chapter 21 amputationsabouttheshoulder: · pdf filelower limb deficiencies also play a ......
TRANSCRIPT
Chapter 21Amputations About the Shoulder:Prosthetic ManagementJohn M. Miguelez, CPMichelle D. Miguelez, JDRandall D. Alley, CP
IntroductionThe prosthetic rehabilitation of anindividual with a humeral neck, gle-nohumeral, or interscapulothoraciclevel of absence has traditionally beena significant challenge to the rehabili-tation team, often resulting in poorsuccess rates. Each of these levels isanatomically unique, but the overallapproach to the prosthetic manage-ment is similar (Figure 1). This chap-ter describes the three phases ofprosthetic management that are criti-cal to long-term prosthesis use andpatient satisfaction: (1) the prepros-thetic phase, during which the pros-thetic rehabilitation plan is formu-lated; (2) the interim phase, duringwhich the diagnostic prosthesis,which evolves into the definitiveprosthesis, is created; and (3) thepostprosthetic phase, during whichthe focus is on prosthetic refinementand training. The systematic methodof care described in this chapter canmaximize the patient’s prosthetic re-habilitation potential.
Preprosthetic PhaseThe preprosthetic phase includes thephysical assessment of the patient, athorough consideration of prostheticdesign criteria, a discussion of pros-thetic options and components, and,finally, the formulation of the pros-thetic rehabilitation plan. The physi-cal assessment of the individual withupper limb absence is one of the most
crucial aspects of the rehabilitationprocess, because this is when informa-tion is gathered, both clinically andthrough open dialogue, that serves asthe basis for subsequent rehabilita-tion. Failure to devote sufficient timeand focus to the preprosthetic phasehas directly contributed to the histor-ically suboptimal prosthetic successrates for individuals with limb ab-sence or amputation at the gleno-humeral and associated levels.
AssessmentInitially, the practitioner shouldrecord not only the level(s) andside(s) of involvement but alsowhether or not a loss of dominanceoccurred. An overall health assess-ment should be made, and particularattention should be paid to cardiacand associated circulatory health be-cause such proximal levels of limbloss require the user to expend con-siderable effort during operation of abody-powered or hybrid prosthesis.Ipsilateral considerations include thecause of absence, the date and extentof injury if applicable, tissue condi-tion, range of motion and strength(for gross movement as well as themyoelectric signal), and any associ-ated discomfort or sensitivity relatedto the region, whether from contactpressure, potential weight bearing, ormotions required for operation of theprosthesis. All of these elements arevitally important when considering
not only the socket design but alsothe control strategy. The extent ofcontralateral limb loss, deficiency orother involvement, and the degree offunction present should be noted. Allthe considerations that apply to theipsilateral remnant are relevant to thecontralateral limb, as harnessing de-sign and control strategies must in-corporate contralateral involvement.Lower limb deficiencies also play asignificant role in balance, donningand doffing, and general upper limbcomponent selection. For example,the prosthesis for an individual withan upper limb deficiency who uses acane or a walker should have suffi-cient prehensile grip to withstand theforces applied to these balance aids.
Myotesting is important to deter-mine the feasibility of using myoelec-tric control. The information myo-testing provides is also important as afeedback tool for teaching and train-ing and is a quantifiable assessment ofpatient progress. The interaction ofthe myoelectric signals during agonis-tic and antagonistic contractions ineach relevant muscle or muscle groupmust be assessed, not simply the am-plitude of a single channel in isola-tion. (Agonist and antagonist areloosely defined here as they relate toprosthetic function, which may ormay not differ from physiologic func-tion, depending on the muscle ormuscle groups involved.) Finally, thepractitioner must define the optimal
American Academy of Orthopaedic Surgeons 263
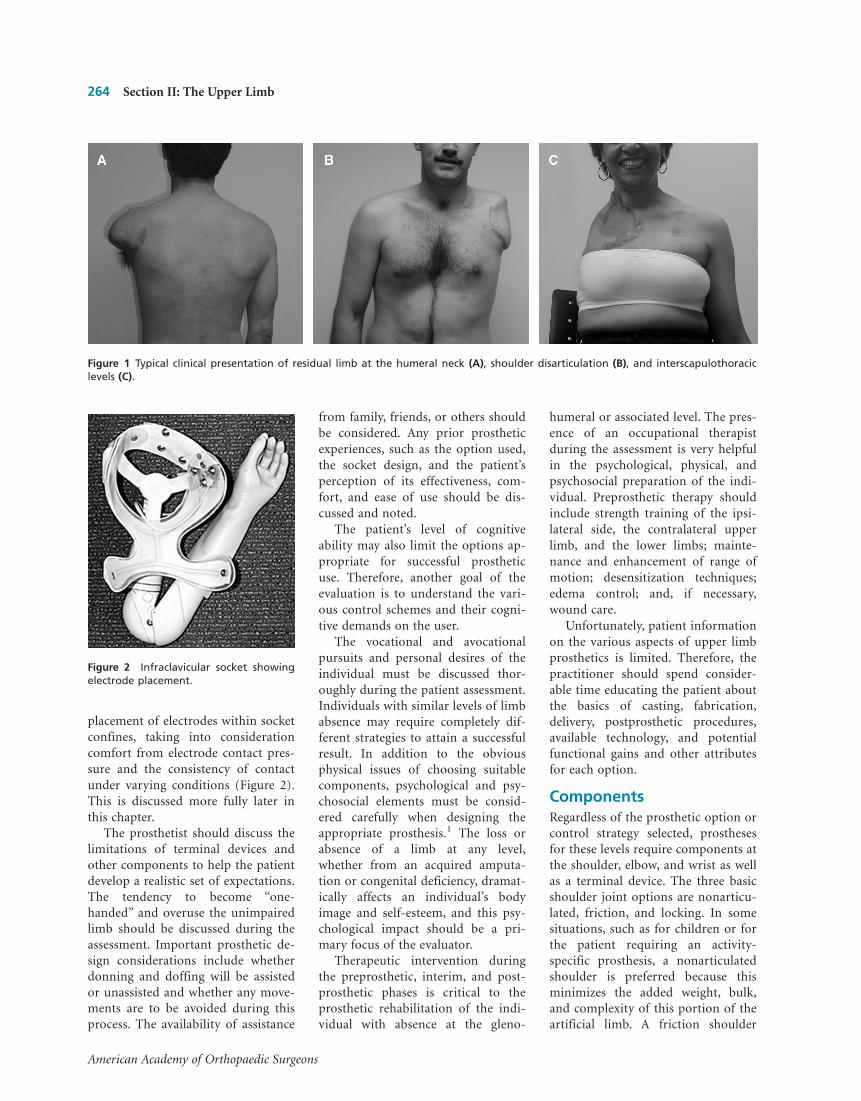
placement of electrodes within socketconfines, taking into considerationcomfort from electrode contact pres-sure and the consistency of contactunder varying conditions (Figure 2).This is discussed more fully later inthis chapter.
The prosthetist should discuss thelimitations of terminal devices andother components to help the patientdevelop a realistic set of expectations.The tendency to become “one-handed” and overuse the unimpairedlimb should be discussed during theassessment. Important prosthetic de-sign considerations include whetherdonning and doffing will be assistedor unassisted and whether any move-ments are to be avoided during thisprocess. The availability of assistance
from family, friends, or others shouldbe considered. Any prior prostheticexperiences, such as the option used,the socket design, and the patient’sperception of its effectiveness, com-fort, and ease of use should be dis-cussed and noted.
The patient’s level of cognitiveability may also limit the options ap-propriate for successful prostheticuse. Therefore, another goal of theevaluation is to understand the vari-ous control schemes and their cogni-tive demands on the user.
The vocational and avocationalpursuits and personal desires of theindividual must be discussed thor-oughly during the patient assessment.Individuals with similar levels of limbabsence may require completely dif-ferent strategies to attain a successfulresult. In addition to the obviousphysical issues of choosing suitablecomponents, psychological and psy-chosocial elements must be consid-ered carefully when designing theappropriate prosthesis.1 The loss orabsence of a limb at any level,whether from an acquired amputa-tion or congenital deficiency, dramat-ically affects an individual’s bodyimage and self-esteem, and this psy-chological impact should be a pri-mary focus of the evaluator.
Therapeutic intervention duringthe preprosthetic, interim, and post-prosthetic phases is critical to theprosthetic rehabilitation of the indi-vidual with absence at the gleno-
humeral or associated level. The pres-ence of an occupational therapistduring the assessment is very helpfulin the psychological, physical, andpsychosocial preparation of the indi-vidual. Preprosthetic therapy shouldinclude strength training of the ipsi-lateral side, the contralateral upperlimb, and the lower limbs; mainte-nance and enhancement of range ofmotion; desensitization techniques;edema control; and, if necessary,wound care.
Unfortunately, patient informationon the various aspects of upper limbprosthetics is limited. Therefore, thepractitioner should spend consider-able time educating the patient aboutthe basics of casting, fabrication,delivery, postprosthetic procedures,available technology, and potentialfunctional gains and other attributesfor each option.
ComponentsRegardless of the prosthetic option orcontrol strategy selected, prosthesesfor these levels require components atthe shoulder, elbow, and wrist as wellas a terminal device. The three basicshoulder joint options are nonarticu-lated, friction, and locking. In somesituations, such as for children or forthe patient requiring an activity-specific prosthesis, a nonarticulatedshoulder is preferred because thisminimizes the added weight, bulk,and complexity of this portion of theartificial limb. A friction shoulder
Figure 2 Infraclavicular socket showingelectrode placement.
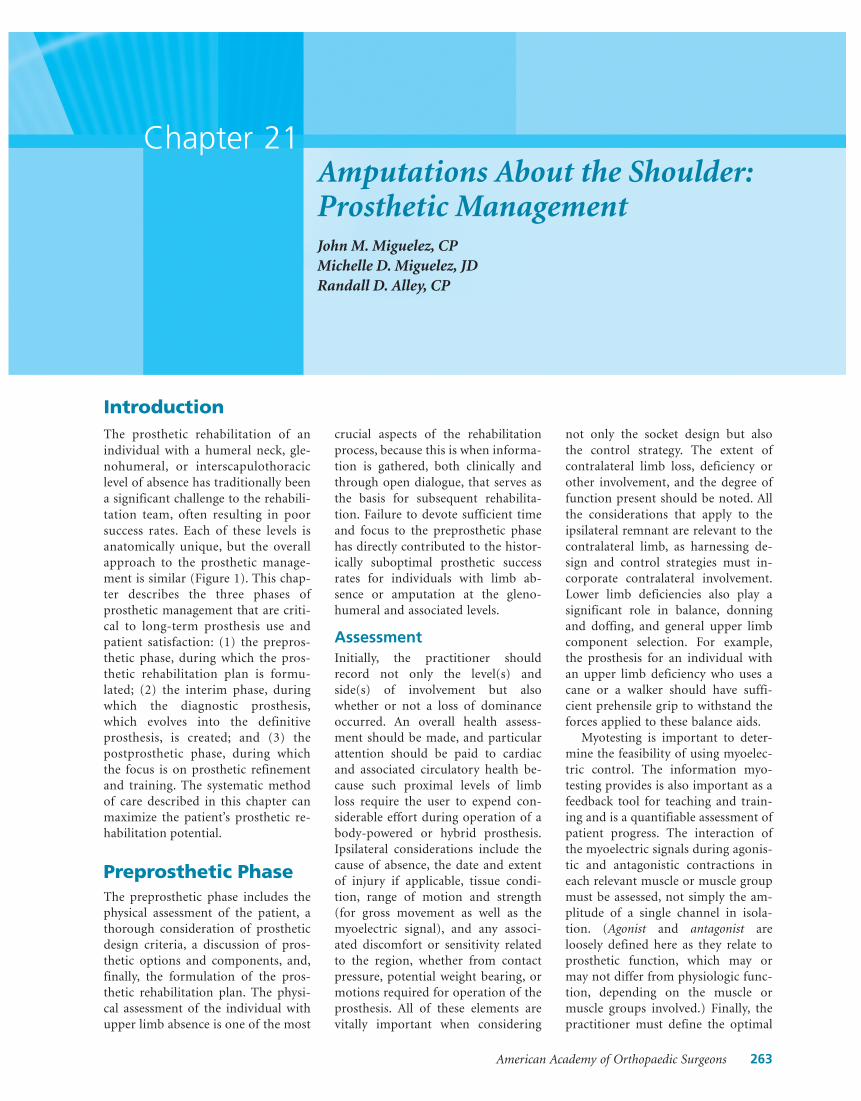
Figure 1 Typical clinical presentation of residual limb at the humeral neck (A), shoulder disarticulation (B), and interscapulothoraciclevels (C).
264 Section II: The Upper Limb
American Academy of Orthopaedic Surgeons
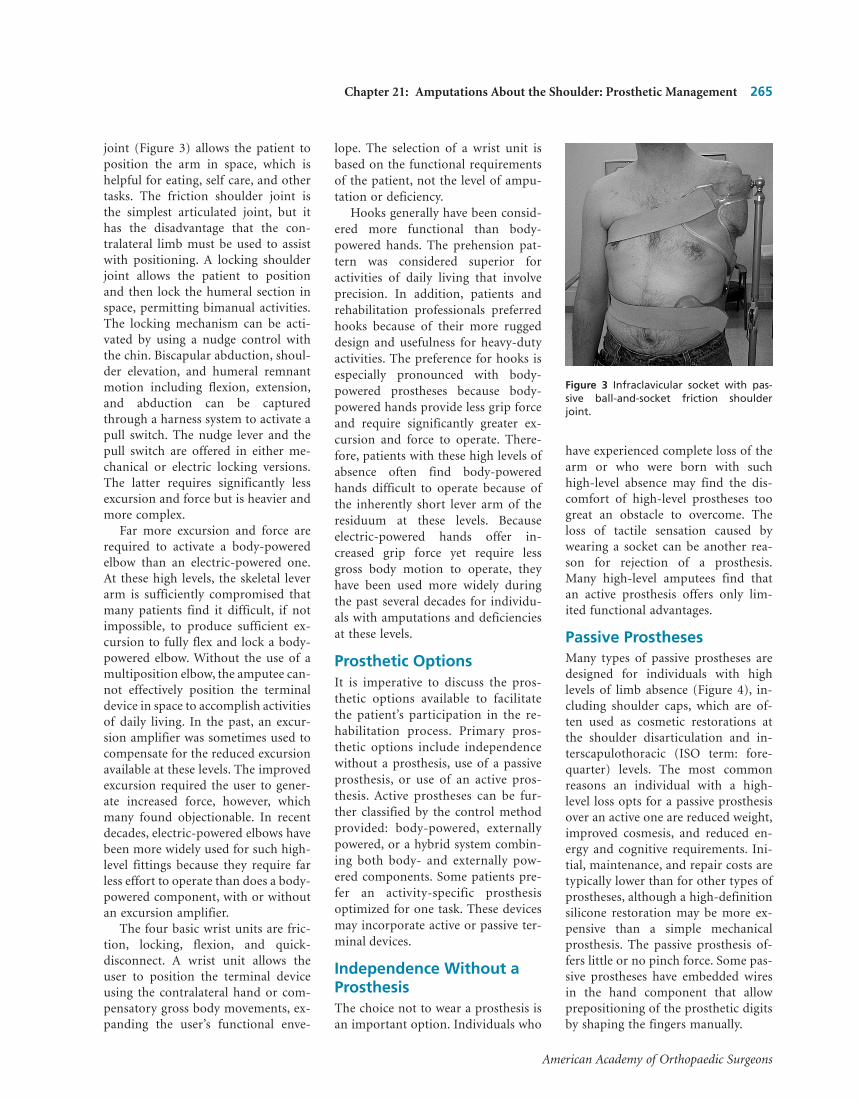
joint (Figure 3) allows the patient toposition the arm in space, which ishelpful for eating, self care, and othertasks. The friction shoulder joint isthe simplest articulated joint, but ithas the disadvantage that the con-tralateral limb must be used to assistwith positioning. A locking shoulderjoint allows the patient to positionand then lock the humeral section inspace, permitting bimanual activities.The locking mechanism can be acti-vated by using a nudge control withthe chin. Biscapular abduction, shoul-der elevation, and humeral remnantmotion including flexion, extension,and abduction can be capturedthrough a harness system to activate apull switch. The nudge lever and thepull switch are offered in either me-chanical or electric locking versions.The latter requires significantly lessexcursion and force but is heavier andmore complex.
Far more excursion and force arerequired to activate a body-poweredelbow than an electric-powered one.At these high levels, the skeletal leverarm is sufficiently compromised thatmany patients find it difficult, if notimpossible, to produce sufficient ex-cursion to fully flex and lock a body-powered elbow. Without the use of amultiposition elbow, the amputee can-not effectively position the terminaldevice in space to accomplish activitiesof daily living. In the past, an excur-sion amplifier was sometimes used tocompensate for the reduced excursionavailable at these levels. The improvedexcursion required the user to gener-ate increased force, however, whichmany found objectionable. In recentdecades, electric-powered elbows havebeen more widely used for such high-level fittings because they require farless effort to operate than does a body-powered component, with or withoutan excursion amplifier.
The four basic wrist units are fric-tion, locking, flexion, and quick-disconnect. A wrist unit allows theuser to position the terminal deviceusing the contralateral hand or com-pensatory gross body movements, ex-panding the user’s functional enve-
lope. The selection of a wrist unit isbased on the functional requirementsof the patient, not the level of ampu-tation or deficiency.
Hooks generally have been consid-ered more functional than body-powered hands. The prehension pat-tern was considered superior foractivities of daily living that involveprecision. In addition, patients andrehabilitation professionals preferredhooks because of their more ruggeddesign and usefulness for heavy-dutyactivities. The preference for hooks isespecially pronounced with body-powered prostheses because body-powered hands provide less grip forceand require significantly greater ex-cursion and force to operate. There-fore, patients with these high levels ofabsence often find body-poweredhands difficult to operate because ofthe inherently short lever arm of theresiduum at these levels. Becauseelectric-powered hands offer in-creased grip force yet require lessgross body motion to operate, theyhave been used more widely duringthe past several decades for individu-als with amputations and deficienciesat these levels.
Prosthetic OptionsIt is imperative to discuss the pros-thetic options available to facilitatethe patient’s participation in the re-habilitation process. Primary pros-thetic options include independencewithout a prosthesis, use of a passiveprosthesis, or use of an active pros-thesis. Active prostheses can be fur-ther classified by the control methodprovided: body-powered, externallypowered, or a hybrid system combin-ing both body- and externally pow-ered components. Some patients pre-fer an activity-specific prosthesisoptimized for one task. These devicesmay incorporate active or passive ter-minal devices.
Independence Without aProsthesisThe choice not to wear a prosthesis isan important option. Individuals who
have experienced complete loss of thearm or who were born with suchhigh-level absence may find the dis-comfort of high-level prostheses toogreat an obstacle to overcome. Theloss of tactile sensation caused bywearing a socket can be another rea-son for rejection of a prosthesis.Many high-level amputees find thatan active prosthesis offers only lim-ited functional advantages.
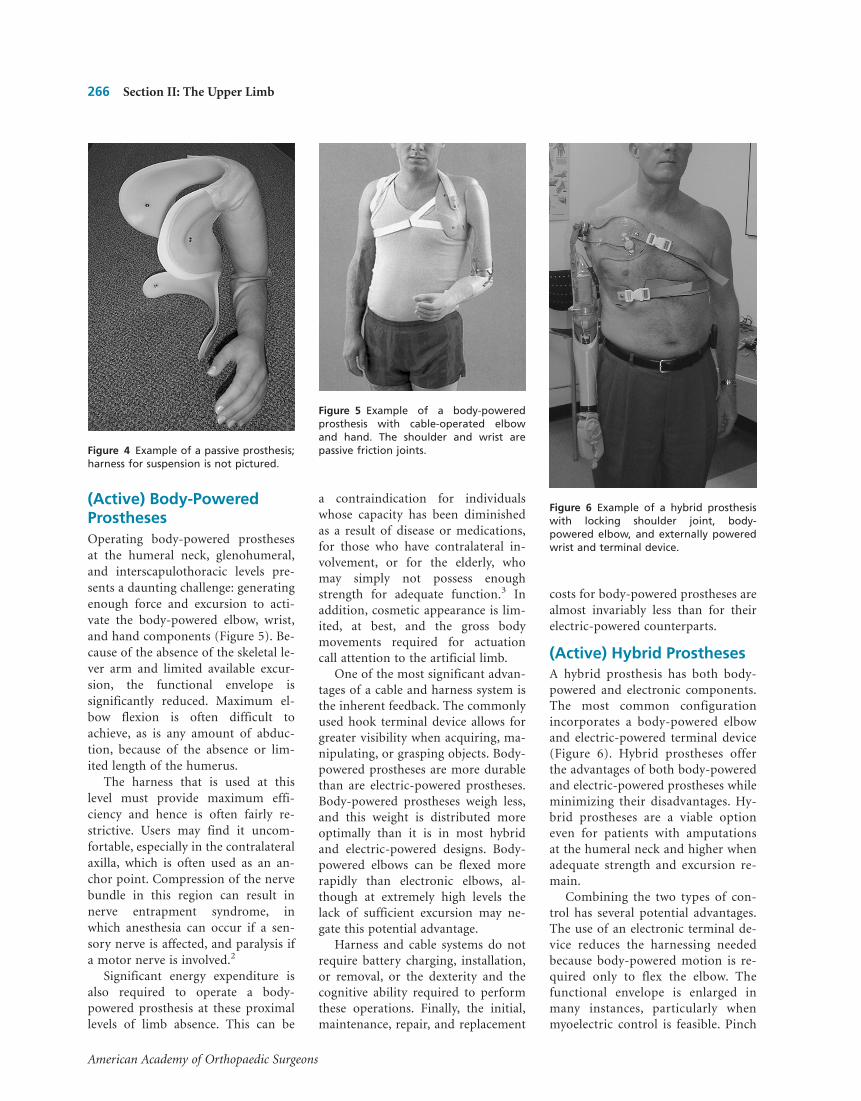
Passive ProsthesesMany types of passive prostheses aredesigned for individuals with highlevels of limb absence (Figure 4), in-cluding shoulder caps, which are of-ten used as cosmetic restorations atthe shoulder disarticulation and in-terscapulothoracic (ISO term: fore-quarter) levels. The most commonreasons an individual with a high-level loss opts for a passive prosthesisover an active one are reduced weight,improved cosmesis, and reduced en-ergy and cognitive requirements. Ini-tial, maintenance, and repair costs aretypically lower than for other types ofprostheses, although a high-definitionsilicone restoration may be more ex-pensive than a simple mechanicalprosthesis. The passive prosthesis of-fers little or no pinch force. Some pas-sive prostheses have embedded wiresin the hand component that allowprepositioning of the prosthetic digitsby shaping the fingers manually.
Figure 3 Infraclavicular socket with pas-sive ball-and-socket friction shoulderjoint.
Chapter 21: Amputations About the Shoulder: Prosthetic Management 265
American Academy of Orthopaedic Surgeons
(Active) Body-PoweredProsthesesOperating body-powered prosthesesat the humeral neck, glenohumeral,and interscapulothoracic levels pre-sents a daunting challenge: generatingenough force and excursion to acti-vate the body-powered elbow, wrist,and hand components (Figure 5). Be-cause of the absence of the skeletal le-ver arm and limited available excur-sion, the functional envelope issignificantly reduced. Maximum el-bow flexion is often difficult toachieve, as is any amount of abduc-tion, because of the absence or lim-ited length of the humerus.
The harness that is used at thislevel must provide maximum effi-ciency and hence is often fairly re-strictive. Users may find it uncom-fortable, especially in the contralateralaxilla, which is often used as an an-chor point. Compression of the nervebundle in this region can result innerve entrapment syndrome, inwhich anesthesia can occur if a sen-sory nerve is affected, and paralysis ifa motor nerve is involved.2
Significant energy expenditure isalso required to operate a body-powered prosthesis at these proximallevels of limb absence. This can be
a contraindication for individualswhose capacity has been diminishedas a result of disease or medications,for those who have contralateral in-volvement, or for the elderly, whomay simply not possess enoughstrength for adequate function.3 Inaddition, cosmetic appearance is lim-ited, at best, and the gross bodymovements required for actuationcall attention to the artificial limb.
One of the most significant advan-tages of a cable and harness system isthe inherent feedback. The commonlyused hook terminal device allows forgreater visibility when acquiring, ma-nipulating, or grasping objects. Body-powered prostheses are more durablethan are electric-powered prostheses.Body-powered prostheses weigh less,and this weight is distributed moreoptimally than it is in most hybridand electric-powered designs. Body-powered elbows can be flexed morerapidly than electronic elbows, al-though at extremely high levels thelack of sufficient excursion may ne-gate this potential advantage.
Harness and cable systems do notrequire battery charging, installation,or removal, or the dexterity and thecognitive ability required to performthese operations. Finally, the initial,maintenance, repair, and replacement
costs for body-powered prostheses arealmost invariably less than for theirelectric-powered counterparts.
(Active) Hybrid ProsthesesA hybrid prosthesis has both body-powered and electronic components.The most common configurationincorporates a body-powered elbowand electric-powered terminal device(Figure 6). Hybrid prostheses offerthe advantages of both body-poweredand electric-powered prostheses whileminimizing their disadvantages. Hy-brid prostheses are a viable optioneven for patients with amputationsat the humeral neck and higher whenadequate strength and excursion re-main.
Combining the two types of con-trol has several potential advantages.The use of an electronic terminal de-vice reduces the harnessing neededbecause body-powered motion is re-quired only to flex the elbow. Thefunctional envelope is enlarged inmany instances, particularly whenmyoelectric control is feasible. Pinch
Figure 4 Example of a passive prosthesis;harness for suspension is not pictured.
Figure 5 Example of a body-poweredprosthesis with cable-operated elbowand hand. The shoulder and wrist arepassive friction joints.
Figure 6 Example of a hybrid prosthesiswith locking shoulder joint, body-powered elbow, and externally poweredwrist and terminal device.
266 Section II: The Upper Limb
American Academy of Orthopaedic Surgeons

force is also much greater with anelectronic device than is possible withbody-powered, voluntary-openingterminal devices. Also, an electronicterminal device usually provides bothvoluntary opening and voluntaryclosing, a more natural reproductionof human hand movement. Operatingthe terminal device via myoelectriccontrol is believed to improve muscletone and reduce disuse atrophy. Ad-vantages of the body-powered el-bow are that it provides more rapidflexion/extension movements, givesthe user important sensory feedbackfrom the harness forces, and reducesthe overall weight of the prosthesis.Also, the initial, maintenance, andrepair costs of the system are lessbecause an electronic elbow is notneeded. Finally, a hybrid controlsystem can encourage simultaneousoperation of the elbow and terminaldevice.
(Active) ExternallyPowered ProsthesesElectric-powered components mini-mize the energy expenditure and dis-comfort associated with a control ca-ble and harness (Figure 7). Both staticand dynamic cosmesis are improvedwhen a control cable is not requiredfor either terminal device or elbowoperation. Like hybrid systems, a myo-electric system offers increased pinchforce, voluntary opening and closing,and, although a prosthetic shoulderjoint permits only passive position-ing, the potential for an even greaterfunctional envelope.
A myoelectric elbow has the disad-vantage of lacking the direct feedbackoffered by a harness and cable system,although indirect feedback is stillavailable based on input effort, dura-tion of supplied signal, elbow vibra-tion, and sound. The weight of a fullyelectronic system is considerable, andcare must be taken to ensure that thesocket provides at least partial sus-pension to minimize the weightborne by sensitive areas. In addition,every externally powered prosthesishas battery installation, removal, and
maintenance requirements, and oper-ation of the primary and secondaryelectronic controls can impose a sub-stantial cognitive demand on the user.Despite these disadvantages, many in-dividuals with glenohumeral-level ab-sences do well with completely elec-tronic prostheses.
Activity-Specific ProsthesesActivity-specific devices include rec-reational prostheses and those de-signed to facilitate work tasks oractivities of daily living. Activity-specific prostheses are very effectivein accomplishing the specific tasks forwhich they are designed. Becausethese prostheses usually require onlysimple controls and minimal compo-nents, they are often less costly thanmore complex designs (Figure 8). Thechief disadvantage of an activity-specific prosthesis is that it has lim-ited utility. Interchangeable activity-specific prostheses can help to addressthis limitation.
Design ConsiderationsThe foundation for successful pros-thesis use is the socket. Unless thesocket is comfortable and securelysuspended, the prosthesis will not be
worn on a sustained basis. At the gle-nohumeral level, the key to achievingstability is an intimately fitted socketthat provides rigidity in load-bearingareas and serves as a secure platformfor anchoring components.4
Individuals with amputations andabsences at the glenohumeral and as-sociated levels have reported manyproblems with long-term prosthesisuse. Frequently mentioned issues in-clude the weight of the prosthesis,heat buildup within the socket, lack ofstability, reduced control of the termi-nal device in certain planes and bodypositions, and difficulty in indepen-dent donning. The socket design mustdistribute the load primarily over ar-eas with sufficient tissue paddingwhile eliminating excessive pressureon skeletal protuberances. Heatbuildup while wearing a prosthesis isdirectly related to the amount of skincovered by the socket and the result-ing lack of heat dissipation. There-fore, reducing the surface area of thesocket can greatly improve comfortand patient acceptance. Lack of sta-bility and reduced control of the ter-minal device in certain planes andbody positions are both results of asocket that changes position duringmovement. Without a stable socket,the efficiency of the harness system isgreatly reduced. Consequently, thewearer must produce more grossbody movement to operate the pros-thesis, resulting in increased fatigueand frustration. With improvedsocket stability, a less complex harnesssystem may be sufficient, which facili-tates the donning process.
Figure 7 Example of an externally pow-ered prosthesis with locking shoulderjoint plus myoelectric elbow, wrist, hand,and interchangeable electronic lock ter-minal device.
Figure 8 Activity-specific terminal devicefor playing billiards. (Courtesy of BobRadocy.)
Chapter 21: Amputations About the Shoulder: Prosthetic Management 267
American Academy of Orthopaedic Surgeons
To create an effective prosthesis,the prosthetist must be able to assessthe many design criteria both individ-ually and as they relate to one an-other. The harness system must be de-termined during the preprostheticphase, as this will influence the socketdesign. The harness is especially criti-cal in bilateral deficiencies or whensignificant areas of scarring or skingraft are present. With amputations atthe humeral neck (see Case Study 2),the remnant humerus can often beused for primary or secondary con-trol strategies, which may affect com-ponent selection and socket design.Finally, it is important to clarify thepatient’s cosmetic expectations for theprosthesis because these consider-ations may also affect component se-lection, socket design, control strate-gies, and long-term acceptance. Theoptimal socket is the one that bal-ances these interrelated goals to meetthe needs of the individual amputee.
Formulation of theRehabilitation PlanThe preprosthetic phase culminateswith the formulation of a detailedprosthetic rehabilitation plan. Com-prehensive evaluations by the other
members of the rehabilitation team,including the physician, the physicaland occupational therapists, the psy-chologist, and the rehabilitation coor-dinator, should be concurrent withthe prosthetic assessment. Interactionand communication among rehabili-tation team members is critical tosuccess at these levels. Once all mem-bers of the rehabilitation team haveoffered their recommendations, a fi-nal rehabilitation plan can be formu-lated. The recommendations musttake into account the patient’s physi-cal capacity and willingness to com-mit to what is often a rigorous fittingand training schedule.5 A patient whohas a sense of control and active par-ticipation in the formulation of therehabilitation plan is more likely toput forth the effort necessary to exe-cute the plan successfully.
The rehabilitation plan integratesthe patient’s prosthetic, therapeutic,psychological, and medical needsbased on short- and long-term goals.Prosthetic options affect occupationaltherapy, physical therapy, and psy-chological counseling.6 One of thegreatest challenges is orchestratingthe interaction of the various services.When treatment team schedules arenot coordinated in advance, lapsesin care can delay the rehabilitationprocess and lead to patient frustrationand discouragement. Progress evalua-tions should be scheduled regularly,
during which the status and theevolving goals of the patient are dis-cussed and the plan modified as nec-essary.
Interim ProstheticPhaseAfter a thorough prosthetic and ther-apeutic rehabilitation plan has beenformulated, the interim prostheticphase starts. During this phase, theprosthesis is created and therapy tran-sitions from general residual limbpreparation to specific prosthetictraining. Therapy could include elec-tromyographic (EMG) site selectionand specific muscle differentiation fora myoelectric prosthesis or furthershoulder complex strengthening forbody-powered components. Thisphase also includes the cast impres-sion, creation of a diagnostic prosthe-sis, and the assessment of functionaluse of the diagnostic prosthesis, and itconcludes with fabrication and deliv-ery of a definitive prosthesis. The di-agnostic prosthesis ensures that opti-mal socket fit and comfort andprosthesis control/function, align-ment, and definitive fabrication spec-ifications have been achieved.
The type of prosthesis control cho-sen influences socket design andshould therefore occur before an im-pression of the patient’s residual limbis taken. Regardless of which pros-thetic option is selected, all gleno-humeral and associated level prosthe-ses require a stable and comfortablesocket to support the prostheticshoulder, elbow, wrist unit, and ter-minal device components.
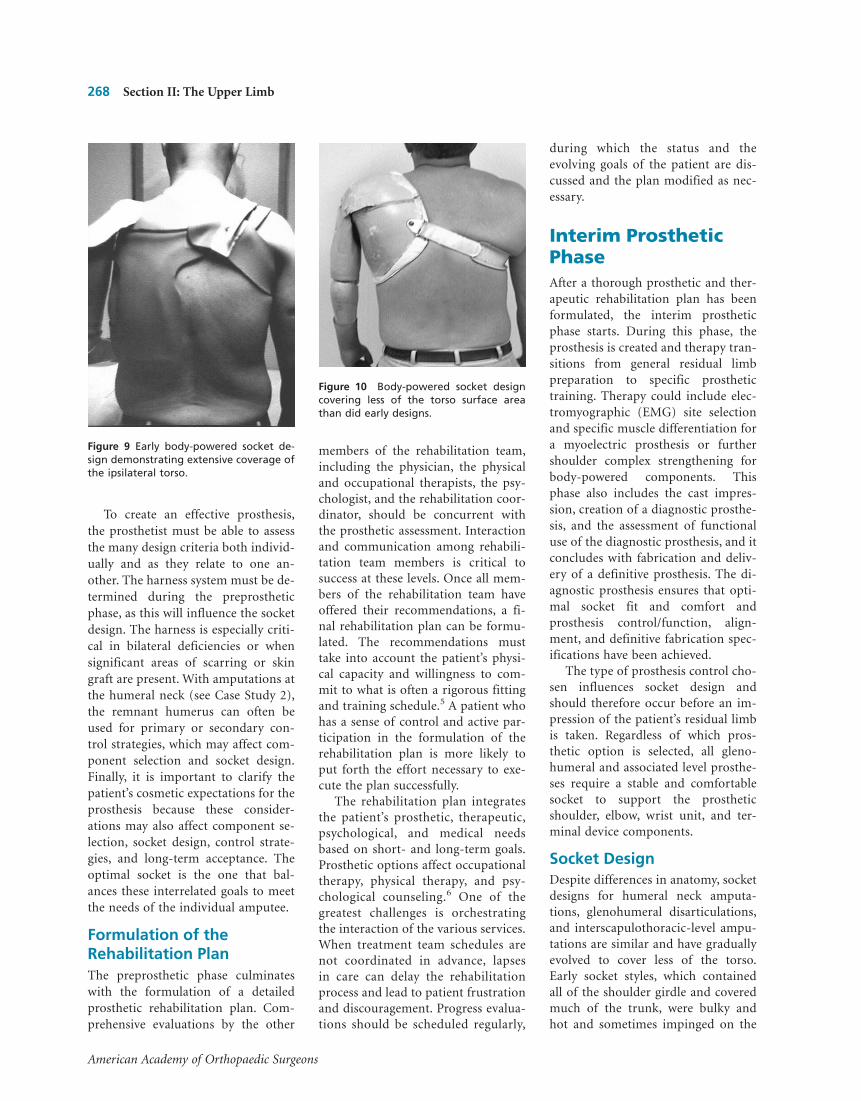
Socket DesignDespite differences in anatomy, socketdesigns for humeral neck amputa-tions, glenohumeral disarticulations,and interscapulothoracic-level ampu-tations are similar and have graduallyevolved to cover less of the torso.Early socket styles, which containedall of the shoulder girdle and coveredmuch of the trunk, were bulky andhot and sometimes impinged on the
Figure 10 Body-powered socket designcovering less of the torso surface areathan did early designs.
Figure 9 Early body-powered socket de-sign demonstrating extensive coverage ofthe ipsilateral torso.
268 Section II: The Upper Limb
American Academy of Orthopaedic Surgeons

clavicle or acromion7,8 (Figure 9).These early designs were replaced bysockets with more abbreviated trim-lines that reduced weight and heatbuildup9 (Figure 10). More extensiveharnessing was often required to sta-bilize the prosthesis, however, despitethe smaller surface area of the socket.
Simpson and Sauter are creditedwith the next evolution in socket de-sign, the Perimeter Frame.10 Made oflightweight aluminum, this socket in-cluded large windows, or “cutouts,” inthe anterior, posterior, and acromio-clavicular regions (Figure 11). Bymoving the acromioclavicular area orhumeral neck inside the socket, theamputee could activate switches con-trolling electronic devices with goodresults. Myoelectrodes in the Perime-ter Frame had limited success, how-ever, because it was difficult to main-tain skin-to-electrode contact.11
In the 1980s, infraclavicular de-signs were developed.12 The infraclav-icular design differs from its prede-cessors because it does not enclose theshoulder complex to support theweight of the prosthesis. Instead, it re-lies on compression of the deltopec-toral muscle group anteriorly and thescapular region posteriorly.13 Inti-mate anatomic contouring of theseload-bearing areas stabilizes thesocket on the torso (Figure 12), en-abling the wearer to effectively posi-tion the terminal device in space. In-fraclavicular sockets are also lessnoticeable under clothing than areother designs. Because the acromio-clavicular complex is not encased inthis design, it is free to move indepen-dently of the socket. This movementcan be used to activate secondarycontrol inputs to control wrist rota-tion, shoulder or elbow locks, etc.14,15
Diagnostic AssessmentThe diagnostic socket with the har-ness affixed should be assessed bothstatically and dynamically while thepatient is standing, sitting, and bend-ing forward and to the side. It is im-portant to evaluate the load-bearingsurfaces and ensure that forces areevenly distributed so that excessive
pressure is not applied to any singlearea.
Diagnostic assessment also focuseson the identification and verificationof sufficient EMG signal recognitionfor myoelectric control, sufficientcapture of excursion for body-powered control, or both for hybridcontrol. An experienced therapist isextremely valuable in assisting the pa-tient and practitioner with locatingand strengthening specific musclegroups. When myoelectric control isselected, the diagnostic socket shouldbe carefully examined for consistentskin contact, especially during con-traction of the desired control mus-cles.16 Some myoelectric systemsrequire the patient to quickly cocon-tract antagonistic muscles to controlfunctions such as unlocking the elbowor transferring control from the ter-minal device to an electric wrist rota-tor.17 Some patients have difficultycontracting both targeted controlmuscles simultaneously and will re-quire either therapy training or a dif-ferent control scheme. When body-powered control is provided, thesocket should be evaluated for maxi-mum range of motion to determineoptimal excursion. At the gleno-
humeral and associated levels, rangeof motion and associated excursionare often insufficient for effectivecontrol of a fully body-powered pros-thesis. This is even more problematicfor children and for people of slightbuild or with narrow shoulders.
Once the controls have been con-firmed, the components can bemounted and aligned. The locationand angles of abduction/adductionand internal rotation of the shoulderjoint should mirror the center of thecontralateral shoulder. With humeralneck–level amputations, the mechani-cal shoulder joint location may not beanatomic, to avoid creating a prosthe-sis with obvious shoulder asymmetry.For patients with cosmetic concerns,one solution is to mount the shoulderjoint inferior to the distal aspect ofthe humeral neck (Figure 13).
After all components have been at-tached and aligned, reliable control ofthe shoulder, elbow, wrist, and termi-nal device should be verified. Second-ary control options, including a re-mote on/off, shoulder lock, elbowunlock, and wrist rotation, requireanalysis of gross body movement andselection of appropriate input op-tions, often push- or pull-type
Figure 11 Perimeter Frame–type socket.A, Anterior view. B, Posterior view.
Figure 12 The prosthetist applies down-ward force to the humeral segment,demonstrating the stability achieved withthis infraclavicular socket design.
Chapter 21: Amputations About the Shoulder: Prosthetic Management 269
American Academy of Orthopaedic Surgeons
switches. Push switches can be acti-vated with the chin, with elevation ofthe acromial complex, or with move-ment of the humeral neck. Pullswitches are attached to the harnessand are activated by excursion of theharness. Verifying control isolation(after each control option is added)ensures that inadvertent activation ofa particular function does not occur.
Before creating the definitive pros-thesis, the prosthetist must determinethe socket material and thickness,frame color and composition, trim-lines, and mounting locations for sec-ondary control inputs. This is best ac-complished while the patient iswearing the diagnostic prosthesis. Theprosthesis is ready for final fabrica-tion when all issues of comfort, con-trol, function, cosmesis, and fabrica-tion have been thoroughly addressed.By following this protocol, few unan-ticipated issues will arise during thedelivery of the definitive prosthesis,and alterations should be minimal.
Postprosthetic PhaseProsthetic delivery is the culminationof much hard work by the patient andthe rehabilitation team and can bequite gratifying. Once the prosthesisis donned, the fit, function, and range
of motion should be assessed care-fully to ensure that accurate duplica-tion of the diagnostic prosthesis hasbeen achieved. Controls and adjust-ments should be verified to optimizefunction. This could include snuggingthe harness of a body-powered com-ponent or fine-tuning the electronicsfor a myoelectric device.
The patient’s perceptions are criti-cal to the process. A prosthesis thatmay appear to fit and function wellfrom the rehabilitation team’s per-spective will still not be successful if itdoes not meet the patient’s require-ments. For example, the harness mayseem too tight or the patient may feelthat too much effort is required orthat cosmetic issues have not been ad-equately addressed. Responding tosuch concerns with specific changesand involving the patient in thedecision-making process gives a senseof empowerment and increases thelikelihood of a positive long-termoutcome.
Another important responsibilityof the rehabilitation team is to helpthe patient develop realistic expecta-tions. When the definitive prosthesisis delivered, the patient must confrontthe limitations of a prosthesis. Eventhe best-designed prosthesis cannotreplace the function of a human arm.This can often be an emotional time,and access to a support network thatincludes a psychologist or counselor
is beneficial. This is especially truefor the glenohumeral-level amputeebecause the loss at this level is sosignificant.
Occupational therapy becomes thefocal point of the postprostheticphase. The goal of postprosthetictherapy should be the integration ofthe prosthesis into the patient’s life-style. The therapist begins with spe-cific controls training: flexing and po-sitioning the elbow, opening andclosing the terminal device, and supi-nating and pronating the wrist. Withguidance and practice, the patient willmaster these skills and then translatethem into task-specific activities.During this process, it is importantthat the therapist and prosthetistmaintain consistent communicationto ensure seamless rehabilitation. Of-ten the prosthesis requires minoradjustments as new tasks are under-taken or to address residual limb vol-ume changes. Care and maintenanceof the prosthesis, including cleaningthe prosthesis and personal hygiene,
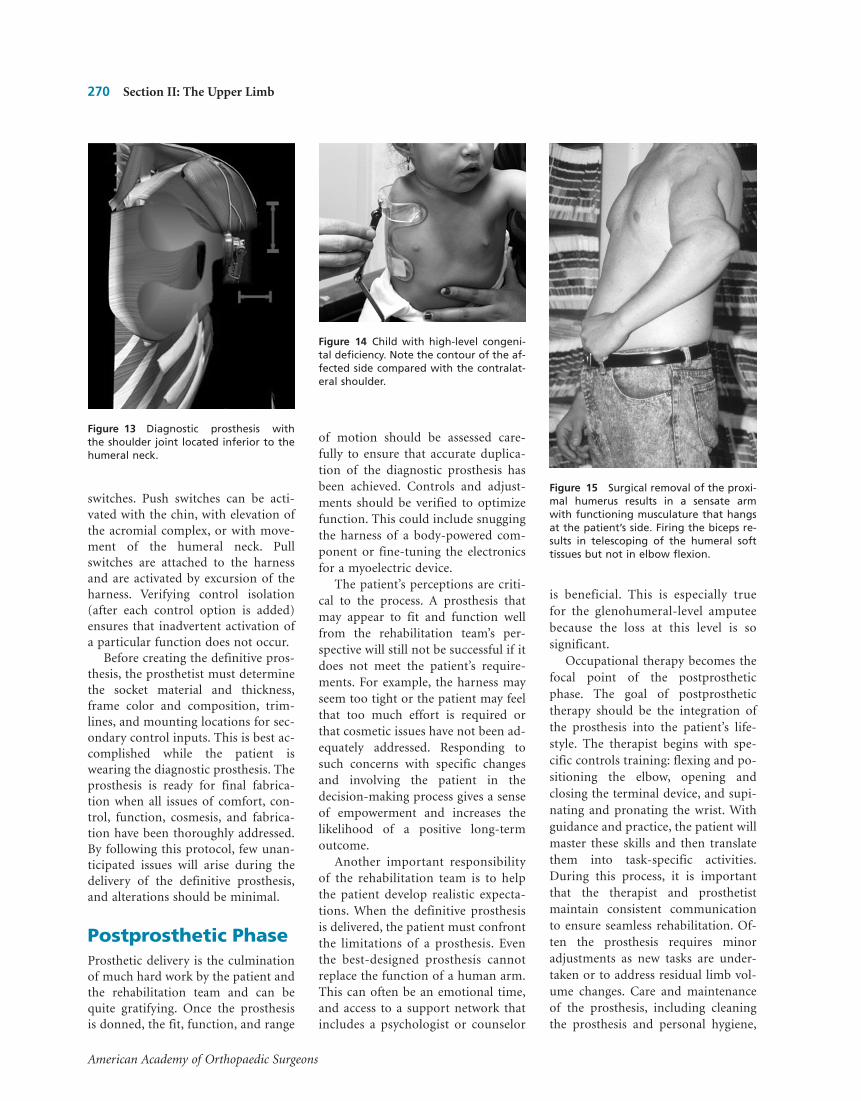
Figure 15 Surgical removal of the proxi-mal humerus results in a sensate armwith functioning musculature that hangsat the patient’s side. Firing the biceps re-sults in telescoping of the humeral softtissues but not in elbow flexion.
Figure 14 Child with high-level congeni-tal deficiency. Note the contour of the af-fected side compared with the contralat-eral shoulder.
Figure 13 Diagnostic prosthesis withthe shoulder joint located inferior to thehumeral neck.
270 Section II: The Upper Limb
American Academy of Orthopaedic Surgeons
should also be discussed. Finally, aspecific plan for long-term follow-upcare and component maintenanceshould be formulated.
SpecialConsiderationsCongenital AbsenceAcquired amputations and congenitalabsences at the glenohumeral levelhave distinct clinical presentationsthat affect prosthetic management dif-ferently. With congenital absence (Fig-ure 14), the clavicle and scapula areoften misshapen and may be fused.They are usually foreshortened, andthe lateral aspects are swept upward,creating a prominent and usually verymobile bony spur.18 The rest of theshoulder area is often fleshy and hasthe potential for weight support, butthe lack of bony structures often re-sults in problems with stability. Theshoulder profile drops away quitesharply from the bony point of theglenoid area, and a prosthetic shoul-der joint can be incorporated withoutcosmetic or technical difficulty.19
Intercalary AmputationsIntercalary amputations, which arerarely encountered, are extremelychallenging for the prosthetist-orthotist to manage. One example isthe Tikhoff-Linberg resection, wheremuch of the humerus is removed butthe balance of the upper limb remainssensate with intact musculature. It istempting to consider these patients ashaving a loss similar to a brachialplexus injury, but prosthetic solutionsthat are successful for brachial plexusinjuries often fail with this population.The overwhelming functional deficitis the complete loss of internal skeletalstability. As a consequence, when thepatient fires the elbow flexors, the armshortens but the forearm does notreach a horizontal position, as shownin Figure 15. Because the forces gener-ated by the upper arm musculature areconsiderable, it is virtually impossibleto create an external “prosthosis” thatwill prevent such telescoping from oc-curring.20 In addition, it is impossibleto carry even very light objects in thehand because the entire arm is con-nected to the torso only by soft tissues.
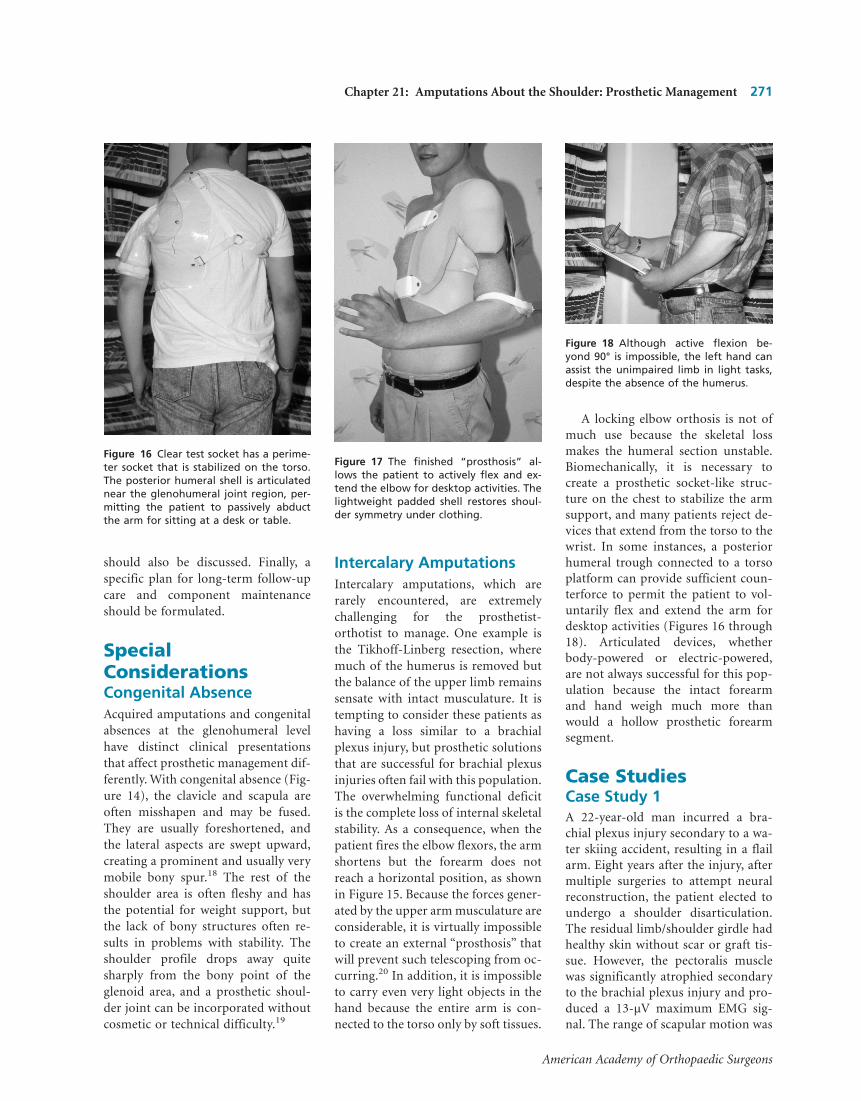
A locking elbow orthosis is not ofmuch use because the skeletal lossmakes the humeral section unstable.Biomechanically, it is necessary tocreate a prosthetic socket-like struc-ture on the chest to stabilize the armsupport, and many patients reject de-vices that extend from the torso to thewrist. In some instances, a posteriorhumeral trough connected to a torsoplatform can provide sufficient coun-terforce to permit the patient to vol-untarily flex and extend the arm fordesktop activities (Figures 16 through18). Articulated devices, whetherbody-powered or electric-powered,are not always successful for this pop-ulation because the intact forearmand hand weigh much more thanwould a hollow prosthetic forearmsegment.
Case StudiesCase Study 1A 22-year-old man incurred a bra-chial plexus injury secondary to a wa-ter skiing accident, resulting in a flailarm. Eight years after the injury, aftermultiple surgeries to attempt neuralreconstruction, the patient elected toundergo a shoulder disarticulation.The residual limb/shoulder girdle hadhealthy skin without scar or graft tis-sue. However, the pectoralis musclewas significantly atrophied secondaryto the brachial plexus injury and pro-duced a 13-µV maximum EMG sig-nal. The range of scapular motion was
Figure 16 Clear test socket has a perime-ter socket that is stabilized on the torso.The posterior humeral shell is articulatednear the glenohumeral joint region, per-mitting the patient to passively abductthe arm for sitting at a desk or table.
Figure 17 The finished “prosthosis” al-lows the patient to actively flex and ex-tend the elbow for desktop activities. Thelightweight padded shell restores shoul-der symmetry under clothing.
Figure 18 Although active flexion be-yond 90° is impossible, the left hand canassist the unimpaired limb in light tasks,despite the absence of the humerus.
Chapter 21: Amputations About the Shoulder: Prosthetic Management 271
American Academy of Orthopaedic Surgeons

extremely limited. The infraspinatusmuscle produced an EMG signal inexcess of 70 µV. The patient reportedoveruse of his surviving hand andwrist and had a strong interest inmaximum function with a good cos-metic appearance.
The patient was fitted with an infra-clavicular socket using myoelectriccontrol to operate an electric elbow,hand, and wrist rotator, plus switchcontrol of an electric locking shoulderjoint. The infraspinatus muscle sitewas used to proportionally control el-bow flexion and terminal device clos-ing, allowing precise positioning ofthe elbow and fingers. The weakerpectoralis muscle was used to providesingle-speed control of terminal de-vice opening. To decrease the weightof the prosthesis and reduce heatbuildup, the socket trimlines were ab-breviated and a window was cut infe-rior to the axilla. The resulting pros-thesis allowed the patient to performbimanual activities with a grip forcein excess of 20 lb. The forearm andhand were covered with a custom sili-cone synthetic skin to closely resem-ble the contralateral limb and to ad-dress the patient’s concerns regardingbody image (Figure 19).
Case Study 2A 39-year-old man presented 5 yearspostinjury with bilateral amputations(left side, transradial level; right side,humeral neck–level) secondary to anelectrical burn (Figure 20). The rightresidual limb/shoulder girdle exhib-ited minimal scar and graft tissue andgood range of motion and strength ofthe humeral neck. However, the leftside (transradial level) had extensivescar and graft tissue in the areas ofthe scapula, pectoralis, deltoid, andaxilla, which limited the ability to an-chor the control/suspension harnessfor the humeral neck–level prosthesisthrough the axilla region. The patienthad adequate EMG signals on bothresidual limbs, in excess of 80 µV. Theteam’s focus was on obtaining patientindependence, reducing prosthesisweight and heat buildup, increasinggrip force, enlarging the functionalenvelope, and limiting shear forces onthe scar and graft tissue.
On the right side (humeral neck–level), the patient was fitted with a hy-brid prosthesis that used myoelectriccontrol of electronic work hooks andwrist rotators, plus cable-operatedcontrol of an elbow with a forearmbalancing unit (Figure 21). The cable-operated elbow significantly reducedthe overall weight of the prosthesis.
The patient used ballistic body move-ments to flex the prosthetic elbow andhumeral neck abduction/flexion tocontrol the elbow locking mechanism,eliminating the need to route harnessstraps for elbow flexion across thefragile axilla region. The infraclavicu-lar socket permitted independentlocking of the cable-operated elbowbecause the humeral neck was notcontained within the socket.
The left side (transradial level) wasfitted with a self-suspending myo-electric prosthesis with an electronicwork hook and wrist rotator control.Myoelectric control offered enhancedgrip force and enlarged the functionalenvelope compared with the patient’sprevious body-powered prosthesis. Byusing a special donning aid incorpo-rating a weighted, extra-long lanyard,the patient learned to don the transra-dial prosthesis independently by usinghis legs and feet to manipulate the lan-yard. He then could use the transradialmyoelectric prosthesis to don theprosthesis on the opposite side. Theincreased grip force, larger functionalwork envelope, and independent don-ning characteristics of these prosthe-
Figure 19 Definitive myoelectric prosthe-sis for an individual with shoulder-levelbrachial plexus injury.
Figure 20 Individual with bilateral ampu-tations, at the humeral neck and at thetransradial level.
Figure 21 Definitive hybrid prosthesis foran individual with bilateral amputations,at the humeral neck and transradial level.Note the position of the shoulder joint
272 Section II: The Upper Limb
American Academy of Orthopaedic Surgeons

ses have allowed this patient to live in-dependently in the community.
SummaryRecent improvements in componentsand control options have achievedsuccessful prosthetic fitting of manyamputees with glenohumeral and as-sociated levels of loss. When body-powered components were the onlyavailable option, prosthetic fitting wasnot as successful. A comprehensiveand systematic approach, coordinatedby an experienced rehabilitation teamconsisting of a physician, physical andoccupational therapists, a psycholo-gist, a rehabilitation coordinator, anda prosthetist can improve long-termsuccess rates with these prostheses.The outcome is best when the patienthas a sense of control and active par-ticipation throughout the rehabilita-tion process. Verifying optimal fit andfunction of the diagnostic prosthesisbefore fabrication of the definitive de-vice has proved to be an effectivemethod to avoid costly modificationsthat can result in loss of confidencefor the patient.
AcknowledgmentThe authors would like to thank JohnW. Michael, MEd, CPO, for contribut-ing the section on fitting intercalaryamputations.
References1. Alley RD: The prosthetist’s evaluation
and planning process with the upperextremity amputee, in Atkins DJ,Meier RH (eds): Functional Restoration
of Adults and Children With Upper Ex-tremity Amputation. New York, NY,Demos, 2004, pp 125-126.
2. Reddy M: Nerve entrapment syn-drome in upper extremity contralat-eral to amputation. Arch Phys MedRehabil 1984;65:24-26.
3. Mckenzie DS: Powered prosthesis forchildren: Clinical considerations.Prosthet Int 1967;3(2/3):5-7.
4. Alley RD, Miguelez JM: Prostheticrehabilitation of glenohumeral leveldeficiencies, in Atkins DJ, Meier RH(eds): Functional Restoration of Adultsand Children With Upper ExtremityAmputation. New York, NY, Demos,2004, pp 244-250.
5. Atkins D: Adult upper-limb prosthetictraining, in Atkins DJ, Meier RH (eds):Comprehensive Management of the Up-per Limb Amputee. New York, NY,Springer-Verlag, 1989, p 58.
6. Canelon MF: Training for a patientwith shoulder disarticulation. Am JOccup Ther 1993;47:174-178.
7. Brooks MA, Dennis JF: Shoulder dis-articulation type prostheses for bilat-eral upper extremity amputees. InterClin Info Bull 1963;2:1-7.
8. Neff GG: Prosthetic principles inshoulder disarticulation for bilateralamelia. Prosthet Orthot Int 1978;2:143-147.
9. Wright TW, Hagen AD, Wood MB:Prosthetic usage in upper extremityamputations. J Hand Surg Am 1995;20:619-622.
10. Neff G: Prosthetic principles in bilat-eral shoulder disarticulation or bilat-eral amelia. Prosthet Orthot Int 1978;2:143-147.
11. Mongeau M, Madon S: Abstract: Eval-uation prosthetic fitting of 13 shoul-der disarticulation clients since 2years. J Assoc Child Prosthet Orthot Clin1990;25:26.
12. Sears HH, Andrew JT, Jacobsen SC:Experience with the Utah arm, hand,and terminal device, in Atkins DJ,Meier RH (eds): Comprehensive Man-agement of the Upper Limb Amputee.New York, NY, Springer-Verlag, 1989,pp 200-201
13. Alley RD, Sears HH: Powered upperlimb prosthetics in adults, in Muzum-dar A (ed): Powered Upper Limb Pros-theses. Berlin, Springer-Verlag, 2004,pp 133-138.
14. Miguelez J, Miguelez M: The Micro-Frame: The next generation of inter-face design for glenohumeral disartic-ulation and associated levels of limbdeficiency. J Prosthet Orthotics 2003;15:66-71.
15. Daly W: Upper extremity socket de-signs. Phys Med Rehabil Clin North Am2000;11:627-638.
16. Heger H, Millstein S, Hunter G:Electrically-powered prostheses for theadult with an upper limb amputation.J Bone Joint Surg Br 1985;67:278-281.
17. Stern P, Lauko T: A myoelectricallycontrolled prosthesis using remotemuscle sites. Inter Clinic Info Bull 1973;12:1-4.
18. Hall C, Bechtol CO: Modern amputa-tion technique in the upper extremity.J Bone Joint Surg 1963;450:1717-1722.
19. Cooper R: Prosthetic principles, inBowker JD, Michael JW: Atlas of LimbProsthetics: Surgical, Prosthetic, andRehabilitation Principles. Rosemont, IL,American Academy of OrthopaedicSurgeons, 2002, pp 271-275. (Origi-nally published by Mosby-Year Book,1992)
20. Ham SF, Eisma WJ, Schraffordt KoopsH, Oldhoff J: The Tikhoff-Linbergprocedure in the treatment of sarco-mas of the shoulder girdle. J SurgOncol 1993;53:71-77.
Chapter 21: Amputations About the Shoulder: Prosthetic Management 273
American Academy of Orthopaedic Surgeons
