changes in the qrs complex after aortic valve...
TRANSCRIPT

British Heart Journal, I972, 34, 553-560.
Changes in the QRS complex after aorticvalve replacement
F. Follathl and W. R. Ginks2From the Unit of Clinical Cardiology, Department of Medicine, Royal PostgraduateMedical School, London
The electrocardiograms of 50 patients after isolated aortic valve replacement were examined.Two main types of postoperative QRS changes were found. In I3 patients intraventricularconduction defects developed, predominantly in theform ofa left anterior hemiblock as an isolatedlesion or combined with other focal blocks. The other prominent finding was the appearance ofabnormal Q waves suggesting inferior wall infarction in 8 patients, and anterior wall infarctionin one.
Intraventricular conduction defects were interpreted as evidence of involvement of the con-ducting system during removal of the abnormal valve, whereas uneven myocardial blood flowduring coronary perfusion was thought to be responsiblefor the appearance of abnormal Q waves.The clinical importance of these findings is discussed.
Interest in intraventricular conduction defectshas recently been renewed by Rosenbaumet al. (i969a). They showed the trifascicularcharacter of the conduction system and intro-duced the term 'hemiblock' to describe con-duction disturbances in one ofthe two divisionsof the left bundle. Left anterior hemiblock wasdefined by left axis deviation between -30°and -goo, initial QRS forces directed in-feriorly and to the right, and slight prolonga-tion of the QRS duration by o0o2 sec or less(Rosenbaum et al., I969c). Left posteriorhemiblock was characterized by right axisdeviation to + I200, superiorly directed initialforces, and terminal QRS forces to the rightand inferiorly (Rosenbaum et al., Ig6gb;Castellanos et al., I969).
Focal conduction defects not only changethe QRS complex profoundly, thus obscur-ing the signs of ventricular hypertrophy andmyocardial infarction, but they may be thefirst warning of complete atrioventricularblock which may threaten life. Consideringthe anatomical relation of the bundle of Hisand its main branches to the ventricular sep-tum and the aortic valve (Fig. i), mechanicalinjury to these structures seems likely toReceived 7 June 1971.1 Present address: Department of Cardiac Surgery,Buergerspital, Basle, Switzerland.2 Present address: Department of Medicine, Univer-sity Hospital of San Diego County, 225 West Dickin-son Street, San Diego, California 92I03, U.S.A.
develop during cardiac surgery. Atrioventri-cular block and bundle-branch block arewell-known complications after closure ofventricular septal defects (McGoon, Ongley,and Kirklin, I964; Kulbertus, Coyne, andHallidie-Smith, I969) and the frequentdevelopment of left parietal block after trans-ventricular aortic valvotomy has also beenreported (Samson and Bruce, I962). Aorticvalve replacement, when coronary perfusionand cross-clamping of the aorta presentadditional hazards to the myocardium, seemsto carry an increased risk of intraventricularconduction defects. In recent reports on valvereplacement, the occasional production ofatrioventricular block has been described(Kloster, Bristow and Griswold, I965;Gannon et al., I965) but the incidence ofbundle-branch block or changes of the elec-trical axis were not mentioned.
In this paper, the electrocardiographicchanges were analysed in 50 patients inorder to investigate postoperative abnormali-ties of the QRS complex.
Patients and methodsFifty patients undergoing isolated aortic valvereplacement between 1967 and 1970 were in-cluded in this study (42 Starr-Edwards valves,7 homografts, and i fascia lata repair). The onlycriterion for inclusion in this study was the avail-ability of a 12 lead pre- and postoperative electro-cardiogram. Patients who died in the immediate
on 12 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.6.553 on 1 June 1972. D
ownloaded from

554 Follath and Ginks
FIG. I Schematic representation of theintraventricular conducting system viewedfrom the left ventricle (LV) showing itsrelation to aortic and mitral valves. A=aorta; AMV= anterior mitral leaflet;LAB= anterior division of the left bundle;LPB =posterior division of the left bundle;RB = right bundle-branch (coursing the rightventricular septal surface). (Modified afterHudson, I967.)
postoperative period without having a completeelectrocardiogram recorded were thus excludedfrom the series. There were no late deaths amongthe patients.The electrocardiograms were analysed for
changes of the QRS complex with special empha-sis on the following criteria. (I) Initial ventricularactivation (0o02 sec vector); (2) frontal planeQRS axis; (3) terminal QRS forces; (4) durationof the QRS complex. Serial postoperative electro-cardiograms were reviewed to examine theevolution of the different changes.The routine procedure at valve replacement
consisted of (i) initiation of cardiac bypass andcooling tO 32°C; (2) aorta cross-clamped andopened; (3) perfusion of both coronary arteriesto maintain a pressure of 70-90 mmHg (mean);(4) fibrillation of the heart; (5) excision of theabnormal valve and valve replacement.
Operative data relating to coronary perfusionand aortic clamping, the state of the aortic valve,and the site of calcification and its subvalvularextension, were analysed. The early postoperativecourse was also studied in each patient.
ResultsThe electrocardiographic changes in the 50patients after aortic valve replacement arelisted in the Table.
(a) Preoperative abnormalities In 7 pa-tients there was evidence of pre-existingintraventricular conduction defect. In onethere was complete heart block which re-gressed after operation to right bundle-branch block with left anterior hemiblock.Three patients had complete left bundle-branch block before operation; i developedright bundle-branch block with left anteriorhemiblock after operation, another regressedto left anterior hemiblock and in the otherpatient left bundle-branch block persistedafter operation. Three further patients hadleft anterior hemiblock before operation andthis conduction defect persisted after valvereplacement.
In i patient there were abnormal Q wavesin leads II, III, and aVf before operation.This patient developed changes suggestinganterior wall infarction after operation, thedetails of which are discussed later.
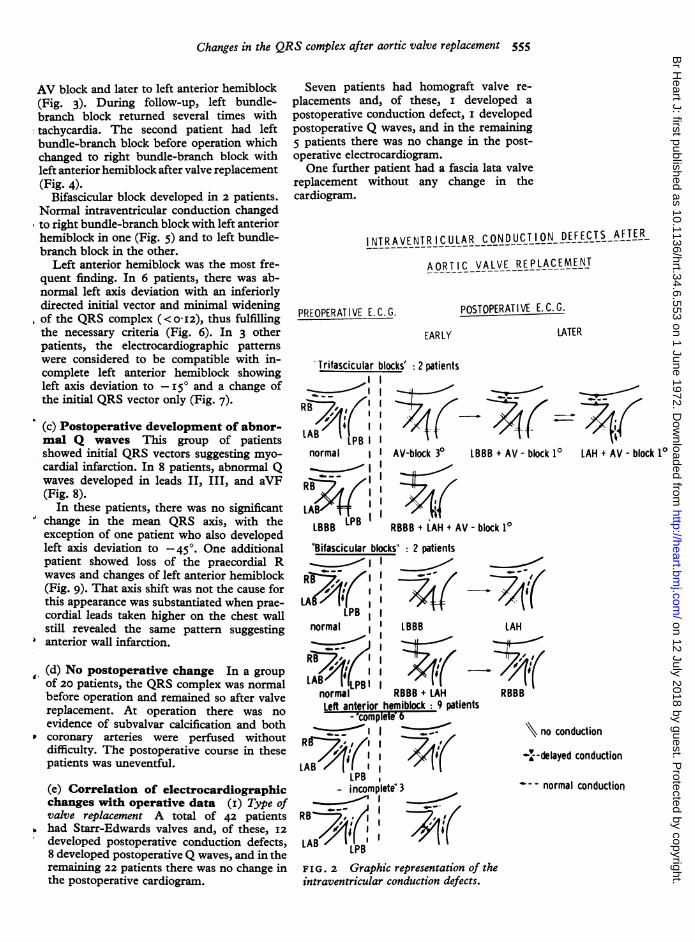
(b) Postoperative development of intra-ventricular conduction defects The dif-ferent types of intraventricular conductiondefect occurring after operation are sche-matically represented in Fig. 2.Damage to all three fascicles (trifascicular
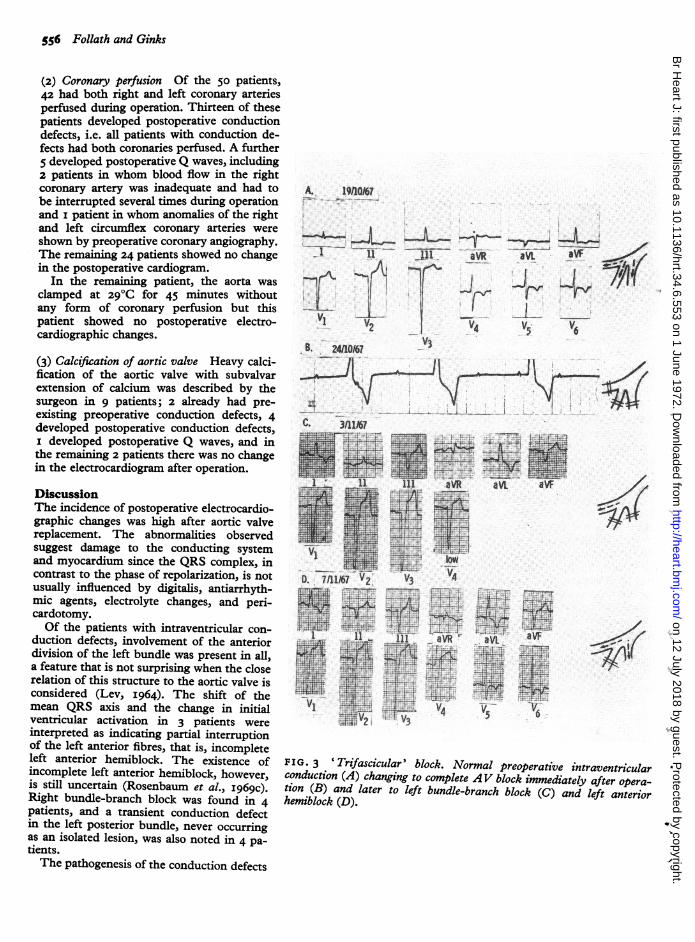
block) was found in 2 patients. The firstdeveloped complete AV block during opera-tion, needing artificial pacing for three days.The electrocardiogram subsequently changedto left bundle-branch block with first degree
TABLE QRS changes in 50 patients afteraortic valvEe replacement
(i) Preoperative pre-existing abnormalities (8 patients)(a) Conduction defects
Trifascicular block IBifascicular block 3Left anterior hemiblock 3
(b) Abnormal Q waves in leads II, III, aVF I
(2) Postoperative changes (22 patients)(a) Conduction defects
Trifascicular blockBifascicular blockLeft anterior hemiblock
(b) Abnormal Q wavesIn leads II, III, aVFIn VI-V4
(3) No postoperative change (20 patients)
22
9
8I
on 12 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.6.553 on 1 June 1972. D
ownloaded from
Changes in the QRS complex after aortic valve replacement 555
AV block and later to left anterior hemiblock(Fig. 3). During follow-up, left bundle-branch block returned several times withtachycardia. The second patient had leftbundle-branch block before operation whichchanged to right bundle-branch block withleft anterior hemiblock after valve replacement(Fig. 4).
Bifascicular block developed in 2 patients.Normal intraventricular conduction changedto right bundle-branch block with left anteriorhemiblock in one (Fig. 5) and to left bundle-branch block in the other.
Left anterior hemiblock was the most fre-quent finding. In 6 patients, there was ab-normal left axis deviation with an inferiorlydirected initial vector and minimal wideningof the QRS complex (<o0I2), thus fulfillingthe necessary criteria (Fig. 6). In 3 otherpatients, the electrocardiographic patternswere considered to be compatible with in-complete left anterior hemiblock showingleft axis deviation to -I5° and a change ofthe initial QRS vector only (Fig. 7).
(c) Postoperative development of abnor-mal Q waves This group of patientsshowed initial QRS vectors suggesting myo-cardial infarction. In 8 patients, abnormal Qwaves developed in leads II, III, and aVF(Fig. 8).
In these patients, there was no significantchange in the mean QRS axis, with theexception of one patient who also developedleft axis deviation to -45'. One additionalpatient showed loss of the praecordial Rwaves and changes of left anterior hemiblock(Fig. 9). That axis shift was not the cause forthis appearance was substantiated when prae-cordial leads taken higher on the chest wallstill revealed the same pattern suggestinganterior wall infarction.
, (d) No postoperative change In a groupof 20 patients, the QRS complex was normalbefore operation and remained so after valvereplacement. At operation there was noevidence of subvalvar calcification and both
* coronary arteries were perfused withoutdifficulty. The postoperative course in thesepatients was uneventful.
(e) Correlation of electrocardiographicchanges with operative data (i) Type ofvalve replacement A total of 42 patientshad Starr-Edwards valves and, of these, I2developed postoperative conduction defects,8 developed postoperative Q waves, and in theremaining 22 patients there was no change inthe postoperative cardiogram.
Seven patients had homograft valve re-placements and, of these, i developed apostoperative conduction defect, i developedpostoperative Q waves, and in the remaining5 patients there was no change in the post-operative electrocardiogram.One further patient had a fascia lata valve
replacement without any change in thecardiogram.
INTRAVENTRICULAR CONDUCTION DEFECTS AFTER
AORTIC VALVE REPLACEMENT
PREOPERATIVE E. C. G.
EAR LY
POSTOPERATIVE E. C. G.
LATER
Trifascicular blocks" : 2 patientsII
RBI
LAB LPBInormal I
I1
RBBB BIILAB?+ I
LBBBLP
AV-block 30 LBBB + AV - block 10
RBBB + lAH + AV- block 10"Bifascicular blocks" 2 patients
B I
U\t- X
normal I LBBB
LAB"r IPBi Inormal RBBB + LAHLeft anterior hemiblock 9 patients
-"completeOb
LAB '-'iiLPB
- incomplete' 3
LAB LPB
FIG. 2 Graphic representation of theintraventricular conduction defects.
LAH +AV- block 10
LAH
RBBB
N no conduction
-'--delayed conduction
- - normal conduction
-0- --II
41- 4
on 12 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.6.553 on 1 June 1972. D
ownloaded from
556 Follath and Ginks
(2) Coronary perfusion Of the 50 patients,42 had both right and left coronary arteriesperfused during operation. Thirteen of thesepatients developed postoperative conductiondefects, i.e. all patients with conduction de-fects had both coronaries perfused. A further5 developed postoperative Q waves, including2 patients in whom blood flow in the rightcoronary artery was inadequate and had tobe interrupted several times during operationand i patient in whom anomalies of the rightand left circumflex coronary arteries wereshown by preoperative coronary angiography.The remaining 24 patients showed no changein the postoperative cardiogram.
In the remaining patient, the aorta wasclamped at 29gC for 45 minutes withoutany form of coronary perfusion but thispatient showed no postoperative electro-cardiographic changes.
(3) Calcification of aortic valve Heavy calci-fication of the aortic valve with subvalvarextension of calcium was described by thesurgeon in 9 patients; 2 already had pre-existing preoperative conduction defects, 4developed postoperative conduction defects,I developed postoperative Q waves, and inthe remaining 2 patients there was no changein the electrocardiogram after operation.
DiscussionThe incidence of postoperative electrocardio-graphic changes was high after aortic valvereplacement. The abnormalities observedsuggest damage to the conducting systemand myocardium since the QRS complex, incontrast to the phase of repolarization, is notusually influenced by digitalis, antiarrhyth-mic agents, electrolyte changes, and peri-cardotomy.Of the patients with intraventricular con-
duction defects, involvement of the anteriordivision of the left bundle was present in all,a feature that is not surprising when the closerelation of this structure to the aortic valve isconsidered (Lev, I964). The shift of themean QRS axis and the change in initialventricular activation in 3 patients wereinterpreted as indicating partial interruptionof the left anterior fibres, that is, incompleteleft anterior hemiblock. The existence ofincomplete left anterior hemiblock, however,is still uncertain (Rosenbaum et al., I969c).Right bundle-branch block was found in 4patients, and a transient conduction defectin the left posterior bundle, never occurringas an isolated lesion, was also noted in 4 pa-tients.The pathogenesis of the conduction defects
A. 19/1067
V1 V4~~~~~~~1
.~~~~~~~~~~~~~''
B. 2411067
.A
C. 3/11/67
4+t
11 11 aVi aV'..a. aVF_:s | = ;~~~~~~~~~~~~~4B. 7 21167 2 V3
X<1+ il ~~il- a-VR- a- a
M:X....zA '@ giS~~71~~~~~~~Vtt[-r-:- -i & 4:.
V3
FIG. 3 'Trifascicular' block. Normal preoperative intraventricularconduction (A) changing to complete AV block immediately after opera-tion (B) and later to left bundle-branch block (C) and left anteriorhemiblock (D).
on 12 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.6.553 on 1 June 1972. D
ownloaded from

Changes in the QRS complex after aortic valve replacement 557
Ill.-..H
4eI.V3|s
*.. ... -..
aVR
re
aV
*jlit..SCV^ .
50
§ .
I... I
. ....;
Vi
aVR aVI aVF
V6
v5
FIG . 4 ' Trifascicular' involvement of the conduction system. Preoperative left bundle-branchblock (A) changing to right bundle-branch block and left anterior hemiblock after valve replace-ment (B).
is probably due to involvement of the con-
ducting system during removal of the ab-normal valve. Haemorrhagic lesions andnecrosis of the atrioventricular conductingsystem have been observed not infrequentlyafter aortic valve replacement (Hudson, I967;Niles and Sandilands, I969). Whether con-duction defects are more likely to developafter Starr-Edwards valve insertion than afterhomograft valve replacement is uncertain,since the two procedures are not equallyrepresented in this series.The second prominent finding was the
development of abnormal Q waves suggestinginferior infarction in 8 patients, and anteriorwall infarction in i patient. Attention hasbeen drawn to the association between thesechanges and the difficulties of coronaryartery perfusion. An alternative explanation,however, which might account for the ap-pearance of Q waves in the inferior leads is aconduction disturbance in the left posteriorbundle. Experimental dissection of the leftposterior bundle in primates produces an
electrocardiographic pattern resembling in-ferior wall infarction (Watt and Pruitt, I969).
Left posterior hemiblock has also been shownclinically to cause a shift of the initial QRSvector superiorly and therefore Q waves inleads II, III, and aVF (Rosenbaum et al.,I969b). Recently the spontaneous develop-ment of wide slurred Q waves in the inferiorleads was described in patients with aorticvalve disease without any evidence of coro-nary artery disease (Warembourg et al.,I970). These authors suggested that the re-gurgitant jet of aortic incompetence wasresponsible for the abnormal Q waves bycausing endocardial fibrosis in the area ofthe left posterior bundle. One of the acceptedcriteria of left posterior hemiblock is, how-ever, a rightward shift of the mean frontalplane QRS axis, which is not a feature in ourpatients with inferior Q waves.In conclusion, the frequency of intraventri-
cular conduction defects after aortic valvereplacement emphasizes the important ana-
tomical relation between the conductingsystem and the aortic valve cusps. In addi-tion, the development and variability in thetypes of intraventricular blocks lend furthersupport to the concept of trifascicular intra-
L+.. ... v... 4
25.13. :8
A.
..¶r.I ..
E>1.VI
B t ,
Vi
I
on 12 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.6.553 on 1 June 1972. D
ownloaded from

558 Follath and Ginks
...;a" "-oF%
ti .: .. ...:- 4--,. ....Q .a.p-; j K..
i; V t2jt- >+§'1@{t..A.i-.:.'S
A s4._ I ... w. .
....._. .̂.. ^.........I
Px-GSi S_S, Z..tnj....tit"' :47., ^
(a
-4
.4
3it"
-(4
'-0
b.t
OL'3t s:
s44 o kt~~~~~'a
'ati}
~t.QE ^ -
S~~~- '3 X *
.30 %CNw~~~~1',3
-X 0o3z4 '.
'3t
'a tes
O3
'0 0t'
-4
on 12 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.6.553 on 1 June 1972. D
ownloaded from

Changes in the QRS complex after aortic valve replacement 559
W#XgRts4 uJdgttuw4L 4
' i Fe b: wE5. t: v
1 tlmnntltt4
11f1 ONS*J.l4 MET
Mr
Ii )1%.I
.zt:tt:C-
Ih4
00
ad
0toY
Z0-a i.t:ot;:'- *, +
0 CN >
I
0- XX l0 ii_
..T.-i.. "'
,
t. ...4 -.1-
on 12 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.6.553 on 1 June 1972. D
ownloaded from

560 Follath and Ginks
ventricular conduction. The clinical impor-tance of these conduction defects is not clear.With the exception of the patient with tran-sient third degree AV block, no haemo-dynamic complications were seen and thepostoperative course was no different fromthose without electrocardiographic changes.Nevertheless, it is possible that there is anincreased risk of developing complete AVblock in later life (Lasser, Haft, and Fried-berg, I968).At present, the differentiation between
inferior wall infarction and left posteriorhemiblock awaits further study. In view ofthe difficulties of coronary artery perfusionin our patients, myocardial necrosis seemsthe most likely explanation for the appear-ance of Q waves in the inferior leads.
W. H.
2412170
A 111~~~~~~~~~~~~~~1aV aVWaV_~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.H
V,1 2 V3 V4 V5 .
We are indebted to Professor J. F. Goodwin forhelpful criticism and advice, and to Mr. W. P.Cleland and Professor H. H. Bentall who per-formed the operations.
ReferencesCastellanos, A., Jr., Maytin, O., Arcebal, A. G., and
Lemberg, L. (I969). Alternating and co-existingblock in the divisions of the left bundle branch.Diseases of the Chest, 56, I03.
Gannon, P. G., Sellers, R. D., Kanjuh, V. I., Edwards,J. E., and Lillehei, C. W. (I965). Complete heartblock following replacement of the aortic valve.Circulation, 33-34, Suppl. I, I52.
Hudson, R. E. B. (I967). Surgical pathology of theconducting system of the heart. British HeartJournal, 29, 646.
Kloster, F. E., Bristow, J. D., and Griswold, H. E.(I965). Medical problems in mitral and multiplevalve replacement. Progress in CardiovascularDiseases, 7, 504.
Kulbertus, H. E., Coyne, J. J., and Hallidie-Smith,K. A. (I969). Conduction disturbances before andafter surgical closure of ventricular septal defect.American Heart Journal, 77, I23.
Lasser, R. P., Haft, J. I., and Friedberg, C. K. (I968).Relationship of right bundle-branch block andmarked left axis deviation (with left parietal orperi-infarction block) to complete heart block andsyncope. Circulation, 37, 429.
Lev, M. (I964). Anatomic basis for atrioventricularblock. American Journal of Medicine, 37, 742.
McGoon, D. C., Ongley, P. A., and Kirklin, J. W.(I964). Surgical heart block. American Journal ofMedicine, 37, 749.
Niles, N. R., and Sandilands, J. R. (I969). Pathologyof heart valve replacement surgery. Diseases of theChest, 56, 373.
Rosenbaum, M. B., Elizari, M. V., Lazzari, J. O.,Nau, G. J., Levi, R. J., and Halpern, M. S.(I969a). Intraventricular trifascicular blocks.Review of the literature and classification. Ameri-can Heart journal, 78, 450.
Rosenbaum, M. B., Elizari, M. V., Lazzari, J. O.,Nau, G. J., Levi, R. J., and Halpern, M. S.(I969b). Intraventricular trifascicular blocks. Thesyndrome of right bundle-branch block withintermittent left anterior and posterior hemiblock.American Heart Journal, 78, 306.
2D40.1..uk -^ . -- -.... .X. . .6...
_*
=1 111 aVRt
a - ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~..aVI aWF
mYF mWt z_','-F-F --
'Ii~~~~~~~~~~~~~~~~~~~~~~~~~~~EEV1 V2 V3 V4 V5
FIG. 9 Postoperative anterior wall infarction with poor R wave pro.gression in Vi-V3.
Rosenbaum, M. B., Elizari, M. V., Levi, R. J., Nau,G. J., Pisani, N., Lazzari, J. 0., and Halpern, M. S.(1969c). Five cases of intermittent left anteriorhemiblock. American J7ournal of Cardiology, 24, I.-
Samson, W. E., and Bruce, R. A. (1962). Left ventri-cular parietal block produced by transventricularaortic commissurotomy. American Heart Journal,63, 41.
Warembourg, H., Pauchant, M., Thery, Cl., Lekieffre,J., Ducloux, G., and Gosselin, B. (I970). Blocintraventriculaire posterieur au cours de l'insuffi-sance aortique. Archives des Maladies du Cawu etdes Vaisseaux, 63, 408.
Wart, T. B., and Pruirt, R. D. (I969). Left posteriorfascicular block in canine and primate hearts.Circulation, 40, 677.
Requests for reprints to Dr. W. R. Ginks,Departrent of Medicine, University Hospital ofSan Diego County, 225 West Dickinson Street,San Diego, California 92I3, U.S.A.
...... e
.1.
on 12 July 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.34.6.553 on 1 June 1972. D
ownloaded from