case of orthopedo >> by najma alamami
TRANSCRIPT

Pediatric dentistry
case Presentation
(08712(


Personal historyPatient name : Aya ahmed alhwamla Age : 8years .Sex : Syrian femaleBirth date :22 / 2 / 2006Phone : 01129442186Address : Alexandria 21 october. Order among sibling : 2th Father occupation : own s shop Mother occupation : housewife
Patient name : Aya ahmed alhwamla Age : 8years .Sex : Syrian femaleBirth date :22 / 2 / 2006Phone : 01129442186Address : Alexandria 21 october. Order among sibling : 2th Father occupation : own s shop Mother occupation : housewife

chief complain
Pt came to dental clinic C/O :bad appearance .Difficulty in eating due to missing and carious
teeth. (mother’s own words(
Pt came to dental clinic C/O :bad appearance .Difficulty in eating due to missing and carious
teeth. (mother’s own words(

dental history
This was the child’s third visit to the dentist.Amalgam restoration of # 84The child has bad experience due to painful
extraction of (#75,#74 ). . Has repeated trauma in anterior region during
childhood period Delay exfoliation of ≠ 51 in comparison with ≠ 61
This was the child’s third visit to the dentist.Amalgam restoration of # 84The child has bad experience due to painful
extraction of (#75,#74 ). . Has repeated trauma in anterior region during
childhood period Delay exfoliation of ≠ 51 in comparison with ≠ 61

medical historyDoes child have or had: Yes no
Has child ever had a prolonged illness or been hospitalized?
√
Has child been or is on any medication ? √Does child have any allergy or adverse
reaction to medications?√
Does child have any handicapping condition?
√
NO abnormality mentioned
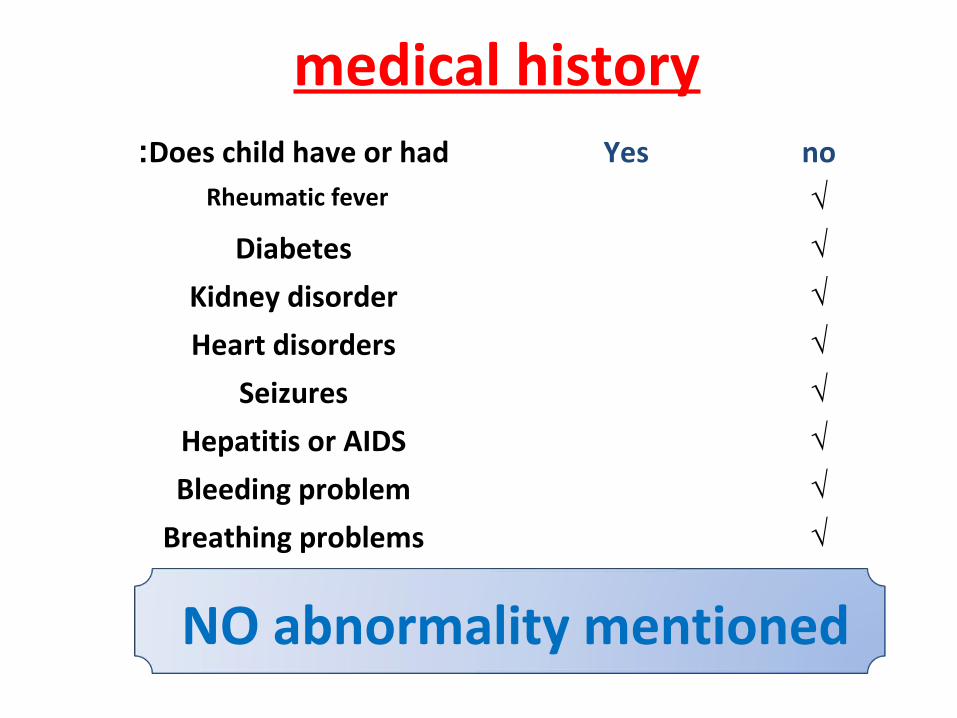
medical historyDoes child have or had: Yes no
Rheumatic fever √
Diabetes √
Kidney disorder √
Heart disorders √
Seizures √
Hepatitis or AIDS √
Bleeding problem √
Breathing problems √
NO abnormality mentioned

Examination of head and neck and extremities
normal abnormalFacial swelling or asymmetry √
TMJ √
Eyes √
Nose √
Lymph nodes √
Fingers and nails √
Lymph node
Submandibular.Unilateral ( right side ).Palpable. Tender.

Intra oral examination
normal abnormalLips √
Labial & buccal mucosa √
gingiva √
tongue √
palate √
inflammation related to #75 RR

Assessment of oral hygiene ( plaque index - Silness and Loe index(
Tooth Surface score
16 Labial 212 Buccal 164 Buccal 336 Lingual 232 Lingual 1
Plaque index score : ( 2+ 1+3 +1 +2 ) I 5 =2
Poor
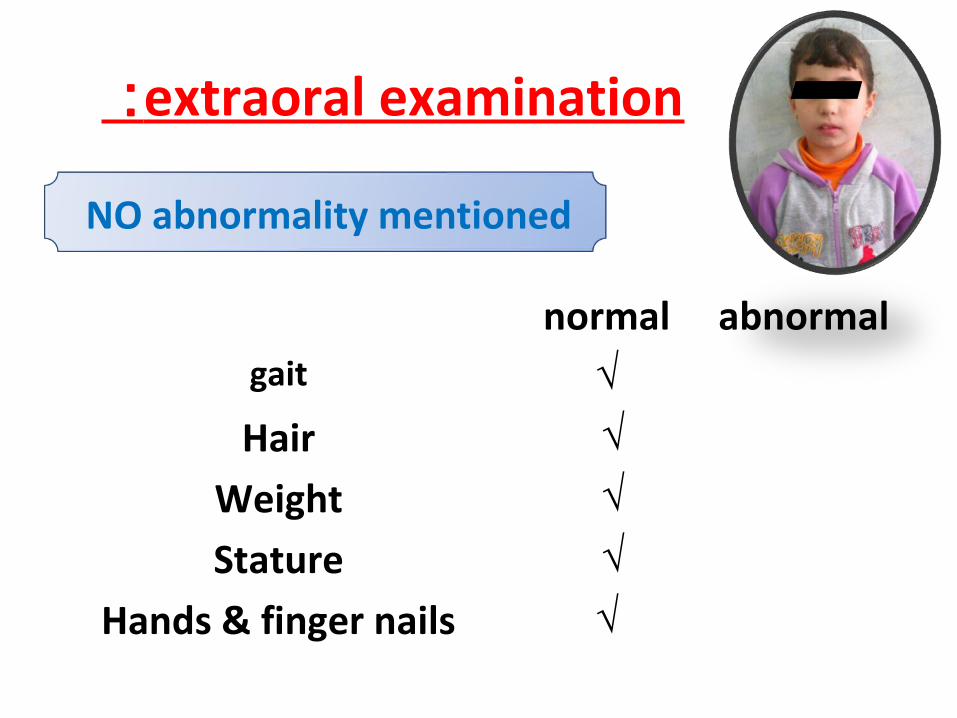
extraoral examination :
normal abnormalgait √
Hair √
Weight √
Stature √
Hands & finger nails √
NO abnormality mentioned

Frontal facial profile
(( symmetrical ((

right
Lateral facial profile( convex (
Left
Left
right
right
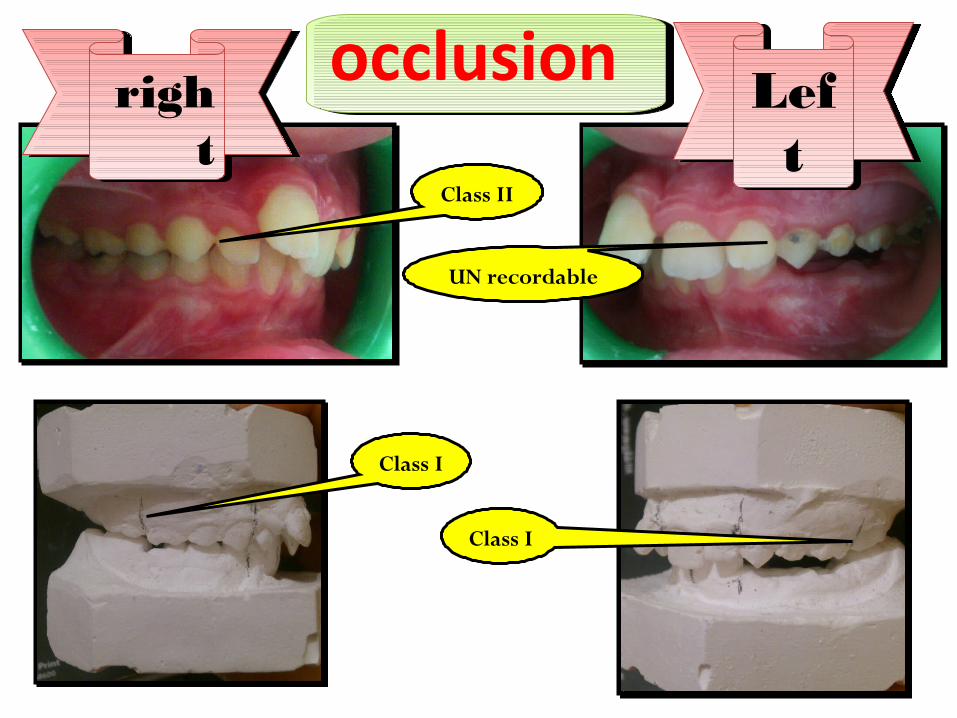
occlusionocclusion
Class II
UN recordable
Class I
Class I

occlusion
midline deviation to word right side .

Over jet & Overbite
Right side at #11 & #41 :Over jet : 9mm due to protrusion of #11.Over bite 50%
Right side at #11 & #41 :Over jet : 9mm due to protrusion of #11.Over bite 50%
Left side at #21 & #31 Over jet : 4mmOver bite 70 %
Left side at #21 & #31 Over jet : 4mmOver bite 70 %
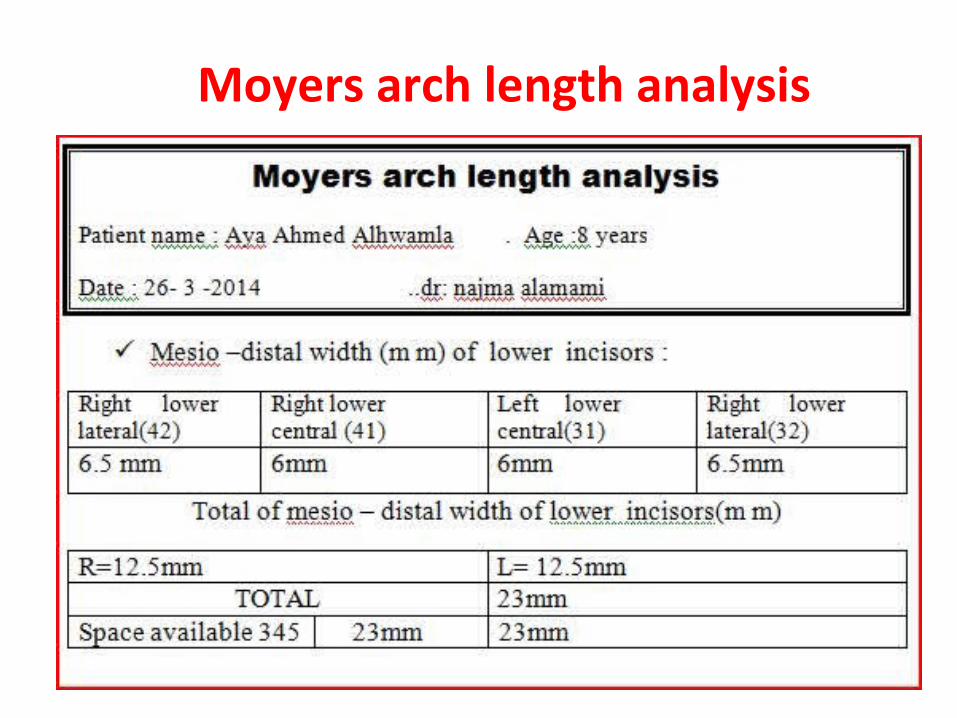
Moyers arch length analysis


Behavioral assessment
cooparative ..according to Frankl’s scale
and Wright’s modifications :
Rating 3 >>> (+ve)

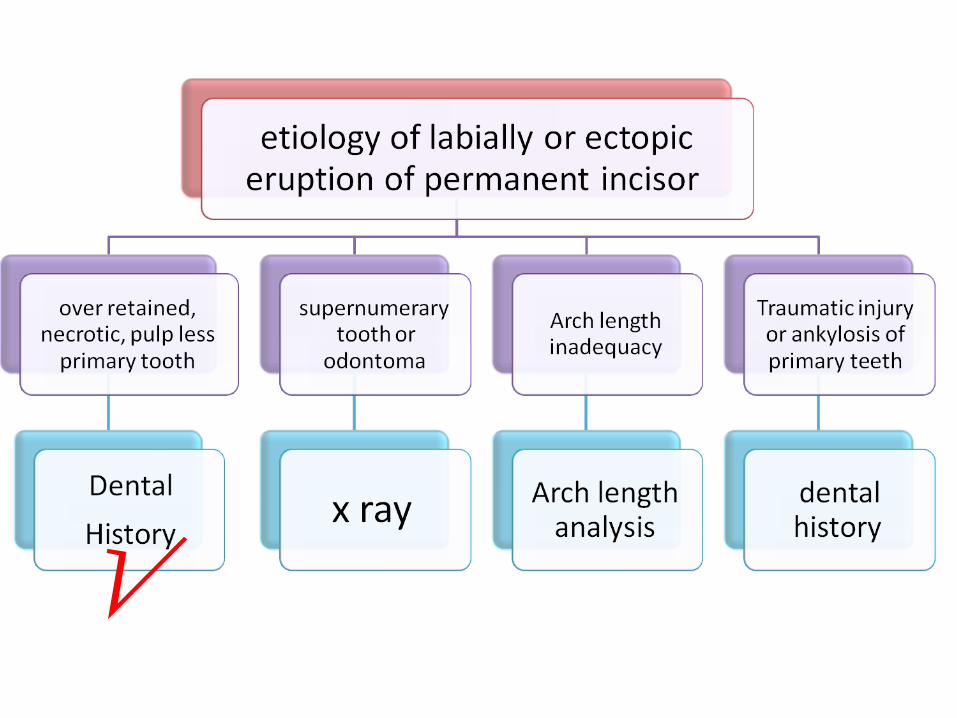
Dental examinationProtrusion #11(Labial or ectopic eruption)
RR
Class I
Class I
Class I Class I
Badly decayed
Multi surfaces caries
Rotation#22
Retroclined#21

Dental examination
Protrusion #11(Labial or ectopic eruption)
Rotation#22
Retroclined#21
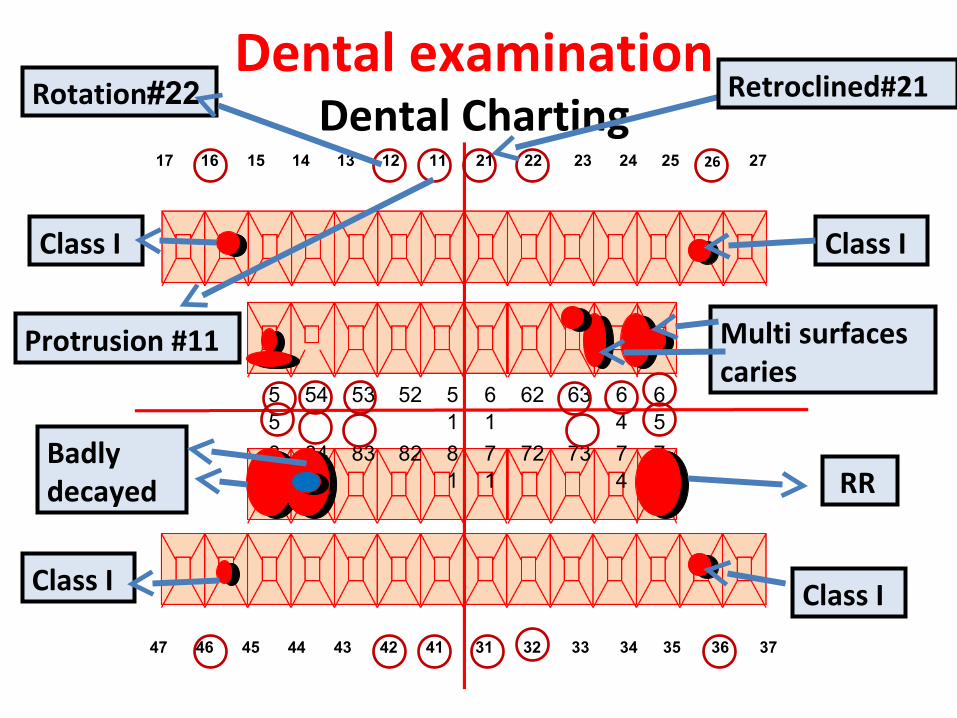
Dental examinationDental Charting
47 46 45 44 43 42 41 31 32 33 34 35 36 37
55
54 53 52 51
61
62 63 64
65
85
84 83 82 81
71
72 73 74
75
17 16 15 14 13 12 11 21 22 23 24 25 26 27
Protrusion #11
RR
Class I Class I
Class I Class I
Badly decayed
Multi surfaces caries
Rotation#22 Retroclined#21

Investigation
)panorama X-rays() per apical X-rays(

Study cast
Investigation


Calorie Range = 1200Calorie Range = 1200


sedentary …. Calorie level: 1200
Food group Recommended amounts
Total diet consumed
Actual deficiency
Grain group 6oz 10 oz +4 oz
Vegetable group 2.5 cups 1cup - 1.5 cup
Fruit group 1.5cup 1 cup - 0.5cup
Milk group 3 cups 1 cup -2 cup
Meat and beans group
5oz 4oz - 1 oz
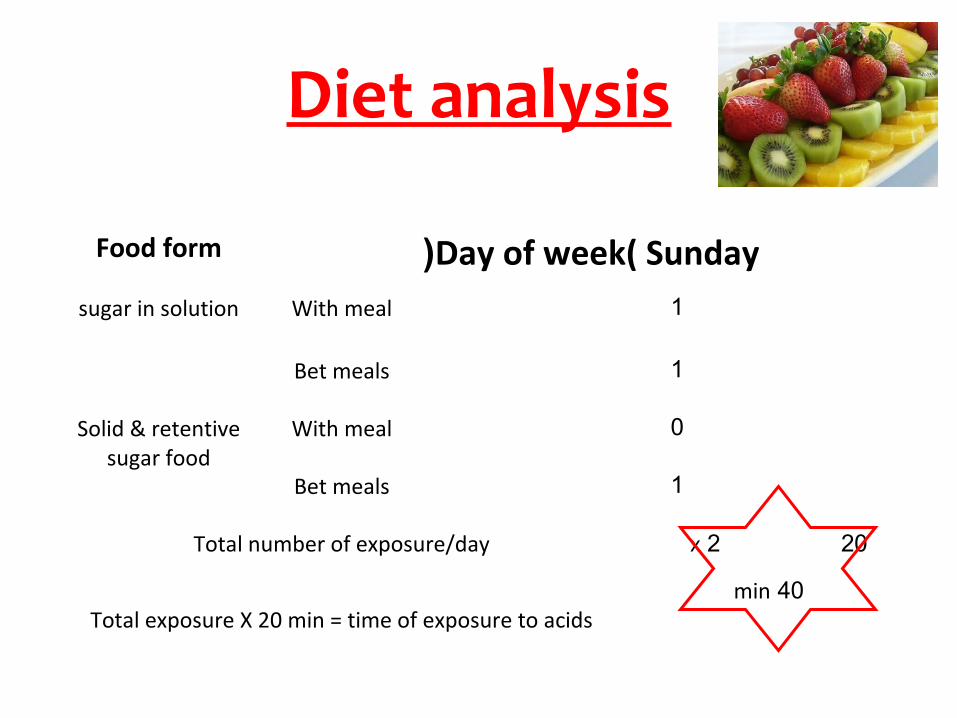
Diet analysis
Food form Day of week( Sunday (sugar in solution With meal 1
Bet meals 1
Solid & retentive sugar food
With meal 0
Bet meals 1
Total number of exposure/day 20 2 x
Total exposure X 20 min = time of exposure to acids40 min
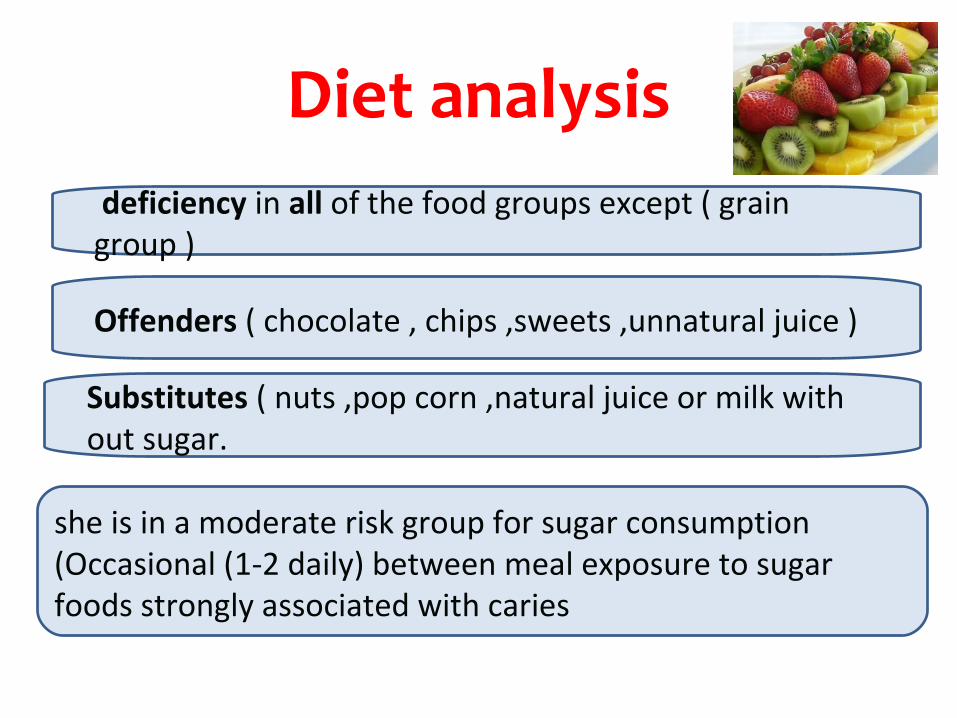
Diet analysis.
deficiency in all of the food groups except ( grain group )
Offenders ( chocolate , chips ,sweets ,unnatural juice )
Substitutes ( nuts ,pop corn ,natural juice or milk with out sugar.
she is in a moderate risk group for sugar consumption (Occasional (1-2 daily) between meal exposure to sugar foods strongly associated with caries

Diagnosis

Problem List
Esthetic problem
Premature loss of primary teeth
Poor dietary habits.
- high caries risk .
- fair oral hygiene
√


1st Visit:1) Medical and dental history.2) Examination of chief complain3) Extra oral and Intra oral Examination.4) Preoperative Photographs and study cast.5) Per apical and panoramic x ray .6) Diagnosis & consultation with orthodontic specialist.7) Oral hygiene instruction .

Factors to be considered before treatment:
Incisor positioning and space available.Stage of eruption.Degree of labial eruption .Axial inclination of the tooth.Class I molar and canine relationships.( cooperation of patient )

Consultation phase.
Orthodontist: consultation( dr. Hanan Ismail) .
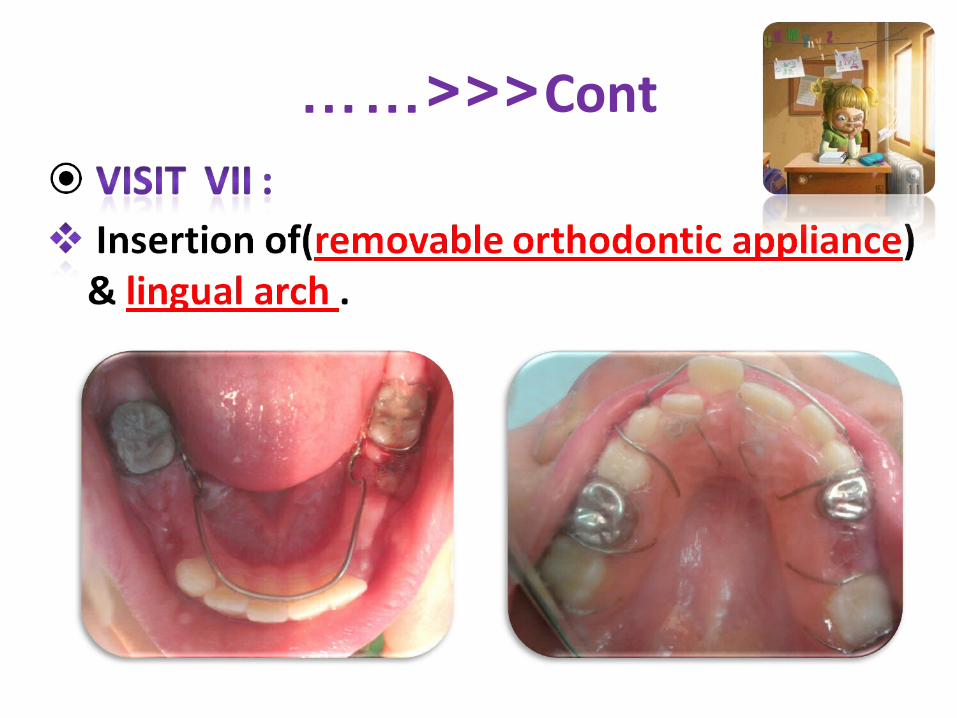
Hawley’s appliance to correction mal alignment with finger spring, Z spring , 2 Adams clasps &active labial bow
Or 2 x 4 technique.

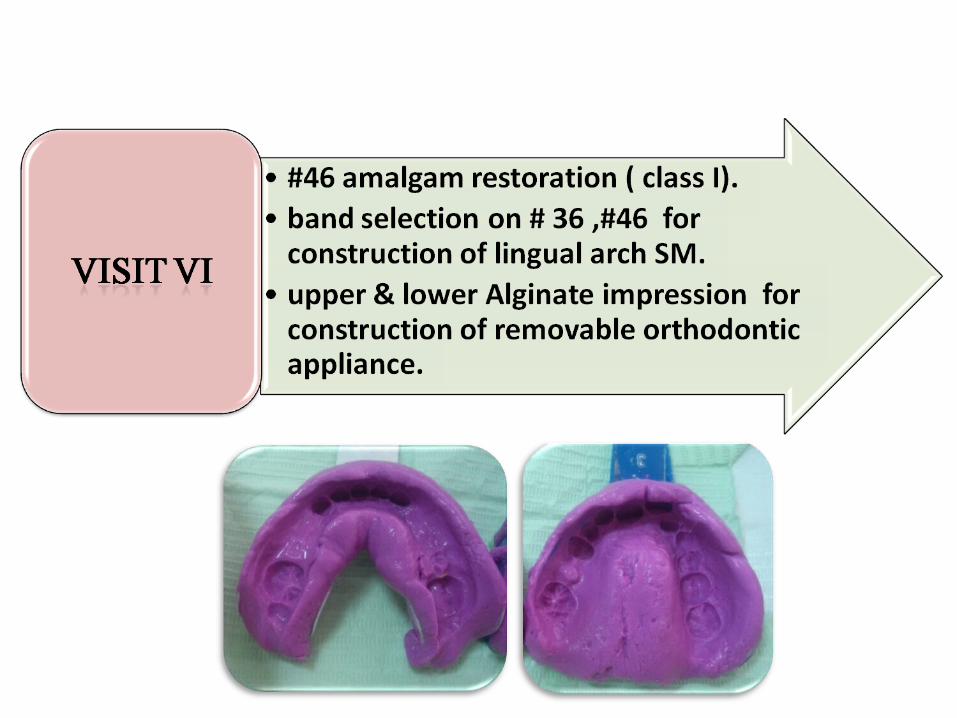
Restorative Phase

Surgical Phase
Cont……<<<

??? Under follow up : DD:hypo plastic # 35.Bifurcation of # 75.Inter septal bone.

Hawley’s appliance
Z spring finger spring,
Adams clasps Adams clasps
&active labial bow

Disadvantages:Patient cooperation.Effective only when there is enough space for aligning the teeth.Technical disadvantages:Need of engaging the spring to the involved tooth or teeth.Difficult adjustment if breakage occurs.

5(Maintenance Phase
Recall weekly to :activation of z spring , finger spring and active
labial bow .Reinforcement of OHI
Brushing technique : roll techinque (Soft brush , pea size Tooth paste – twice daily).
Topical fluoride applicationProfessional :-(1.23% APF gel For 4 minutes every
week during a 4 to 6 week’s period.At home: Fluoridated Toothpaste.



After correction of malocclussion , a removable appliance was used daily as retainer for a 3 months.
Check integrity of all restorations.Check any new lesions or any defect in restoration.Check space maintainer appliances.Check occlusion development.

Before
after

Before
After

Before
After

Before
After

BeforeBefore
After

extraction of remaining root of lower primary molar

Orthodontist: consultation( dr. Hanan Ismail) 2x 4 fixed bracketing technique
as it provides complete control of anterior teeth position.
requires no adjustment by the patient. allows accurate and rapid positioning of the
teeth( lateral incisor ).Correct Medline deviation .Allow bodily and tipping of teeth.
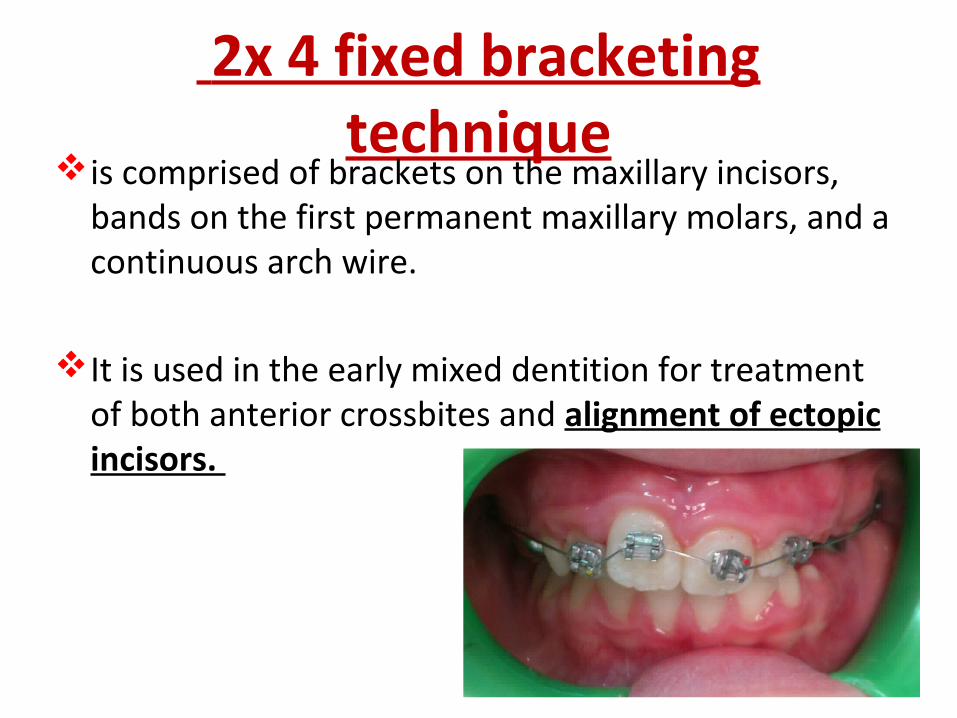
2x 4 fixed bracketing technique
is comprised of brackets on the maxillary incisors, bands on the first permanent maxillary molars, and a continuous arch wire.
It is used in the early mixed dentition for treatment of both anterior crossbites and alignment of ectopic incisors.

brackets
nickelTitanium arch wire
bonding agent
composite

2x 4 fixed bracketing technique
stripping down the contact point of the canine by the use of sand paper strips a little at a time at one weekly intervals.
Oral hygiene instruction

2x 4 fixed bracketing technique
After 2 weeks

2x 4 fixed bracketing technique
After 4 weeks

2x 4 fixed bracketing technique
After 4 weeks
Conclusion
Early diagnosis and successful treatment of
developing malocclusions can have both short-
term and long-term benefits while achieving the
goals of occlusal harmony and function and
dento facial esthetics.
