client registration packet peds - familypath autism …€¦ · · 2015-07-09microsoft word -...
TRANSCRIPT
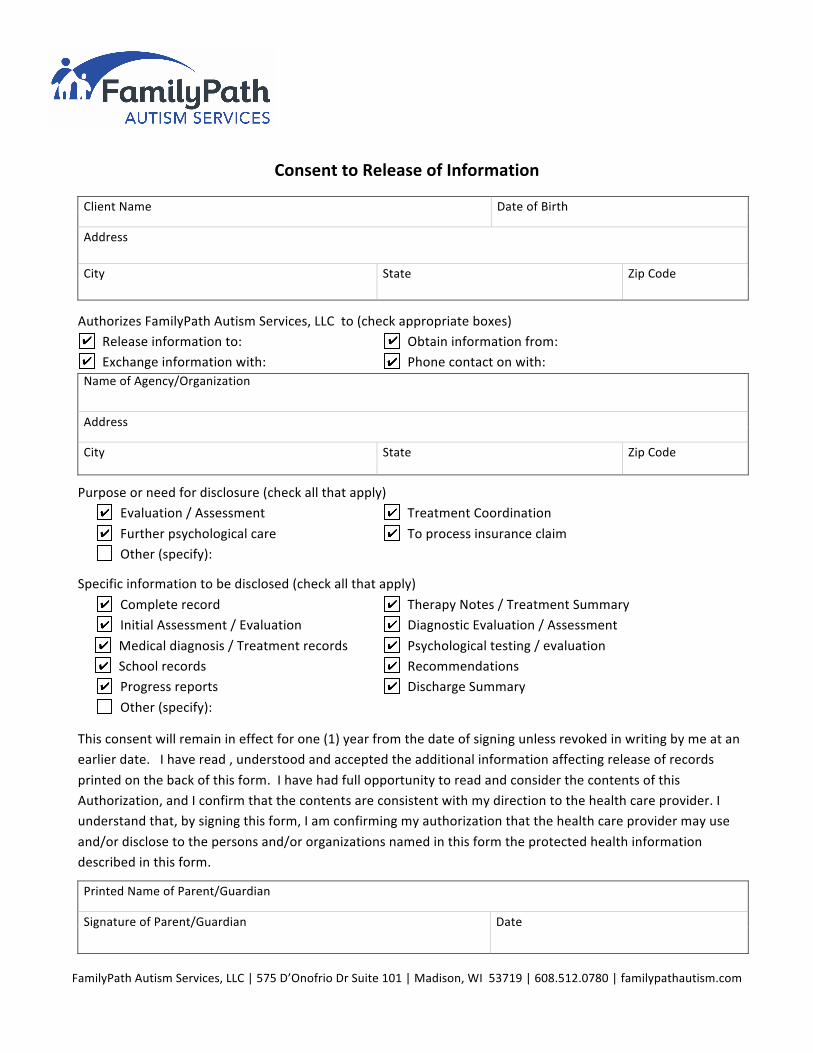
FamilyPath Autism Services, LLC | 575 D’Onofrio Dr Suite 101 | Madison, WI 53719 | 608.512.0780 | familypathautism.com
Consent to Release of Information
Client Name Date of Birth
Address
City State Zip Code
Authorizes FamilyPath Autism Services, LLC to (check appropriate boxes) Release information to: Obtain information from: Exchange information with: Phone contact on with:
Name of Agency/Organization
Address
City State Zip Code
Purpose or need for disclosure (check all that apply) Evaluation / Assessment Treatment Coordination
Further psychological care To process insurance claim Other (specify):
Specific information to be disclosed (check all that apply)
Complete record Therapy Notes / Treatment Summary Initial Assessment / Evaluation Diagnostic Evaluation / Assessment
Medical diagnosis / Treatment records Psychological testing / evaluation School records Recommendations Progress reports Discharge Summary
Other (specify):
This consent will remain in effect for one (1) year from the date of signing unless revoked in writing by me at an earlier date. I have read , understood and accepted the additional information affecting release of records
printed on the back of this form. I have had full opportunity to read and consider the contents of this Authorization, and I confirm that the contents are consistent with my direction to the health care provider. I understand that, by signing this form, I am confirming my authorization that the health care provider may use
and/or disclose to the persons and/or organizations named in this form the protected health information described in this form.
Printed Name of Parent/Guardian
Signature of Parent/Guardian Date