bsi prevention update 10-11 - nc quality center · – inser=on’bundle,’maintenance’bundle...
TRANSCRIPT

1
Preven&on of Catheter-‐Related Bloodstream Infec&ons
October 2011
Robert J. Sherertz, MD Hospital Epidemiologist
Professor of Infec@ous Diseases
10/12/11
CLABSI Background
• Historically, when hyperalimenta=on first appeared, BSI rates of 50-‐100% were reported. Then specialist teams consis=ng of a single surgeon and a single nurse were created and BSI rates dropped to less than 1%.
• Message: excellent asep=c technique by specialists can prevent BSI.
• Corollary: Can generalists do as well? Recent studies strongly indicate the answer is yes.
10/12/11

2
Preven@ng CLABSI • Educa=on • Inser=on Bundle • NC BSI Preven=on Collabora=ve: Phase I
– Inser=on Bundle • NC BSI Preven=on Collabora=ve: Phase II
– Inser=on Bundle, Maintenance Bundle • Other issues
– Novel technologies – Blood draws through lines – Subs=tute nurses – Surveillance
• Summary
10/12/11
Educa=on • Simula=on Training (Educa=on)
– Beginning in 1996, our hospital was the first to show that simula=on training for CVC inser=on can decrease the risk of CLABSI.3 Subsequently many other quasi-‐experimental design before-‐aYer studies have confirmed this finding.1,2
– We are now moving beyond mannequins to using fresh cadavers to facilitate:
• Anatomic landmark training • Ultrasound instruc=on • Sterile technique instruc=on
1: Khouli H, Chest. 2010 Aug 12. 2: Barsuk JH, Arch Intern Med. 2009 Aug 10;169(15):1420-‐3. 3: Sherertz, Ann Intern Med. 2000 Apr 18;132(8):641-‐8.
10/12/11

3
Educa=on: Simula=on Training
10/12/11
Inser=on Bundle • Recent reports from the Ins=tute for Healthcare Improvement (IHI) and the
Keystone Project have shown that “Bundled” healthcare interven=ons in combina=on with a change in culture (CUSP) can lead to drama=c reduc=ons in CLABSI. – hap://www.ihi.org/ihi
– Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, Sexton B, Hyzy R, Welsh R, Roth G, Bander J, Kepros J, Goeschel C. An interven=on to decrease catheter-‐related bloodstream infec=ons in the ICU. N Engl J Med. 2006 Dec 28;355(26):2725-‐32
– Michigan Bundle: HH,Checklist, MSB, CHG skin prepara=on, avoiding femoral catheters, removing unnecessary catheters (maintenance).
– Recent review of Bundles: Zingg, Current Opin Infect Dis 2011;24: 377.
10/12/11

4
Inser=on Bundle • North Carolina became the second state aXer Michigan to use the Johns Hopkins CUSP (Comprehensive Unit Based Safety Program) approach for reducing BSI.
• The program was funded by AHRQ and overseen in North Carolina by the NC Center for Hospital Quality and Pa@ent Safety (NCCHQPS), Cary NC in partnership with JHU, the Keystone Center for Pa@ent Safety and Quality of the Michigan Health & Hospital Associa@on, and the American Hospital Associa@on’s Health Research and Educa@on Trust.
10/12/11
Inser=on Bundle 1. Hand Hygiene 2. CHG skin prep
3. MSB 4. Subclavian
preferred over femoral or jugular
5. CVC Checklist Subclavian
10/12/11
5
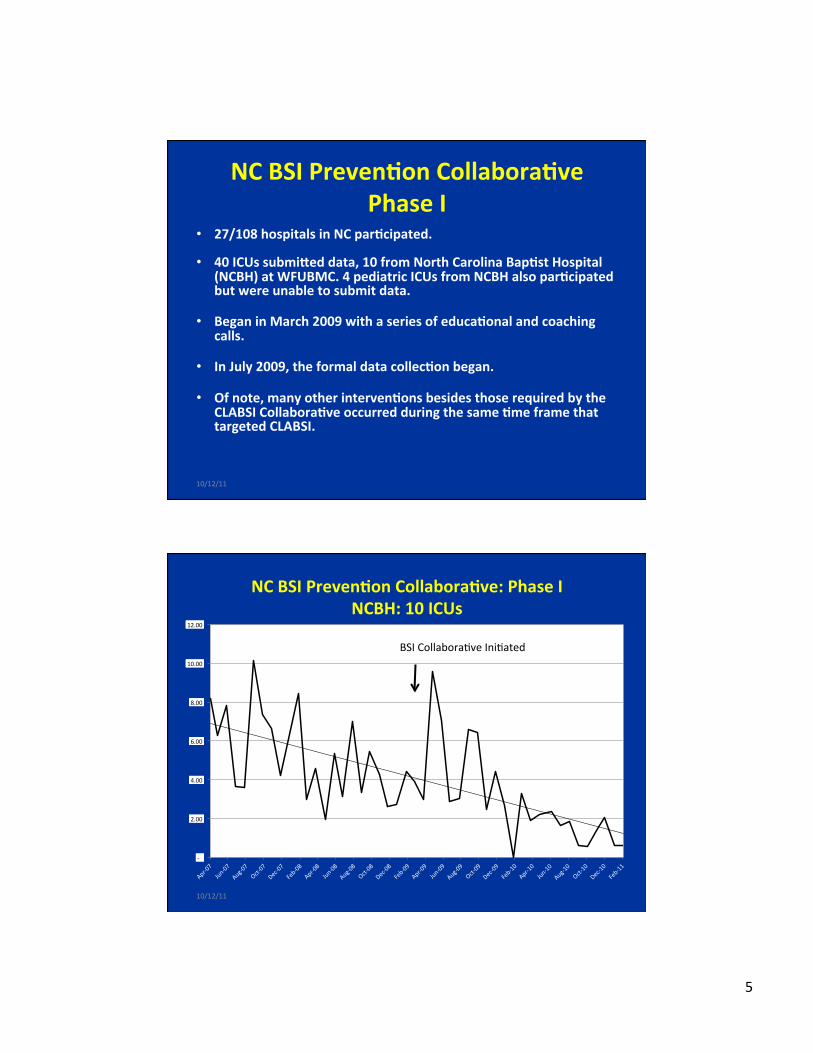
NC BSI Preven=on Collabora=ve Phase I
• 27/108 hospitals in NC par=cipated.
• 40 ICUs submiaed data, 10 from North Carolina Bap=st Hospital (NCBH) at WFUBMC. 4 pediatric ICUs from NCBH also par=cipated but were unable to submit data.
• Began in March 2009 with a series of educa=onal and coaching calls.
• In July 2009, the formal data collec=on began.
• Of note, many other interven=ons besides those required by the CLABSI Collabora=ve occurred during the same =me frame that targeted CLABSI.
10/12/11
-‐
2.00
4.00
6.00
8.00
10.00
12.00
NC BSI Preven=on Collabora=ve: Phase I NCBH: 10 ICUs
Eliminate CLABSI Collabora@ve BSI Collabora@ve Ini@ated
10/12/11

6
Lesson 1: Semng Goals Approved by CMO, CEO, Board
F i s c a l Year
B a s e l i n e CLABSI Rate
Year End Goal Rate Achieved
FY2008 7.5 6.8 5.5
FY2009 5.5 4.9 4.7
FY2010 4.7 3.7 3.3
FY2011 3.3 1.6 (25th NHSN) 0.9 (2/11)
10/12/11
Lesson 2: Rapid Cycle Improvements
CLABSI Interven=ons before March 2009: 10 in 144 months
• 7/95 – BSI educa=on to resident MDs • 1/98 – CHG/Ag-‐SD CVC implemented • 1/02 – CHG as CVC skin prep started • 2004 – Monthly feedback of BSI rates • 04-‐06 – CVC hub connector evalua=ons • 8/05 – CVC checklist (paper) • 1/06 – CHG patch implemented • 2/08 – Ins=tu=onal CLABSI goals established • 6/08 – 6/09, trial of minocycline/rifampin coated CVC, changed back
to CHG/Ag-‐SD • 9/08 – began par=cipa=on in NC SHIM BSI Reduc=on Collabora=ve
10/12/11

7
Rapid Cycle BSI Improvements CLABSI Interven=ons aYer March 2009: 17 in 44 months
• 3/09 – Began par=cipa=on in AHRQ BSI Reduc=on Collabora=ve, monthly mee=ngs • 5/09 – Implemented electronic CVC checklist • 6/09 – Recommended peripheral BC over CVC BC, decreased CVC wire change for Dx • 8/09 – Mandatory daily queries about CVC line necessity, daily goals sheet • 10/09 – Standardized ICU CVC inser=on carts, standard inventory list • 11/09 – Yearly BSI mandatory educa=on implemented • 12/09 – Changed hub connectors secondary to poor performance • 2/10 – CHG daily bathing for all ICU pa=ents • 5/10 – Real =me repor=ng of BSI to ICU leadership, weekly ICU leadership mee=ngs • 7/10 – PICC catheter inser=on improvement process ini=ated • 8/10 – BSI Reduc=on Collabora=ve extended to ED, OR, radiology, hospital floors • 9/10-‐12/10 – Trial of clear CHG dressings • 10/10 – Twice weekly rounding on HemOnc pa=ents CVC sites, CVC maintenance kit • 12/10 – Electronic CVC checklist compliance available
10/144 months vs 17/44 months, P<0.0001 10/12/11
Lesson 3: Gain buy in by collabora=ng on format of data presenta=on. Format 1 (thru 2/11)
Unit FY11 Goal FY12 Goal 6 Mon Avg BSI in 6 m. Days Since Last Inf
MICU (4C,4RT) 2.3 1.1 1.3 4 91
SICU (4A,4B) 1.7 0.7 0.0 0 199
5A 0.8 0.2 0.0 0 367
5B 3.0 1.4 0.0 0 244
5C 1.9 0.0 0.0 0 415
6AIM 0.0 0.0 1.3 2 13
BMT 0.0 0.0 1.5 2 46
BU 3.1 1.2 2.3 1 122
CCU 0.0 0.0 2.0 1 171
All (Adult, no BMT) 1.6 0.6 0.9 8 13
PICU 2.5 1.1 1.4 1 202
NICU By weight By weight 3.1 9 53 10/12/11

8
Format 2
10/12/11
Lesson 4: HemOnc and NICU pa=ents require a different approach.
10/12/11

9
Jan Feb Mar Apr May Jun Jul Aug Sep Oct
2010
0
10
20
Num
ber of Patients with
BSI
BSI by Catheter TypeBroviac
Hickman
Internal Jug
PermCath
PICC
Portacath
SG
TLC
Umbilical
Vascath
Other
BSI by Catheter Type.tc10/12/11
3.125
2.325
3.18
0.787
0 0 0
0.478
1.49
0 0 0
1.04
1.42
0 0
0.5
1
1.5
2
2.5
3
3.5
DH CB JS LS G
PICC
Infec=on
s/Inser=on
s x 100
CVCs inserted by Radiology; Early CLABSI (<14 days): Examined PICC Infec=on Rate by Inserter: June -‐Nov 2010
Jun-‐Jul Aug-‐Sep Oct-‐Nov 10/12/11

10
For Late CLABSI (>14 days): BMT Twice Weekly Rounds
• For late CLABSI the BMTU Nurse Manager, Infec=on Preven=onist, and Hospital Epidemiologist began twice weekly rounds on all BMT unit pa=ents looking for: – central line dressings being clean, dry, and intact – bloody dressings changed within <24 hours – date of dressing change noted – dressings changed within 7 days for transparent dressing or 2 days for gauze
dressing – Biopatch being used and applied correctly – IV tubing changed in 96 hrs – Any IV tubing not infusing properly – Capped with sterile end cap.
• Deficiencies pointed out and corrected real =me
• BSI rate: 3.5/1000 dd (36 months) decreased to 1.8/1000 dd (5 months aYer interven=on); P<0.001. Presented at 2011 Na=onal APIC
10/12/11
Lesson 5: It is possible to be very aggressive about reducing line days! Unit 1st 12 months 2nd 12 months P value
MICU 252 ± 20 days 162 ± 19 days P < 0.001
SICU A 187 ± 51 days 111 ± 25 days P < 0.001
SICU B 141 ± 39 days 104 ± 15 days P = 0.009
Trauma 95 ± 31 days 42 ± 14 days P < 0.001
BU 108 ± 35 days 73 ± 23 days P = 0.01
CT Surgery 187 ± 31 days 163 ± 30 days P = 0.08
Neurosurgery 96 ± 32 days 114 ± 23 days P = 0.13
Stepdown unit 269 ± 45 days 251 ± 38 days P = 0.29
No change in BMT or NICU line days 10/12/11

11
Lesson 6: Cost Savings Es=mates are well received by Administra=on
Low: $7,288/BSI, High: $29,156/BSI
Year #CLABSIs # CLABSIs Prevented1
Es=mated CLABSI Savings (x million)
2007 180 -‐-‐ -‐-‐
2008 131 49 $0.36-‐$1.43
2009 82 98 $0.71-‐$2.85
2010 33 147 $1.07-‐$4.28
10/12/11
Lesson 7: Intense pressures by clinicians to not call BSIs
• Examples of reasons offered to exclude – Pa=ent was afebrile – We didn’t put in their CVC – They have a pneumonia – Etc, etc
• The IPs or hospital epidemiologist calling the system has the ability to game the system.
10/12/11

12
Summary of Lessons Learned from Phase 1
• High level approval of goals is very important – Once this happens, change occurs quickly.
• Rapid cycle improvements can be very effec=ve. • Agreeing on graph formats helps with buy-‐in.
– Comparisons to other units is quite powerful. • HemOnc and NICU catheters require a different approach:
look at inserters and maintainers separately • Reduce line days!!! • Cost effec=veness data sells the program administra=vely. • If CMS doesn’t figure out a valida=on methodology; BSIs
can be reduced by gaming the system.
10/12/11
NC BSI Preven=on Collabora=ve Phase II
• August 2011 – June 2013
• Free for hospital units with CLABSI rates > 1.5/1000dd, $1500/par=cipa=ng unit if rate is < 1.5/1000dd
• CLABSI Inser=on Bundle – emphasized in phase 1 and phase 2
• CLABSI Maintenance Bundle – to be emphasized in phase 2 – Monthly CUSP mee=ngs
10/12/11

13
Maintenance Bundle
• Zingg, Crit Care Med 2009; 37:2167 – Quasi-‐experimental design, before-‐aYer – HH, op=mized catheter dressing, nontouch technique for CVC manipula=on, prepara=on of infusates, op=mized catheter care
– Provides details of teaching modules – 75% reduc=on in CLABSI (P<0.001)
• Guerin, Am J Infect Control 2010; 38:430 – Quasi-‐experimental design, before-‐aYer – Wearing mask and sterile gloves, scrubbing with 2% CHG, applying a CHG sponge
– 80% reduc=on in CLABSI (P=0.004)
10/12/11
Preven=ng CLABSI
• Other issues – Novel technologies
• An=infec=ve Coa=ngs • CHG dressings, hub disinfec=on, bathing • Catheter lock solu=ons
– Blood draws through lines – Subs=tute nurses – Surveillance
10/12/11

14
Novel Technologies • An=-‐infec=ve Coa=ngs
10/12/11
Novel Technologies • An=-‐infec=ve coa=ngs
Maki, AIM 1997;127:257 CR-‐BSI N % /1000 DD
AgSD/CHG (1st G) 208 1.0 1.61 Uncoated 195 4.6
7.64 Raad, AIM 1997;127:267 CR-‐BSI
N % /1000 DD M/R 130 0.0 0.00 Uncoated 136 3.7
6.13 Darouiche, NEJM 1999;340:1 CR-‐BSI
N % /1000 DD M/R 356 0.3 0.33 AgSD/Ch (1st G) 382 3.4 4.15
10/12/11

15
Catheter Zones of Inhibi=on aYer Implanta=on
Marik, Crit Care Med 1999;27:1128 10/12/11
Novel Technologies
• An=-‐infec=ve coa=ngs
Rupp, … , Sherertz, AIM 2005;143:570 CR-‐BSI N % /1000 DD
AgSD/CHG (2nd G) 384 0.3 0.42 Uncoated 393 0.8 1.24
CRI (Quant CC) N % /1000 DD
AgSD/CHG (2nd G) 208 9.3 13.3 Uncoated 195 16.3 24.1
10/12/11

16
Ag/CHG (2nd) M/R Ag/CHG (2nd)
10/12/11
Novel Technologies • CHG Dressings
Timsit, JAMA 2009;301:1231 Karpanen, J An=microb Chemo 2011 RCT, decreased risk of BSI 66:1777. Persistent ac=vity for 7d
Advantage: circumferen=al contact Disadvantage: polarity, lack of visibility
Advantage: visibility, no polarity Disadvantage: lack of circumferen=al contact
10/12/11

17
Novel Technologies
• CHG hub disinfec=on – Onder A, Ped Nephrol, 2009;24:1741. – Prospec=ve before-‐aYer quasi-‐experimental design
– Ini=al hub prepping with PI, then CHG prep – All catheter sites have CHG patch – BSI rates decreased from 2.2 to 1.0/1000 dd
• P=0.04
10/12/11
Novel Technologies • CHG Bathing
– Popovich, ICHE, 2009;30:959. • CLA-‐BSI decreased from 5.31 to 0.69/1000 dd (P<0.05) aYer ini=a=ng daily CHG baths in a MICU with a commercial CHG cloth (2% impregnated).
– Popovich, Intensive Care Med, 2010;36:854. • CLA-‐BSI did not decrease (3.81/1000 dd to 4.6/1000 dd) in a SICU using the same approach.
– Climo, Crit Care Med; 2009;37:1858. • Acquisi=on of MRSA and VRE decreased 2-‐fold (P<0.05) aYer implemen=ng daily bathing with CHG (4oz in basin of water).
10/12/11

18
Novel Technologies
• Lock Solu=ons: Clinical Trials – Ethanol – Citrate/gentamicin – EDTA/minocyline
10/12/11
70% Ethanol Lock (2h) vs. Placebo: A Prospective Randomized Study
Parameter
70% Ethanol (n=226)
Placebo (n=222)
P
Strictly endoluminal CRBSI 2 7 .10 Presumed endoluminal CRBSI 8 9 .81 Combined primary endpoint 10 16 .23 Primary bacteremia 91 91 .95 Exoluminal CRBSI 11 8 .64 D/C Lock 2° AE 11 1 .06 ↓ Lock Freq 2° AE 10 0 .002
Slobbe, … , Rijnders. PLoS 5(5)e10840:5, 2010 10/12/11

19
Novel Technologies • Lock Solu@ons: citrate/gentamicin
– Labiola, Nephrol Dial Transplant, 2008;23:1666.
Fig. 2. Forest plot: fixed effects. The rela=ve risk of CRB in the eight studies included in our meta-‐analysis. The bold line represents the overall rela=ve risk. The summary risk ra@o is 0.32 (95% CI 0.10–0.42), indica@ng a significant protec@ve effect of an an@microbial lock solu@on in the preven@on of CRB.
10/12/11
Novel Technologies
• Lock Solu@ons: EDTA/minocycline
TABLE 3 EFFECT OF MINOCYCLINE–EDTA VERSUS HEPARIN FLUSH SOLUTIONS ON THE RELATIVE RISK OF CATHETER COLONIZATION AND CATHETER-‐RELATED BLOODSTREAM INFECTION IN PATIENTS RECEIVING SHORT-‐TERM HEMODIALYSIS
Heparin Minocycline–EDTA P Catheter-‐related bacteremia 8.3%
0% .35 Catheter coloniza=on 64.3% 9.1% .005
Bleyer, … , Raad, Sherertz, ICHE, 2005; 26: 520.
10/12/11

20
Blood Draws Through Lines
• Issues related to drawing BC through lines – Sherertz, J Pediatrics 1992;120:455.
– Risk of line infec=on is directly propor=onal to the number of line breaks.
– Many hospitals are minimizing this risk by planning the number of blood draws so that they are kept to the absolute minimum. This is oYen being done at the same =me as the ongoing need for the CVC is reassessed.
10/12/11
Blood Draws Through Lines
• Valved Catheter Hubs
– Jarvis, … , Sherertz, CID, 2009;49:1821. • HA-‐BSI rates increased in 5 hospitals aYer transi=oning from needles or split septums to valved catheter hubs.
– Sherertz, Eur J Clin Microb Infect Dis 2011; epub • Blood drawn through valved catheter hubs has a 10-‐20% frequency of posi=vity (Clave, Q-‐syte < Clearlink).
• This could poten=ally lead to 2-‐fold greater frequency of BC posi=vity, ie false posi=ves.
10/12/11

21
Blood Draws Through Lines • Jones,…, Sherertz, SHEA Mee=ng 2011.
– NICU babies with CVC, paired CBC/PBC – Concordant pairs were more likely to be associated with persistent
posi=ve BC than discordant pairs (57% vs 16%, P<0.001).
• Park, Diagn Microbiol Infect Dis 2011;70:31. – HemOnc pa=ents with 112 CBC+/PBC-‐ pairs – Subsequent BSI with same organism
• Appropriate an=bio=cs: 3/81 (4%) • Inappropriate an=bio=cs: 6/31 (19%)
– Laaer suggests 80% were false posi=ve
• Guembe, CID 2010; 50: 1575. – How many lumens should be cultured to diagnose CRBSI?
• Culturing 2/3 lumens misses 16% of CRBSI • Culturing 1/3 lumens misses 37% of CRBSI
10/12/11
Blood Draws Through Lines
• Changing hub to do blood cultures. – 91 pa=ents, BC drawn by 3 methods
• Through old cap • Through new cap • Peripherally
– Frequency of BC posi=vity • Old cap BC – 39.6% • New cap BC – 19.8% • Peripheral BC -‐ 10%
Mathew A, J Infus Nurs 2009;32:212. 10/12/11

22
Subs=tute Nurses
• Robert, ICHE, 2000; 21: 12-‐17 – The influence of the composi=on of the nursing staff on primary bloodstream infec=on rates in a surgical intensive care unit. The more floaters and contract nurses, the greater the risk of BSI.
• Sherertz, ICHE, 2003; 24:887-‐9. – Vascular catheters inserted in the trenches versus guideline documents: can the discrepancies be resolved? Reviews issues related to nurse staffing.
10/12/11
Surveillance
• Lin, Quality of tradi=onal surveillance for public repor=ng of nosocomial bloodstream infec=on rates. JAMA 2010; 304;2035. – Compared Infec=on Control Preven=onist (ICP) assessed BSI with computer algorithm assessed BSI.
– Median ICP rates 3.3 vs 9.0 for computer algorithm
– Medical center with the lowest rate by ICP had the highest rate by computer algorithm
10/12/11

23
Sterile Technique Issues Evidence1 Novel Technologies (Evidence)
CLABSI Educa@on IIA Mannequins (IIA)
Hands on beker than lecture
Inser@on Bundle: AgS/CHG, M/R (IA)
HH, CHG prep, MSB, avoid femoral IA CHG dressings (IA)
Checklist, CVC inser@on cart IA Valved catheter hubs (IIA)
Maintenance Bundle: CHG daily bathing (IA)
Mask, sterile gloves, rounds IIA CHG hub disinfec@on (IIB)
Minimizing line draws, IIA Lock Solu@ons (IA)
Blood Draws Through Lines
BC Technique (phlebotomist vs RN) IA Changing hubs (IIA)
Peripheral BC only? IIB
CLABSI Surveillance/Feedback IIB Automated soXware (?)
Summary BSI Preven=on Strategies
Mermel, ICHE 2008;29:S22 -‐ BSI Preven=on Guidelines 10/12/11
Conclusions • Basic sterile technique is the most important aspect of preven=ng CLABSI.
• Novel technologies can reduce the risk of CLA-‐BSI and decrease the risk of false posi=ves, but can be overwhelmed if not associated with good sterile technique. It is recommended to use these only if sterile technique is not effec=ve.
• Other variables such as drawing blood through lines, nurse staffing and caliber of personnel performing BSI surveillance can drama=cally affect BSI rates.
10/12/11