burns- derm presentation
TRANSCRIPT
BURN DISEASESONAZI THERESA
SOURCES:U.S. Department of Health & Human ServicesNational Library of Medicine
WORLD HEALTH ORGANIZATIONPubMed Citations
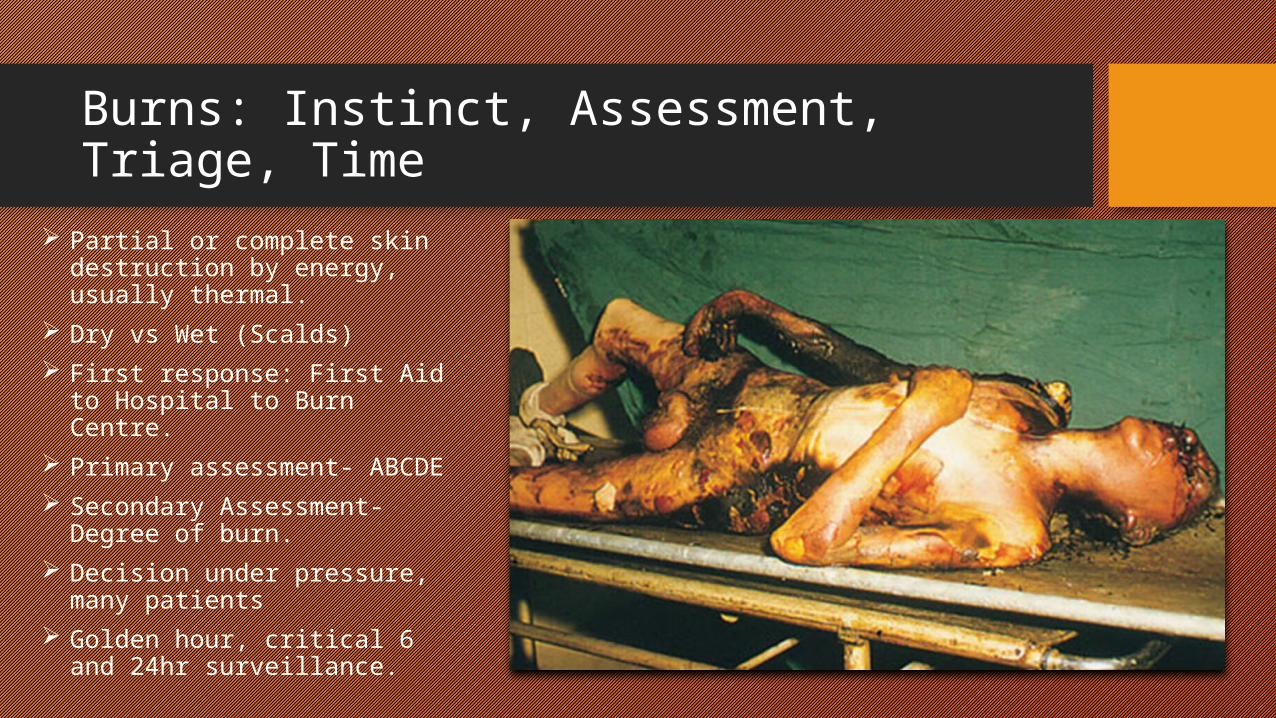
Burns: Instinct, Assessment, Triage, Time Partial or complete skin
destruction by energy, usually thermal.
Dry vs Wet (Scalds) First response: First Aid to
Hospital to Burn Centre. Primary assessment- ABCDE Secondary Assessment-
Degree of burn. Decision under pressure,
many patients Golden hour, critical 6 and
24hr surveillance.
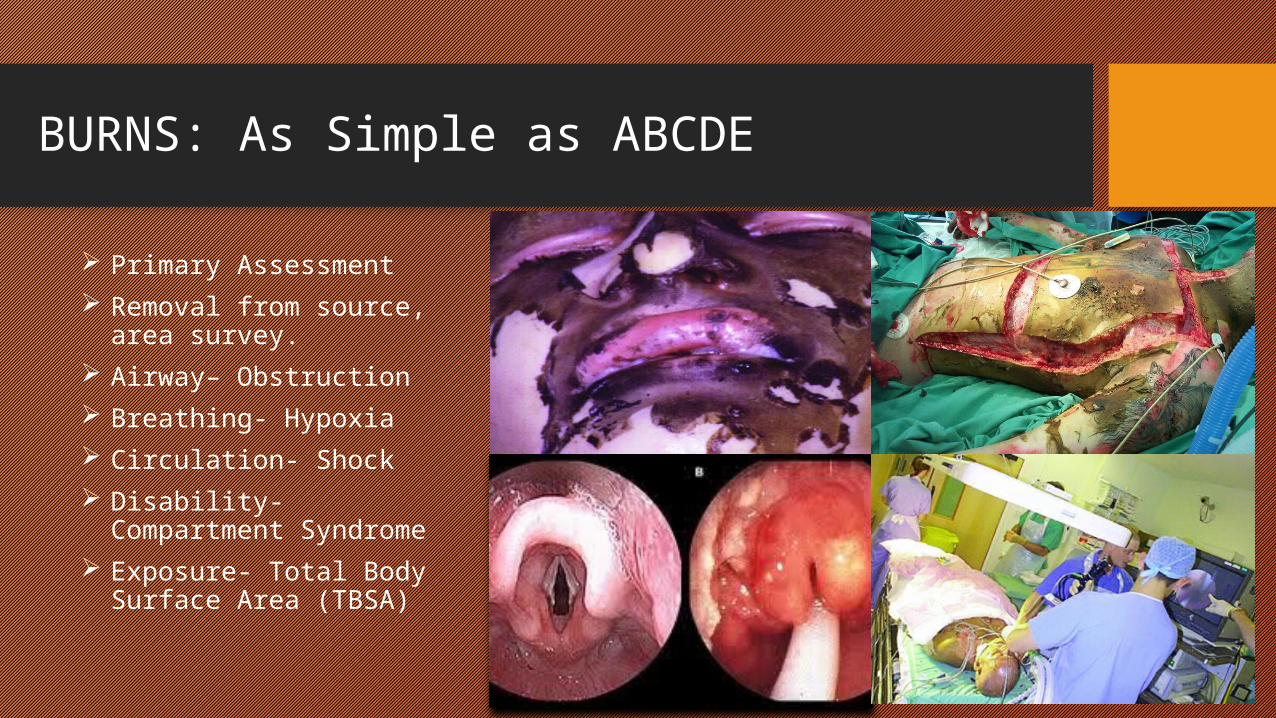
BURNS: As Simple as ABCDE
Primary Assessment Removal from source, area
survey. Airway– Obstruction Breathing- Hypoxia Circulation- Shock Disability- Compartment
Syndrome Exposure- Total Body
Surface Area (TBSA)
BURNS: A-Airway and B-Breathing
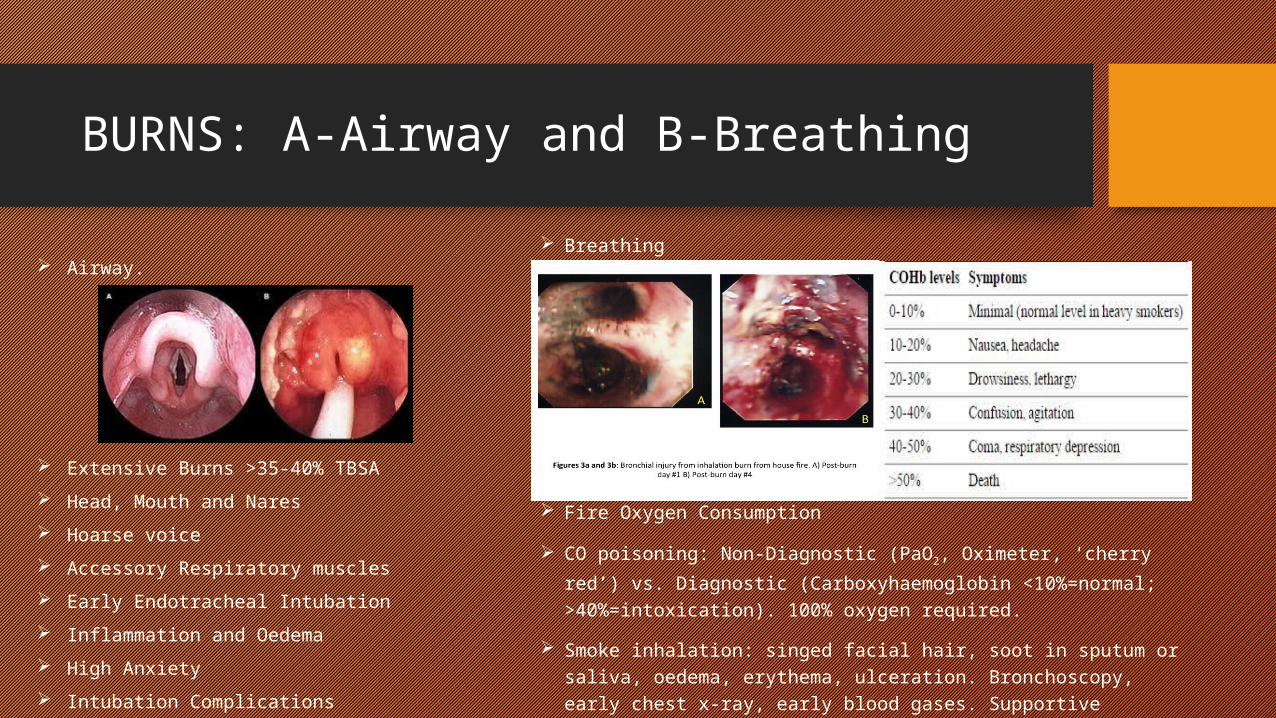
Airway.
Extensive Burns >35-40% TBSA Head, Mouth and Nares Hoarse voice Accessory Respiratory muscles Early Endotracheal Intubation Inflammation and Oedema High Anxiety Intubation Complications
Breathing
Fire Oxygen Consumption
CO poisoning: Non-Diagnostic (PaO2, Oximeter, ‘cherry red’) vs. Diagnostic (Carboxyhaemoglobin <10%=normal; >40%=intoxication). 100% oxygen required.
Smoke inhalation: singed facial hair, soot in sputum or saliva, oedema, erythema, ulceration. Bronchoscopy, early chest x-ray, early blood gases. Supportive pulmonary treatment, aggressive respiratory therapy.
BURNS: C-Circulation and D-Disability Circulation. Massive Capillary Leak Fluid Shift Fluid requirements directly proportional to TBSA,
degree, comorbidity and inhalation. >20% TBSA, IV access with 2 large-bore
cannulas in: Unburned>>Burned>Central access*>Cut-downs**. Blood assessment.
Peripheral circulation. Circumferential burn. Foley Catheter. 24-hr Urine output 0.5ml/kg/hr in
adults and 1ml/kg/hr in children. >20% TBSA. Ringer’s Lactate solution. Isotonic, cheap, easy
storage. Parkland Formula: 4 x weight in kg x %TBSA
burn. Give 1/2 of that volume in the first 8 hours Give other 1/2 in next 16 hours
Disability: Neurological (GCS) and Compartment Syndrome
Severe pain (worse with movement), numbness, cool extremity, tight feeling compartments.
Palpable arterial pulse. pressure >30 mmHg may compromise
muscle/nerves Measured by arterial line monitor (place needle
into compartment) Escharotomy. Fasciotomy. Expertise. Homeostasis. High index of suspicion in completely
circumferential burns. Foley catheter for abdominal pressure.

ESCHAROTOMY IN CIRCUMFERENTIAL BURN
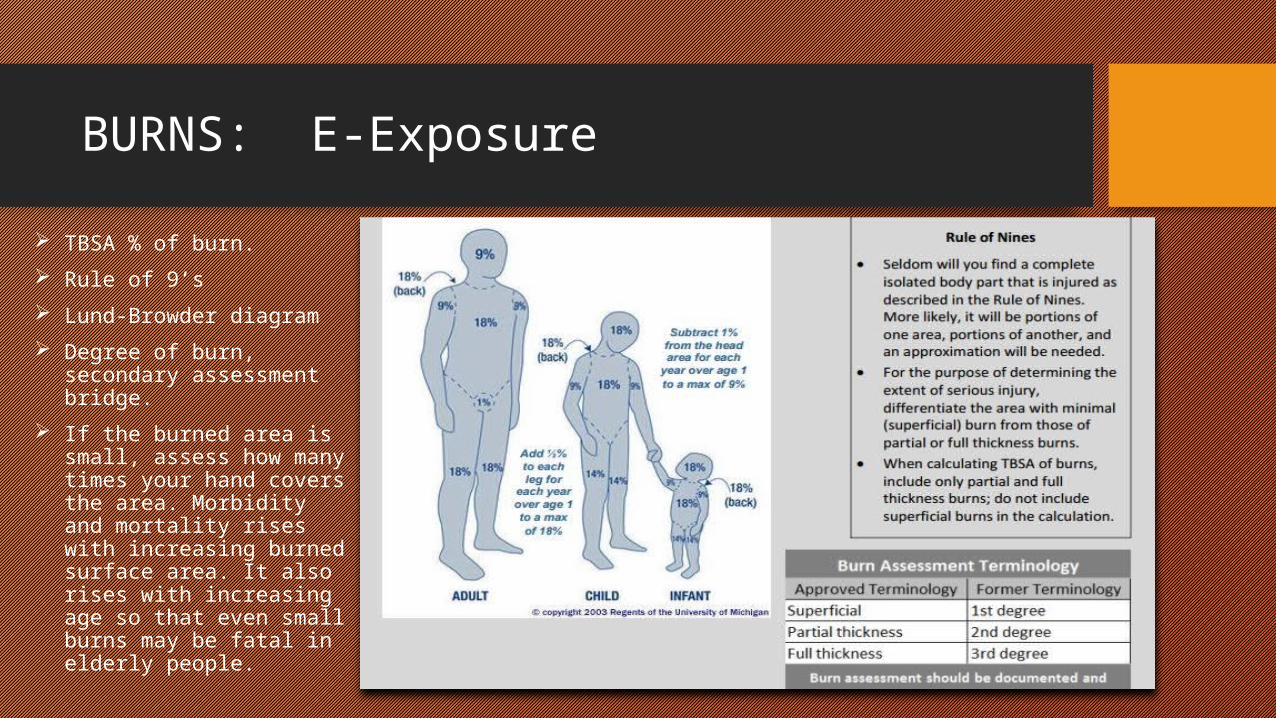
BURNS: E-Exposure
TBSA % of burn. Rule of 9’s Lund-Browder diagram Degree of burn, secondary
assessment bridge. If the burned area is small,
assess how many times your hand covers the area. Morbidity and mortality rises with increasing burned surface area. It also rises with increasing age so that even small burns may be fatal in elderly people.
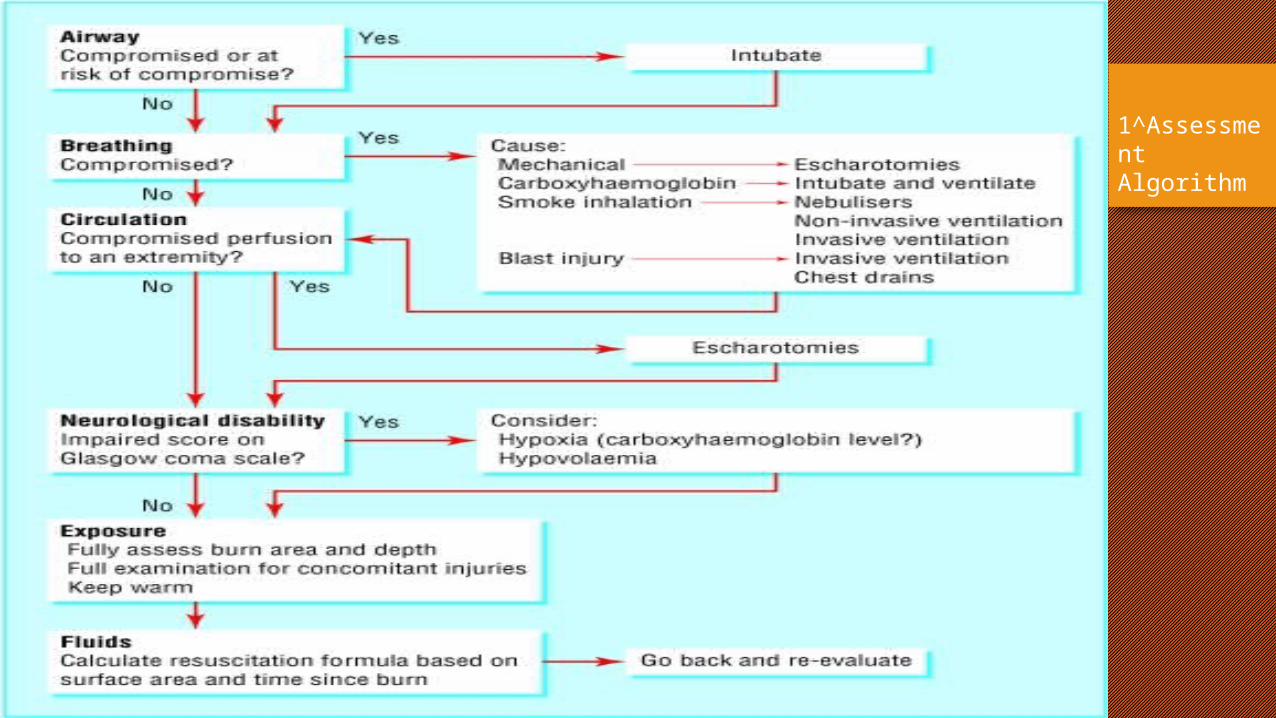
1^Assessment Algorithm
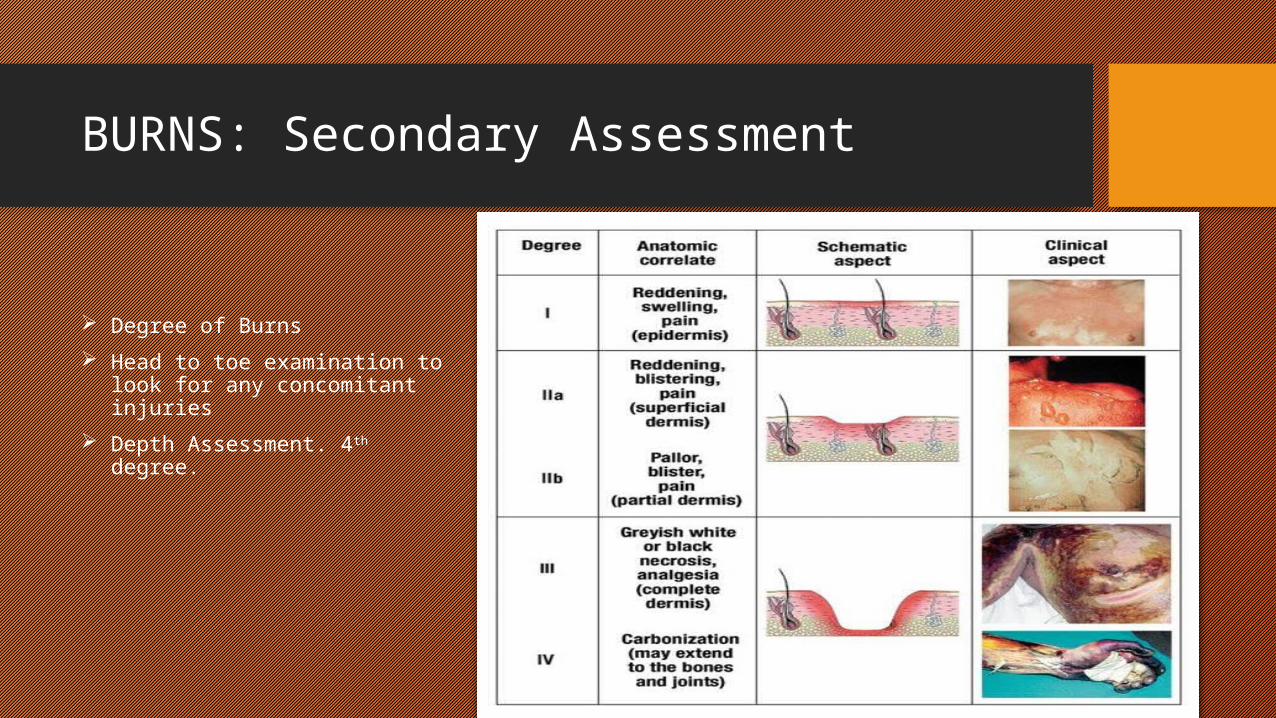
BURNS: Secondary Assessment
Degree of Burns Head to toe examination to look
for any concomitant injuries Depth Assessment. 4th degree.
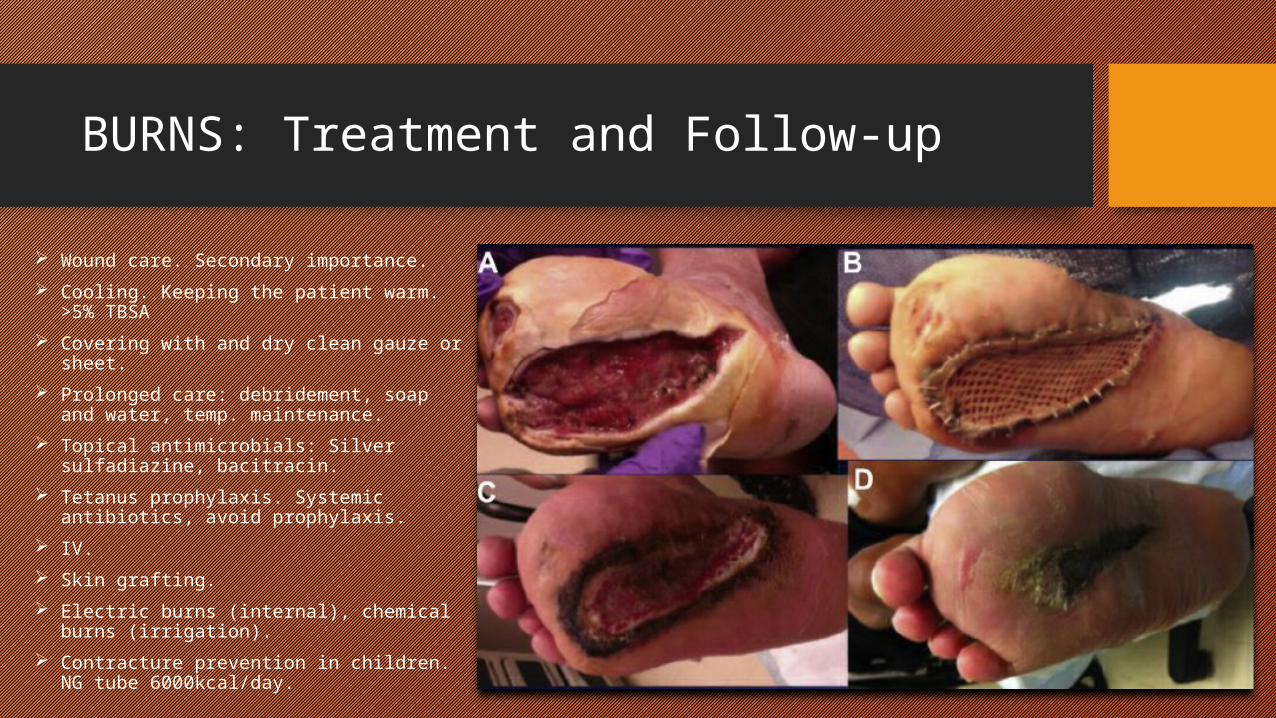
BURNS: Treatment and Follow-up
Wound care. Secondary importance. Cooling. Keeping the patient warm. >5%
TBSA Covering with and dry clean gauze or
sheet. Prolonged care: debridement, soap and
water, temp. maintenance. Topical antimicrobials: Silver sulfadiazine,
bacitracin. Tetanus prophylaxis. Systemic antibiotics,
avoid prophylaxis. IV. Skin grafting. Electric burns (internal), chemical burns
(irrigation). Contracture prevention in children. NG
tube 6000kcal/day.

THANK YOU