brewster central school district instructional support
TRANSCRIPT

Page 1 of 4
Brewster Central School District Instructional Support Team Minutes
Kindergarten Student’s Name: _______________________ Date: ________________ Teacher’s Name: ________________ Grade: _______________ Date parent notified of IST referral __________ D. O. B. ______________ Prior IST Referral: Y / N Date ___________ Present: __ R. Young __ J. Conroy __ P. Sieker __ S. Chamberlain __ R. Mueller Principal Asst. Principal Psychologist Speech & Language Social Worker Special Education Teacher: Reading Teacher: Remedial Math: Other: Reason for Referral: __________________________________________________________________________ What would you like the IST to accomplish? According to prior reports, are the present concerns similar? Please be specific. List several strengths, talents, or specific interests for this student: Special Area Reports: Gym: Music: Art: Library: Recess: SERVICES Current Services LEVEL OF SERVICE Prior Services LEVEL OF SERVICE ___Consultant teacher _________________ ___ _________________ ___AIS Reading/ELA _________________ ___ _________________ ___AIS Math _________________ ___ _________________ ___Speech and Language _______________ ___ _________________ ___ESL _________________ ___ _________________ ___Counseling _________________ ___ _________________ ___OT _________________ ___ _________________ ___PT _________________ ___ _________________ ___APE _________________ ___ _________________ ___Assistive Technology _________________ ___ _________________ Days absent this year________ Tardiness ____________ Early Pick-up ____________ Other (please explain) _________________________________________________________________________________ With whom does the child reside? ________________________________________________________________________ Primary language spoken in the home_____________________________________________________________________ Current Family or Student Stressors (illness, separation/divorce, etc.) ____________________________________________ Prior School Experience other than Brewster: Place __________________________ Grade(s) ______________________
Page 2 of 4
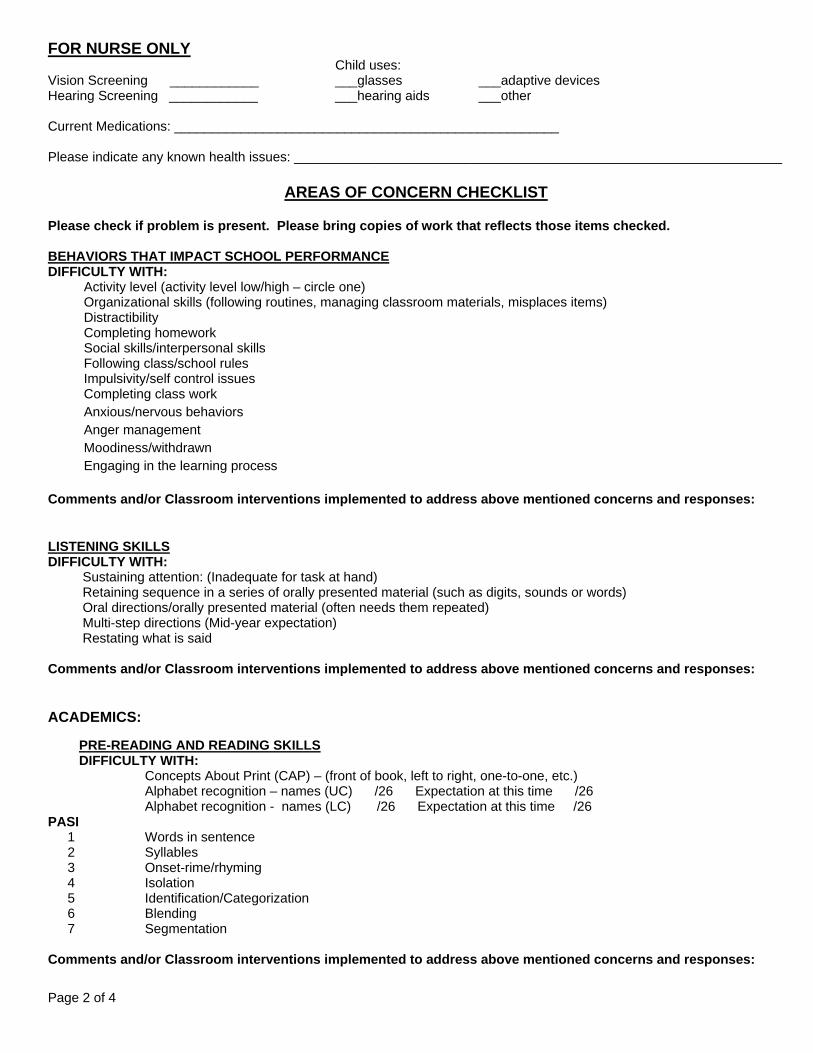
FOR NURSE ONLY
Child uses: Vision Screening ____________ ___glasses ___adaptive devices Hearing Screening ____________ ___hearing aids ___other Current Medications: ____________________________________________________ Please indicate any known health issues: __________________________________________________________________
AREAS OF CONCERN CHECKLIST
Please check if problem is present. Please bring copies of work that reflects those items checked. BEHAVIORS THAT IMPACT SCHOOL PERFORMANCE DIFFICULTY WITH: Activity level (activity level low/high – circle one) Organizational skills (following routines, managing classroom materials, misplaces items) Distractibility Completing homework Social skills/interpersonal skills Following class/school rules Impulsivity/self control issues Completing class work Anxious/nervous behaviors Anger management Moodiness/withdrawn Engaging in the learning process Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: LISTENING SKILLS DIFFICULTY WITH: Sustaining attention: (Inadequate for task at hand) Retaining sequence in a series of orally presented material (such as digits, sounds or words) Oral directions/orally presented material (often needs them repeated) Multi-step directions (Mid-year expectation) Restating what is said Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: ACADEMICS: PRE-READING AND READING SKILLS
DIFFICULTY WITH: Concepts About Print (CAP) – (front of book, left to right, one-to-one, etc.) Alphabet recognition – names (UC) /26 Expectation at this time /26 Alphabet recognition - names (LC) /26 Expectation at this time /26 PASI
1 Words in sentence 2 Syllables 3 Onset-rime/rhyming 4 Isolation 5 Identification/Categorization 6 Blending 7 Segmentation
Comments and/or Classroom interventions implemented to address above mentioned concerns and responses:

Page 3 of 4
WRITING SKILLS DIFFICULTY WITH: Conventional pencil grip Writing (slow or awkward) Letter reversals Attach Writing Sample Rubric Level _____________ Class Rubric Level _____________ Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: MATHEMATICAL SKILLS DIFFICULTY WITH: One-to-one correspondence Number identification Rote Counting Number reversals Identifying/creating patterns Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: COMMUNICATION DIFFICULTY WITH: Verbal expression Making inferences/drawing conclusions Following multi-step directions Grasping abstract concepts Grammatical and/or syntax errors when speaking or writing Pragmatic language (taking turns, topic maintenance, sustaining eye contact) Comprehending and using grade-level vocabulary Interpreting social cues Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: ACCOMMODATIONS List specific classroom accommodations that demonstrate differentiated instruction for the student (NOT RTI): READING SCORES PASI Level __________ Class PASI Level ________ Grade Level Expectation ___________ DIBELS Benchmark Scores ISF LNF PSF NWF ORF Kindergarten 8B 25M 8B 27M 40E 18M 35E 13M 25E
Additional Assessments/Comments (informal assessments and screenings) Please attach copies of most recent report cards, any raw current state test score data and practice data and any additional narrative statement from teach

Page 4 of 4
INTERVENTIONS Tier I (Classroom Teacher Directed) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
Assessment Date
Targeted Skills Group
Earobics
Leap into Phonics
RAZ Kids
Other
Other
Tier II (AIS and/or Related Service - Direct) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
AssessmentDate
Targeted Skills Group
Language for Learning
Fundations: Double Dose
Earobics
Read Naturally
Edmark
Soar to Success
RAZ-Kids
Other
Other
Tier III (Special Education and/or Related Services - Direct) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
Assessment Date
Targeted Skills Group
Fundations: Double Dose
Earobics
Read Naturally
Edmark
RAZ-Kids
Other

Page 1 of 5
Brewster Central School District Instructional Support Team Minutes
First-Grade Student’s Name: _______________________ Date: ________________ Teacher’s Name: ________________ Grade: _______________ Date parent notified of IST referral __________ D. O. B. ______________ Prior IST Referral: Y / N Date ___________ Present: __ R. Young __ J. Conroy __ P. Sieker __ S. Chamberlain __ R. Mueller Principal Asst. Principal Psychologist Speech & Language Social Worker Special Education Teacher: Reading Teacher: Remedial Math: Other: Reason for Referral: __________________________________________________________________________ What would you like the IST to accomplish? According to prior reports, are the present concerns similar? Please be specific. List several strengths, talents, or specific interests for this student: Special Area Reports: Gym: Music: Art: Library: Recess: SERVICES Current Services LEVEL OF SERVICE Prior Services LEVEL OF SERVICE ___Consultant teacher _________________ ___ _________________ ___AIS Reading/ELA _________________ ___ _________________ ___AIS Math _________________ ___ _________________ ___Speech and Language _______________ ___ _________________ ___ESL _________________ ___ _________________ ___Counseling _________________ ___ _________________ ___OT _________________ ___ _________________ ___PT _________________ ___ _________________ ___APE _________________ ___ _________________ ___Assistive Technology _________________ ___ _________________ Days absent this year________ Tardiness ____________ Early Pick-up ____________ Other (please explain) _________________________________________________________________________________ With whom does the child reside? ________________________________________________________________________ Primary language spoken in the home_____________________________________________________________________ Current Family or Student Stressors (illness, separation/divorce, etc.) ____________________________________________ Prior School Experience other than Brewster: Place__________________ Grade(s) ______________________

Page 2 of 5
FOR NURSE ONLY Child uses:
Vision Screening ____________ ___glasses ___adaptive devices Hearing Screening ____________ ___hearing aids ___other Current Medications: ____________________________________________________ Please indicate any known health issues: __________________________________________________________________
AREAS OF CONCERN CHECKLIST
Please check if problem is present. Please bring copies of work that reflects those items checked. BEHAVIORS THAT IMPACT SCHOOL PERFORMANCE DIFFICULTY WITH: Activity level (activity level low/high – circle one) Organizational skills (following routines, managing classroom materials, misplaces items) Distractibility Completing homework Social skills/interpersonal skills Following class/school rules Impulsivity/self control issues Completing class work Anxious/nervous behaviors Anger management Moodiness/withdrawn Engaging in the learning process Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: LISTENING SKILLS DIFFICULTY WITH: Sustaining attention: (inadequate for task at hand) Retaining sequence in a series of orally presented material (such as digits, sounds or words) Oral directions/orally presented material (often needs them repeated) Multi-step directions Restating what is said Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: ACADEMICS: PRE-READING AND READING SKILLS
DIFFICULTY WITH: Alphabet recognition – names (UC) /26 Expectation at this time /26 Alphabet recognition - names (LC) /26 Expectation at this time /26 Letter-sound Task - /31 Expectation at this time /31 Grade-level sight words PASI
1 Words in sentence 2 Syllables 3 Onset-rime/rhyming 4 Isolation 5 Identification/Categorization 6 Blending 7 Segmentation 8 Addition (initial/final – circle one/both) 9 Deletion (initial/final – circle one/both) 10 Substitution (initial/final – circle one/both)

Page 3 of 5
Identifying long vowels Identifying short vowels Reading two and three letter words “Sound blending” syllables into words Sounding out words when reading Decoding words: (whole word and/or phonological substitutions – circle one/both) Self-correcting errors when reading Referring back to the passage to answer comprehension questions Retelling: (explaining what was read/sequence of story events – circle one/both) Comprehension (main ideas/details/context clues/beginning inference skills – circle those that
apply) Following written directions Remembering details of what he/she read Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: WRITING SKILLS DIFFICULTY WITH: Conventional pencil grip Writing (slow or awkward) Proper letter formations and/or letter reversals Putting words in the correct order when writing sentences Writing complete sentences Writing down thoughts Staying on topic Attach Writing Sample Rubric Level _____________ Class Rubric Level _____________ Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: MATHEMATICAL SKILLS DIFFICULTY WITH: One-to-one correspondence Number identification Rote Counting Number formation and/or reversals Basic operation skills (addition, subtraction) Concepts (concrete/abstract – circle one/both) Math vocabulary Identifying/creating patterns Recalling facts automatically Calculations (slow) Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: COMMUNICATION DIFFICULTY WITH: Verbal expression Making inferences/drawing conclusions Following multi-step directions Grasping abstract concepts Grammatical and/or syntax errors when speaking or writing Pragmatic language (taking turns, topic maintenance, sustaining eye contact) Comprehending and using grade-level vocabulary Interpreting social cues Comments and/or Classroom interventions implemented to address above mentioned concerns and responses:

Page 4 of 5
ACCOMMODATIONS List specific classroom accommodations that demonstrate differentiated instruction for the student: READING SCORES DRA Level __________ Class Average _________ Grade Level Expectation _______ PASI Level __________ Class PASI Level ______ Grade Level Expectation _______ PSI Level ___________ Class PSI Level _______ Grade Level Expectation _______ DIBELS Benchmark Scores LNF PSF NWF ORF First 37B 35B 35M 35E 24B 50M 50E 20M 40E
Additional Assessments/Comments (informal assessments and screenings) Please attach copies of most recent report cards, any raw current state test score data and practice data and any additional narrative statement from teach

Page 5 of 5
INTERVENTIONS Tier I (Classroom Teacher Directed) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
Assessment Date
Targeted Skills Group
Earobics
Leap into Phonics
RAZ Kids
Other
Other
Tier II (AIS and/or Related Service - Direct) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
AssessmentDate
Targeted Skills Group
Language for Learning
Fundations: Double Dose
Earobics
Read Naturally
Edmark
Soar to Success
RAZ-Kids
Other
Other
Tier III (Special Education and/or Related Services - Direct) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
Assessment Date
Targeted Skills Group
Fundations: Double Dose
Earobics
Read Naturally
Edmark
RAZ-Kids
Other
Page 1 of 7
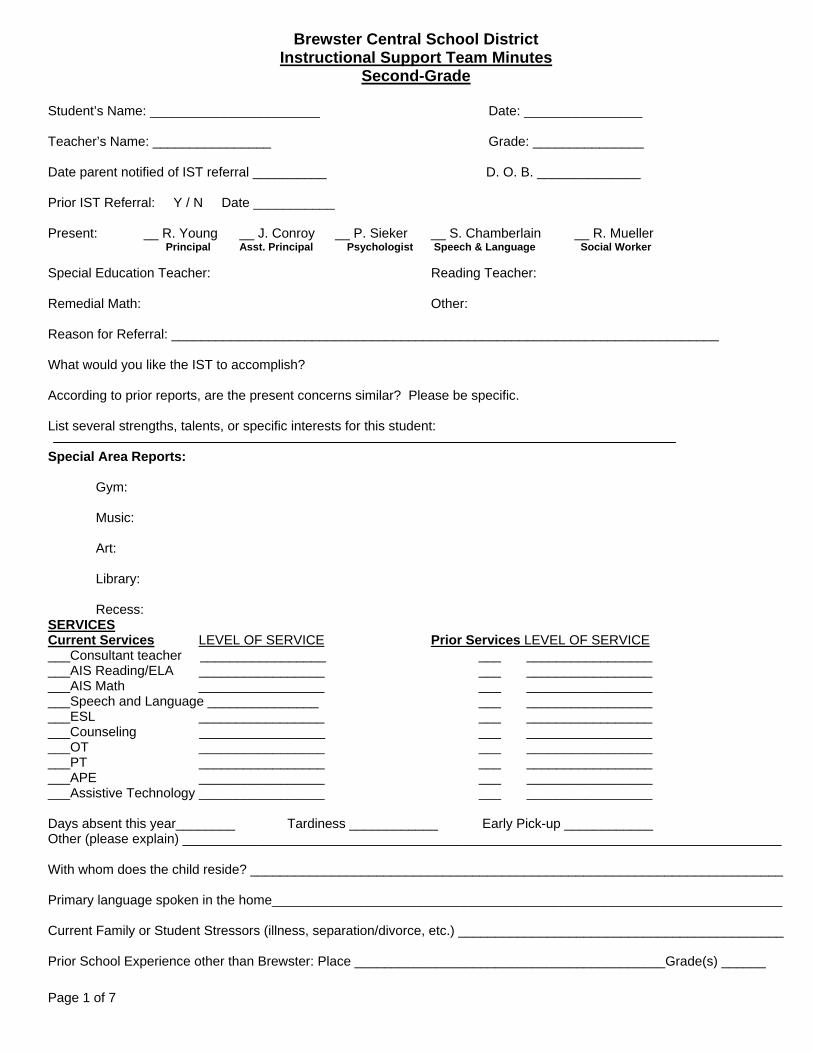
Brewster Central School District Instructional Support Team Minutes
Second-Grade
Student’s Name: _______________________ Date: ________________ Teacher’s Name: ________________ Grade: _______________ Date parent notified of IST referral __________ D. O. B. ______________ Prior IST Referral: Y / N Date ___________ Present: __ R. Young __ J. Conroy __ P. Sieker __ S. Chamberlain __ R. Mueller Principal Asst. Principal Psychologist Speech & Language Social Worker Special Education Teacher: Reading Teacher: Remedial Math: Other: Reason for Referral: __________________________________________________________________________ What would you like the IST to accomplish? According to prior reports, are the present concerns similar? Please be specific. List several strengths, talents, or specific interests for this student: Special Area Reports: Gym: Music: Art: Library: Recess: SERVICES Current Services LEVEL OF SERVICE Prior Services LEVEL OF SERVICE ___Consultant teacher _________________ ___ _________________ ___AIS Reading/ELA _________________ ___ _________________ ___AIS Math _________________ ___ _________________ ___Speech and Language _______________ ___ _________________ ___ESL _________________ ___ _________________ ___Counseling _________________ ___ _________________ ___OT _________________ ___ _________________ ___PT _________________ ___ _________________ ___APE _________________ ___ _________________ ___Assistive Technology _________________ ___ _________________ Days absent this year________ Tardiness ____________ Early Pick-up ____________ Other (please explain) _________________________________________________________________________________ With whom does the child reside? ________________________________________________________________________ Primary language spoken in the home_____________________________________________________________________ Current Family or Student Stressors (illness, separation/divorce, etc.) ____________________________________________ Prior School Experience other than Brewster: Place __________________________________________Grade(s) ______

Page 2 of 7
FOR NURSE ONLY Child uses:
Vision Screening ____________ ___glasses ___adaptive devices Hearing Screening ____________ ___hearing aids ___other Current Medications: ____________________________________________________ Please indicate any known health issues: __________________________________________________________________

Page 3 of 7
AREAS OF CONCERN CHECKLIST
Please check if problem is present. Please bring copies of work that reflects those items checked. BEHAVIORS THAT IMPACT SCHOOL PERFORMANCE DIFFICULTY WITH: Activity level (activity level low/high – circle one) Organizational skills (following routines, managing classroom materials, misplaces items) Distractibility Completing homework Social skills/interpersonal skills Following class/school rules Impulsivity/self control issues Completing class work Planning of long-term projects Anxious/nervous behaviors Anger management Moodiness/withdrawn Engaging in the learning process Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: LISTENING SKILLS DIFFICULTY WITH: Sustaining attention: (Inadequate for task at hand) Retaining sequence in a series of orally presented material (such as digits, sounds or words) Oral directions/orally presented material (often needs them repeated) Multi-step directions Restating what is said Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: ACADEMICS: PRE-READING AND READING SKILLS
DIFFICULTY WITH: Grade-level sight words PASI
1 Words in sentence 2 Syllables 3 Onset-rime/rhyming 4 Isolation 5 Identification/Categorization 6 Blending 7 Segmentation 8 Addition (initial/final – circle one/both) 9 Deletion (initial/final – circle one/both) 10 Substitution (initial/final – circle one/both)
Identifying long vowels Identifying short vowels Reading two and three letter words “Sound blending” syllables into words Sounding out words when reading Decoding words: (visual and/or phonological substitutions – circle one/both) Self-correcting errors when reading Reading silently: (Sub-vocalizing) Referring back to the passage to answer comprehension questions Retelling: (explaining what was read/sequence of story events – circle one/both) Comprehension (main ideas/details/context clues/beginning inference skills – circle those that

Page 4 of 7
apply) Following written directions Remembering details of what he/she read Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: WRITING SKILLS DIFFICULTY WITH: Conventional pencil grip Writing (slow or awkward) Proper letter formations and/or letter reversals Mechanics (use of capitals, punctuation) Spelling in written work (circle which apply: omits letters, adds letters, letters out of order, omits
suffix-ed) Writing (circle which apply: omits words in sentences; uses poor grammar; incorrect word order;
incomplete sentences; off topic) Writing down thoughts Vocabulary usage (simpler than in speech) Expanding an answer or providing details when writing Organizing thoughts in written work
Attach Writing Sample Rubric Level _____________ Class Rubric Level _____________ Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: MATHEMATICAL SKILLS DIFFICULTY WITH: One-to-one correspondence Number identification Rote Counting Number formation and/or reversals Basic operation skills (addition, subtraction) Concepts (concrete/abstract – circle one/both) Math vocabulary Identifying/creating patterns Number concepts, place value to 1000
Number sense (addition & subtraction to sums of 20) Recalling facts automatically Calculations (slow) Multi-step calculation problems/regrouping Multi-step equation word problems Solving word problems (circle what applies: identifying clue word, calculation errors, choosing
correct operation, choosing strategy) Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: COMMUNICATION DIFFICULTY WITH: Verbal expression Making inferences/drawing conclusions Following multi-step directions Grasping abstract concepts Grammatical and/or syntax errors when speaking or writing Pragmatic language (taking turns, topic maintenance, sustaining eye contact) Comprehending and using grade-level vocabulary Interpreting social cues Comments and/or Classroom interventions implemented to address above mentioned concerns and responses:

Page 5 of 7
ACCOMMODATIONS List specific classroom accommodations that demonstrate differentiated instruction for the student (NOT RTI): READING SCORES DRA Level __________ Class Average _________ Grade Level Expectation _______ PASI Level __________ Class PASI Level ________ Grade Level Expectation _______ PSI Level ____________ Class PSI Level _________ Grade Level Expectation _______ DIBELS Benchmark Scores NWF ORF Second 50B 44B 68M 90E
Additional Assessments/Comments (informal assessments and screenings) Please attach copies of most recent report cards, any raw current state test score data and practice data and any additional narrative statement from teach

Page 6 of 7
INTERVENTIONS Tier I (Classroom Teacher Directed) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
Assessment Date
Targeted Skills Group
Earobics
Leap into Phonics
RAZ Kids
Other
Other
Tier II (AIS and/or Related Service - Direct) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
AssessmentDate
Targeted Skills Group
Language for Learning
Fundations: Double Dose
Earobics
Read Naturally
Edmark
Soar to Success
RAZ-Kids
Other
Other
Tier III (Special Education and/or Related Services - Direct) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
Assessment Date
Targeted Skills Group
Fundations: Double Dose
Earobics
Read Naturally
Edmark
RAZ-Kids
Other

Page 7 of 7

Page 1 of 7
Brewster Central School District Instructional Support Team Minutes
Third-Grade
Student’s Name: _______________________ Date: ________________ Teacher’s Name: ________________ Grade: _______________ Date parent notified of IST referral __________ D. O. B. ______________ Prior IST Referral: Y / N Date ___________ Present: __ R. Young __ J. Conroy __ P. Sieker __ S. Chamberlain __ R. Mueller Principal Asst. Principal Psychologist Speech & Language Social Worker Special Education Teacher: Reading Teacher: Remedial Math: Other: Reason for Referral: __________________________________________________________________________ What would you like the IST to accomplish? According to prior reports, are the present concerns similar? Please be specific. List several strengths, talents, or specific interests for this student: Special Area Reports: Gym: Music: Art: Library: Recess: SERVICES Current Services LEVEL OF SERVICE Prior Services LEVEL OF SERVICE ___Consultant teacher _________________ ___ _________________ ___AIS Reading/ELA _________________ ___ _________________ ___AIS Math _________________ ___ _________________ ___Speech and Language _______________ ___ _________________ ___ESL _________________ ___ _________________ ___Counseling _________________ ___ _________________ ___OT _________________ ___ _________________ ___PT _________________ ___ _________________ ___APE _________________ ___ _________________ ___Assistive Technology _________________ ___ _________________ Days absent this year________ Tardiness ____________ Early Pick-up ____________ Other (please explain) _________________________________________________________________________________ With whom does the child reside? ________________________________________________________________________ Primary language spoken in the home_____________________________________________________________________ Current Family or Student Stressors (illness, separation/divorce, etc.) ____________________________________________ Prior School Experience other than Brewster Place____ _______________________________________Grade(s) ______

Page 2 of 7
FOR NURSE ONLY Child uses:
Vision Screening ____________ ___glasses ___adaptive devices Hearing Screening ____________ ___hearing aids ___other Current Medications: ____________________________________________________ Please indicate any known health issues: __________________________________________________________________

Page 3 of 7
AREAS OF CONCERN CHECKLIST
Please check if problem is present. Please bring copies of work that reflects those items checked. BEHAVIORS THAT IMPACT SCHOOL PERFORMANCE DIFFICULTY WITH: Activity level (activity levels low/high – circle one) Organizational skills (following routines, managing classroom materials, misplaces items) Distractibility Completing homework Social skills/interpersonal skills Following class/school rules Impulsivity/self control issues Completing class work Planning of long-term projects Anxious/nervous behaviors Anger management Moodiness/withdrawn Engaging in the learning process Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: LISTENING SKILLS DIFFICULTY WITH: Sustaining attention: (Inadequate for task at hand) Retaining sequence in a series of orally presented material (such as digits, sounds or words) Oral directions/orally presented material (often needs them repeated) Multi-step directions Restating what is said Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: ACADEMICS: PRE-READING AND READING SKILLS
DIFFICULTY WITH: Grade-level sight words “Sound blending” syllables into words Sounding out words when reading Decoding words: (visual and/or phonological substitutions – circle one/both) Self-correcting errors when reading Reading silently: (Sub-vocalizing) Referring back to the passage to answer comprehension questions Retelling: (explaining what was read/sequence of story events – circle one/both) Comprehension (main ideas/details/context clues/inference skills – circle those that apply) Following written directions Remembering details of what he/she read Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: WRITING SKILLS DIFFICULTY WITH: Conventional pencil grip Writing (slow or awkward) Proper letter formations and/or letter reversals Mechanics (use of capitals, punctuation) Spelling in written work (circle which apply: omits letters, adds letters, letters out of order, omits
suffix-ed...)

Page 4 of 7
Writing (circle which apply: omits words in sentences; uses poor grammar; incorrect word order; incomplete sentences; off topic)
Vocabulary usage (simpler than in speech) Expanding an answer or providing details when writing Organization in written work
Attach Writing Sample Rubric Level _____________ Class Rubric Level _____________ Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: MATHEMATICAL SKILLS DIFFICULTY WITH: “Skip” counting Number reversals Basic operation skills (addition, subtraction, multiplication, division) Concepts (concrete/abstract – circle one/both) Math vocabulary Identifying/creating patterns Number concepts, place value to 1000
Number sense (addition, subtraction, multiplication, division) Recalling facts automatically Calculations (slow) Multi-step calculation problems Multi-step equation word problems Decoding word problems Solving word problems (circle what applies: identifying clue word, calculation errors, choosing
correct operation, choosing strategy) Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: COMMUNICATION DIFFICULTY WITH: Verbal expression Making inferences/drawing conclusions Following multi-step directions Grasping abstract concepts Grammatical and/or syntax errors when speaking or writing Pragmatic language (taking turns, topic maintenance, sustaining eye contact) Comprehending and using grade-level vocabulary Interpreting social cues Comments and/or Classroom interventions implemented to address above mentioned concerns and responses: ACCOMMODATIONS List specific classroom accommodations that demonstrate differentiated instruction for the student (NOT RTI): READING SCORES DRA Level __________ Class Average _________ Grade Level Expectation _______ PSI Level _______ Class PSI Level _______ Grade Level Expectation _______ DIBELS Benchmark Scores ORF Third 77B 92M 110E
Additional Assessments/Comments (informal assessments and screenings)

Page 5 of 7
Please attach copies of most recent report cards, any raw current state test score data and practice data and any additional narrative statement from teach

Page 6 of 7
INTERVENTIONS Tier I (Classroom Teacher Directed) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
Assessment Date
Targeted Skills Group
Earobics
Leap into Phonics
RAZ Kids
Other
Other
Tier II (AIS and/or Related Service - Direct) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
AssessmentDate
Targeted Skills Group
Language for Learning
Fundations: Double Dose
Earobics
Read Naturally
Edmark
Soar to Success
RAZ-Kids
Other
Other
Tier III (Special Education and/or Related Services - Direct) Intervention Group
Size Freq. Duration
Of SessionPerson Responsible
Start Date
Assessment Date
Targeted Skills Group
Fundations: Double Dose
Earobics
Read Naturally
Edmark
RAZ-Kids
Other

Page 7 of 7

IST Recess Report Name: ________________________________ Date: ________________________ Homeroom Teacher’s Name: _______________________________________________ Social Interaction: Active/Inactive (Circle One - explain if necessary) Type of Play: Comments:


IST Recess Report Name: ________________________________ Date: ________________________ Homeroom Teacher’s Name: ________________________________________________ Social Interaction: Active/Inactive (Circle One - explain if necessary) Type of Play: Comments:

IST PROCESS IST is a problem solving forum that allows us to look at the whole child from different points of view. The complexity of learning sometimes leaves us at a loss as to how to help a child be successful. This is not uncommon. Fortunately, we have an outstanding faculty with many years of experience and areas of expertise. If in doubt about going to IST, please speak with Robin or John. HOW TO GET A IST STARTED: Academic or Behavioral: Complete your grade-level IST paperwork on-line and email to Roseann and Terry. Roseann will send an email to all those who will be involved. ISTs take place on Thursday afternoons. You will be assigned a time and coverage will be provided. PRIOR TO THE MEETING:
Contact the parents by phone FIRST and then send home the IST parent letter. They will receive the summary notes from the meeting. Parents should never be caught off-guard about how their child is progressing – especially if they are struggling.
Be prepared and bring to the IST:
1. Student work 2. Comparative student/class samples 3. Student’s attendance record 4. Any anecdotal records regarding your concerns
Regularly attending the IST meetings will be:
Robin Young and/or John Conroy Pam Sieker -Psychologist Ruth Mueller – Social Worker Sue Chamberlain or Sheila Moroney – Speech and Language Therapists Classroom teacher and/or person referring A grade-level special education teacher Any other appropriate invited staff
May attend when appropriate: Donna Schneider or Francis Lang – Math Specialists The reading specialist working with your students Lisa Goeddel – Occupational Therapist Sue Fox – Physical Therapist
All specialists {PE, Music, Art, and Library} provide written feedback for the meeting. Please alert each of the child you are bringing to IST when you bring your class to that special.

BREWSTER CENTRAL SCHOOL DISTRICT John F. Kennedy Elementary Brewster, New York 10509
845-279-2087
Instructional Support Team (IST)
It’s a Good Thing What is an Instructional Support Team? A natural part of life is the occurrence of challenges, this hold true for children and for adults. When our students are challenged academically, socially and/or emotionally, our faculty join together to support a student in any manner within our means. The IST is an informal brainstorming meeting to meet the needs of your child as effectively as possible. Who is there? On behalf of your child, an IST was organized to include a variety of professionals in the building in order to look at the whole child from various views. The team usually consists of:
*Robin Young (J.F.K. Principal) *John Conroy (J.F.K. Assistant Principal) *Pam Sieker (J.F.K. Psychologist) *Ruth Mueller (J.F.K. Social Worker) *Your Child’s Classroom Teacher *Special Education Teacher *Sue Chamberlain or Sheila Moroney (J.F.K. Speech Therapists)
The following members may participate when appropriate:
*Reading Specialist *Math Specialist *Occupational Therapist *Physical Therapist *English as Second Language (ESL) Teacher
When a specialist is not able to attend, but may have valuable information about your child, he/she submits a written report explaining how your child is functioning academically, socially, and emotionally. Is My Child the Only One? Absolutely not! We average well over 100 ISTs per school year. How will I know what happened? Your child’s teacher will share concerns with you before the IST and share information after the IST. You will also receive a copy of summary notes from the meeting. The purpose of the meeting is to problem-solve and support your child’s success as a student and community citizen. If you have any questions or concerns, please contact your child’s teacher or the appropriate member of the team. Sincerely, Robin Young Ed.D.

BREWSTER CENTRAL SCHOOL DISTRICT John F. Kennedy Elementary Brewster, New York 10509
845-279-2087
Instructional Support Team (IST)
It’s a Good Thing What is an Instructional Support Team? A natural part of life is the occurrence of challenges, this hold true for children and for adults. When our students are challenged academically, socially and/or emotionally, our faculty join together to support a student in any manner within our means. The IST is an informal brainstorming meeting to meet the needs of your child as effectively as possible. Who is there? On behalf of your child, an IST was organized to include a variety of professionals in the building in order to look at the whole child from various views. The team usually consists of:
*Robin Young (J.F.K. Principal) *John Conroy (J.F.K. Assistant Principal) *Pam Sieker (J.F.K. Psychologist) *Ruth Mueller (J.F.K. Social Worker) *Your Child’s Classroom Teacher *Special Education Teacher *Sue Chamberlain or Sheila Moroney (J.F.K. Speech Therapists)
The following members may participate when appropriate:
*Reading Specialist *Math Specialist *Occupational Therapist *Physical Therapist *English as Second Language (ESL) Teacher
When a specialist is not able to attend, but may have valuable information about your child, he/she submits a written report explaining how your child is functioning academically, socially, and emotionally. Is My Child the Only One? Absolutely not! We average well over 100 ISTs per school year. How will I know what happened? Your child’s teacher will share concerns with you before the IST and share information after the IST. You will also receive a copy of summary notes from the meeting. The purpose of the meeting is to problem-solve and support your child’s success as a student and community citizen. If you have any questions or concerns, please contact your child’s teacher or the appropriate member of the team. Sincerely, Robin Young Ed.D.