carol adair key messages for practice and policy
TRANSCRIPT

Concurrent Substance Useand Mental Disorders in Adolescents:Key Messages from the Current Literature forPractice and Policy
C.E. AdairACCFCR PresentationJanuary 20, 2010Edmonton, Alberta

Page 2
A Brief Overviewof The Review
Acknowledgements:T. Bischoff, N. Petrowski, S. Jones, L. Simpson, D. Ma, A. Adair
Page 3
Purpose, Methods, Overall Impressions• to capture and synthesize current knowledge and practice on the topic of
concurrent SUD/MD in adolescents to inform policy‐making, services and research planning, and practice
• systematic = to reduce bias/ensure others would come to the same conclusions
• 3 main strategies: The search detail is documented Abstracts chosen using specific criteria and rater agreementQuality articles given greater weight
• knowledge is fragmented but has advanced rapidly, and is of reasonably good quality

Page 4
Contents of the Report
• Concept, Terms, and Definitions• Epidemiology• Natural History/Longitudinal Course• Findings from Etiologic (Causal) Research• Individual, Societal and Family Burden• Pathways to Care/Service Use• Interventions for Adolescent Concurrent Disorders• The ‘Big Picture’: Service Systems and Policy• Synthesis and Top Recommendations
Appendices:– Glossary of Definitions– Studies of Prevalence– Prevention Programs– Recommended Reading– Resources from the Grey Literature

Page 5
The REAL Purpose
Could Noah’s Life Have Been Saved? Confronting Dual Diagnosis and a Fragmented Mental Health SystemGordon R. Seidenberg, Psychiatric Services, Vol. 59 (11); November 2008

Page 6
A Brief Overview of the Topic:Concurrent Substance Use
and Mental Disorders in Adolescents

Page 7
Concepts, Definitions, Terms
• comorbidity, comorbid disorders, co‐occurring disorders, concurrent disorders, dual disorders, dual diagnosis……
“a combination of mental, emotional and psychiatric problems with the use of alcohol and/or other psychoactive drugs”(Health Canada 2002)

Page 8
Epidemiology: FrequencyPrevalence depends….on where you look:
Whole Population: 3‐4%(15‐24 year olds/2x other ages)
Primary Care: 7%
MH tx settings (OP/IP): 12‐67%
SUD tx settings (OP/IP): 55‐85%
High Risk Groups/Settings:juvenile justice, child welfare/foster care, homeless/runaway youth:
concurrent disorders are the rule rather than the exception

Page 9
Epidemiology: Who is at Risk?• Most Associated Disorders: disruptive behavior disorders, mood disorders,
PTSD, eating disorders, and borderline personality disorder
• Gender: among those with disorders, girls at slightly higher risk for concurrence overall and present a greater range and severity of psychopathology.
• Age: increase with age in teen years, but in some treatment settings may be more prevalent in younger.
• Ethnicity: Differences not marked; where found attributed to social disadvantage. Review of FN/aboriginal studies – all higher rates of disorders and much lower rates of service use
• KEY to check literature relevant to specific settings/populations to know what to expect/how to plan

Page 10
Natural HistoryChildhood/preadolescent mental disorders (esp. DBDs) are strongly
associated with SUDs in adolescence…• Several studies, including a large NZ birth cohort followed 25 years have documented this
pattern using rigorous analyses• Childhood disorder nearly quadruples the risk of a disorder in adolescence • The earlier the MD the earlier SUD onset, and the worse the course and outcome• Even children with MDs in treatment often went on to develop SUDs• The preadolescence (ages 9 ‐ 12) was a particularly “risky period for development of these
problems” (Mason 2004)
Adolescent concurrent disorders are strongly associated with disorders in early adulthood (SUDs, mood, personality)• Mental health issues (broadly defined) are very persistent through to young adulthood; few
resolve without intensive intervention • Studies looking back find 75% of adults with substance abuse
have a history of mental health issues

Page 11
Noah’s Dad on Natural History

Page 12
Natural HistoryWhich comes first?
it depends on the disorder paire.g. depression/AUD
Understanding the exceptions….….• The ‘off diagonal’ trajectories:• troubled adolescents who “turn their lives around and become well‐
functioning young adults”• those who do well as adolescents and then “fall apart during the
transition” to adulthood.

Page 13
Causal Mechanisms
Page 14
Noah’s Dad on Causal Mechanisms
Page 15
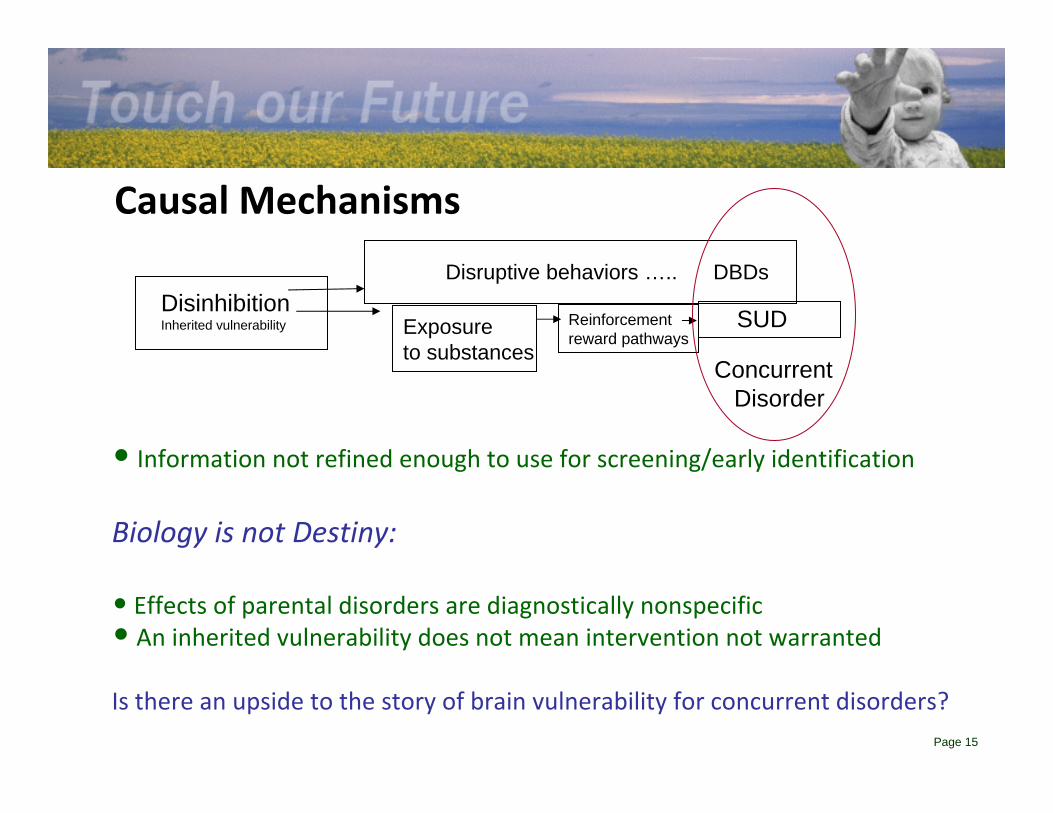
Causal Mechanisms
DisinhibitionInherited vulnerability
ConcurrentDisorder
SUDExposureto substances
Disruptive behaviors ….. DBDs
Reinforcementreward pathways
• Information not refined enough to use for screening/early identification
Biology is not Destiny:
• Effects of parental disorders are diagnostically nonspecific• An inherited vulnerability does not mean intervention not warranted
Is there an upside to the story of brain vulnerability for concurrent disorders?

Page 16
Causal Mechanisms (cont.)• parts of the brain that are involved in vulnerability to
addictive behaviors (i.e. centers of motivation, impulsivity and novelty seeking) same parts involved in adjusting to adult roles and in innovation
• underlying processes are adaptive –even if they can go awry
• KEY – understanding helps ensure interventions are developmentally appropriate and see positive opportunities in these processes

Page 17
Risk + Protective Factors• A lot known about risk and protective factors separately, but
good news is that most RF and PF are shared
• Multi‐level frameworks include factors at the individual, interpersonal and environmental levels
• Increasingly studies of complex interactions – such as how specific PFs can buffer specific RFs
• Knowledge of BOTH critical to effective prevention
• Importance of early life and family factors: Brook et al. (2006) emphasize “the centrality of the parent‐child relationship, especially the non‐conflictual mutual attachment between parents and child”.
• SES, social and school success also important

Page 18
Noah’s Dad on Risk and Protective Factors
Page 19
Implications for Intervention

Page 20
Noah’s Dad on Implications for Intervention

Page 21
Key Messages for the System/Policy Level
Page 22
Noah’s Dad on the “System”
Page 23
The Rationale for System/Policy‐level Action
CostsPersonal Earnings – serious MDs will reduce earnings on
average about 16k USD per year – total reduced earnings over 190B
Societal Costs:• estimates high (depression & SUDS whole pop’n) estimated
to exceed 500B USD for the US• know for comorbidity in general that direct and indirect costs
exponentially increase relative to single disorders – smaller groups of individuals account for larger proportion of costs
• no specific cost studies for adolescents – but also know any health condition that comes on early in life has a much greater overall societal costs over time

Page 24
The Rationale for System/Policy‐level Action
Consequences• Morbidity ‐ severity of symptoms and more problematic course of illness
• Associated Illnesses ‐ elevated physical health problems and health risk behavior
• Life Impact ‐ poorer functioning and quality of life; which often continue into adulthood
• Family Burden – emotional, financial ‐ poorly documented ‐ STIGMA
• Loss of Life ‐ suicide and other causes of premature mortality

Page 25
Noah’s Dad on Life Impact, Family Burden and Loss of Life

Page 26
The Current Service “System” ‐ AccessOnly a minority get care:
• The proportion of adolescents that receives care for either a SUD, MD or both is below 50% ‐ some estimates 10% for any SUD (vs. 20% for adults)
• Having >1 disorder increases chance of receiving tx for adults but not consistently for youth
• Proportions who get follow‐up care also small• Long lag times from initiation of problems to service contact, until major life problems are present

Page 27
The Current Service “System” ‐ Access
Clinical factors (e.g. symptoms) have very little to do with contacting care (esp. for SUDS)
• Family factors, adolescent and parent motivation, ability to pay, precipitating events are stronger predictors
• Parental recognition is poor – less likely for SUDs and concurrent disorders; even when parents have concerns and child is taken to see a physician regularly; there is reluctance to raise the concerns

Page 28
The Current Service “System” ‐ Access
Youth rarely seek treatment on their own from conventional services• 97% of youth in a Canadian primary care setting who had 2 or more disorders declined an invitation to speak with their doctorabout their symptoms
• Reasons:• wish to handle the issue on one’s own• do not know what help is available and where to find it• inability to access due to time or cost of treatment• skepticism about the effectiveness of treatment• stigma

Page 29
The Current Service “System” – Course of Care
• Failure to identify ‐ even in settings where one would expect heightened index of suspicion
• Even when identified, often a failure (or inability) to act(refer or provide appropriate care)– E.g. only 15% of 792 youth in St. Louis public mental health care identified
as having a probable SUD had had it addressed over 2 years
• For those identified and treated ‐ concurrent disorders more challenging than single disorders– Difficulty with engagement, adherence with both treatment and
medication, suboptimal tx response, earlier and more frequent relapse, treatment drop‐out, overall a more difficult and protracted clinical course
• Most tx designed for single disorders
Page 30
Noah’s Dad on the Course of Care

Page 31
The Current Service “System” – Outcomes• Sustained symptom and/or functioning improvement achieved in a minority of patients
• Study limitations on outcomes• Bright spots – e.g. body of literature on predictors of
relapse in SUDs that considers presence of a MD that informs relapse prevention

Page 32
The Policy Landscape
International • WHO called for national policies for every country – by 2002 only 7% of
countries• Emphasize that for youth care needs to be different than adult care• Outlined characteristics of effective policies and provide toolkit for
development• U.S. – lots of initiatives for adults – many state‐level system level initiatives
for children and youth but most not specific to concurrent disorders • Australia – treatment systems still quite separate – integration a policy but
little implementation (Godfrey 2005)
Page 33
The Policy Landscape
National• Canada – national (general) mental health strategy MHCC –
additions will include a framework for child & youth mental health service reform generally
• BC child & youth mental health plan (2003) & Alberta child & youth mental health plan (2008) include new funding and actions that have implications for concurrent disorders but concurrent disorders not specifically addressed

Page 34
Noah’s Dad on Integration

Page 35
Is integration (alone) the solution?• Has been considered THE solution for > 10 years, but largely not achieved
• Barriers are well described
• A more nuanced and cautious perspective e.g. Canadian Executive Council on Addictions report “On the Integration of Mental Health and Substance Use Service and Systems”.– prevalence and need level highly variable by population and setting
– integration plans need to consider the risk benefit for both those w/ and w/o concurrent disorders within a broad evidence‐informed strategic planning approach

Page 36
Is integration (alone) the solution?• Recommendations include:
• adequate resources for thoughtful and targeted integration initiatives
• a program of research and demonstration projects (esp. at the systems level)
• a strengths‐based approach which values and recognizes commonalities across mental health and SUD services (among others)
• A population health approach which includes planning for integration of broader health services, and in particular primary care is also advocated.

Page 37
Treatment as Prevention• Effective treatment of child and preadolescentmental health issues now
considered as having “enormous potential” “an exciting notion” “an outstanding opportunity” for prevention of SUDs in adolescence
• Easier to reach and engage at risk and those w/ early symptoms
• “There is now adequate research to warrant viewing certain childhood psychological disorders as reliable signals of greater than average susceptibility to substance abuse…this is a prevention approach that should be considered and evaluated for implementation” (Glantz 2002)
• Practical Suggestions:– clinicians incorporate SUD prevention in treatment– have patients participate in other SUD prevention programs– teach parents about SUD risk and preventive steps
Page 38
System‐Level Changes ‐ ExamplesArticles found for initiatives in several states (late 1980s/1990s); all involving
attempts to coordinate or integrate multiple services for high risk youth with emphasis on community care – few addressed concurrent disorders specifically
• Fort Bragg (North Carolina) – disappointing initial results, but more recent analysis better
• Connecticut – outcomes quite poor for youth w/ concurrent disorders
• Ohio – reduced rate of youth becoming involved with juvenile justice by 30%
• Massachusetts – ambulatory service use increased at lower cost than expected
• Mississippi – system described but outcomes not reported
KEY LEARNINGS – system‐wide changes can be made; evaluation needs to be more sophisticated

Page 39
Going Even Bigger (cont.)Early Life Mental Health Promotion (Australia)Key features:
• risk being identified earlier - driver of a renewed emphasis on very early prevention and intervention
• primary care linked• universal component – all new parents• parenting education• targeted interventions/outreach to at risk of families in need• being tested in a cluster randomized trial (Bayer and colleagues 2007)

Page 40
Going Even Bigger (cont.)• Article drawing on policies and treatment evidence sources in the
UK for addressing adolescent substance misuse• Recommend population approach • Key features (theoretical - not fully implemented):
– education, prevention, early intervention and treatment– holistic, multi-agency, outcome-focused – recognizes differences between adults’ and adolescents’ needs and behaviors – legal frameworks for care of minors incl. competence, age appropriateness, parental
responsibility, confidentiality and protection from harm – youth engagement, age appropriate youth friendly services– co-located with social and educational support services with specially trained staff– four tier framework for stepped model of care
• Authors also recommend detailed evidence-based care pathways approach to enhance implementation and evaluation (Munoz-Solomando 2007)

Page 41
Going Even Bigger ‐ Population Health Approaches
Promotion/Prevention and Early Intervention (PPEI) partnership (Australia) “Headspace”
Key features:• partnership between mental health, SU, and public health professionals• integration of mental health and substance misuse services includes school,
community and traditional mental health service delivery• school-based components: curriculum plus broader whole school approach• includes foci on children of parents with mental illness, on suicide and on
early detection of young people in need • connects specialized mental health care with settings where adolescents
present with problems and/or are comfortable to present• engaging adolescents: confidentiality, competence, youth participation• evidence-based treatment• links to accommodation, education and employment services for young
people aged 12 to 25 years• not much mention of SUDS
(Rowling 2007)(Patton 2007)

Page 42
The Role of Research• Many calls for effectiveness research• Multi‐faceted (complex) interventions in real world settings w/
contextual factors (e.g. At Home/Chez Soi)• Can also examine etiology, so knowledge can be advanced on causes as
well as solutions• E.g. The U.S. NIMH Blueprint for Change: Research on Child and
Adolescent Mental Health which outlines a new cyclical model of treatment research & development. Traditional research time frames (20 years) no longer acceptable
• Knowledge translation and exchange is integrated in the effectiveness research – within which tools and methods for implementation beyond the demonstration projects themselves
• “An increasing understanding of the high prevalence and longer‐term effects of youth onset mental disorders has not yet been adequately matched by intervention research or the evaluation of different models of mental health service delivery”. (Patton et al. 2007)

Page 43
Noah’s Dad on Research
Page 44
Conclusions• There is a depth and richness to the literature on adolescent
concurrent disorders
• Advances have been made on many fronts
• Many points of consensus a chorus of recommendations which are grounded in both evidence and collective wisdom
• No easy solutions and much work remains to be done
• Innovations, ideas and related resources that can be tapped for strategic planning and specific actions in all realms: practice, research and policy
• Concurrent disorders in adolescents are enormously concerning and challenging, but there is much that can be done to reduce their frequency and impact on current and future generations.

Page 45
The Last Word from Noah’s Dad