L,Brown MM, Jager HR. Cognitive dysfunction in patients with cerebralmicrobleeds on T2*-weighted gradient-echo MRI. Brain. 2004;127:2265–2275.
7. Won Seo S, Hwa Lee B, Kim EJ, Chin J, Sun Cho Y, Yoon U, Na DL.Clinical significance of microbleeds in subcortical vascular dementia.Stroke. 2007;38:1949–1951.
8. Boulanger JM, Coutts SB, Eliasziw M, Gagnon AJ, Simon JE, Subra-maniam S, Sohn CH, Scott J, Demchuk AM. Cerebral microhemorrhagespredict new disabling or fatal strokes in patients with acute ischemicstroke or transient ischemic attack. Stroke. 2006;37:911–914.
9. Fan YH, Zhang L, Lam WW, Mok VC, Wong KS. Cerebral microbleedsas a risk factor for subsequent intracerebral hemorrhages among patientswith acute ischemic stroke. Stroke. 2003;34:2459–2462.
10. Jeon SB, Kang DW, Cho AH, Lee EM, Choi CG, Kwon SU, Kim JS.Initial microbleeds at MR imaging can predict recurrent intracerebralhemorrhage. J Neurol. 2007;254:508–512.
11. Kwa VI, Franke CL, Verbeeten B Jr, Stam J. Silent intracerebral micro-hemorrhages in patients with ischemic stroke. Amsterdam VascularMedicine Group. Ann Neurol. 1998;44:372–377.
12. Lee SH, Park JM, Kwon SJ, Kim H, Kim YH, Roh JK, Yoon BW. Leftventricular hypertrophy is associated with cerebral microbleeds in hyper-tensive patients. Neurology. 2004;63:16–21.
13. Roob G, Schmidt R, Kapeller P, Lechner A, Hartung HP, Fazekas F. MRIevidence of past cerebral microbleeds in a healthy elderly population.Neurology. 1999;52:991–994.
14. Werring DJ, Coward LJ, Losseff NA, Jager HR, Brown MM. Cerebralmicrobleeds are common in ischemic stroke but rare in TIA. Neurology.2005;65:1914–1918.
15. Viswanathan A, Guichard JP, Gschwendtner A, Buffon F, Cumurcuic R,Boutron C, Vicaut E, Holtmannspotter M, Pachai C, Bousser MG,Dichgans M, Chabriat H. Blood pressure and haemoglobin A1c areassociated with microhaemorrhage in CADASIL: a two-centre cohortstudy. Brain. 2006;129:2375–2383.
16. Verdecchia P, Schillaci G, Guerrieri M, Gatteschi C, Benemio G, BoldriniF, Porcellati C. Circadian blood pressure changes and left ventricularhypertrophy in essential hypertension. Circulation. 1990;81:528–536.
17. Dolan E, Stanton A, Thijs L, Hinedi K, Atkins N, McClory S, Den HondE, McCormack P, Staessen JA, O’Brien E. Superiority of ambulatoryover clinic blood pressure measurement in predicting mortality: theDublin outcome study. Hypertension. 2005;46:156–161.
18. Staessen JA, Thijs L, Fagard R, O’Brien ET, Clement D, de Leeuw PW,Mancia G, Nachev C, Palatini P, Parati G, Tuomilehto J, Webster J.Predicting cardiovascular risk using conventional vs ambulatory bloodpressure in older patients with systolic hypertension. Systolic Hyper-tension in Europe Trial Investigators. JAMA. 1999;282:539–546.
19. O’Brien E, Asmar R, Beilin L, Imai Y, Mallion JM, Mancia G, MengdenT, Myers M, Padfield P, Palatini P, Parati G, Pickering T, Redon J,Staessen J, Stergiou G, Verdecchia P. European Society of Hypertensionrecommendations for conventional, ambulatory and home blood pressuremeasurement. J Hypertens. 2003;21:821–848.
20. 2003 European Society of Hypertension-European Society of Cardiologyguidelines for the management of arterial hypertension. J Hypertens.2003;21:1011–1053.
21. Manning G, Rushton L, Donnelly R, Millar-Craig MW. Variability ofdiurnal changes in ambulatory blood pressure and nocturnal dippingstatus in untreated hypertensive and normotensive subjects. Am JHypertens. 2000;13:1035–1038.
22. Wardlaw JM, Lewis SC, Keir SL, Dennis MS, Shenkin S. Cerebralmicrobleeds are associated with lacunar stroke defined clinically andradiologically, independently of white matter lesions. Stroke. 2006;37:2633–2636.
Henskens et al Brain Microbleeds and Ambulatory Blood Pressure 67
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from

23. Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA. MR signalabnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR.1987;149:351–356.
24. Fazekas F, Kleinert R, Offenbacher H, Schmidt R, Kleinert G, Payer F,Radner H, Lechner H. Pathologic correlates of incidental MRI whitematter signal hyperintensities. Neurology. 1993;43:1683–1689.
25. Pantoni L, Garcia JH. Pathogenesis of leukoaraiosis: a review. Stroke.1997;28:652–659.
26. Landis JR, Koch GG. The measurement of observer agreement for cate-gorical data. Biometrics. 1977;33:159–174.
27. Lee SH, Bae HJ, Yoon BW, Kim H, Kim DE, Roh JK. Low concentrationof serum total cholesterol is associated with multifocal signal loss lesionson gradient-echo magnetic resonance imaging: analysis of risk factors formultifocal signal loss lesions. Stroke. 2002;33:2845–2849.
28. Kim DE, Bae HJ, Lee SH, Kim H, Yoon BW, Roh JK. Gradient echomagnetic resonance imaging in the prediction of hemorrhagic vs ischemicstroke: a need for the consideration of the extent of leukoariosis. ArchNeurol. 2002;59:425–429.
29. Thijs L, Staessen J, Fagard R, Zachariah P, Amery A. Number ofmeasurements required for the analysis of diurnal blood pressureprofile. J Hum Hypertens. 1994;8:239 –244.
30. Fotherby MD, Potter JF. Reproducibility of ambulatory and clinic bloodpressure measurements in elderly hypertensive subjects. J Hypertens.1993;11:573–579.
31. Kinoshita T, Okudera T, Tamura H, Ogawa T, Hatazawa J. Assessmentof lacunar hemorrhage associated with hypertensive stroke by echo-planar gradient-echo T2*-weighted MRI. Stroke. 2000;31:1646–1650.
32. Lee SH, Kwon SJ, Kim KS, Yoon BW, Roh JK. Cerebral microbleeds inpatients with hypertensive stroke. Topographical distribution in the su-pratentorial area. J Neurol. 2004;251:1183–1189.
33. Staessen JA, Asmar R, De Buyzere M, Imai Y, Parati G, Shimada K,Stergiou G, Redon J, Verdecchia P. Task Force II: blood pressure mea-surement and cardiovascular outcome. Blood Press Monit. 2001;6:355–370.
34. Tanaka A, Ueno Y, Nakayama Y, Takano K, Takebayashi S. Smallchronic hemorrhages and ischemic lesions in association with spon-taneous intracerebral hematomas. Stroke. 1999;30:1637–1642.
35. Wardlaw JM, Sandercock PA, Dennis MS, Starr J. Is breakdown of theblood-brain barrier responsible for lacunar stroke, leukoaraiosis, anddementia? Stroke. 2003;34:806–812.
36. Lee SH, Heo JH, Yoon BW. Effects of microbleeds on hemorrhagedevelopment in leukoaraiosis patients. Hypertens Res. 2005;28:895–899.
68 Hypertension January 2008
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from
Jan LodderLéon H.G. Henskens, Robert J. van Oostenbrugge, Abraham A. Kroon, Peter W. de Leeuw and
Hypertensive PopulationBrain Microbleeds Are Associated With Ambulatory Blood Pressure Levels in a
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2007 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/HYPERTENSIONAHA.107.1006102008;51:62-68; originally published online December 10, 2007;Hypertension.
http://hyper.ahajournals.org/content/51/1/62World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org/content/suppl/2007/11/15/HYPERTENSIONAHA.107.100610.DC1Data Supplement (unedited) at:
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on March 17, 2018
http://hyper.ahajournals.org/D
ownloaded from

Title page
Full title: BRAIN MICROBLEEDS ARE ASSOCIATED WITH AMBULATORY
BLOOD PRESSURE LEVELS IN A HYPERTENSIVE POPULATION
Authors:
Léon H.G. Henskens, MDa
Robert J. van Oostenbrugge, MD PhDb
Abraham A. Kroon, MD PhDa
Peter W. de Leeuw, MD PhDa
Jan Lodder, MD PhDb
Affiliations: a Department of Internal Medicine, Division of General Internal Medicine, Subdivision
Vascular Medicine, University Hospital Maastricht and Cardiovascular Research Institute
Maastricht (CARIM), Maastricht University, Maastricht, The Netherlands. b Department of Neurology, University Hospital Maastricht and Cardiovascular Research
Institute Maastricht (CARIM), Maastricht University, Maastricht, The Netherlands.
Short title: Brain microbleeds and ambulatory blood pressure
Word count of manuscript: 5.540 (including title page, abstract, text, references, legends, tables and figures)
Word count of abstract: 245
Number of figures: 2
Corresponding author:
Léon H.G. Henskens, MD, Department of Internal Medicine, University Hospital
Maastricht, P. Debyelaan 25, P.O. Box 5800, 6202 AZ Maastricht, The Netherlands.
Telephone: +31 43 388 2136; fax: +31 43 387 5006; e-mail:

- 1 -
ONLINE SUPPLEMENT: REPRODUCIBILITY OF AMBULATORY BLOOD
PRESSURE COMPONENTS
Methods
The reproducibility of the 24-hour, awake and asleep BP levels, and the relative nocturnal BP
dip, was determined according to Bland and Altman by calculating coefficients of
repeatability, defined as twice the standard deviation (SD) of the differences between the
duplicate recordings.1 To enable comparisons between the different BP components, the
repeatability coefficients were expressed as a percentage of the nearly maximal variation,
calculated as four times the SD of the average of the two recordings.2 High percentages of
nearly maximal variation indicate considerable variation between the repeated recordings,
reflecting lower reproducibility. To determine the reproducibility of the nocturnal
hypertension status and the non-dipping pattern we investigated the number of participants
who confirmed their initial classification on the second ABPM. Kappa statistics were applied
to evaluate the consistency of these classifications. According to Landis and Koch, kappa
values below 0.40 signified poor, 0.40 to 0.59 moderate, 0.60 to 0.79 substantial, and values
above 0.80 outstanding reproducibility.3 Differences between related BP data were assessed
using the paired-samples t-test or McNemar’s test when appropriate

- 2 -
Results
Differences in mean 24-hour, awake and asleep BP levels, and the relative nocturnal BP dip
between the first and second ABPM were small (all <0.5 mmHg) and not statistically
significant (Table S1, P>0.05). The repeatability coefficient (expressed as a percentage of the
nearly maximal variation) of the relative nocturnal BP dip was higher, indicating lower
reproducibility, than that of the 24-hour, awake as well as asleep BPs (Table S1).
One-hundred-and-fifty-four (72.3%) participants confirmed their initial nocturnal
hypertension status on the second ABPM, 24 (11.3%) were normotensive on both sessions
and 35 (16.4 %) showed a variable nocturnal normotension/hypertension pattern (Figure
S1A). The nocturnal BP status was moderately reproducible (Table S1, Cohen’s kappa 0.48).
Fifteen (7.0%) subjects showed a non-dipping pattern on both sessions, 169 (79.4%)
confirmed their initial dipping status and 29 (13.6%) showed a variable dipping/non-dipping
pattern (Figure S1B). The dipping status was also moderately reproducible (Table S1,
Cohen’s kappa 0.43). Differences in proportions of nocturnal hypertensives as well as non-
dippers between the first and second ABPM were non-significant (Table S1, P>0.05)

- 3 -
References
1. Bland JM, Altman DG. Statistical methods for assessing agreement between two
methods of clinical measurement. Lancet. 1986;1:307-310.
2. Staessen J, Bulpitt CJ, O'Brien E, Cox J, Fagard R, Stanton A, Thijs L, Van Hulle S,
Vyncke G, Amery A. The diurnal blood pressure profile. A population study. Am J
Hypertens. 1992;5:386-392.
3. Landis JR, Koch GG. The measurement of observer agreement for categorical data.
Biometrics. 1977;33:159-174.

- 4 -
Figure legends
Figure S1A
Reproducibility of the nocturnal hypertension status. HH indicates hypertensive on both
ABPMs (prevalence 72.3%); HN, hypertensive on the first, normotensive on the second
ABPM (6.5%); NH, normotensive on the first, hypertensive on the second ABPM (9.9%);
NN, normotensive on both ABPMs (11.3%).
Figure S1B
Reproducibility of the dipping pattern. NN indicates non-dipper on both ABPMs (prevalence
7.0%); ND, non-dipper on the first, dipper on the second ABPM (8.9%); DN, dipper on the
first, non-dipper on the second ABPM (4.7%); DD, dipper on both ABPMs (79.4%).

- 5 -
Table
Table S1 Reproducibility of ambulatory BP components
BP component Ambulatory BP* Reproducibility†
First Second Combined
24-hour BP, mmHg:
SBP 150.3 ± 18.5 150.3 ± 18.3 150.3 ± 17.9 16.4 (22.9)
MAP 112.3 ± 13.2 112.3 ± 13.2 112.3 ± 12.9 11.8 (22.9)
DBP 93.3 ± 11.8 93.2 ± 11.9 93.3 ± 11.6 10.4 (22.4)
Awake BP, mmHg:
SBP 155.6 ± 18.7 156.0 ± 18.8 155.8 ± 18.6 18.3 (24.6)
MAP 116.8 ± 13.4 117.0 ± 13.5 116.9 ± 13.0 13.1 (25.2)
DBP 97.4 ± 12.1 97.4 ± 12.2 97.4 ± 11.9 11.4 (23.9)

- 6 -
Table I continued
Asleep BP, mmHg
SBP 131.3 ± 20.1 131.1 ± 18.7 131.2 ± 18.8 19.0 (25.3)
MAP 96.4 ± 14.5 96.5 ± 13.5 96.4 ± 13.6 14.4 (26.5)
DBP 78.9 ± 12.8 79.2 ± 11.9 79.0 ± 11.9 13.2 (27.7)
Relative nocturnal BP (MAP) dip, % 17.5 ± 8.0 17.4 ± 7.3 17.5 ± 7.1 11.6 (40.8)
Nocturnal hypertension, n (%):
Yes 168 (78.9) 175 (82.2) 154 (72.3)‡ 0.48
No 45 (21.1) 38 (17.8) 59 (27.7)
Nocturnal non-dipping, n (%):
Yes 34 (16.0) 25 (11.7) 15 (7.0)§ 0.43
No 179 (84.0) 188 (88.3) 198 (93.0)

- 7 -
* Ambulatory BP levels of the first and second monitoring session, and on the basis of both ABPMs (combined). Differences in continuous as
well as categorical ambulatory BP components between the first and second monitoring session were all non-significant (P>0.05, paired samples
t-test and McNemar's test, respectively).
† Reproducibility of ambulatory BP components expressed as the Bland-Altman coefficient of repeatability (% of nearly maximal variation) for
continuous data, and Cohen's kappa for categorical data.
‡ Nocturnal hypertension present on both ABPMs.
§ Non-dipping pattern present on both ABPMs.

- 8 -
Figures
Figure S1A

- 9 -
Figure S1B