chapter 15 fluid and acid-base balance - the …biology/classes/255/chapter15.pdffluid balance water...
TRANSCRIPT

Chapter 15Chapter 15
Fluid and AcidFluid and Acid--Base BalanceBase Balance
V. Pag. 559-589
VI. Pag. 547-577

Fluid BalanceWater constitutes ~60% of body weight.
All cells and tissues are surrounded by an aqueous environment. Most biochemical reactions inside the cell occurs in the cytosol.
Body systemsmaintain homeostasis
Homeostasis
Cells make up body systems
Fluid balance is critical for maintaining bodyhomeostasis

Fluid BalanceDisruption of normal fluid balance can disrupt cell function
No net movement of water
Water tends to move in causing cell swelling
Water tends to move out of cellcausing cell shrinking

Water Distribution
In the human organism, water is distributed between:
1) The intracellular fluid(~62%)
2) The extracellular fluid that consist of plasma(6.6%) and interstitial fluid (26.4%)Slide 30
VesselsHeart(pump)
Tissues
Cells
Circulating plasma(20% of extracellular fluid)
Interstitial fluid(80% of extracellular fluid)
Figure 10.21Page 364
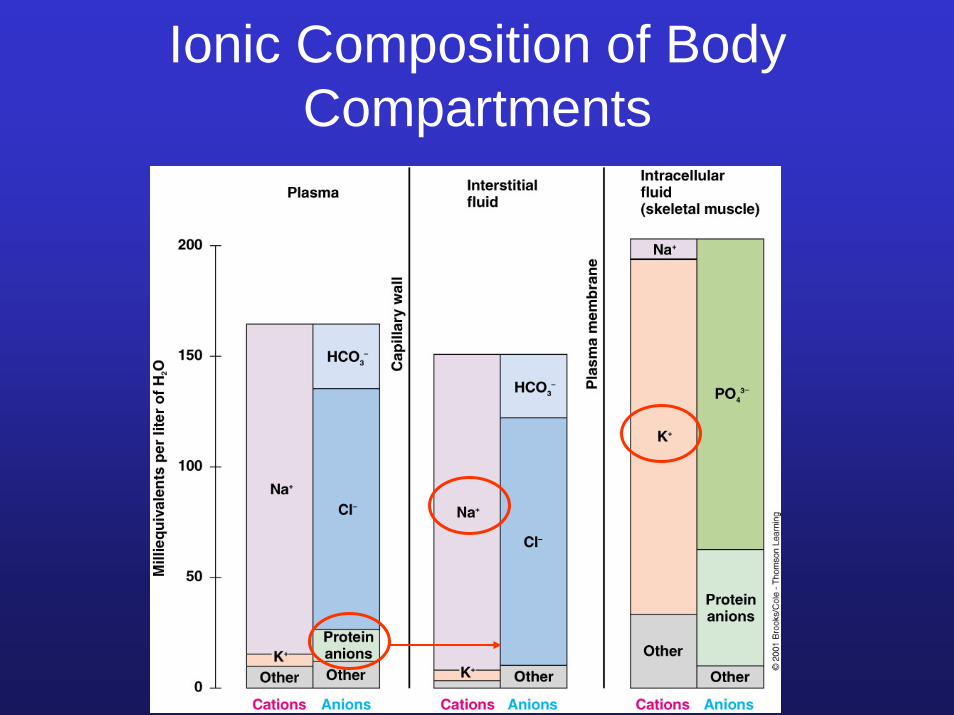
Ionic Composition of Body Compartments
Ionic Composition of Body Compartments
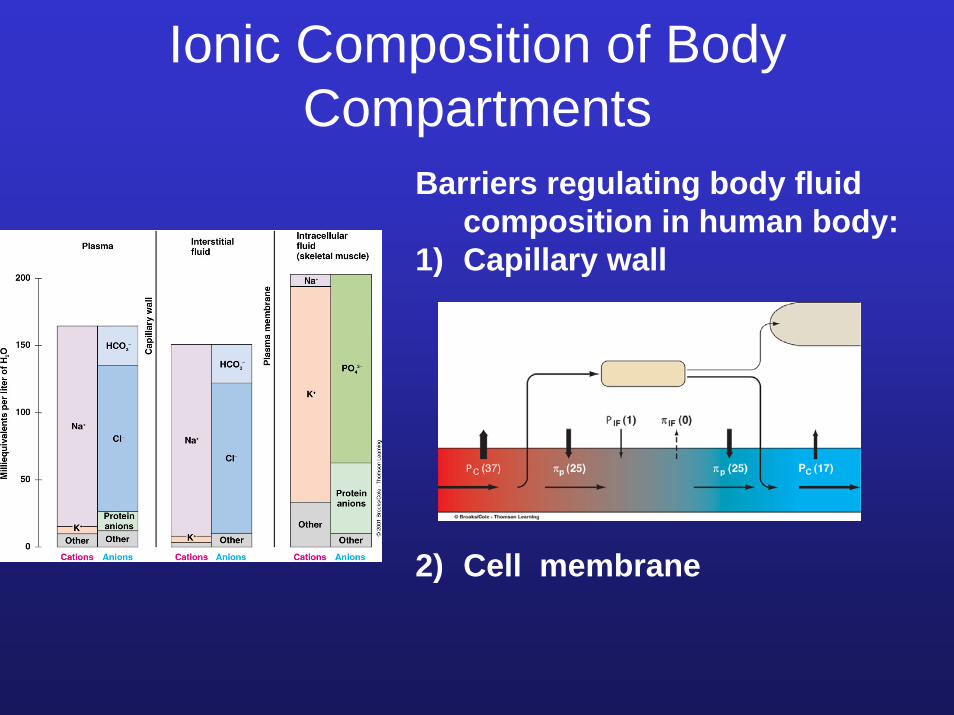
Barriers regulating body fluid composition in human body:
1) Capillary wall
2) Cell membrane

Fluid Balance
Fluid balance is maintained by regulating:
1) Extracellular fluid volume. Effect on blood pressure
2) Osmolarity: measure of solutes dissolved in aqueous medium. Effect on cell volume
Slide 30
VesselsHeart(pump)
Tissues
Cells
Circulating plasma(20% of extracellular fluid)
Interstitial fluid(80% of extracellular fluid)
Figure 10.21Page 364

Fluid BalanceDisruption of normal fluid balance can disrupt cell function
No net movement of water
Water tends to move in causing cell swelling
Water tends to move out of cellcausing cell shrinking

Regulation of Extracellular Fluid Volume is Important
in the Regulation of Blood PressureReduction in EC volume causes a fall in blood pressure
Short term regulation of blood pressure:
1) Baroreceptor reflex , and
2) Fluid shift between plasma and intestinal fluid
Long term regulation of blood pressure:
1) Control of Na+ ions filtration and reabsorption by the renin-angiotensin-aldosterone system
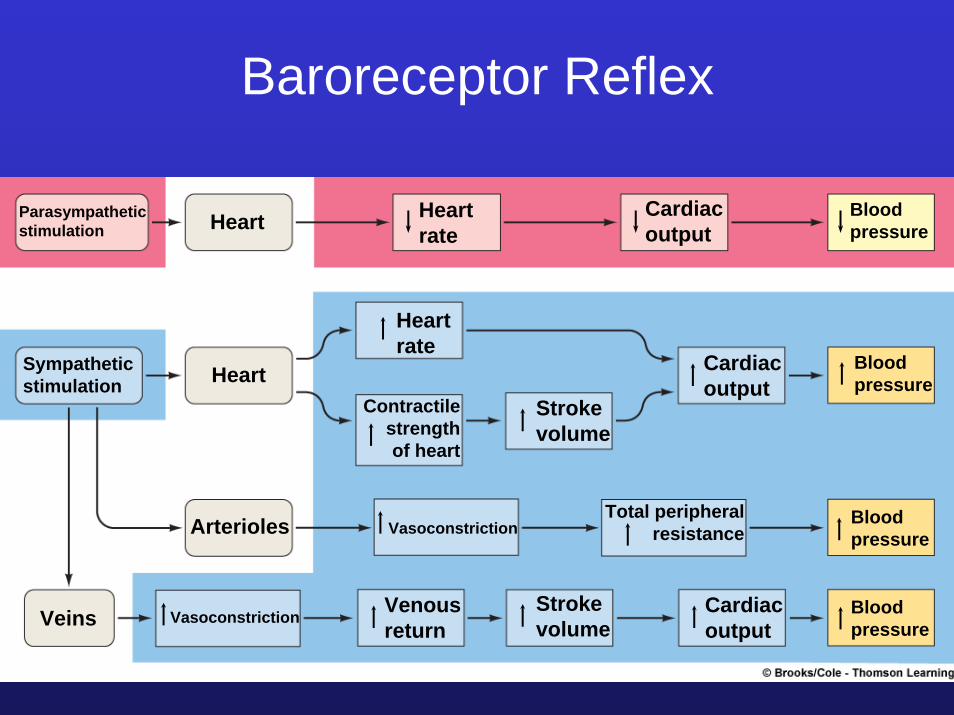
Parasympatheticstimulation Heart Heart
rateCardiacoutput
Bloodpressure
Sympatheticstimulation Heart
Heartrate
Contractilestrengthof heart
Strokevolume
Cardiacoutput
Cardiacoutput
Bloodpressure
Bloodpressure
Bloodpressure
Total peripheralresistance
Strokevolume
VenousreturnVeins Vasoconstriction
VasoconstrictionArterioles
Baroreceptor Reflex
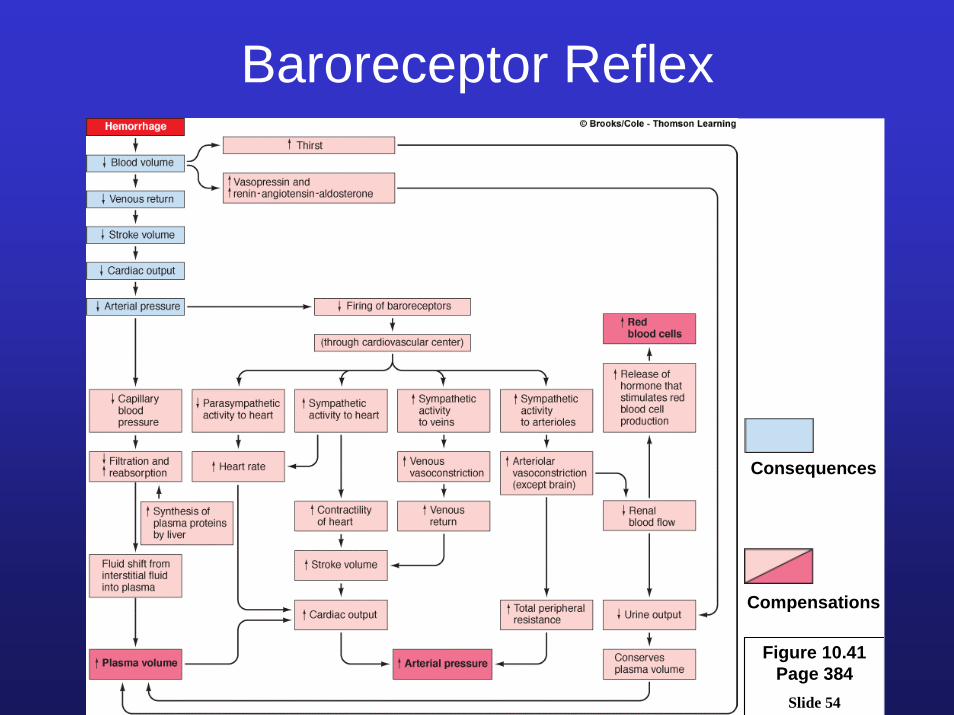
Baroreceptor Reflex
Slide 54
Figure 10.41 Page 384
Consequences
Compensations
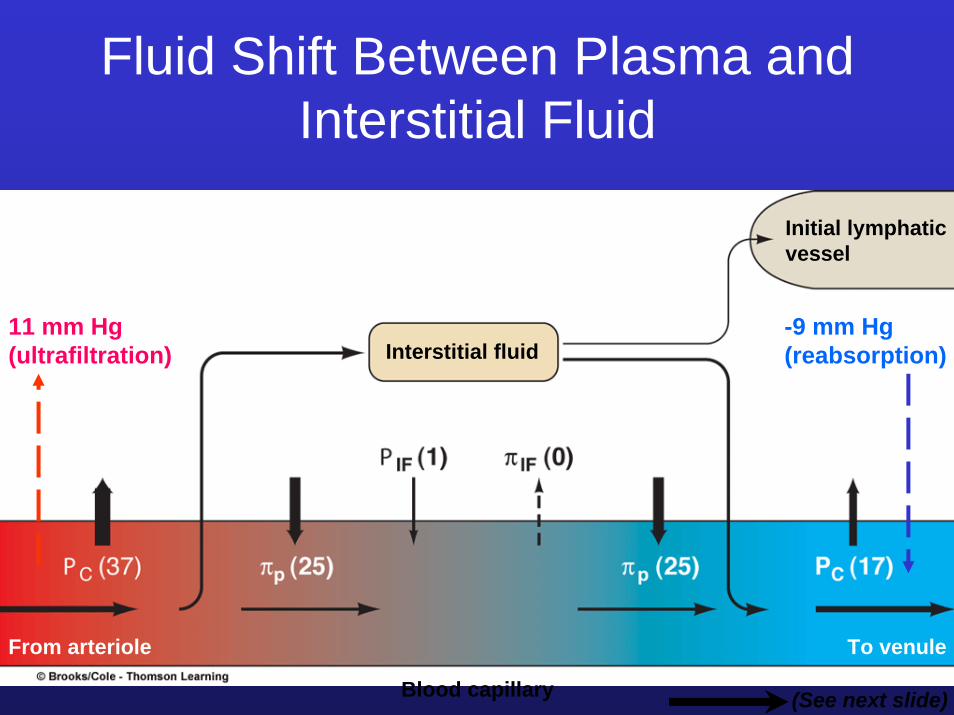
11 mm Hg(ultrafiltration) Interstitial fluid
From arteriole To venule
-9 mm Hg(reabsorption)
Initial lymphaticvessel
Blood capillary (See next slide)
Fluid Shift Between Plasma and Interstitial Fluid

Long Term Control of Blood Pressure: Na+ Control
1) Regulation of Na+ filtration in glomerulus by GFR2) Regulation of Na+ reabsorption by the renin-angiotensin-
aldosterone system

Long Term Control of Blood Pressure: Na+ Control
Decreased blood pressure or Na+ load
Decreased Na+
filtration rate
Decreased blood pressure or Na+
load
Increased renin production and insertion of Na+ channels in luminal membrane and Na+/K+
ATPase in basolateral membrane

Juxtaglomerular ApparatusMacula dense cells can detect changes in flow rate and
release vasoactive substances (vasoconstrictors and vasodilators) that alter capillary blood flow.
Granular cells sense changes in pressure and release renin.
Sese chages in blood pressure, NaCl volume.Secrete renin
Sense changes in flow rate.
Secrete vasoactive Substances (endothelin)
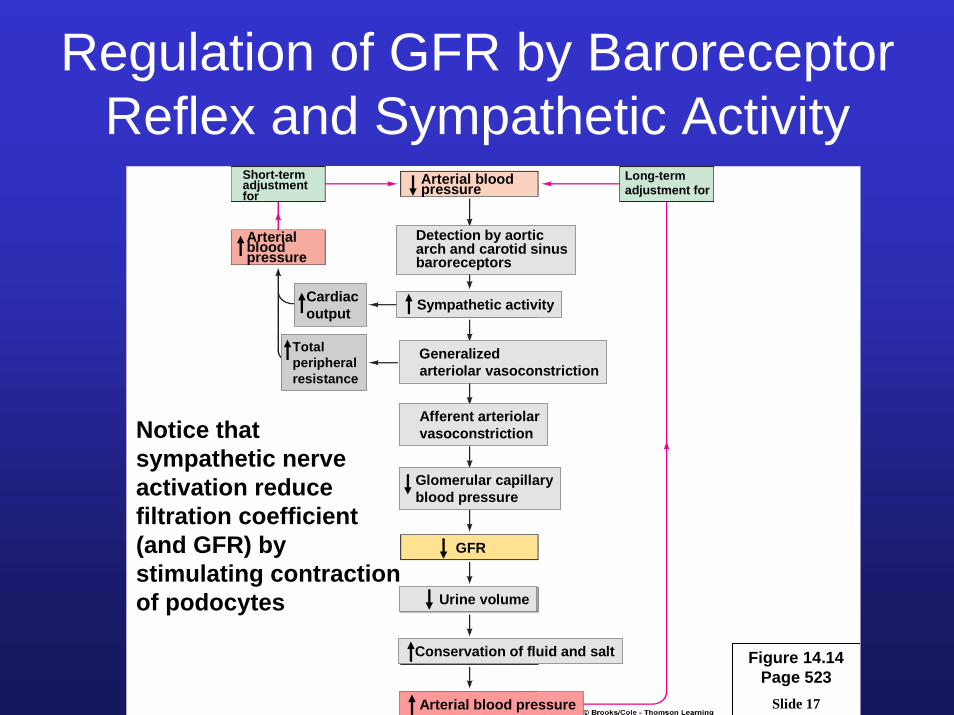
Regulation of GFR by Baroreceptor Reflex and Sympathetic Activity
The idea here is toincrease blood volume when drop in blood pressure occurs
Slide 17
Short-termadjustment for
Arterial blood pressure
Long-termadjustment for
Arterialblood pressure
Detection by aorticarch and carotid sinusbaroreceptors
Cardiacoutput
Totalperipheralresistance
Sympathetic activity
Generalizedarteriolar vasoconstriction
Afferent arteriolarvasoconstriction
Glomerular capillaryblood pressure
GFR
Urine volume
Conservation of fluid and salt
Arterial blood pressure
Figure 14.14Page 523
Notice that sympathetic nerve activation reduce filtration coefficient (and GFR) by stimulating contraction of podocytes

Renin-Angiotensin-Aldosterone Regulates Na+ Reabsorption
Aldosterone acting on distal/collecting tubules, drives the insertion of new Na+ channels and Na+/K+ ATPases in tubular cells
Slide 23
Figure 14.19Page 529
NaCl / ECF volume /
Arterial blood pressure
Liver Kidney Lungs Adrenalcortex Kidney
H2Oconserved
Na+ (and CI–)osmotically holdmore H2O in ECF
Na+ (and CI–)conserved
Na+ reabsorptionby kidney tubules( CI–
reabsorptionfollows passively)
Vasopressin Thirst Arteriolarvasoconstriction
H2O reabsorptionby kidney tubules
Fluid intake
ReninAngiotensin-convertingenzyme
Angiotensinogen Angiotensin I Angiotensin II Aldosterone

Aldosterone FunctionAldosterone stimulates Na+ reabsorption by promoting
the insertion of new Na+ channels in the luminal membrane and additional Na+/K+ ATPase carriers in the
basolateral membrane
© Brooks/Cole - Thomson Learning
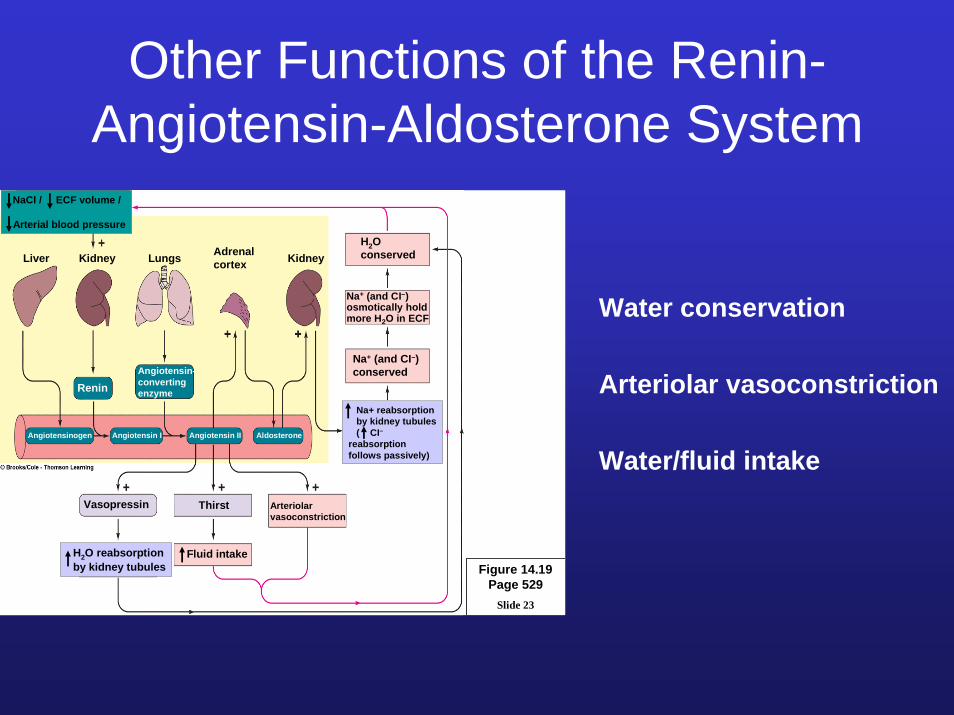
Other Functions of the Renin-Angiotensin-Aldosterone System
Slide 23
Figure 14.19Page 529
NaCl / ECF volume /
Arterial blood pressure
Liver Kidney Lungs Adrenalcortex Kidney
H2Oconserved
Na+ (and CI–)osmotically holdmore H2O in ECF
Na+ (and CI–)conserved
Na+ reabsorptionby kidney tubules( CI–
reabsorptionfollows passively)
Vasopressin Thirst Arteriolarvasoconstriction
H2O reabsorptionby kidney tubules
Fluid intake
ReninAngiotensin-convertingenzyme
Angiotensinogen Angiotensin I Angiotensin II Aldosterone
Water conservation
Arteriolar vasoconstriction
Water/fluid intake
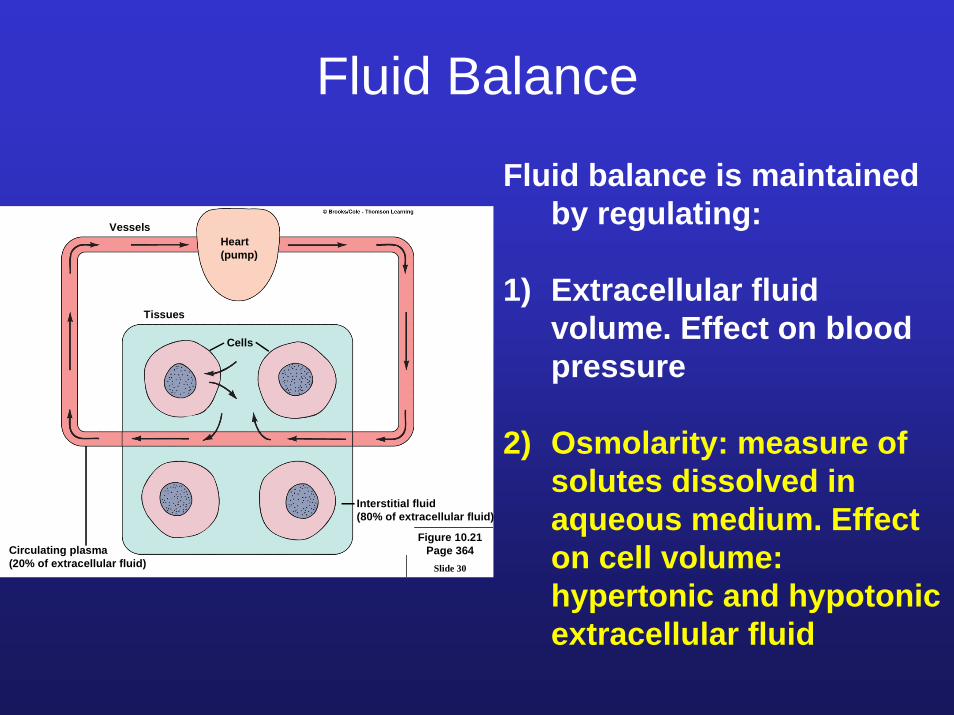
Fluid Balance
Fluid balance is maintained by regulating:
1) Extracellular fluid volume. Effect on blood pressure
2) Osmolarity: measure of solutes dissolved in aqueous medium. Effect on cell volume: hypertonic and hypotonic extracellular fluid
Slide 30
VesselsHeart(pump)
Tissues
Cells
Circulating plasma(20% of extracellular fluid)
Interstitial fluid(80% of extracellular fluid)
Figure 10.21Page 364

Osmolarity-Induced Changes in Cell Volume
No net movement of water
Water tends to move in causing cell swelling
Water tends to move out of cell. Cell shrinking

Ionic Composition of Body Compartments
Between plasma andinterstitial fluid, differences in osmolarity are due tounequal distribution of plasma proteins
Between interstitial fluidand intracellular fluid differences in osmolarity are due to differences inionic composition

Regulation of Osmolarity in Human Body
Osmolarity can be regulated by:
1) Water intake (angiotensin-thirst)
2) Water output (vasopressin effect on kidneys)
Slide 30
VesselsHeart(pump)
Tissues
Cells
Circulating plasma(20% of extracellular fluid)
Interstitial fluid(80% of extracellular fluid)
Figure 10.21Page 364

Vasopressin Release Controls Water Secretion and Osmolarity

Fromproximaltubule
Filtrate has concentrationof 100 mosm/liter as itenters distal andcollecting tubules
In the face of water deficit: vasopressin stimulates water movement out of distal/collecting tubules
Collectingtubule
Loop ofHenle
Medulla
Cortex
Distal tubule
Concentration ofurine may be upto 1,200 mosm/literas it leavescollecting tubule
= permeability to H2Oincreased by vasopressin
= passive diffusion of H2O
= active transport of NaCl
= portions of tubule impermeable to H2O
*
*
*
*

Figure 15.4Page 569
ECF volume
Arterialblood pressureOsmolarity
Hypothalamicosmoreceptors(dominant factorcontrolling thirst andvasopressin secretion)
Left atrial volume receptors(important only in large changes in plasmavolume/arterial pressure)
Hypothalamic neurons
Thirst Vasopressin
Arteriolarvasoconstriction
H2O intake H2O permeabilityof distal and collecting tubules
H2O reabsorption
Urine output
Plasma osmolarity Plasma volume

Angiotensin Regulates Thirst AND Water Intake
Slide 23
Figure 14.19Page 529
NaCl / ECF volume /
Arterial blood pressure
Liver Kidney Lungs Adrenalcortex Kidney
H2Oconserved
Na+ (and CI–)osmotically holdmore H2O in ECF
Na+ (and CI–)conserved
Na+ reabsorptionby kidney tubules( CI–
reabsorptionfollows passively)
Vasopressin Thirst Arteriolarvasoconstriction
H2O reabsorptionby kidney tubules
Fluid intake
ReninAngiotensin-convertingenzyme
Angiotensinogen Angiotensin I Angiotensin II Aldosterone
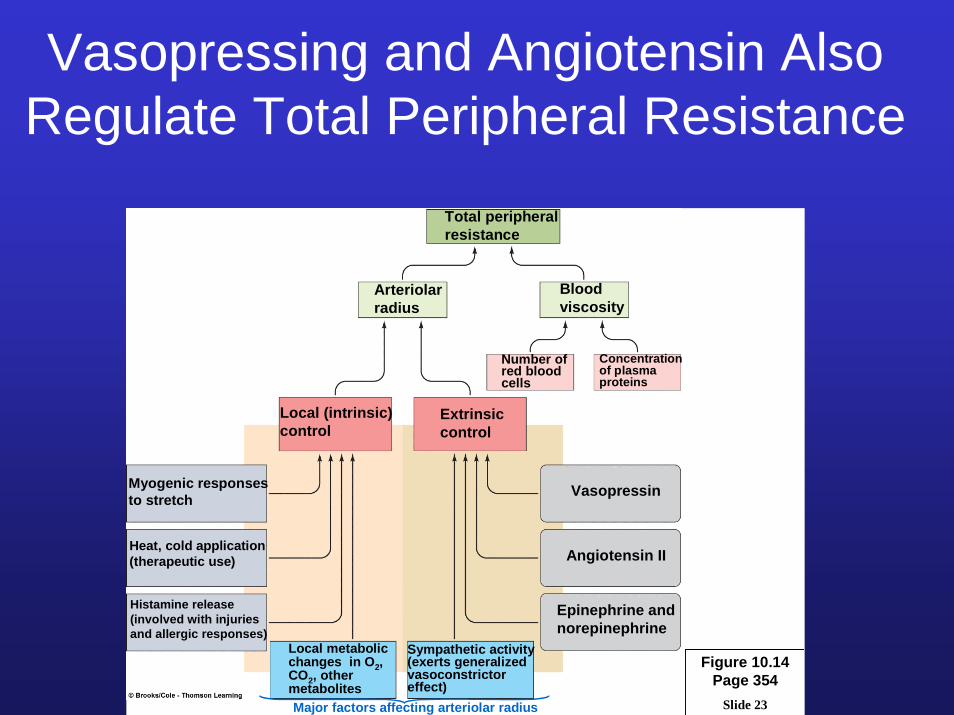
Vasopressing and Angiotensin Also Regulate Total Peripheral Resistance
Slide 23
Figure 10.14Page 354
Total peripheral resistance
Arteriolar radius
Blood viscosity
Number ofred blood cells
Concentrationof plasma proteins
Local (intrinsic) control
Extrinsic control
Myogenic responses to stretch Vasopressin
Heat, cold application(therapeutic use) Angiotensin II
Histamine release(involved with injuriesand allergic responses)
Epinephrine and norepinephrine
Local metabolic changes in O2, CO2, other metabolites
Sympathetic activity(exerts generalizedvasoconstrictor effect)
Major factors affecting arteriolar radius

Acid-Base BalanceRegulation of free H+ in body fluids
Acids are substances that generate free H+ in solution Ex: H2CO3 HCl
Bases are substances that accept free H+ in solutionEx: HCO3
- NaOH

Acids Release H+ in SolutionStrong Acid versus Weak Acid
Strong acids undergo complete dissociation in solution
Weak acids undergo incomplete dissociation in solution. At certain point, the amount of dissociated ions and whole molecule reach an equilibrium
Concentration of each component in the reaction is regulated by the law of mass action and dissociation constant Khttp://www.chembio.uoguelph.ca/educmat/chm19104/chemtoons/chemtoons4.htm

pH
Acids are substances that generate free H+ in solution
How do we quantify the amount of H+ present in a solution?
pH is a number that allow us to quantify the amount of H+ in solution:
pH= log 1/[H+]

pH ScaleSince pH is inversely proportional to the H+
concentration, an acidic solution will have a low pH and a basic solution will have a high pH
Notice that a pH = 7 is considered a neutral pH.
Pure water have a pH = 7
Physiologically, a pH = 7.4 is considered normal and correspond to the average pH of blood
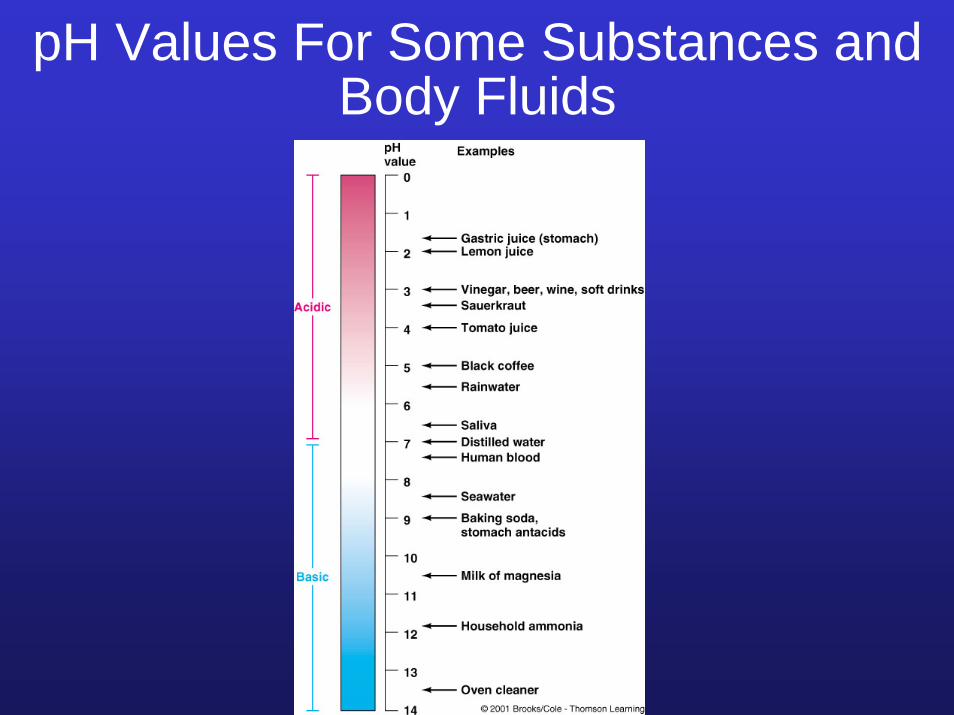
pH Values For Some Substances and Body Fluids

Physiological Changes Induced By H+
Fluctuations
Blood pH = 7.4Acidosis pH < 7.35Alkalosis pH > 7.45
Death may occur if 6.8 < Blood pH <8

Physiological Changes Induced By pH Changes
1) Increased H+ (acidosis) depresses nerve activity, whereas decreased H+ causes overexcitability of the nervous system
2) Changes in H+ concentration can modify protein structure and change enzymatic activity
3) Increased H+ results in lower K+
secretion in kidneys

K+ and H+ SecretionBasolateral pump can use K+ or H+ for Na+ reabsorption.
If body fluids become acidic then kidneys will secrete more H+ and leave K+ in blood…Not good!
H+
H+
H+H+

Sources of H+ in Human Body
1) Carbonic acid formation (H2CO3)
2) Inorganic acids produced during nutrients degradation(Sulfuric and phosphoric acid formation)
3) Organic acids produced during cell metabolism(Lactic acid, Fatty acids)

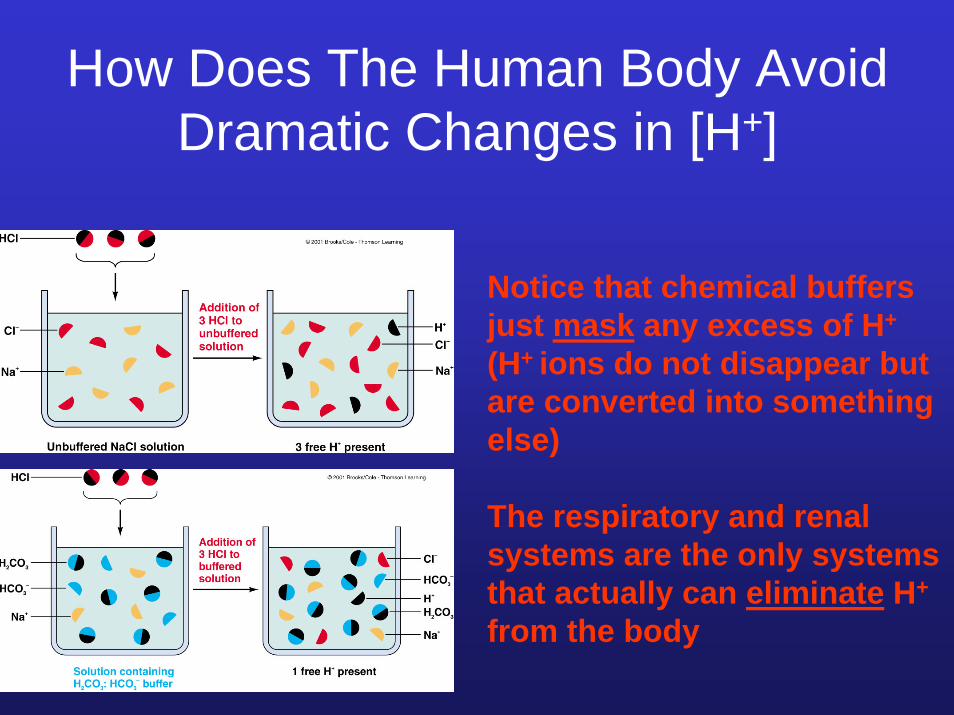
How Does The Human Body Avoid Dramatic Changes in [H+]
1) Chemical buffers
2) Respiration
3) Renal function

How Does The Human Body Avoid Dramatic Changes in [H+]:Role of Chemical Buffers
A Chemical buffer is a mix of a weak acid and its salt that can minimize pH changes when strong acids or bases are added.
Effect of law of mass action.Addition of a one component will shift equilibrium and partially compensate for changes in pH.
http://www.chembio.uoguelph.ca/educmat/chm19104/chemtoons/chemtoons5.htm

Chemical Buffers in Human Body
Carbonic acid-bicarbonate buffer (H2CO3/HCO3
-)is the most important system that control blood pH
Protein Buffer (Intracellular buffer)
Hemoglobin buffer
Phosphate buffer (Intracellular buffer)
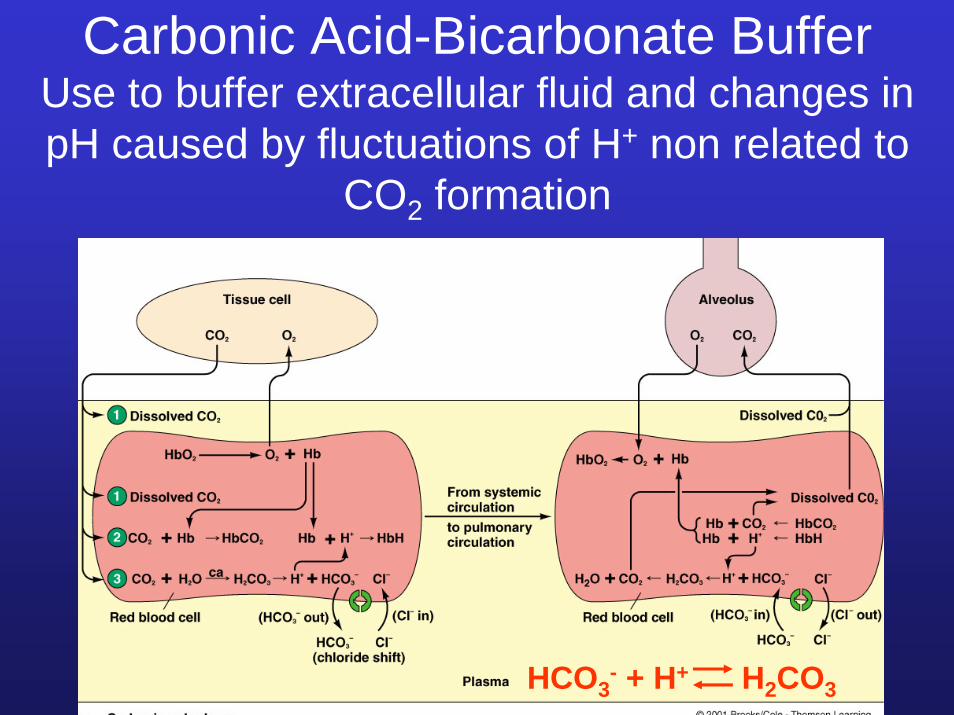
Carbonic Acid-Bicarbonate BufferUse to buffer extracellular fluid and changes in pH caused by fluctuations of H+ non related to
CO2 formation
HCO3- + H+ H2CO3

The Henderson-Hasselbalch Equation describes the relationship between H+ and the other members of the
bufferCO2 + H2O H2CO3 HCO3
- + H+
pH = pK + log ([HCO3- ]/ [CO2])
pH = 7.4 (normal pH)pK is a constant, for H2CO3 = 6.1
[HCO3- ]/ [CO2] = 20/1 (normal)
[HCO3- ] is regulated by the kidneys
[CO2] is regulated by lungs
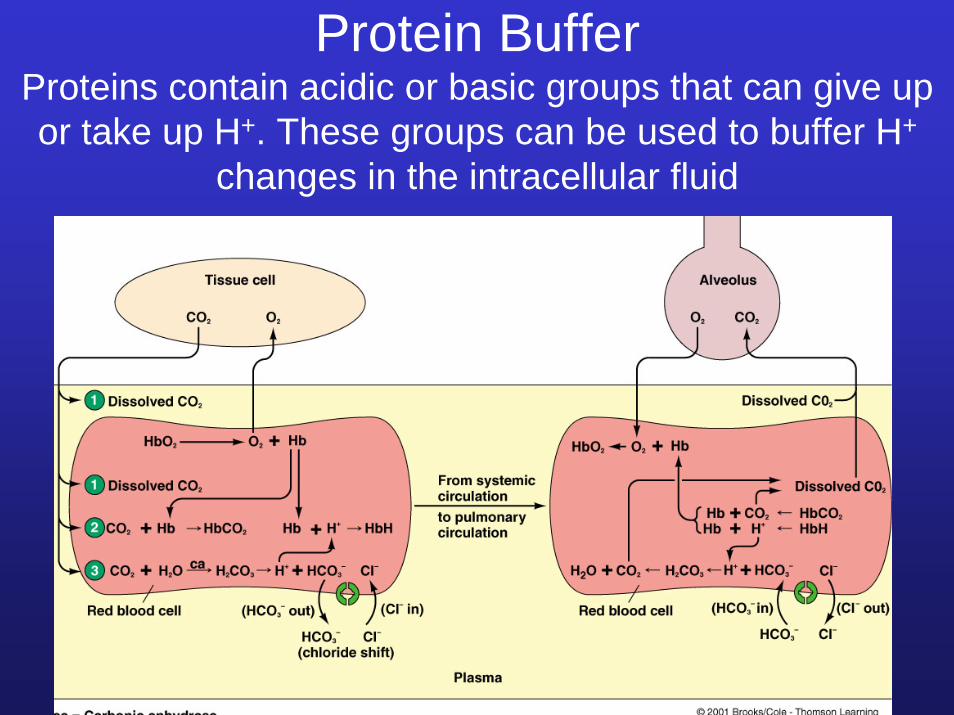
Protein BufferProteins contain acidic or basic groups that can give up or take up H+. These groups can be used to buffer H+
changes in the intracellular fluid

Hemoglobin BufferUse to buffer H+ generated from carbonic acid
Hb + H+ HHb

Phosphate BufferUse to buffer urine and intracellular fluids
Na2HPO4 + H+ NaH2PO4 + Na+
(basic phosphate salt) (acid phosphate salt)

How Does The Human Body Avoid Dramatic Changes in [H+]
Regulation of pH by Respiration
CO2 + H2O H2CO3 HCO3- + H+
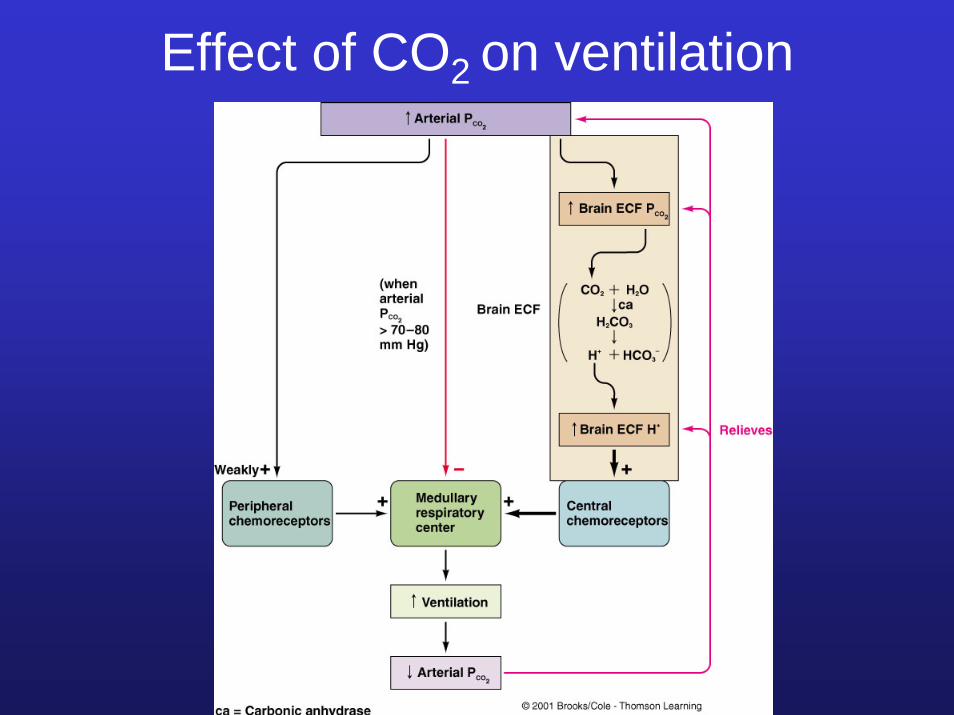
Effect of CO2 on ventilation

How Does The Human Body Avoid Dramatic Changes in [H+]
Chemical buffers (can regulate plasma pH instantly)
Respiration (is involved in the minute-to-minute regulation of plasma pH, but can not fully compensate for charges in pH)
Renal function (is involved in the long term regulation of pH- from hours to days)
How Does The Human Body Avoid Dramatic Changes in [H+]
Notice that chemical buffers just mask any excess of H+
(H+ ions do not disappear but are converted into something else)
The respiratory and renal systems are the only systems that actually can eliminate H+
from the body

Kidneys Control pH by Adjusting:1) H+ excretion
(H+ filtration is very low)2) HCO3
- filtration-reabsorption 3) NH3 secretion
HCO3-
H+
HCO3-
NH3
HCO3-
CO2H+

Kidneys Regulate pHMore Effectively Than the Lungs
(Lungs only regulate CO2. Beside regulating HCO3
-, kidneys regulate H+ formed as a result of metabolic activity: lactic & fatty acids formation)
Notice there is no H+ reabsorption in kidneys. There isonly HCO3
-
reabsorption

Kidneys Control pH by Adjusting:1) H+ excretion
(H+ enter kidneys by secretion resulting in a very acid urine, there is very little filtration WHY?)
Basolateral pump can use K+ or H+ for Na+
reabsorption. If body fluids become acidic then kidneys will secrete more H+
H+ in urine is buffered by phosphate buffers and NH3
H+

H+ excretion is influenced by:1) [H+] in plasma
2) [CO2] in plasma
HCO3-
HCO3-
H+
HCO3-
CO2H+
The ability of the kidneys to regulate H+ and CO2independently allows regulation of free H+
produced as a result of respiratory and/or metabolic activity. There is no neuronal/hormonal control
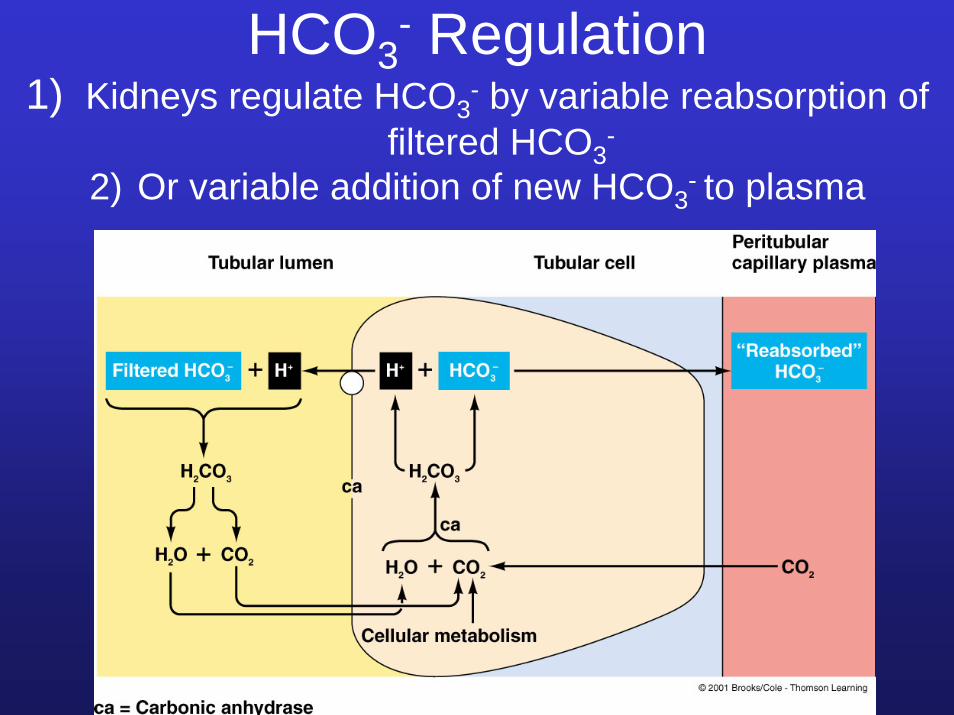
HCO3- Regulation
1) Kidneys regulate HCO3- by variable reabsorption of
filtered HCO3-
2) Or variable addition of new HCO3- to plasma

Kidneys Control pH by Adjusting:1) Kidneys regulate HCO3
- by variable reabsorption of filtered HCO3
-
HCO3- is filtered
but can not cross the luminal membrane. Notice however that HCO3
- can cross the basolateral membrane
There is a indirect reabsorption of filtered HCO3
-

HCO3- Regulation
2) Variable addition of HCO3- to plasma
(Buffering of H+ with phosphate allows release of new HCO3
- from peritubular capillaries)

Difference Between New and Reabsorbed HCO3
-
Notice differential permeability of luminal and basolateral membrane of tubular cells to HCO3
-
Luminal membrane is impermeable to HCO3
-
Basolateral membrane is permeable to HCO3
-

How Do the Kidneys Buffer Secreted H+?
1) Phosphate Buffer (Na2HPO4) 2) NH3 secretion
Na2HPO4
H+
H+Na2HPO4 + H+ NaH2PO4 + Na+

Why Is The Kidney Excreting Na2HPO4Continuously?
(Chapter 14)
Carrier saturation limits transport of a substance in tubules- tubular maximum
If concentration of substance in tubules goes above tubular maximumexcretion will take place-renal threshold
Kidneys regulate Na2HPO4plasma levels
[Glucose] 125 mg
[Na2HPO4] 300 mg

How Do the Kidneys Buffer Secreted H+?
1) Phosphate Buffer (Na2HPO4) 2) NH3 secretion
H+
H+
NH3 + H+ NH4+
Notice:NH3 is formed and released into the lumen by tubular cells
NH4+ is impermeable to luminal
membranesNH3
NH3

Acid-Base Imbalances Arise From:1) Respiratory Disturbance2) Metabolic Disturbance
HCO3-
HCO3-
H+
HCO3-
CO2H+
Respiratory disturbance may cause:Respiratory acidosis (too much CO2)Respiratory alkalosis (too little CO2
Metabolic disturbance may cause:Metabolic acidosis (too little HCO3
-)Metabolic alkalosis (to much HCO3
-)

Acid-Base Imbalance
Notice: kidneys control HCO3-
and H+ by regulating the creation of new HCO3
- or the reabsorbtion of filtered HCO3
-
During respiratory acidosis (+CO2) kidneys conserve more HCO3
- and add more new HCO3
- while secreting more H+
During respiratory alkalosis (-CO2) kidneys conserve more H+ and excrete more HCO3
-

Acid-Base ImbalanceRespiratory
AcidosisRespiratory
AlkalosisMetabolicAcidosis
MetabolicAlkalosis
Too much CO2, hypoventilation
Too little CO2, hyperventilation
Fall in HCO3- Increase in HCO3
-
Cause: Lung disease
Depression of respiratory centerRespiratory motor
dysfunction
AnxietyAspirin
poisoningHigh altitude
DiarrheaDiabetes mellitus
Strenuous exercise
Renal failure
VomitingIngestion of
alkaline compounds
Compensation:Chemical buffers
Kidneys(notice that
damaged lungs can not regulate CO2)
Chemical buffersLungs
Kidneys
Chemical buffersLungs
Kidneys
Chemical buffersLungs
Kidneys