brocas aphasia
TRANSCRIPT
-introduction to aphasia-etiology
-treatment strategies and techniques
Aphasia is an impairment of language. An acquired communication disorder that impairs a person’s ability to process language, but does not affect intelligence.
Impairs ability to speak and understand others and most people with aphasia experience difficulty reading and writing.

Different areas of the brain are specialized for different functions. It is possible to divide the brain up into different modules which can cooperate in performing the functions of perception, movement, thought, and speech. One important brain module is the language module.We shall see that there our linguistic abilities really require several modules that cooperate.

Dominant hemisphere
• Language lateralize to the dominant hemisphere:
o80% of people are right handed.
o 96-99% of right handed people in the left hemi sphere.
o 60% of left handed people also lateralize to the left
o 25% of left handed shows right dominancy.
o the remaining are mixed dominancy.

Expressive aphasia was first identified by the French neurologist Paul Broca. By examining the brains of deceased individuals who acquired expressive aphasia in life, he concluded that language ability was localized in the ventroposterior region of the frontal lobe

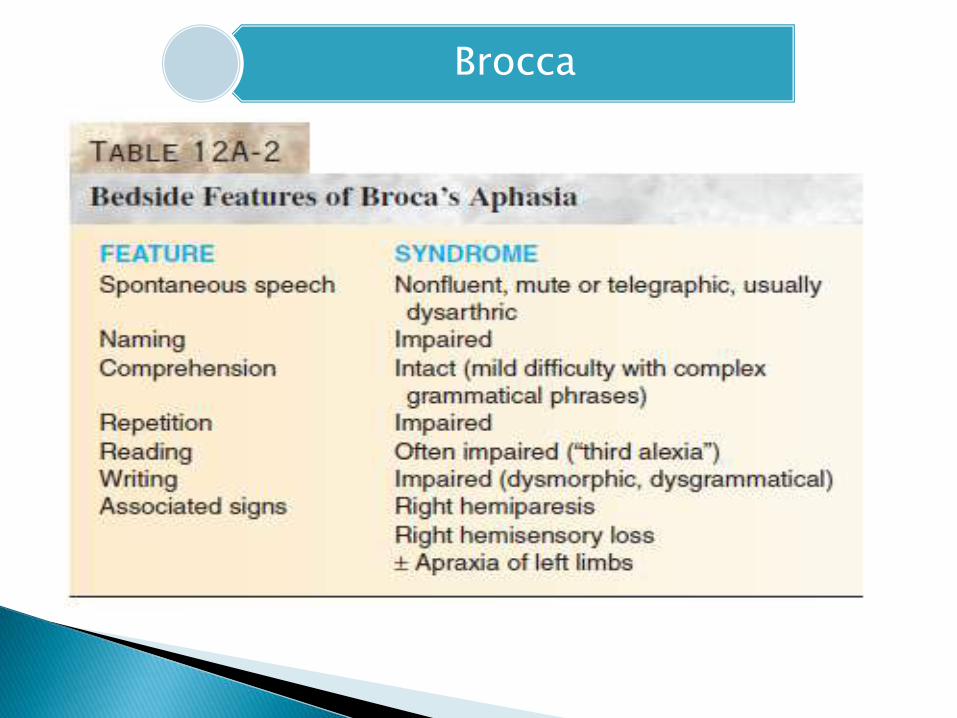
Broca’s aphasia is a non-fluent type of aphasia that is commonly associated with verbal apraxia, relatively good auditory comprehension, agrammatic speech, and poor repetition
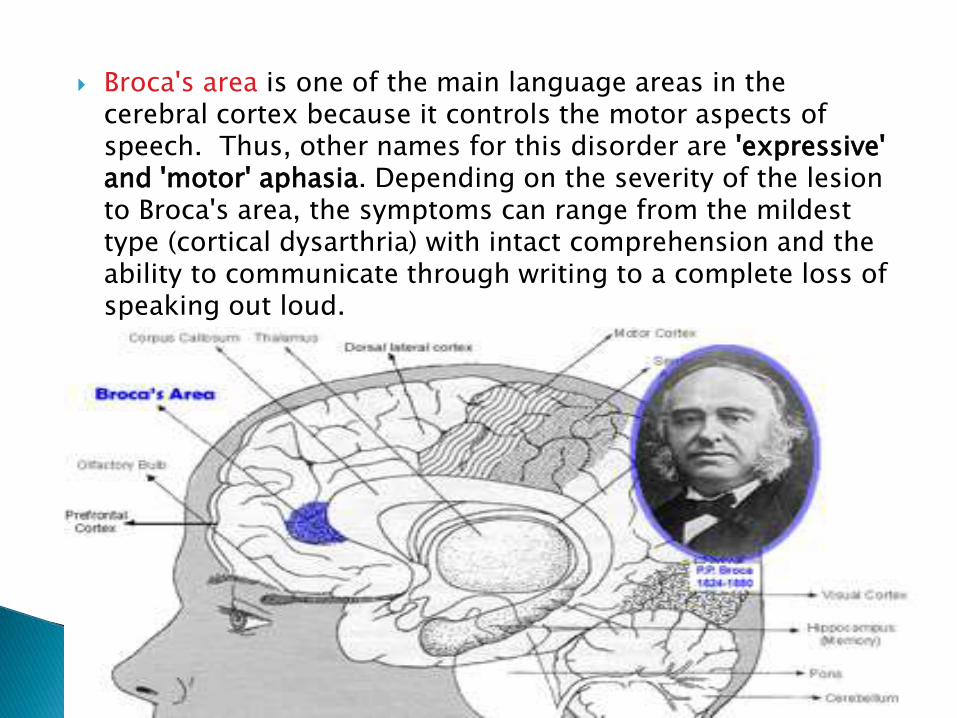
Broca's area is one of the main language areas in the cerebral cortex because it controls the motor aspects of speech. Thus, other names for this disorder are 'expressive' and 'motor' aphasia. Depending on the severity of the lesion to Broca's area, the symptoms can range from the mildest type (cortical dysarthria) with intact comprehension and the ability to communicate through writing to a complete loss of speaking out loud.

Expressive aphasia, known as Broca's aphasia in clinical neuropsychology and agrammatic aphasia in cognitive neuropsychology

– Traditional Broca Area” Brodmann’s 44&45”
– left frontoparietal lesions
– territory of the upper division of the left middle cerebral artery
• Damage to Broca’s area alone is not enough to produce
Broca’s aphasia
• Usually involves Broca’s area + surrounding areas
including M1 & insula.

Distinct brain areas identified in terms of anatomical structure
•So e.g. Broca’s area issometimes definedas consisting of 44,45;much of the literatureuses these numbers because of their precisedefinitions.
Expressive aphasia differs from dysarthria, which is characterized by a patient's inability to properly move the muscles of the tongue and mouth to produce speech. Expressive aphasia contrasts with receptive aphasia, which is characterized by a patient's inability to comprehend language or speak with appropriately meaningful words.

– Effortless
– excessively fluent (logorrhea).
– Paragrammatism:• speaker of a foreign language would notice nothing
a miss, but a listener who shares the patient’s language detects speech empty of meaning, containing verbal paraphasias, neologisms, and jargon productions.
Individuals with Broca's aphasia frequently speak short, meaningful phrases that are produced with great effort. For them, speech is difficult to initiate, non-fluent, labored, and halting. Affected people often omit small words such as "is", "and", and "the"
Brocca

". For example, a person with Broca's aphasia may say, "Walk dog" which could mean "I will take the dog for a walk",

Individuals with Broca's aphasia are able to understand the speech of others to varying degrees. Because of this, they are often aware of their difficulties and can become easily frustrated by their speaking problems.
It is associated with right hemiparesis, meaning that there can be paralysis of the patient's right face and arm.
Similarly, writing is difficult as well. Intonation and stress patterns are deficient.
Naming is deficient, often with bizarre, paraphasicsubstitutions for the correct name
patients show greater deficit in one modality than in the other.
Pathogenesis and etiology of aphasia

• Vascular lesions:– Ischemic strokes, the most common cause of
aphasia.
– The clinical features of the aphasia are of crucial importance to the vascular diagnosis.
– hemorrhagic strokes an important cause of aphasia, most commonly the basal ganglionichemorrhages associated with hypertension.
– AVM, drugs, may cause hemorrhages
– amyloid angiopathy.
– cerebral vasculitis.
• Traumatic brain injury– depressed skull fractures
– hematomas of the intracerebral, subdural, and epidural spaces
– Gunshot wounds produce focal aphasic syndromes
• Tumors of the left hemisphere– The onset of the aphasia is gradual, and edema and
mass effect may result in other cognitive deficits.
– Enlarging tumor may be difficult to distinguish from a diffuse encephalopathy or early dementia.

• Infections of the nervous system– Brain abscesses can mimic tumors and
present with aphasia
– Chronic infections, such as tuberculosis or syphilis, can result in focal abnormalities.
– Herpes simplex encephalitis has a predilection for the temporal lobe and
orbital frontal cortex, and aphasia can be an early manifestation, along with headache, confusion, fever, and seizures.• Aphasia often is a permanent sequel in
survivors of herpes encephalitis.
– AIDS: either the AIDS dementia complex or the opportunistic infections.

• degenerative central nervous system diseases– Alzheimer’s disease may be
more common in familial cases and may predict poor prognosis.
– dialysis dementia syndrome: started with stuttering followed by true aphasia and dementia
• Seizures: – Epileptic aphasia is important
to recognize because anticonvulsant drug therapy can prevent the episodes
• Get the person's attention before you start speaking.
• Maintain eye contact and watch the person’s body language and use of gesture.
• Minimize or eliminate background noise (TV, radio, other people).
• Simplify your sentence structure and emphasize key words.
• Reduce your rate of speech.

• Keep your voice at a normal level. Do not speak loudly unless the person asks you to do so.
• Keep communication simple, but adult. Don't "talk down" to the person with aphasia.
• Give the individual time to speak. Resist the urge to finish sentences or offer words.
• Communicate with drawings, gestures, writing, and facial expressions in addition to speech.
• Encourage the person to use drawings, gestures, and writing.
•Use "yes" and "no" questions rather than open-ended questions.•Praise all attempts to speak and downplay any errors. Avoid insisting that that each word be produced perfectly.•Engage in normal activities whenever possible.•Encourage independence and avoid being overprotective.

Impairment based therapies:A person with aphasia initially wants to speak better and make sense
of language spoken by others. Therefore, speech-language pathologists attempt to repair what is broken. Therapies focus an individual's attention on tasks that allow him or her to comprehend and speak as successfully as possible. A therapy session may be the only time of the day in which the mental mechanics of language are exercised with minimal frustration.These include all _RESTORATIVE APPROACHES

Communication based therapies:
Communication oriented treatments, in part, assist the person in
conveying messages and feelings with alternative means of communicating .In addition, an individual is encouraged to use any remaining language ability that succeeds in conveying messages. Therefore, communication-based activities continue to be partly "language-based" and are likely to incorporate impairment-based objectives simultaneously.These accompanies _COMENSATORY STRATEGIES

Constraint-Induced Movement Therapy
Constraint induced language therapy
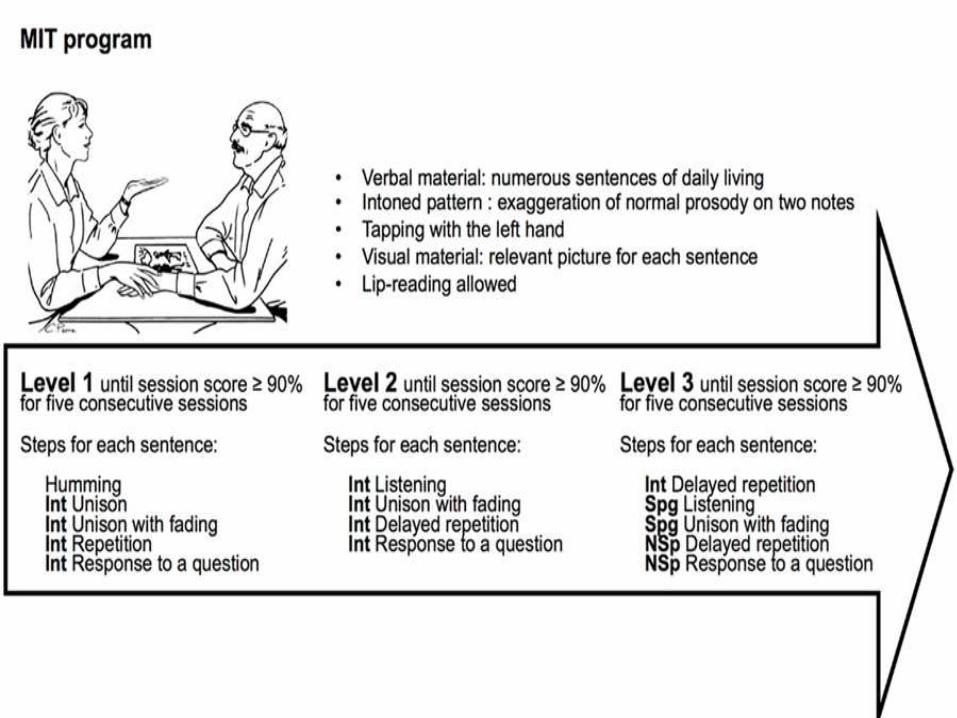
Melodic Intonation Therapy (MIT)
Tele-rehabilitation

This therapy is modeled after a physical therapy for paralysis in which a patient is "forced," for example, to use an impaired side of the body, because the good side has been restricted or constrained.
In applying this principle to communication functions, a person with aphasia may be constrained in using intact gesture in order to direct the individual to use impaired spoken language.

TIME
A second, and perhaps more well-known, component of this treatment is that it is more intensive than typical therapy schedules and it lasts for a relatively short duration. For example, the therapy may be administered for three hours daily for two weeks

◦ Best candidates are patients whose Auditory Comprehension is better than their verbal expression and verbal expression is severely impaired
◦ Strategies:
Intonation pattern uses a range of 3-4 notes
Elements include an exaggerated melody line composed of at least 2 syllables. The rhythm and point of stress help to convey meaning
MIT is slower, similar to Chant Talking
Program Progresses to Longer syntactic units and to Clinician Question, Client Answer using progressively faster melodic patterns.


Established procedures are provided over the Internet with web cameras so that the therapist and person with aphasia can see and hear each other.
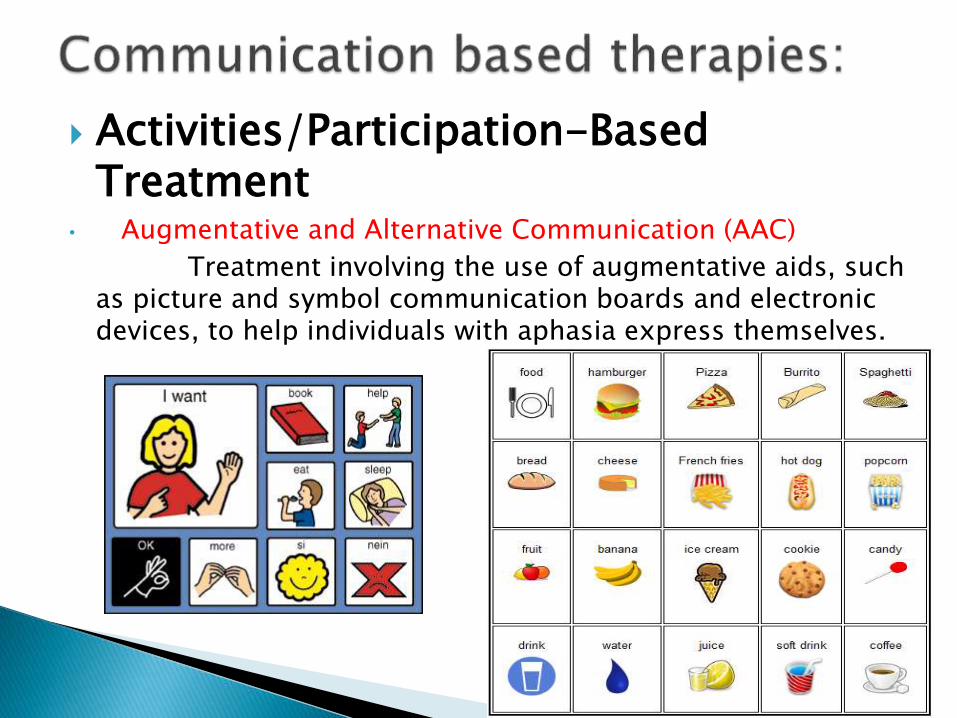
Activities/Participation-Based Treatment
• Augmentative and Alternative Communication (AAC)
Treatment involving the use of augmentative aids, such as picture and symbol communication boards and electronic devices, to help individuals with aphasia express themselves.


• Promoting Aphasics' Communication Effectiveness (PACE)
A conversational treatment in which any modality can be used to communicate ideas from one partner to the other. The client and clinician take equal turns in the sender and receiver roles, and this promotes conversational participation.
The clinician and patient exchange newinformation.
Instead of having a picture of an object or event(called the message) in simultaneous view of theclinician and patient, a stack of message stimuli isplaced face down to keep messages from the view ofa message receiver. A client selects a card andattempts to convey the message on the card. TheBrussels modification is to place a screen about eightinches high between the patient and clinician, and themessage receiver chooses the message from options.
Principle Details
The clinician and patient participate equally assenders and receivers of messages.
This principle puts the turn-taking feature ofconversation into the interaction. The clinician andclient simply alternate in drawing a card and sendingmessages.
The patient has a free choice as to thecommunicative modes used to convey amessage.
Contrary to training one modality such as gesture ordrawing, the patient is left to choose the mode that isused for any message. We do not tell a client toperform in a particular way.
The clinician’s feedback as a receiver is basedon the patient’s success in conveying themessage.
The new information condition should make thisinevitable for both participants. Our feedback shouldlet the client know if he or she got the idea across. Ifwe already know the message, we should respond asif we did not know.
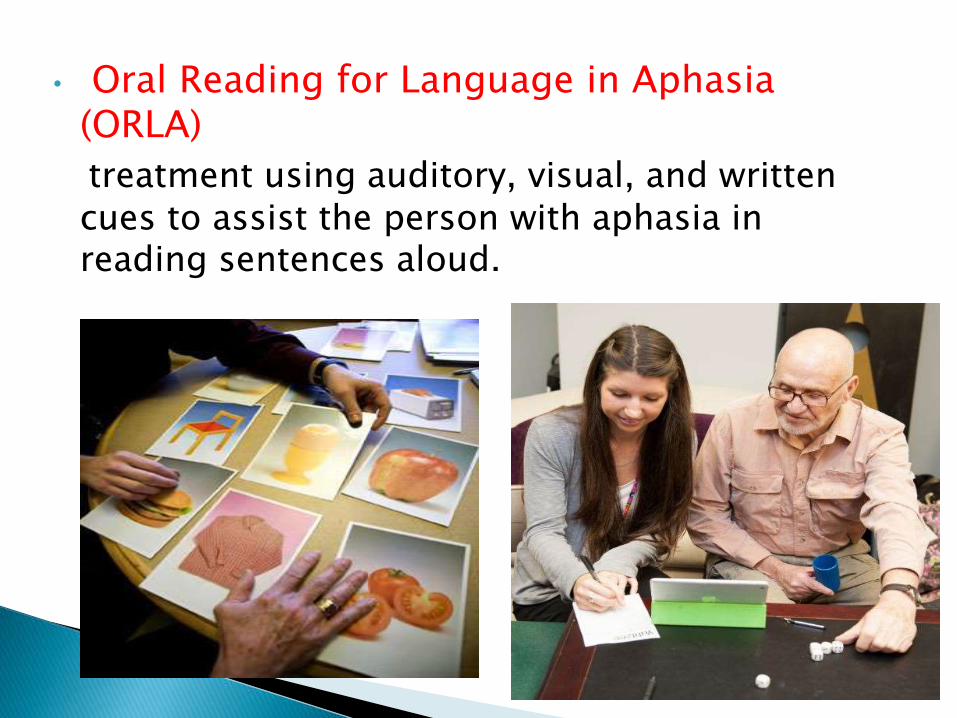
• Oral Reading for Language in Aphasia (ORLA)
treatment using auditory, visual, and written cues to assist the person with aphasia in reading sentences aloud.

• Constraint induced language therapyIn CILT, a small group of patients with aphasia take part in language activities in which they are constrained to verbal responses that are shaped toward more expansive utterances over time. In contrast to other aphasia treatment approaches that promote the use of compensatory communication modalities such as gesture, drawing, or writing, in CILT no compensatory nonverbal communication strategies are allowed during the language activities. Improved verbal responses are the goal of treatment. Furthermore, treatment is provided on an intensive schedule, up to three hours per day for five days per week.

Partner Approaches
• Conversational Coaching
This strategy aims at increasing communicative
confidence through the practice of scripted conversations.
Procedures:1. Effective strategies for each partner (with and without
aphasia) are collaboratively identified. These could be verbal or nonverbal communication strategies.
2. The couple selects the strategies that they are most comfortable with and which ones they will work on using.

3.A communication situation is created, such as viewing a short video clip. One partner views the video and has the job of communicating the information to the other partner.Bothpartners should be using their identified communication strategies to achieve a collaborative result. Partners take turns exchanging information in each conversational role (sender and receiver).
4. The clinician acts as a coach to each of the two partners as they exchange and build information together.
• Supported Communication Intervention (SCI)Supported communication intervention (SCI) is an approach to
aphasia rehabilitation that emphasizes the need for multimodality communication, partner training, and opportunities for social interaction
LIFE PARTICIPATION APPROACH TO APHASIA (LPAA)
Call for a broadening and refocusing of clinical practice and research on the consequences of aphasia
Focus on re-engagement in life
Places life concerns of those affected by aphasia at the center of all decision making
Empowerment and collaboration on interventions may lead to more rapid return to active life and reduce the consequences that lead to long-term health costs

Assessment includes determining relevant life participation needs
In addition to assessing communication and deficits, clinicians should be equally interested in how the patient does with support
Clinicians take on take on roles in addition to doing therapy, such as “communication partner”, “coach” or “problem solver”
Clinicians evaluate and document on:
Life activities and satisfaction
Social connections and satisfaction
Emotional well-being

Word Finding Treatment
• Response Elaboration Training (RET)
A type of “loose training” which works to improve
lexical retrieval and the number of content words produced by an individual with aphasia (Conley & Coelho, 2003).Forward chaining, or elaboration, of the client’s utterances is used.
•

RET Steps Clinician’s stimulus
Patient’s response
Clinicianfeedback
1) Elicit initial verbalresponse to picture
Line drawing of simpleevent (man with abroom) “Tell me what’shappening in thispicture.”
“Man…sweeping”
2) Reinforce, model,and shape initialresponse
Great. The manis sweeping
3) Wh- cue to elicitelaboration ofinitial response
Why is he sweeping?”
“Wife…mad!”
4) Reinforce, model,and shape the twopatient responsescombined
“Way to go! Theman is sweepingthe floor becausehis wife is mad.”
5) Second model andrequest repetition
“Try and say the wholething after me. Say ‘Theman is sweeping thefloor because his wife ismad.’”
“Man…sweeping…wife…mad.”
Good job!”
6) After reinforcementelicit delayedinitiation of thecombinedresponse.
“Now, try to say it onemore time.”
“The man…sweeping becausehis wife…mad.”
• Opposites ExerciseThis exercise helps with repairing word-finding abilities and articulation, as well as expanding limited concepts. For this exercise, write down ten words, such as "up," "mad" and "bright." Then, ask for the opposite of the word. For instance, you would ask, "What is the opposite of up?" You would then reply with "down." This exercise can increase in difficulty, with concepts increasing in complexity as the sufferer's tolerance strengthens. For instance, try "frustration" and "joy."


• Preposition Exercise
This exercise uses two spoons and a box, and helps firm the concept of prepositions. To start, place the box on a surface and place both spoons anywhere relative to the box, such as on the box and beside it. These spoons would not be in the same location. Then ask, "Which spoon is on the box?" He would then reply by picking up or pointing at the spoon. You can increase the difficulty by using multiple spoons.



• Semantic Feature Analysis TreatmentSFA is used to improve word-retrieval abilities in clients with
aphasia. This is done via spoken production of a target, most usually prompted through a picture stimulus, alongside structured elicitation of a series of semantic features that are associated with the target. This combination of elicitation of a target and semantic features is hypothesised to strengthen (or reactivate) the semantic network around the target and thereby facilitating improved word retrieval on subsequent attempts. As the client is also encouraged to verbally produce the target, phonological representations of the target are also accessed and may therefore also improve the activation pathways between semantic and phonological representations.

SFA is generally carried out with the aid of a ‘worksheet’ that may be presented on paper or via computer screen. The worksheet generally presents single-word or sentence prompts to elicit the semantic features (e.g. Location/Where would you find it?). When the client provides an appropriate response, these are generally written in the relevant space by the clinician.
Present target picture and ask client to name the picture (i.e. apple) Regardless of whether client correctly names the target picture, ask the
client to provide a verbal response for each of the semantic features (e.g. fruit, grows on a tree, round, eat it, respectively)
Once client provides a response for all semantic features, prompt client to again name the picture
Review the completed worksheet ◦ Clinician may provide review by integrating all information within a description (e.g.
an apple is a fruit that grows on trees. It is round and you eat it)◦ Client may be encouraged to again verbally produce the target and semantic features
from the responses that have been written on the worksheet.

THANKYOU