canadian society of internal medicine annual meeting 2019 …€¦ · dalhousie university 1...
TRANSCRIPT

Canadian Society of Internal MedicineAnnual Meeting 2019
Halifax, NS
Travel Medicine,The Before & After.
Travel and your patient with chronic illness
PAUL CHARLEBOIS, MD, CCFP, FRCPC, CTROPMED
DALHOUSIE UNIVERSITY
1 CANADIAN FIELD HOSPITAL/ CANADIAN FORCES HEALTH SERVICES CENTRE(ATLANTIC)
QEII HEALTH SCIENCE CENTRE/ DARTMOUTH GENERAL HOSPITAL

CSIM Annual Meeting 2019
Paul Charlebois- Travel Medicine- The Before & After Thursday October 2nd, AM
The following presentation represents the views of the speakerat the time of the presentation. This information is meant foreducational purposes, and should not replace other sources
of information or your medical judgment.
Learning Objectives:• Identify patients who require special counselling prior to
travel.• To have a better understanding of the potential pitfalls your
patients with chronic illness may have when voyaging abroad.
• Assess the likely common and uncommon causes of fever in a returning traveler.
• How to manage fever/ illness in a returning traveler.

Disclosures
I will not be able to make you travel medicine experts in 60 minutes.
What I hope to do is give you some guidelines that will assist your patients at risk who wish to undertake travel.
Disclosures
I have no financial disclosures.
The opinions expressed during this talk are my own and should not be taken as official policy of the Government of Canada or the Department of National Defence.
The information presented during this talk comes primarily from Canadian sources. However, certain international sources will be discussed and care should be taken when applying information from these as they may suggest off-label use for certain therapeutics.
Unless otherwise noted, the photos are my own.

Where does my interest in travel medicine come from?

Outline
Identifying the risk.Travel Medicine resources for the
Internist.The pre-travel consultation.The post-travel issues.Some illustrative cases.

Identifying the Risk

What is the most common vaccine-preventable disease in Canadian travelers?

Why is this important?Population at risk
The World Tourism Organization estimates that by 2030 (11 years from now), the number of international tourists may reach 2 billion.
and
It is estimated that between 15-30% of these people will be 60 years of age or older.
and We are getting much better at managing chronic disease, so these
individuals will have the ability to travel.
Darrat 2019

Why is this important?The statistics.
Unfortunately, people die when travelling abroad.
This pie graph gives a quick snapshot of what befell French travelers in the early part of this century.
Note that infections are only responsible for less than 2% of the total, yet that is what we tend to focus on.
Travel Medicine 3rd Ed.

Why is this important?The statistics.
From another source.
Once again, infections claim only a small number of travelers.
Connolly, R 2017

Why is this important?The statistics.
Death and International Travel-The Canadian Experience 1996-2004
MacPherson DW, 2007

Risks of Travel
Injuries and Accidents Acquired illness
Infectious Diseases
Non-infectious disorders
Mental health issues
Exacerbation of existing illness
Environmental exposures Heat
Humidity
Pollution

Your patients at risk
There are a number of patient groups that are identified in the travel medicine literature that are identified as having special needs. These include: The pregnant or breastfeeding traveler
The pediatric and adolescent traveler
The older traveler The physically challenged traveler
The traveler with pre-existing disease
The immunocompromised patient Those visiting friends and relatives (VFR’s)

Your patients at risk
There are a number of patient groups that are identified in the travel medicine literature that are identified as having special needs. These include: The pregnant or breastfeeding traveler The pediatric and adolescent traveler
The older traveler The physically challenged traveler
The traveler with pre-existing disease The immunocompromised patient Those visiting friends and relatives (VFR’s)
Travel Medicine is constantly changing…
The threats faced by travelers are always in a state of flux.
As with all aspects of medicine, you need to have up to date resources to provide quality care.
What makes Travel Medicine different is that its practice intertwines medicine with:
• geography
• politics
• economics
• climate science
• entomology
• understanding human behavior

Travel Medicine Resources for the Internist

Where can you turn for help?
Travel Medicine Clinics Reference texts
Journals
Travel medicine websites Electronic discussion forums, notifications and feeds.
Other health care professionals.
Travel Medicine 3rd Ed.
Travel medicine clinics
These are often available in larger centres but may not be an option in more rural areas.
Most offer co-ordinated services, such as consultations and vaccinations.
Unfortunately, much of what is offered is not covered under provincial health insurance plans.
The American Society of Tropical Medicine and Hygiene and International Society of Travel Medicine have guides to travel medicine providers in your area.

Reference Texts
Comprehensive overview.
By their nature, textbooks tend to have dated information.
Good for process and organization of approach, but you may need to get more updated information from journals and websites.

Journals
Provide original research and review articles for travel medicine.
Not typically used for ready reference, but review articles may be helpful.
Travel Websites
Large websites are often run by governments or large non-governmental organizations.
Usually well organized and up to date.However, they do have some pros & cons
that you should be aware of.

World Health Organization
Pros
Very world view
Comprehensive
Cons
Comprehensive
Lists all potential therapies including many that are not available in Canada.
Some recommendations are weighted on a cost/benefit analysis for use in lower resource settings
Centers for Disease Control-“The Yellow Book”
Pros
Very comprehensive.
User friendly.
The power of the CDC behind it!
Cons
It is made for US clinicians, and there are some differences between Canadian and American travelers, including:
• Where they travel
• What therapies are available
• Risk tolerance
Committee to Advise on Tropical Medicine and Travel (CATMAT)
Pros
It’s Canadian and is produced by Canadian clinicians.
Recommendations and therapies conform to the needs and availabilities of Canadian travelers.
Bilingual- English/French
Cons
Not quite as slick or comprehensive as CDC website (but covers many of the points).

Electronic Forums, Notifications & Feeds
If you have a large patient population that travels, you may wish to subscribe to a service that gives you regular updates on issues in travel medicine. Examples: TravelMed provided by ISTM.
There are also travel medicine forums that are active on social media (Facebook/Twitter), but be sure you know who is providing the information.

Other Health Care Professionals
Infectious disease specialists Pediatricians
Pharmacists
Immunization clinics that provide Yellow Fever vaccine
Colleagues with an interest in travel

The Pre-Travel VisitTHE “BEFORE”YOUR PATIENT IS EXCITEDLY PLANNING THEIR TRIP!

Again, I am not suggesting you are going to be travel medicine specialists.
However, if you care for people with chronic medical problems, you are in a position to give guidance.
You can save your patient with well controlled heart failure a lot of grief when they announce at their next visit:
“Doc, I’m going on the trip of a lifetime!”

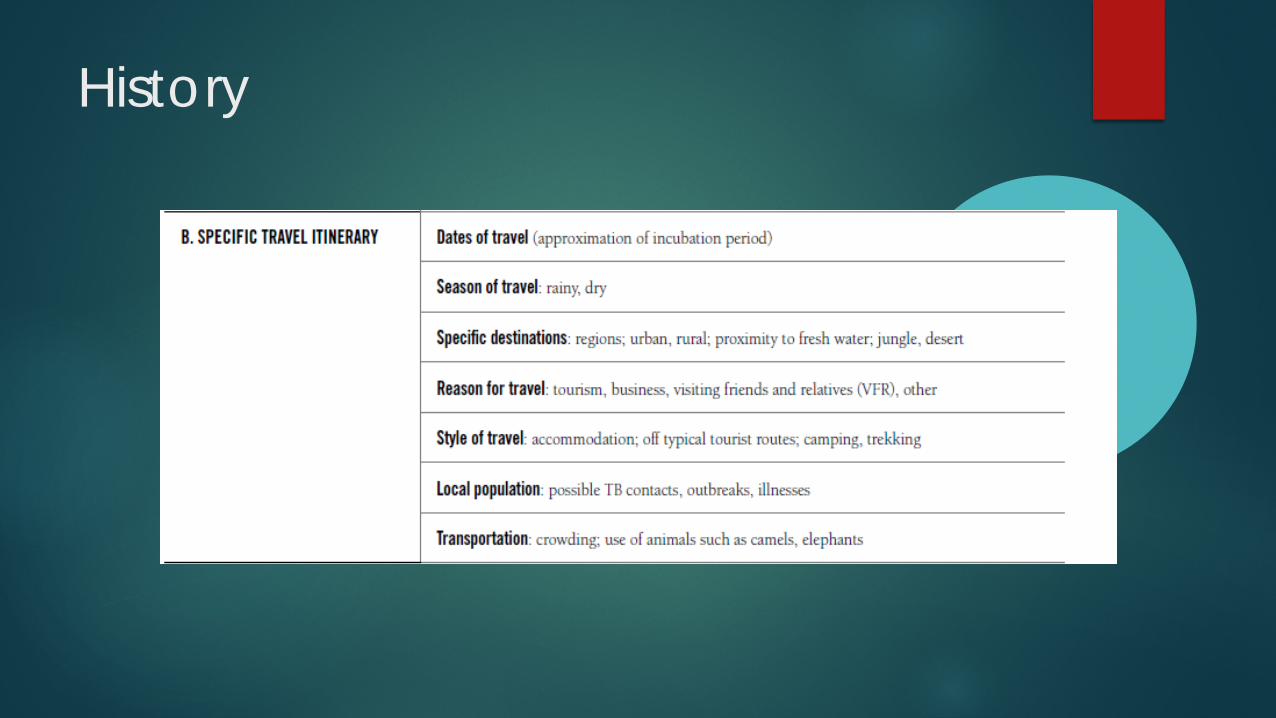
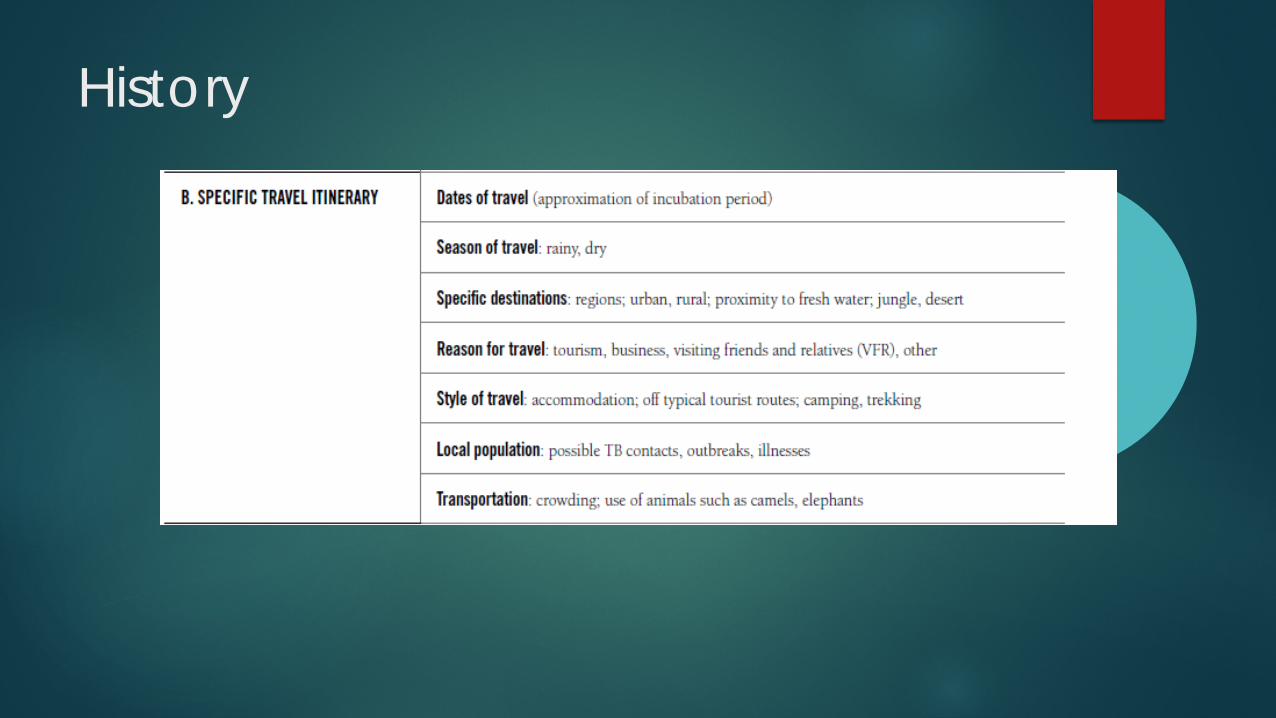
Key pieces of information that will guide your care (or assist you in seeking advice!)*
Exact itinerary
Time of year
Mode(s) of travel
Type of travel
Reasons for travel
* We will revisit these in the second half of the talk when your patient comes home with a medical issue.
CATMAT Fever in Returning Traveller2011

Exact Itinerary
Get specifics Don’t fall into the
“Polar Bear Trap” What time of year? Wet or rainy? Don’t forget about
the equator.

Mode of Travel
Road Transportation River Cruise

Type of Travel
Budget Luxury

Reasons for Travel
PleasureBusinessEco-tourismExtreme vacationsMVRA - Missionary, volunteer, research, aid workStudentVFR?- Visiting Friends and Relatives

Hagmann 2014

Think about what might interfere with your patient’s illness or therapy?

Flying is not physiologic!
Decreased partial pressure of oxygen.
Low humidity.
Expanding and contracting gases.
Immobility.

Specific conditions-Cardiovascular Disease
Compensated heart failure may be particularly hard to control on vacation.
Long bus rides and poor bathroom facilities may lead to diuretic non-compliance.
Over-indulgence in local delicacies can lead to very high sodium intake.
Travel Medicine 3rd Ed.

Specific conditions-Respiratory Disease
Patients with well controlled COPD might manage very well here at home.
However, lung irritants are a real issue in some popular tourist destinations, whether these be natural (sand, dust, pollen) or man made (industrial pollutants).
Make sure your patients have an action plan ready.
CNN.com

Specific conditions-Diabetes
The proper management of diabetes includes careful management of oral intake and timing of insulin.
Travel across time zones is bad enough with jet lag but can really play havoc with diabetes management.
Discussion with their diabetes case manager will be helpful!
When travelling east, your travel day will be shorter. If you lose more than two hours, you may need to take fewer units of intermediate or long-acting insulin.
When travelling west, your travel day will be longer. If you gain more than two hours, you may need to take extra units of short-acting insulin and more food.
-Diabetes Canada Website
worldatlas.com

Specific conditions-Renal Disease
People with well controlled renal disease should be counselled on a few items.
Depending on renal function, certain medications may be contraindicated.
Fluid and salt balance are crucial.
May wish to travel with medications to self-treat travelers’ diarrhea.
Specific conditions-Gastrointestinal Disease
GI issues are a big problem for the healthy traveler.
When you have a pre-existing GI condition, this may be even more of an issue.
May wish to travel with medications to self-treat travelers’ diarrhea.
Some therapies cause your patient to become immunocompromised and can increase risk of infection (next slide).
Bathroom maps and other resources are available through patient support groups and foundations (Crohn’s & Colitis Foundation)

Specific conditions-The immunocompromised patient
The traveler who is immunocompromised faces some challenges:
The inability to receive certain vaccinations (yellow fever as an example).
Increased risk of acquiring certain infections and increased risk of severity of those infections (TB, malaria).
CATMAT Yellow Fever

SummaryEssential Items to be carried by travelers with underlying medical conditions
All required medication and print-out of all prescriptions MedicAlert ® bracelet Health insurance Brief summary of their medical problem including key lab
results/ECG Medical contact in destination country (through travel
agent, insurance or other agency) Emergency medical contact at home

Seeking Healthcare Abroad
This is really something that should be arranged before hand.
Many travel destinations have clinics with North American trained clinicians who can provide services in English.
Remind patients that although in many jurisdictions, medications can be purchased without a prescription, counterfeit medications are a big business in many parts of the world!

Questions up to now?

Post-travel issuesTHE “AFTER”
YOUR PATIENT HAS JUST COME HOME…AND THEY ARE FEELING FEVERISH!

How do we approach a returning traveller with fever?
Answer: just like any other patient… Start with a good history and physical. Where our normal process may fail us is in the
tests we want to order and the pathogens we may face.
Over the next few slides, I hope to outline some of the unique challenges in assessing fever in a returning traveller.

My Resource

A Disclosure…
The Goal of this Assessment
To find out the source of the fever. Remember, that it may be related to travel, but then
again it may not be. The goals of initial rapid assessment is to determine if we
are dealing with a life-threatening, highly communicable or treatable illness.

The thought process…

An Important Point
The top four differential diagnoses in a patient returning from a tropical region with a fever:
• Malaria• Malaria• Malaria• Everything else

History

History

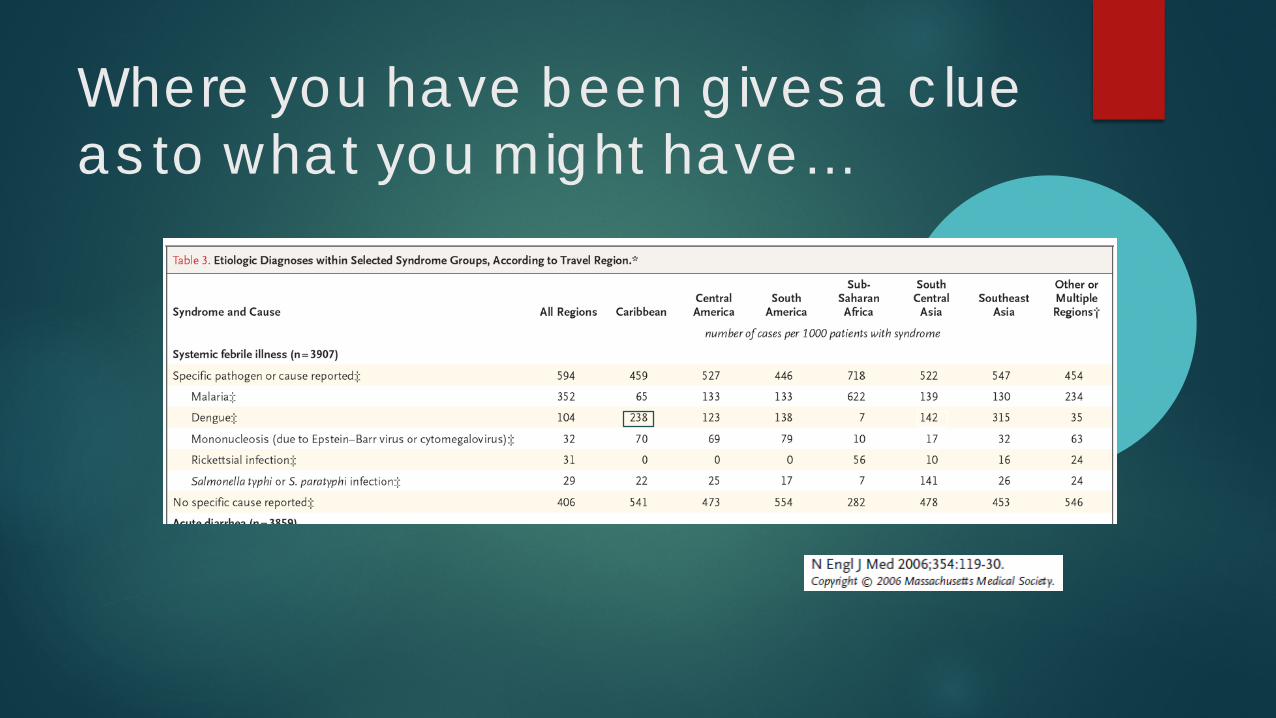
Where in the World?

Where you have been gives a clue as to what you might have…

History

History

History

History

Physical Exam
A complete physical exam is essential. Goal will be to look for signs of exotic disease, while ensuring you do
not miss a common local pathogen.
You must do a careful skin exam to look for bites and rashes. Excessive modesty may lead to a missed diagnosis!!!

Laboratory Investigations

Laboratory Investigations

Empiric Treatment

Empiric Treatment

Some Illustrative Cases

Remember, the cases that I am presenting were not seen and diagnosed here:

Or here:

Or even here:

But here!

Our Introductory Case…
29 yo female…VFR- 10 day prodrome of feeling mildly unwell after returning from a month long trip to India.
4 day hx of high fevers, arthralgias, constipation- then developed diarrhea
Now in ER- looks very unwell, clinically volume deplete and febrile.

History
No
Yes
History

Where in the World?

Where you have been gives a clue as to what you might have…

Case 1
So from the location of travel and story, three big differentials arise: Malaria (malaria, malaria)
Typhoid
Dengue

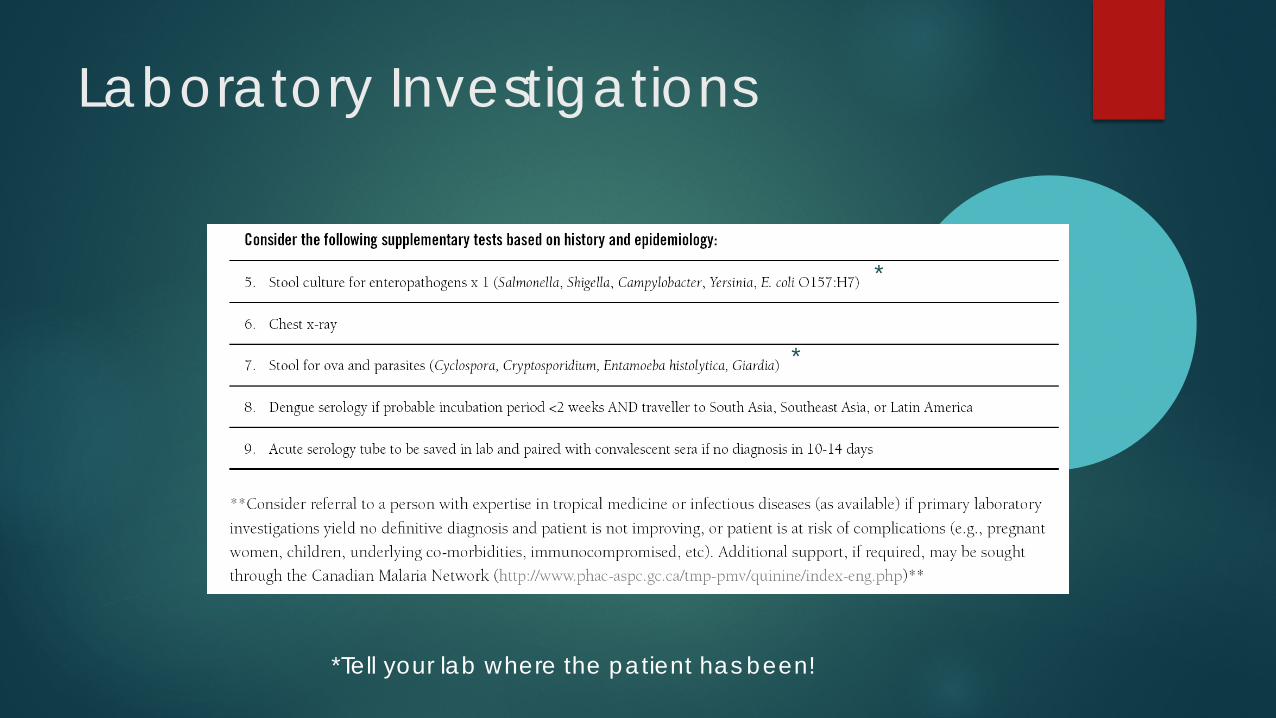
Laboratory Investigations
*Tell your lab where the patient has been!
*
Laboratory Investigations
*Tell your lab where the patient has been!
*
*
Case 1
Seen by ID. Looked better after some fluid. Presumptive diagnosis of malaria- started on Malarone on spec after
all other blood work done.
D/C’ed home because it was felt she was reliable.
Case 1
Next day the blood cultures grew something: Gram- rods
Patient was brought back- she looked more ill and was actually transferred to our stepdown.
Started on high dose broad spectrum abx (IV ceftriaxone 2g q24h)
Case 1
Evenuntually Samonella typhi (or Samonella enterica ser. typhi) was isolated.
Resistant to fluoroquinolones
Patient stepped down to oral trimethoprim/sulfamethoxazole.
Improved over two days and discharged home

Case 2A CAUTIONARY TALE…
Case 2
49 yo Canadian-born pilot, working in the oil fields of Nigeria. Returned to Canada after the latest of many trips to Africa.
Seasoned African traveler
Presents with acute febrile illness approximately 10 days after returning home.

Case 2
In ER, acutely unwell. Severe thrombocytopenia.
Acute renal failure.
Symptoms have been present for less than 24 hours.
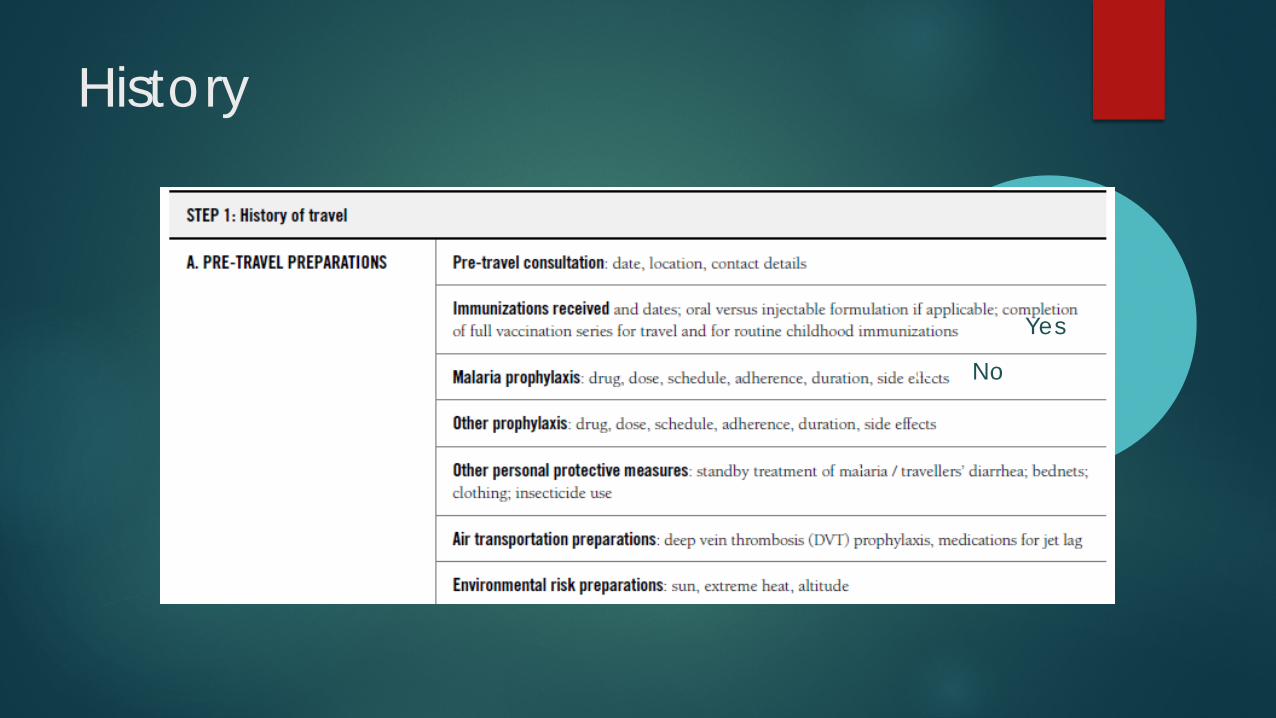
History
No
No
No
No
Yes

History

Where in the World?

Where you have been gives a clue as to what you might have…

Laboratory Investigations
*Tell your lab where the patient has been!
*

Laboratory Investigations
*Tell your lab where the patient has been!
*
*

Case 2
A investigation was performed….

Case 2
Initial malaria smear showed 26% parasitemia!!! Rapidly treated with "newly available" IV anti-malarial agent,
Artesunate.
Despite rapid recognition and response to treatment, he rapidly developed ARDS, AKI and profound anemia.

Case 2
Prolonged ICU stay Intubation
Exchange transfusion
Dialysis Eventual discharge and discontinuation of dialysis.
Patient back home, renal function now normal.

Case 2
This patient should be classified as very fortunate. He knew that malaria was a possibility and did not wait to seek
medical attention. He alerted the ER staff to this possibility. If he hadn't, the outcome might have been very different.

Dr. Jay KeystoneJanuary 28, 1943 - September 3, 2019
Jay was known for his wonderful sense of humour, clever political incorrectness and lectures on travel medicine and how to give a presentation.

Dr. Keystone’s Simple Mantra toAvoid Travel Related Illness
Don’t get bit,(by insects or animals)
Don’t do “it” ,(where “it” is any risky activity without proper protection)
Don’t eat s**t,(food, water and hand hygiene are critical)
and
Don’t get lit!(adhering to the above rules becomes difficult when intoxicated!)

Questions?
References
Travel Medicine 3rd Ed., Keystone, JS, Freedman, DO, et. Al. Ed., Elsevier Saunders, 2013. ISBN 978-1-4556-1076-8
MacPherson DW, et. al. Death and International Travel- The Canadian Experience:1996 to 2004, Journal of Travel Medicine, 14(2), 2007 pp.77-84.
Darrat, M and Flaherty, GT, Retrospective analysis of older travelers attending a specialist travel health clinic, Tropical Diseases, Travel Medicine and Vaccines (2019) 5:17
Hagmann, SHF, Travel-associated disease among US residents visiting US GeoSentinel clinicls afer return from international travel, Family Practice, 2014, 31(6)
Connolly, R, et.al., Repatriation of human remains following death in international travelers, Journal of Travel Medicine, 24(2), 2017, pp1-6
CATMAT, Fever in the Returning International Traveller Initial Assessment Guidelines, CCDR Vol 37 July 2011.
CATMAT, Statement for Travellers and Yellow Fever, CCDR Vol 39, March 2013

Case 3CONSEQUENCES OF A CARIBBEAN VACATION…

Case 3
16 yo male presents with 5 day hx of retro-orbital headache, nausea and vomiting following a vacation to the Dominican Republic.
Symptoms started 13 days after returning home.
Otherwise well.
Stayed primarily on resort with good food and water “discipline”.

History
No
Up to date
History

Where in the World?
Where you have been gives a clue as to what you might have…

Case 3
So from the location of travel and story, three big differentials arise: Malaria (malaria, malaria)
Dengue
Mononeucleosis

Laboratory Investigations
*Tell your lab where the patient has been!
*

Laboratory Investigations
*Tell your lab where the patient has been!
*
*

Case 3
Work-up completed. He looked unwell.
Mild elevations in transaminases, mild thrombocytopenia. WBC 5
No focal or localizing signs. Malaria smears negative x2
Responded well to symptomatic treatment
Case 3
Patient defervesced and continued to improve. All cultures negative, malaria smears negative x4
Presumptive diagnosis of dengue.
Dengue serology positive

DENGUE

Case 4PERPLEXING PRESENTATION…

Case 4
58 yo female Just returned from two month long visit with friends and relatives in
Nigeria
Presents with 4 day history of intermittent fever and lower abdominal pain.

History
No
No
No
No

History

Where in the World?

Where you have been gives a clue as to what you might have…

Case 4
So from the location of travel and story, three big differentials arise: Malaria (malaria, malaria)
Rickettsial infection
Katayama fever (say what?)

Laboratory Investigations
*Tell your lab where the patient has been!
*

Laboratory Investigations
*Tell your lab where the patient has been!
*
*

Case 4
Admitted to MTU. Extensive work-up and investigation with nothing positive.
Seen by ID.
After two days, urine grew pseudomonas. Treated with cipro and symptoms resolved