cardiomyopathy in dmd current state of evidence for heart-specific therapy…
DESCRIPTION
Cardiomyopathy in DMD Current state of evidence for heart-specific therapy…. Action Duchenne, London – November 2014. John P. Bourke Consultant Cardiologist & Senior Lecturer. Cardiology Department Freeman Hospital & Newcastle University Newcastle upon Tyne United Kingdom. - PowerPoint PPT PresentationTRANSCRIPT

Cardiomyopathy in DMDCardiomyopathy in DMD
Current state of evidence for heart-specific therapy…
Cardiology DepartmentFreeman Hospital & Newcastle University
Newcastle upon TyneUnited Kingdom
John P. BourkeJohn P. BourkeConsultant Cardiologist & Senior Lecturer
Action Duchenne, London – November 2014
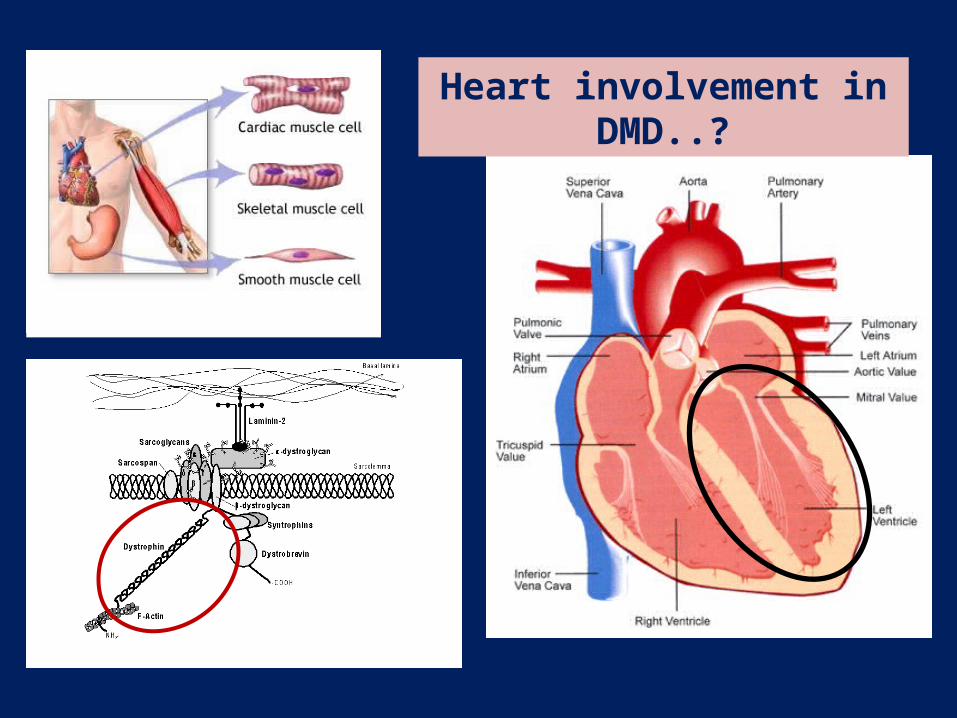
Heart involvement in DMD..?
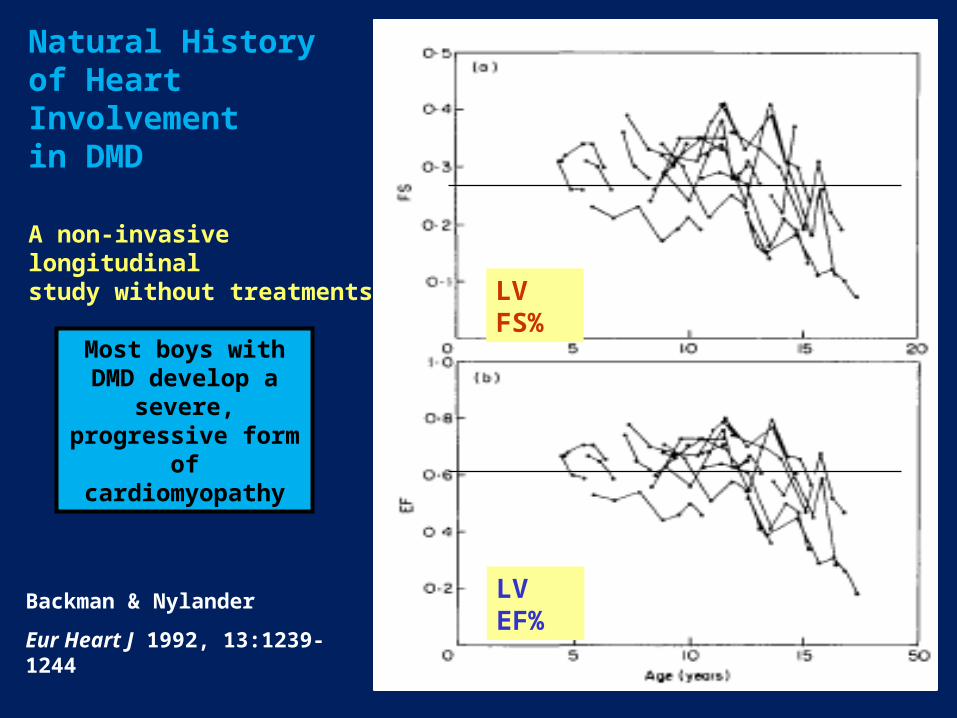
Natural History of Heart Involvement in DMD
A non-invasive longitudinal study without treatments
Backman & Nylander
Eur Heart J 1992, 13:1239-1244
LV FS%
LV EF%
Most boys with DMD develop a severe,
progressive form of cardiomyopathy
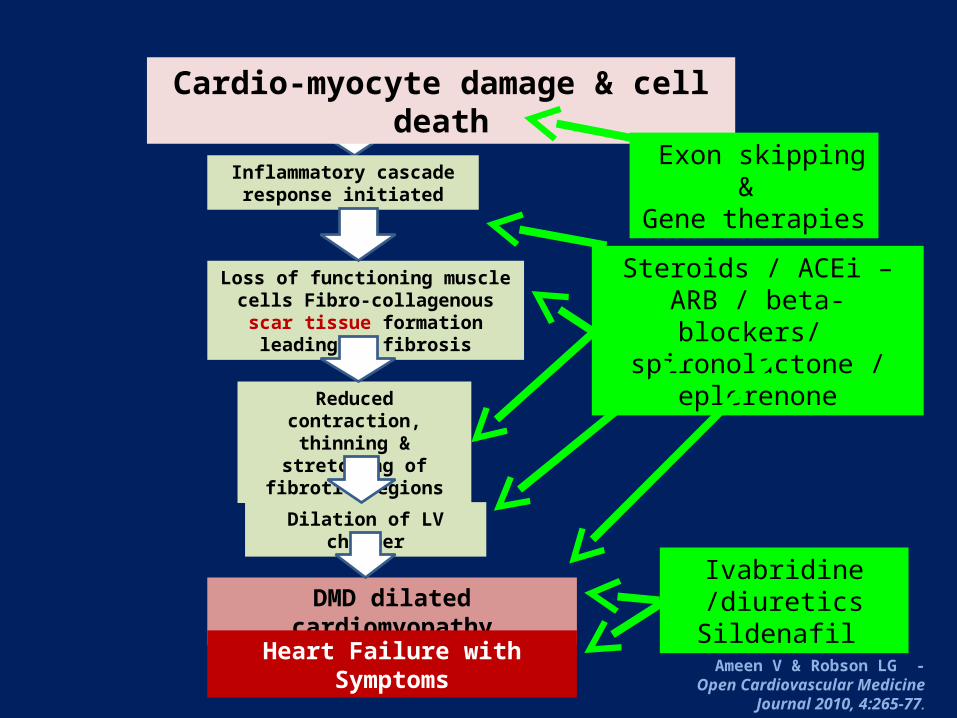
Cardio-myocyte damage & cell death
Inflammatory cascade response initiated
Loss of functioning muscle cells Fibro-collagenous scar tissue formation
leading to fibrosis
Reduced contraction, thinning & stretching of
fibrotic regions
DMD dilated cardiomyopathy
Dilation of LV chamber
Ameen V & Robson LG - Open Cardiovascular Medicine Journal
2010, 4:265-77.
Exon skipping & Gene therapies
Steroids / ACEi – ARB / beta-blockers/ spironolactone /
eplerenone
Ivabridine /diuretics Sildenafil
Heart Failure with Symptoms
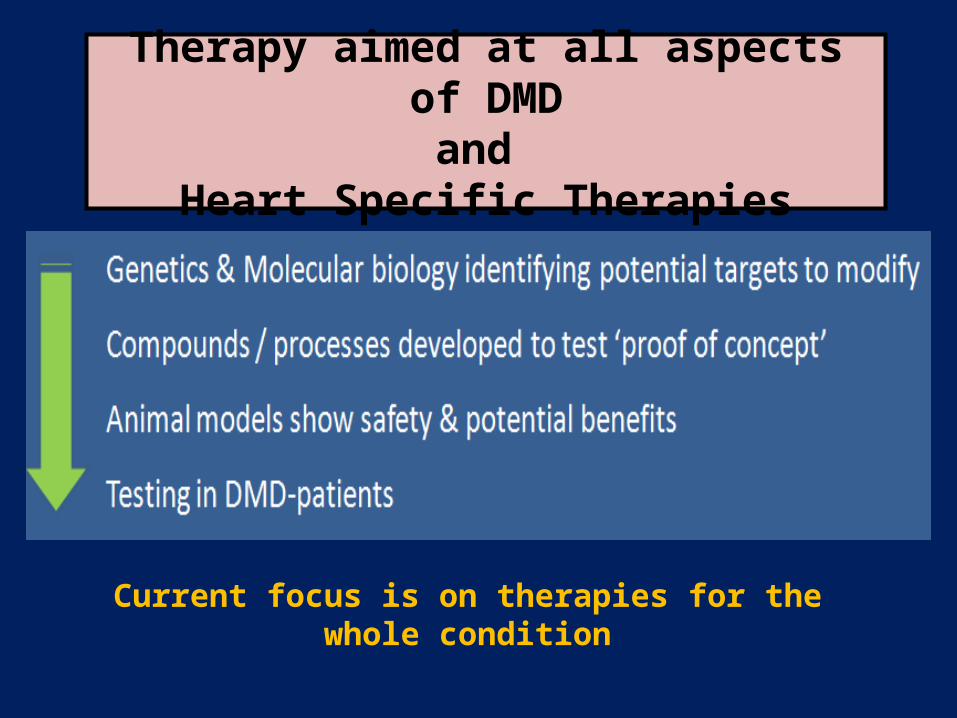
Therapy aimed at all aspects of DMDand
Heart Specific Therapies
Current focus is on therapies for the whole condition
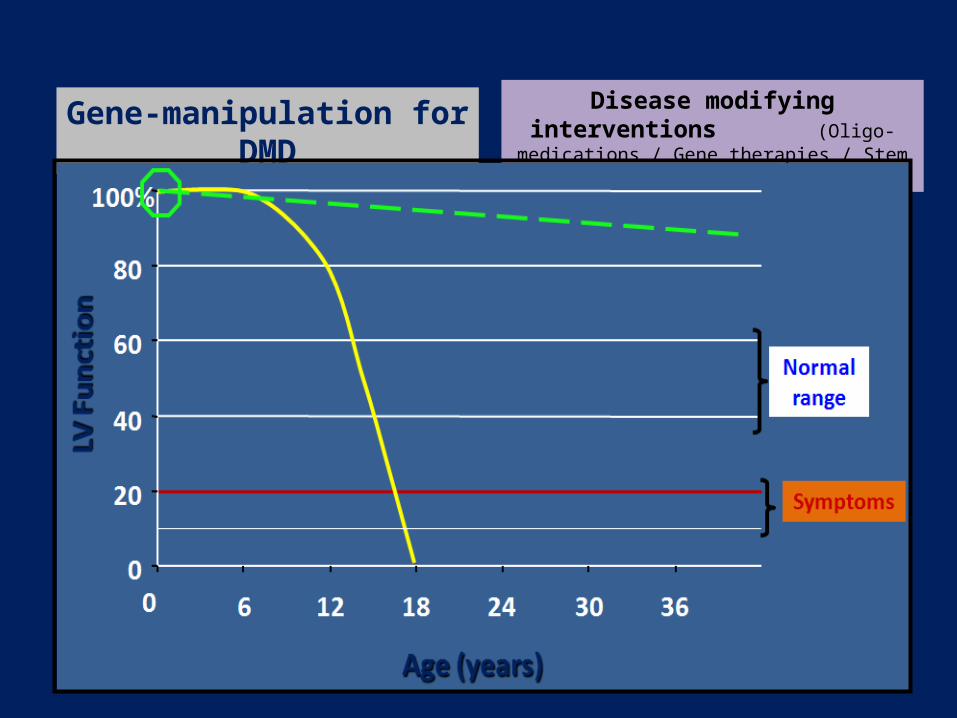
Gene-manipulation for DMD Disease modifying interventions (Oligo-medications / Gene therapies / Stem Cells)

DMD disease-modifying therapies – Heart Issues(?)
Nature of therapy Action
Engrafted foetal cardiomyocytes
mdx mouse & canine models Selective repair seems deleterious to rest of the heart
Cell based therapies - Satellite cells (x)- Mesangioblasts (√)
Multi-potent progenitor cells capable of making any mesodermal tissue (including skeletal or cardiac muscle)
Gene therapy Mini- or micro-dystrophin constructs
Aiming to improve the phenotype (DMD to BMD); Harder to target the heart
Anti-sense oligonucleotides
Exon-skipping[phosphorodiamidate morpholino- oligomers (PMOs)]
Allows production of truncated functional protein (systemic or organ specific delivery)Not all penetrate / benefit the heart
Multiple parallel research programmes in various DMD models ongoing ...

Success of an intervention will be time dependent ..!
Smoke Detector / Fire Extinguisher
Fire Brigade & Rescue
Insurance & Investigation
Therapy of DMD-adults cannot compensate for therapies needed in childhood !

0
20
40
60
80
100%
0 6 12 18 24 30 36
LV F
uncti
onLV
Fun
ction
Symptoms
Age (years)Age (years)
Normal range
Medication & other therapies for Heart Involvement in DMD
Disease modifying interventions (Oligo-medications / Gene therapies / Stem cells)
Drugs to reduce ‘heart strain’ (ACE-inhibitors / ARBs / Beta-blockers /
Sinus node slowing agents)
Drugs to reduce symptoms (Milrinone / Sildenafil / Diuretics / Digoxin)
Drugs to ‘reduce reaction to damage’ (Steroids / Anti-fibrois agents / ARBs)
Mechnaical Pump-support (Pacing / LVAD / Transplant)
Changing the natural history of heart involvement in DMD
Glucocorticoid steroid therapy in DMD
Benefits & Adverse Effects
All cause mortality & cardiovascular outcomes with prophylactic steroid therapy in DMD
► Aim: impact of steroid therapy on cardiomyopathy & mortality in DMD
► Retrospective cohort review of DMD pts on ACEi +/- steroid therapy
► 86 DMD patients (9.1 + 3.5 yrs & followed for 11.3 + 4.1 yrs) - 1972-2006‘... All received ACEi / ARB therapy but steroids at discretion of caregivers & family ..’
► Serial echos & ECGs every 6-12 months
► Deflazacort or prednisolone initiated at 8.6 + 3.5 yrs of age‘..Pts starting steroids were seen by cardiology & ACEi/ARB started at a younger age..’
Schram G, et al. J Am Coll Cardiol 2013, 61:948-54
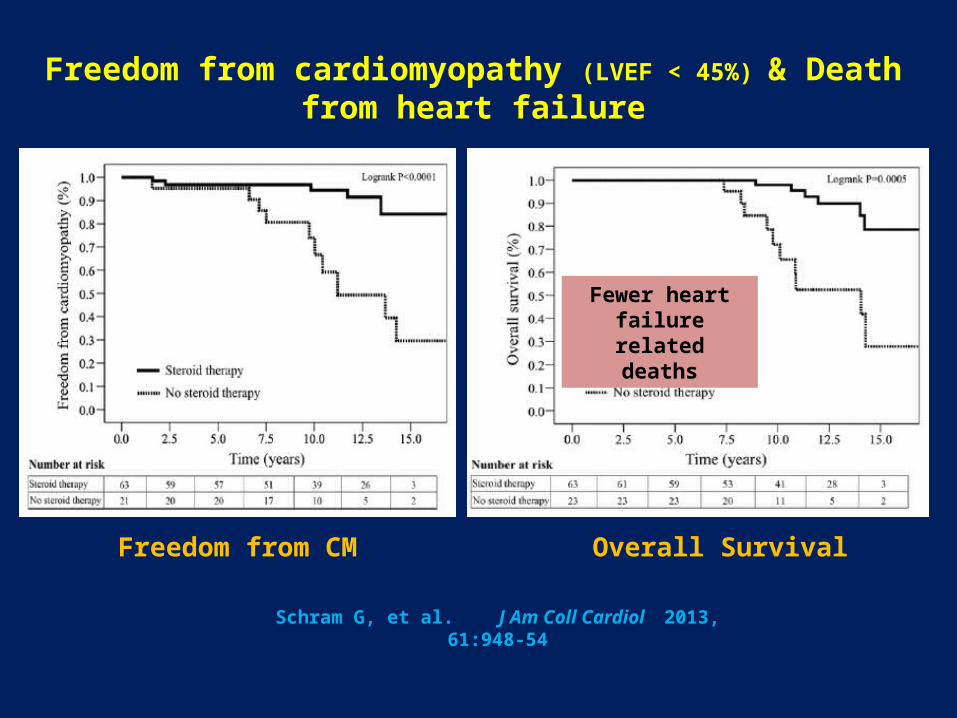
Freedom from cardiomyopathy (LVEF < 45%) & Death from heart failure
Schram G, et al. J Am Coll Cardiol 2013, 61:948-54
Freedom from CM Overall Survival
Fewer heart failure related deaths
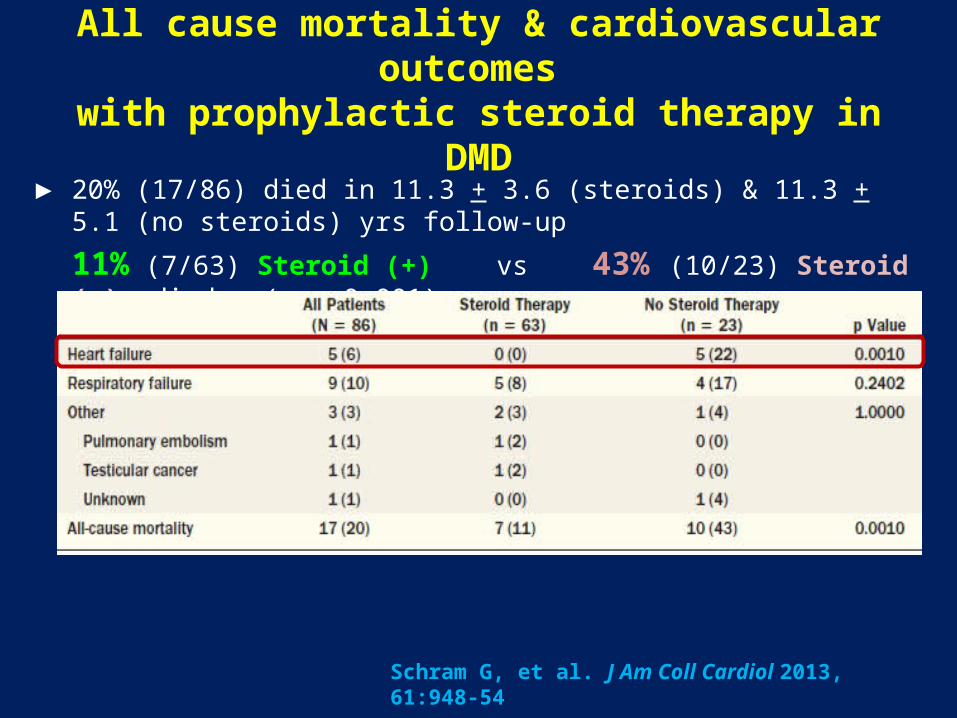
All cause mortality & cardiovascular outcomes with prophylactic steroid therapy in DMD
► 20% (17/86) died in 11.3 + 3.6 (steroids) & 11.3 + 5.1 (no steroids) yrs follow-up
11% (7/63) Steroid (+) vs 43% (10/23) Steroid (-) died (p = 0.001)
Schram G, et al. J Am Coll Cardiol 2013, 61:948-54

Development of Cardiomyopathy
► 28% (21/86) developed LV-dysfunction during follow-up11% (7/63) Steroid (+) vs 61% (14/23) Steroid (-) (p < 0.0001)
► No differences in ECG changes & No arrhythmias in any patient
► Freedom from new-onset cardiomyopathy during follow-up:
► Rate of decline in LVEF% & FS% lower in steroid treated patients
Schram G, et al. J Am Coll Cardiol 2013, 61:948-54
Follow-up (yrs) Steroid (+) Steroid (-)
5 96.8% 95.2%
10 94.4% 73.9%
15 84.1% 29.6%Log-rank p < 0.0001

Steroid effects & the heart in DMD
Silversides et al , 2003 Markham et al, 2005
Steroid agent Deflazacort vs Never Any steroid vs Never
Design Retrospective Retrospective
Age of starting Rx 8.4 + 2 yrs < 21 yrs
Duration of Rx > 3 yrs ---
Patient Number 33 111
Evaluation method Echocardiogram Echocardiogram
ResultsResults Steroid (+) vs (-)Steroid (+) vs (-) Steroid (+) vs (-)Steroid (+) vs (-)
Lost ambulation 48% vs 100%
Cardio-active RxLVEF < 45%LVFS%LVESD (mm)
10% vs 42%5% vs 58%
33 + 7% vs 21 + 8%30 + 6 vs 37 + 8
Lower if steroid (-)< 10 yrs x 4.4 FS% < 28> 10 yrs x 15
Freedom from cardiomyopathy 93% vs 53%
ACE-inhibitors & Beta-blockers in DMD
Benefits when heart already involved

Jefferies JL, et al. Circulation 2005, 112:2799-2804
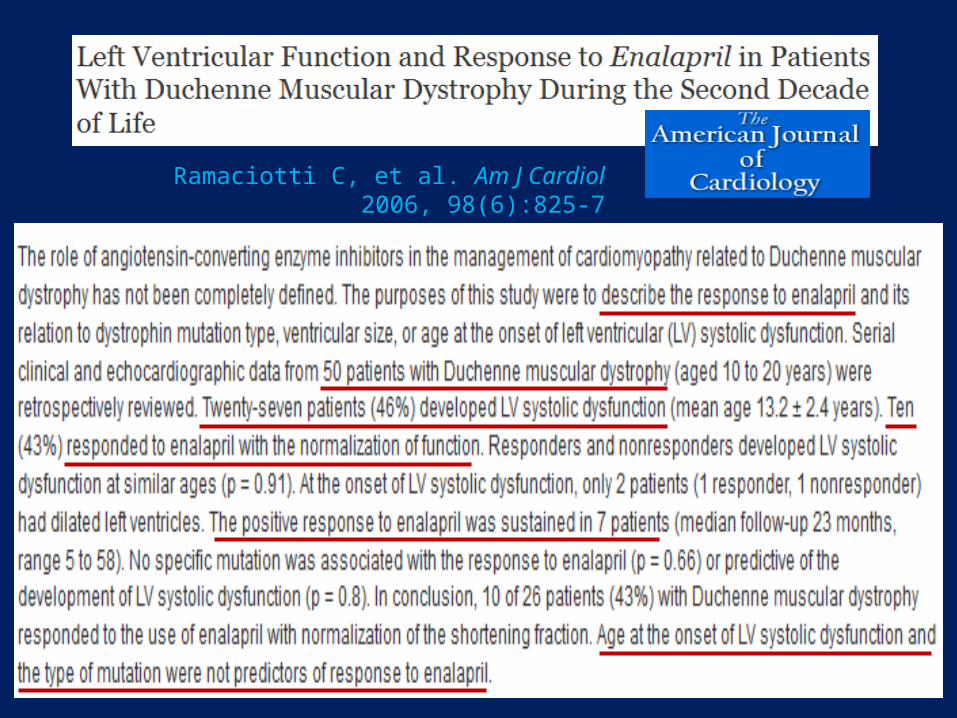
Ramaciotti C, et al. Am J Cardiol 2006, 98(6):825-7
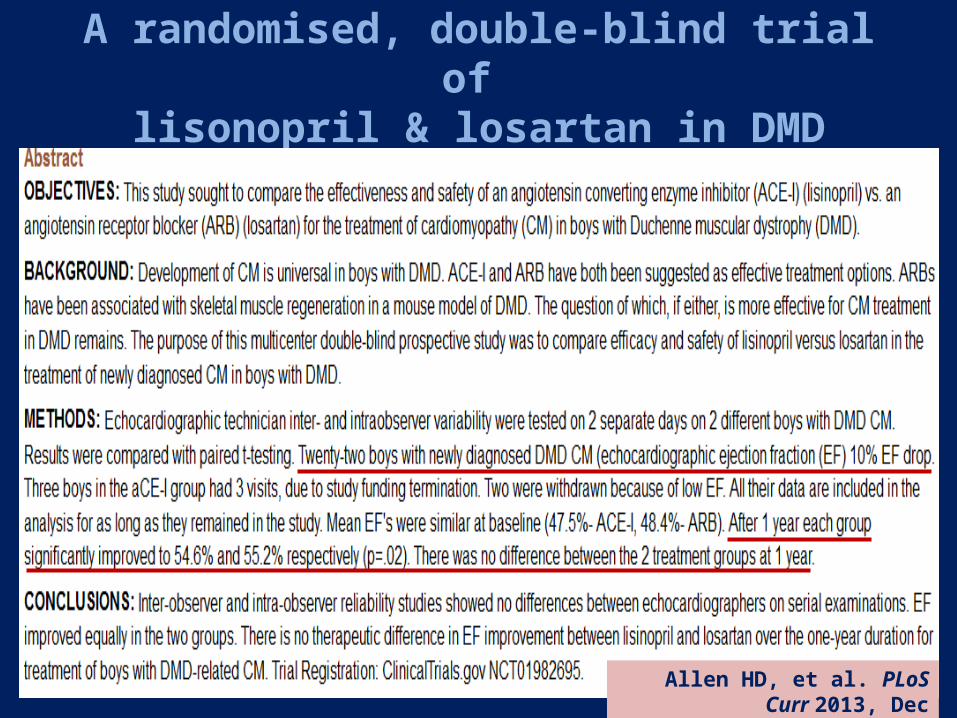
A randomised, double-blind trial of lisonopril & losartan in DMD
Allen HD, et al. PLoS Curr 2013, Dec

Beneficial effects of beta-blockers & ACEi in DMD
Ogata H, et al. J Cardiol 2009, 53(1):72-8

ACE-inhibitors & Beta-blockers before LV-dysfunction in DMD / BMD
Can DCM be prevented?Can DCM be prevented?
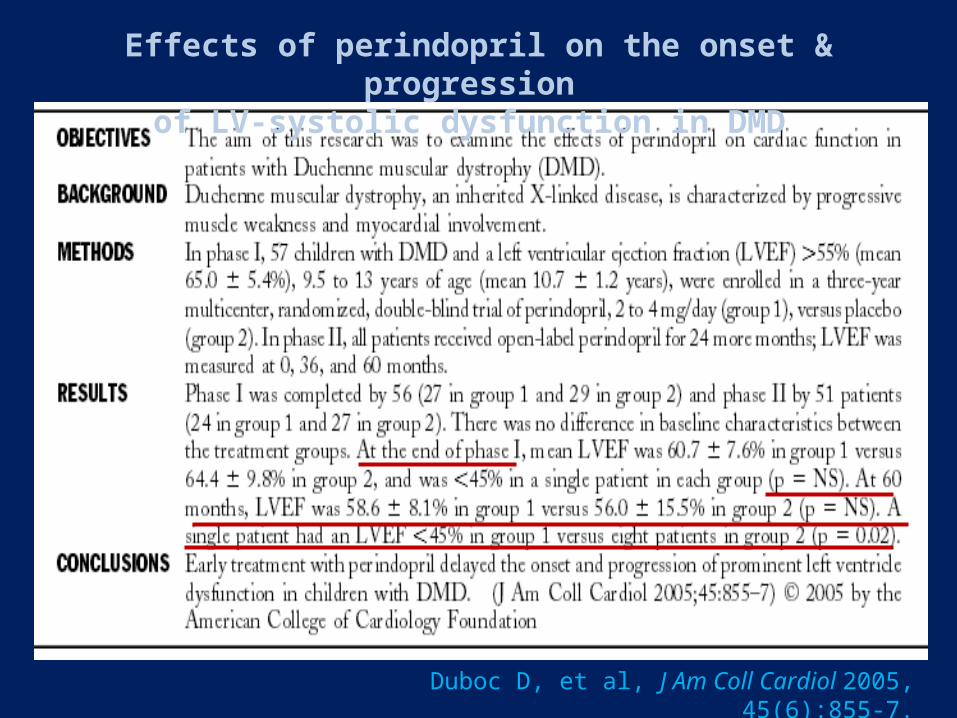
Effects of perindopril on the onset & progression of LV-systolic dysfunction in DMD
Duboc D, et al, J Am Coll Cardiol 2005, 45(6):855-7.

Perindopril preventive treatment on mortality in DMD: 10-year follow-up
♥♥DMD boys 9.5 to 13 yrs & normal LV functionRandomised to perindopril (2-4 mg) or placebo x 3 yrs Open-label perindopril to all thereafter for < 10 yrs
Duboc et al - Am Heart J, 2007, 154:596-602
PerindoprilPerindopril
ThroughoutThroughout(n=28)
Placebo Placebo
InitiallyInitially(n=29)
p
Baseline characteristics
--- --- NS
Alive at 10 yrs 26 (93%) 19 (66%) 0.02
Kaplan-Meier plot --- --- 0.013
ACE-inhibitors: Adverse Effects
► Common hypotension, cough, hyperkalaemia, headache, dizziness, fatigue, nausea, renal impairment
- Persistent dry cough due to bradykinin increase
- Rash & taste disturbance commoner with captopril
- Particular risk of renal failure if renal impairment , NSAIDs & diuretics / dehydration
- Hyperkalaemia due to suppressed aldosterone levels
particularly if in combination with spironolactone / eplerenone
Other drugs for the heart ...
◊ Anti-fibrosis agents (spironolactone / eplerenone)
◊ Ivabradine (sinus node slowing agent)
◊ Growth Hormone (LV- hypertrophy effect)
In heart failure:In heart failure:
◊ Diuretics (furosemide / bendroflumethiazide)
◊ Nitrates (venodilators)
◊ Phosphodiesterase-5 inhibitors (Sildenafil)
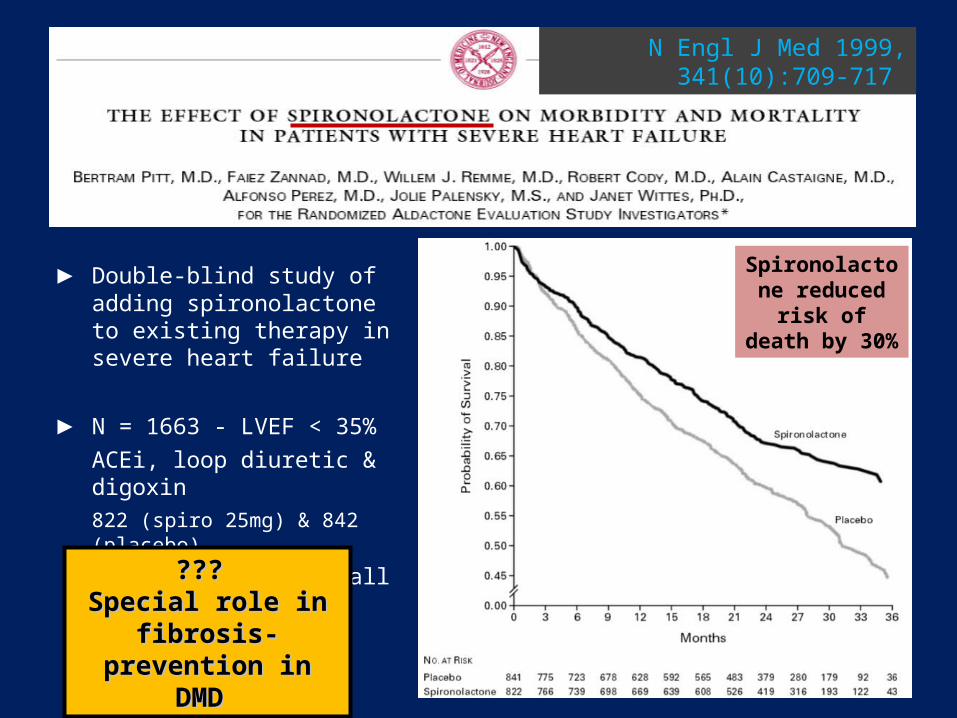
► Double-blind study of adding spironolactone to existing therapy in severe heart failure
► N = 1663 - LVEF < 35%ACEi, loop diuretic & digoxin822 (spiro 25mg) & 842 (placebo)
End-Pt: Death from all causes
N Engl J Med 1999, 341(10):709-717
Spironolactone reduced risk of death by 30%
??? ??? Special role in fibrosis-Special role in fibrosis-
prevention in DMD prevention in DMD
Aldosterone Antagonists (spironolactone & eplerenone)
► Spironolactone (widespread effects)
Gynaecomastia, hyperkalaemia & renal dysfunctionRequires careful monitoring of urea, creatinine & electrolytes
Spironolactone dosage should be no < 25-50 mg/day
Contraindicated, if serum potassium > 5 mmol/l
or serum creatinine > 220micromoles/l
► Eplerenone (~ 1000 times more cardio-specific ....)
Less gynaecomastia but otherwise as for spironolactone
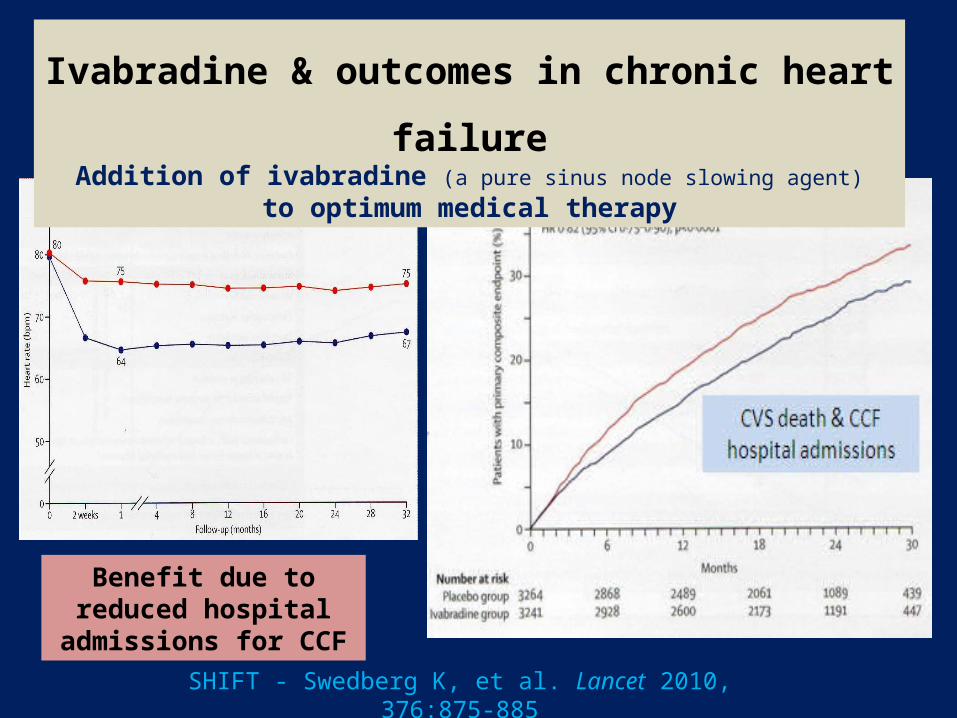
Ivabradine & outcomes in chronic heart failureAddition of ivabradine (a pure sinus node slowing agent)
to optimum medical therapy
SHIFT - Swedberg K, et al. Lancet 2010, 376:875-885
Benefit due to reduced hospital admissions for CCF

Treatments already available for Cardiomyopathy in DMD
Drug Class Action Evidence
Glucocorticoid steroids PrednisoloneDeflazacort
Prolong ambulation / reduce inflammation / maintain cardio-respiratory function
EstablishedEstablished therapy until non-ambulant(adverse effects limit use)
ACE-inhibitors / ARBs PerindoprilEnalaprilLosartan
Delay / prevent remodelling of left ventricle / Anti-fibrotic action (angiotensin & TGF-ß1 blockade)
EstablishedEstablished therapy (early deployment better)
Beta-blockers MetoprololBisoprololCarvedilol
Slow heart / reduce force of LV-contraction
EstablishedEstablished therapy(early deployment probably better)
Aldosterone antagonists SpironolactoneEplerenone
Reduce / prevent fibrosis Theoretical data & use in other contexts supports use(high K-risk with ACEi)
Calcium channel blockers DiltiazemFlunarizine
?? Reduce calcium influx into cells No benefit to date
Anti-oxidants Q10 Idebenone
No benefit to date
How far should we escalate therapies for cardiomyopathy in DMD …?
0
20
40
60
80
100%
0 6 12 18 24 30 36
LV F
uncti
onLV
Fun
ction
Symptoms
Age (years)Age (years)
Normal range
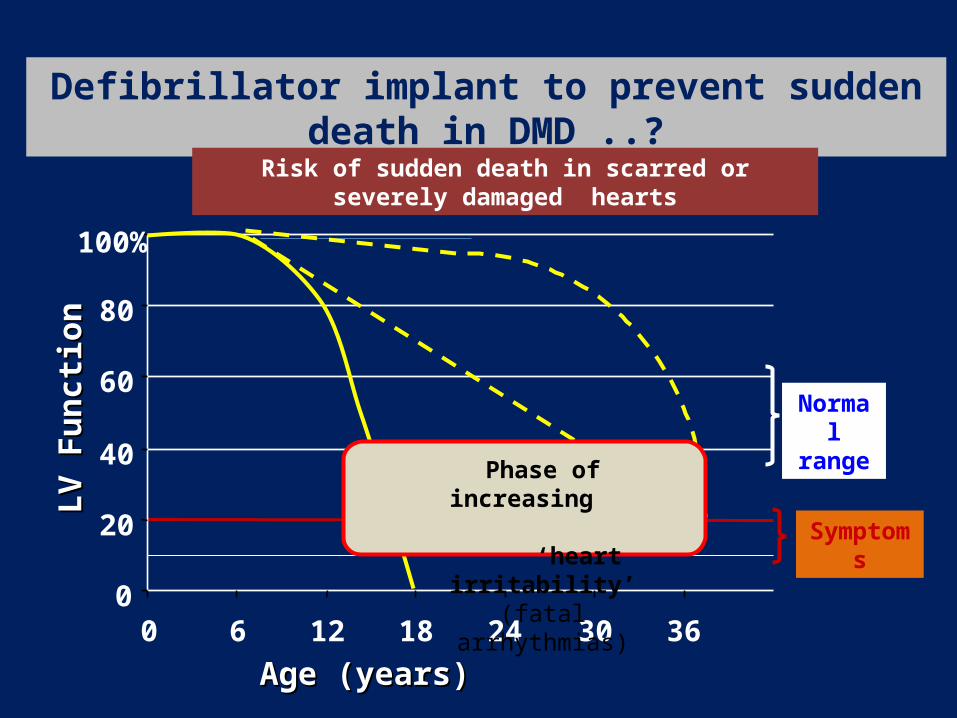
Defibrillator implant to prevent sudden death in DMD ..?
Risk of sudden death in scarred or severely damaged hearts
Phase of increasing ‘heart
irritability’(fatal arrhythmias)
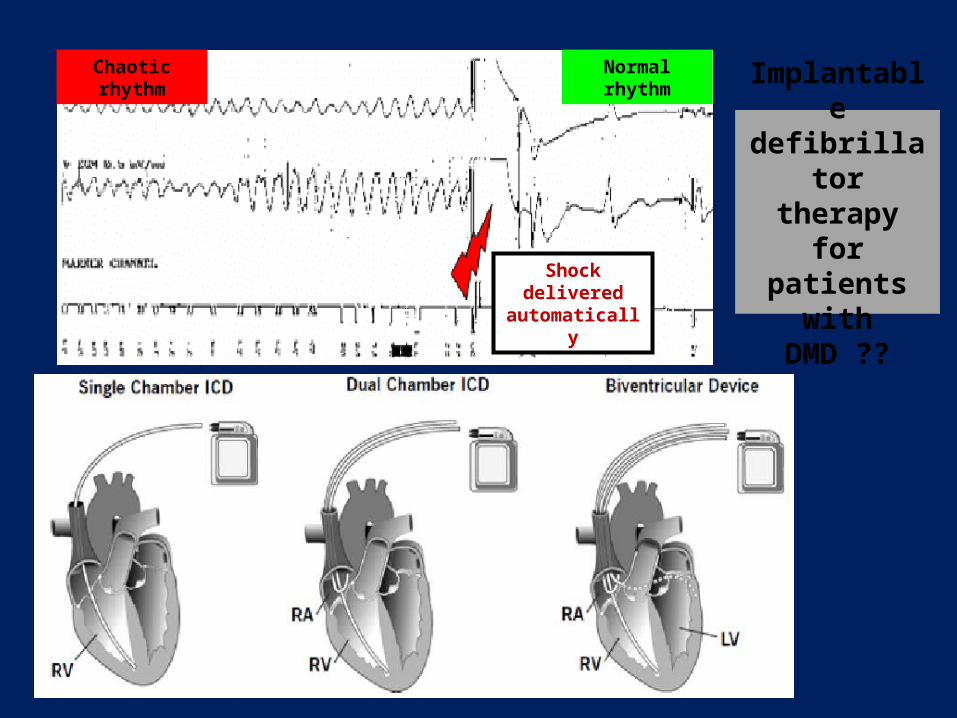
Implantable defibrillator
therapyfor patients
with DMD ??
Chaotic rhythm
Shock delivered automatically
Normal rhythm
Impact of ICD therapy on QoL in DMD?
A registry of DMD-patient experiences & outcomes of ICD therapy, if deployed?

Implantable LV-Assist DeviceImplantable LV-Assist Device
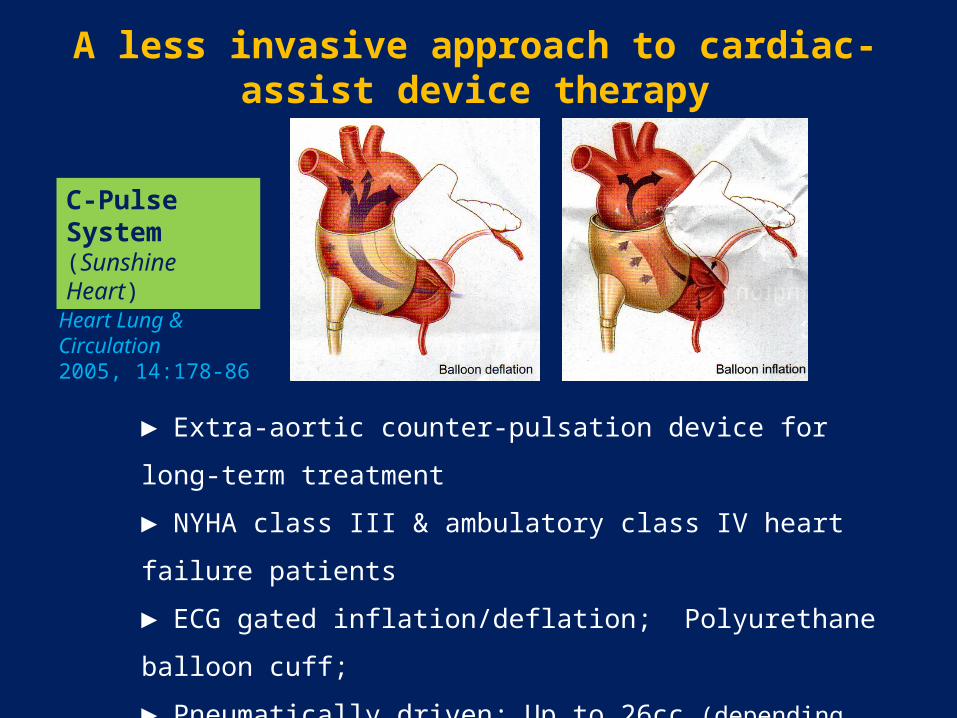
A less invasive approach to cardiac-assist device therapy
► Extra-aortic counter-pulsation device for long-term treatment
► NYHA class III & ambulatory class IV heart failure patients
► ECG gated inflation/deflation; Polyurethane balloon cuff;
► Pneumatically driven; Up to 26cc (depending on aortic size)
► Full or mini-sternotomy implanted;
► EF increased over time by up to 30% !!
Davies et al. Heart Lung & Circulation 2005, 14:178-86
C-Pulse System (Sunshine Heart)
Significant progress but much uncertainty ...
► Stick with what we know is beneficial or begin to combine therapies?
Steroids alone until LV-impaired orSteroids + ACEi + BB + spironolactone from early years
► Content to keep patients asymptomatic alone or push for longer survival?Add ICD therapy to protect against SCD
► Add LV-assist devices when heart failure symptoms intervene despite drugs or time for palliative care pathways?
LVAD or Counter-pulsation devices
How far is it ethical / justified to escalate therapy?

The BHF-funded ‘DMD Heart-Protection Trial’ (Ongoing)
To determine in a major clinical trial whether starting:
◊ combination therapy with ACE-inhibitor & beta-blocker
◊ before the onset of echo-detectable LV dysfunction
◊ delays onset or slows progression rate of cardiomyopathy
◊ five-UK-centre, double-blind, randomised, placebo-controlled trial
◊ over 5 years (2 years recruitment / 3-5 years follow up)

The BHF-funded ‘DMD Heart-Protection Trial’The BHF-funded ‘DMD Heart-Protection Trial’
Inclusion Criteria Inclusion Criteria Recruitment ends 31/12/2014 !!
◊◊ Boys 7 – 12 years old with genetically proven DMDBoys 7 – 12 years old with genetically proven DMD
◊◊ LVEF LVEF >> 60% by Simpson’s biplane method 60% by Simpson’s biplane method (normal range = 63 + 5%)
◊◊ No global or regional wall motion abnormalities No global or regional wall motion abnormalities (echocardiogram)
◊◊ Informed consent from parents / guardians & child’s assentInformed consent from parents / guardians & child’s assent
◊◊ No contra-indication to perindopril or bisoprololNo contra-indication to perindopril or bisoprolol
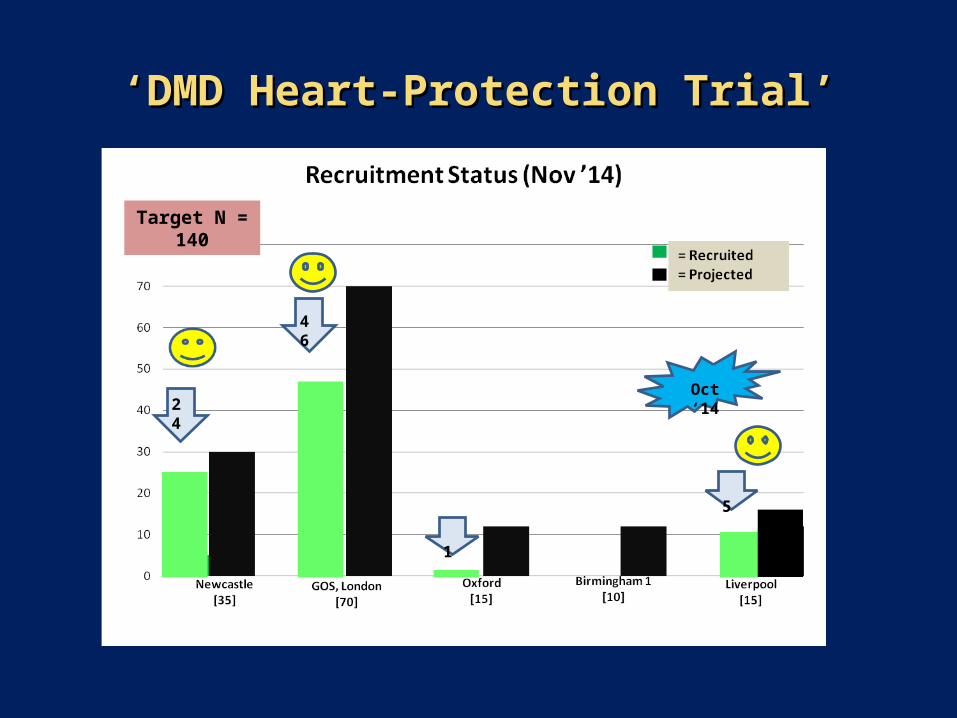
‘‘DMD Heart-Protection Trial’DMD Heart-Protection Trial’
Target N = 140
Oct ‘1424
46
1
5
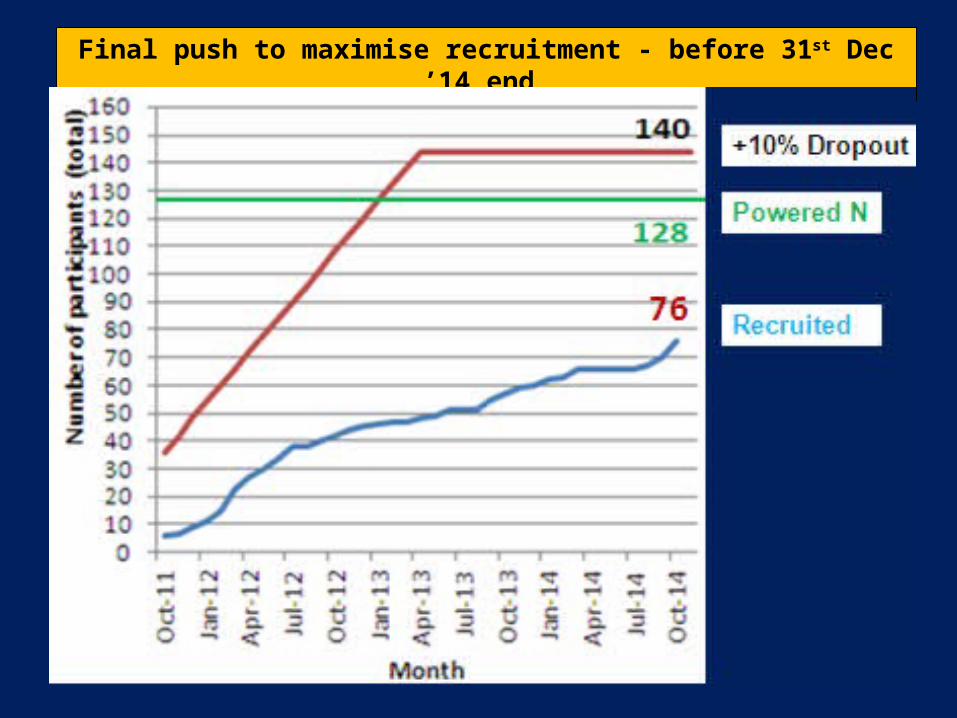
Final push to maximise recruitment - before 31st Dec ’14 end