clinical aspect of dlmi bm orning blood pressure...
TRANSCRIPT

Clinical Aspect of Clinical Aspect of Clinical Aspect of Clinical Aspect of M i Bl d M i Bl d Morning Blood Morning Blood Pressure SurgePressure Surgegg
Eung Ju Kim Eung Ju Kim
Korea University Guro Hospital Korea University Guro Hospital Cardiovascular CenterCardiovascular CenterCardiovascular CenterCardiovascular Center
Seoul, KoreaSeoul, Korea


Ci di Rh thCi di Rh thCircadian RhythmCircadian Rhythm
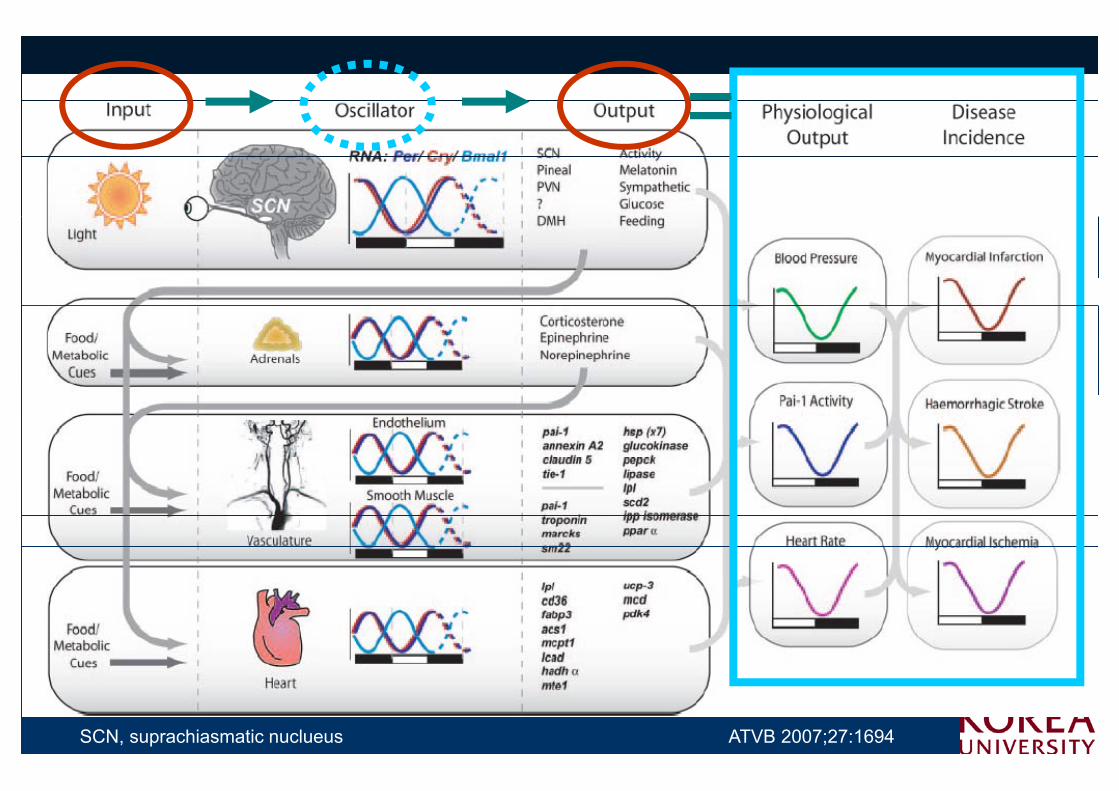
DailyDaily cyclescycles ofof physiologyphysiology andandbehaviorbehavior thatthat areare drivendriven byby ananendogenousendogenous oscillatoroscillator withwith aa periodperiodendogenousendogenous oscillatoroscillator withwith aa periodperiodofof approximatelyapproximately ((circacirca--)) oneone dayday((diesdies oror diemdiem))..
=
SCN, suprachiasmatic nuclueus ATVB 2007;27:1694
CV or hemodynamic parameters y psuch as HR, BP, endothelial HR, BP, endothelial , ,, ,functionfunction, and fibrinolytic activityfibrinolytic activityexhibit variations consistent with circadian rhythmcircadian rhythm.

Diurnal Variation of BPDiurnal Variation of BPDiurnal Variation of BPDiurnal Variation of BPTi f
g)
Time of awakening
Sleep180
(mm
H 160
essu
re ( 140
120
ood p
re 120
100
Blo
18:00 22:00 02:00 06:00 10:00 14:00 18:0080
Time of day
18:00 22:00 02:00 06:00 10:00 14:00 18:00
Lancet 1978;1(8068):795–797Circ Res 1983;53:96–104

EEarly arly MMorning orning BPBP SSurgeurgeEEarly arly MMorning orning BPBP SSurgeurge
MorningMorning
Untreated hypertensives Normotensives200
mH
g)
Systolic (mean+S E )150
ssure
(m
m Systolic (mean+S.E.)
100
Blo
od p
re
9 12 15 18 21 24 3 6 9 9 12 15 18 21 24 3 6 9
50 Diastolic (mean+S.E.)
9 12 15 18 21 24 3 6 9 9 12 15 18 21 24 3 6 9
Time of day (hours) Time of day (hours)
Lancet 1978;1:795–797
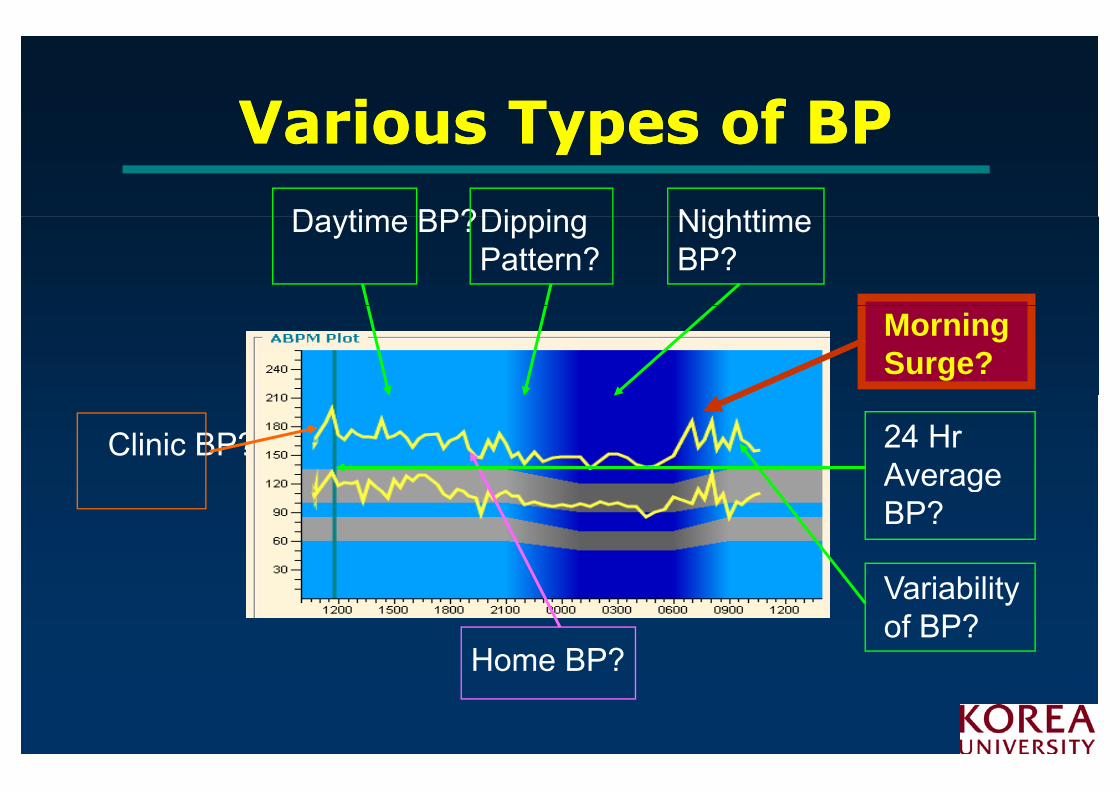
Various Types of BPVarious Types of BPVarious Types of BPVarious Types of BP
Daytime BP? NighttimeDippingDaytime BP? Nighttime BP?
Dipping Pattern?
Morning Surge?
Clinic BP? 24 Hr AverageAverage BP?
Home BP?
Variability of BP?
Home BP?

DefinitionDefinitionDefinitionDefinitionThereThere isis nono universallyuniversally recognizedrecognized definitiondefinition ofofThereThere isis nono universallyuniversally recognizedrecognized definitiondefinition ofofthethe morningmorning surgesurge
Kario et al. Circulation 2003;107:1401
Leary et al J HTNLeary et al. J HTN 2002;20:865
4Hr4Hr 4Hr4Hr

Morning BP SurgeMorning BP SurgeMorning BP Surge Morning BP Surge & Subclinical& Subclinical& Subclinical & Subclinical Organ DamageOrgan DamageOrgan DamageOrgan Damage

MBPS Causes TODMBPS Causes TOD
► MBPS hemodynamic stress TOD► MBPS hemodynamic stress TOD
►High MBPS more likely to have LVH►High MBPS more likely to have LVH
►BP in the morning is a better predictor than office BP►BP in the morning is a better predictor than office BPof:
– the decline in GFR
albuminuria in patients with type 1 diabetes– albuminuria in patients with type 1 diabetes
– albuminuria in patients with type 2 diabetes
11
J Hypertens 2004;22:1113–1118Clin Exp Hypertens 2002;24:249–260
Diabetes Care 2002;25:2218–2223Diabetes Care 2003;26:2473–2475

Early Morning Attenuation of Early Morning Attenuation of y gy gEndothelialEndothelial Function in Function in
H lth HH lth HHealthy HumansHealthy Humans
Circulation 2004;109:2507–2510

Morning BP Surge or Morning BP Surge or Morning BP Surge or Morning BP Surge or Reactivity and LVHReactivity and LVH
MBPR
= MBPS /
(sum of 2-h activity(sum of 2 h activity after arising)0.5
Am J Hypertens 2005;18:1528–1533

Morning BP HyperMorning BP Hyper--Reactivity Reactivity Morning BP HyperMorning BP Hyper Reactivity Reactivity and LVHand LVH
M i BP R ti itM i BP R ti itMorning BP ReactivityMorning BP Reactivity was independentlyindependently associated with
cardiac h pertrophcardiac h pertrophAm J Hypertens 2005;18:1528–1533
cardiac hypertrophycardiac hypertrophy

MMorning orning BP BP is a is a BBetter etter PPredictor redictor hh Cli iCli i ff lb i i ilb i i ithan than Clinic BPClinic BP ofof AAlbuminuria in lbuminuria in
TType 2ype 2 DMDMTType 2ype 2 DMDM
Sens 100%Sens 49%
Specificity 75%Specificity 68%
Specificity 75%
Sens 18%
Specificity 85%
Sens 43%
Specificity 73%
Threshold 135mmHg Threshold 85mmHg
Diabetes Care 2002;25:2218–2223

CV Events OccurCV Events OccurCV Events OccurCV Events OccurMore FrequentlyMore FrequentlyMore FrequentlyMore FrequentlyIn the Morning !In the Morning !In the Morning !In the Morning !

The Early Morning BP SurgeThe Early Morning BP SurgeCoincides with peak time of cardiovascular complications
►Sudden death
Coincides with peak time of cardiovascular complications
►Acute myocardial infarction
►Typical angina pectorisy g
►Silent ischemia
►T t l i h i b d06:00-12:00
►Total ischemic burden
►Ischemic stroke
►Variant angina pectoris (02:00-04:00)
►Platelet aggregability17
►Platelet aggregabilityLancet. 1988;2:755–759; Am Heart J. 1989;118:1098–1099;
Stroke. 1989;20:473–476; Circulation. 1989;80:1617–1626; Ter Arkh 2000;72:47–51
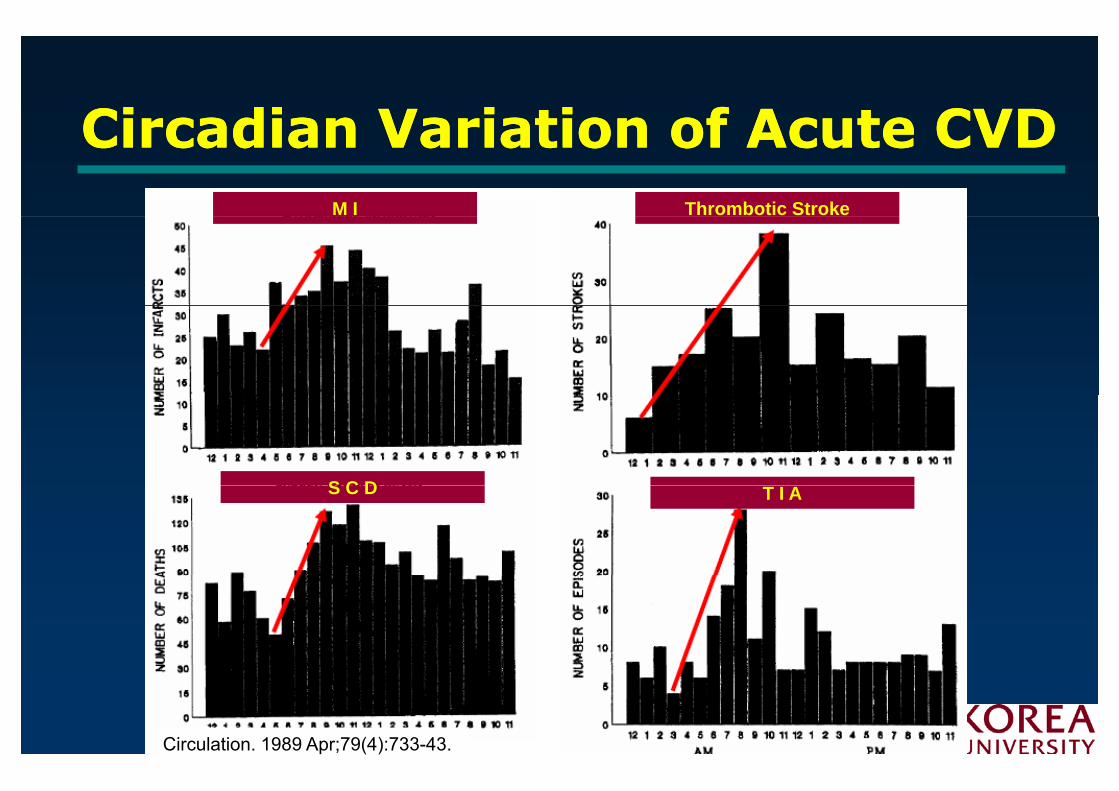
Circadian Variation of Acute CVDCircadian Variation of Acute CVDCircadian Variation of Acute CVDCircadian Variation of Acute CVDM I Thrombotic Stroke
S C D T I AS C D
Circulation. 1989 Apr;79(4):733-43.

Circadian Patterns of Onset Circadian Patterns of Onset of Symptoms of Stroke of Symptoms of Stroke
A: all
B IschemicB: Ischemic
C: Hemorrhagic
D: TIA
Stroke. 1998 May;29(5):992-6

Morning Excess of AMI and Morning Excess of AMI and Morning Excess of AMI and Morning Excess of AMI and Sudden Cardiac Death Sudden Cardiac Death
Am J Cardiol. 1997 Jun 1;79(11):1512-6

Morning Peak of VT Morning Peak of VT Morning Peak of VT Morning Peak of VT Detected by ICDDetected by ICD
120
80
100
E i d60
80Episodes
of VT
20
40
00 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Circulation 1995;92: 1203

Morning BP SurgeMorning BP SurgeMorning BP SurgeMorning BP Surgeis Independentlyis Independentlyis Independentlyis Independently
Associated WithAssociated WithAssociated With…Associated With…

MBPS is Independently Associated MBPS is Independently Associated MBPS is Independently Associated MBPS is Independently Associated With CV ComplicationsWith CV Complications
• Baseline• Baseline
: Untreated 507 HTN
• Then treated
• Mean 7yr f/uM lti i t l i Mean 7yr f/uMultivariate analysis
SBP change on rising
• CV Cx: MI, Angina, CVA, SCD, CRF, HF, PAD, AAA, Carotid stenosis
Journal of Hypertension 2004, 22:1113–1118

MBPS is Independently MBPS is Independently MBPS is Independently MBPS is Independently Associated With StrokeAssociated With Stroke
519 ld HTN• 519 older HTN
• Mean 41mo f/u
22-25% /
f f 2 S
10mmHg
Circulation. 2003;107:1401-1406
After controlling for age, sex, BMI, 24h SBP

WhWhWhy Why yyM i S ?M i S ?Morning Surge ?Morning Surge ?g gg g

MBPS MBPS –– CV Events ; MechanismCV Events ; MechanismVascularMBPS MBPS CV Events ; MechanismCV Events ; Mechanism
SteepSteep BPBP surgesurge
Vascular RemodelingSteepSteep BPBP surgesurgeRemodeling Cardiac
↑↑ oscillatoryoscillatory shearshear stressstress inin vesselvessel wallwallRemodeling↑↑ t i lt i l tifftiff
RemodelingOther CV ↑↑ arterialarterial stiffnessstiffness↑↑ IMTIMT ++ ααRisk Factors CV ↑↑ IMTIMT ++ αα↑↑ LVHLVH
Risk Factors ↑ in Morning Events !↑↑↑ in Morning Events !


MBPS MBPS O id ti StO id ti StMBPS MBPS –– Oxidative StressOxidative Stress
HTN
From PMN
N= 31 O
SFrom
RO
MNC
Hypertens Res 2005;28:755-761

in Carotid Plaque of MBPSin Carotid Plaque of MBPS
Hypertension 2007;49:784-791 HypertensivesHypertensives

↑↑ UP in Carotid Plaque of MBPSUP in Carotid Plaque of MBPS
Hypertension 2007;49:784-791 HypertensivesHypertensives

Circadian Variation of PAICircadian Variation of PAI--1 1 and tPA Activities and tPA Activities
J Am Coll Cardiol, 1998; 32:1962-1968

TherapeuticTherapeuticTherapeutic Therapeutic Strategies toStrategies toStrategies to Strategies to
Control MBPSControl MBPSControl MBPSControl MBPS

Hypertension Hypertension AAwareness, wareness, Hypertension Hypertension AAwareness, wareness, TTreatment and reatment and CControlontrol
7 0
8 0 U S AC a n a d aI t a l yS w e d e n
5 0
6 0
%)
S w e d e nS p a i nE n g l a n dG e r m a n y
Poor rates of control* in western countries
3 0
4 0
idu
als
(%
1 0
2 0
Ind
ivi
0A w a r e T r e a t e d C o n t r o l l e dAware Treated Controlled
Wolf-Maier et al. Hypertension 2004;43:10–17* Threshold of SBP/DBP 140/90 mm Hg
Aware Treated Controlled

In Pts with Controlled Office BP; Also During Morning Hours ?
70
Controlled (morning < 135/85mmHg)
Not controlled
50
60
)
30
40
ients
(%
)
20
30
Pati
0
10
34
ACAMPA study J-MORE
Redón et al. Blood Press Monit 2002;7:111–116Kario et al. Circulation 2003;108:72e–73e

Early Morning BP Surge as a Early Morning BP Surge as a Early Morning BP Surge as a Early Morning BP Surge as a Target for TherapyTarget for Therapy
Consider…Consider…
Pharmacokinetic profile with Pharmacokinetic profile with morning dosingmorning dosingmorning dosing morning dosing
Underlying mechanisms for MBPSUnderlying mechanisms for MBPS

A Therapeutic Blind Spot With A Therapeutic Blind Spot With A Therapeutic Blind Spot With A Therapeutic Blind Spot With Current Therapy in the MorningCurrent Therapy in the Morning
OneOne ofof thethe suggestedsuggested reasonreasonss forfor morningmorningOneOne ofof thethe suggestedsuggested reasonreasonss forfor morningmorninghypertensionhypertension inin treatedtreated subjectssubjects..
InsufficientInsufficient durationduration ofof actionaction (short(short TT11//22))ofof antihyertensiveantihyertensive drugsdrugs leavingleaving patientspatientsofof antihyertensiveantihyertensive drugs,drugs, leavingleaving patientspatientsvulnerablevulnerable..

Ch th ti T St t iCh th ti T St t iChronotherapeutic Tx StrategiesChronotherapeutic Tx Strategies
ChooseChoose drugdrug withwith longlong halfhalf--lifelife withwith highhightroughtrough--toto--peakpeak ratiosratios,, ensuringensuring coveragecoverageduringduring thethe morningmorning surgesurgegg gg ggExtendedExtended--release,release, delayeddelayed--onset,onset, bedtimebedtimedosingdosingdosingdosingTwiceTwice dailydaily dosesdosesCoupledCoupled withwith aa diureticdiuretic

HalfHalf--lives of Various Blood lives of Various Blood HalfHalf lives of Various Blood lives of Various Blood Pressure MedicationsPressure Medications
403 5
4 04
3 0
3 5
242 0
2 5
Hou
rs
129
1 0
1 5H
1 96 5 20
5
A m l o T e l m i L i s i n o C a n d e V a l s a r V e r a p a L o s a rA m l o T e l m i L i s i n o C a n d e V a l s a r V e r a p a L o s a r
J Clin Hypertens 2008;10:140-145

Effects of Two ARBs Approved for Effects of Two ARBs Approved for Effects of Two ARBs Approved for Effects of Two ARBs Approved for Once Daily Dosing on 24 Hour BPOnce Daily Dosing on 24 Hour BP
Missed Dose
Mancia et al AJC 1999: 84; 28SMancia et al AJC 1999: 84; 28S

Duration of Action by Duration of Action by yyTrough:Peak RatioTrough:Peak Ratio
46
Placebo
202
T h
Blood Pressure Ch
Placebo
- 6- 4- 2
P k
TroughChange mmHg
1 2- 1 0
- 8 PeakDrug
- 1 4- 1 2
0 Hours after dosing 240 Hours after dosing 24

Effects of Time of Administration Effects of Time of Administration Effects of Time of Administration Effects of Time of Administration on Diurnal Changes of BPon Diurnal Changes of BP
- 1
0D a y N ig h t 2 4 h o u r
3
- 2
1 y g
Change
of
5
- 4
- 3
0 . 5 m g b id1 m g q d
of
SBP, mmHg
7
- 6
- 5 1 m g q dmmHg
- 8
- 7
- 9
Poirier J Clin Pharm 1993: 33:832Poirier J Clin Pharm 1993: 33:832TrandolaprilTrandolapril

Adherence to Treatment Greater with Once-daily Dosing
1 0 0 1 0 0 ****8 0
9 0
1 0 0
8 0
9 0
1 0 0 ****
6 0
7 0
%) 6 0
7 0
%)
3 0
4 0
5 0
eren
ce (
%
3 0
4 0
5 0
eren
ce (
%1 0
2 0
3 0
Ad
h
1 0
2 0
3 0
Ad
h0
O n c e - d a i l y T w i c e - d a i l y0
O n c e - d a i l y M u l t i p l e d a i l yd o s e s
OD BID OD MultipleClin Ther 2002;24:302–316
d o s e s* P<0.05 vs twice-daily dosing*** P<0.001 vs multiple daily doses
p

Targeting Mechanisms Targeting Mechanisms Targeting Mechanisms Targeting Mechanisms Responsible for MBPSResponsible for MBPS
SympatheticSympathetic NervousNervous SystemSystem↑ Morning BP surge ↑ Morning BP surge Platelet hyperactivationPlatelet hyperactivationPlatelet hyperactivationPlatelet hyperactivationEndothelial cell dysfunctionEndothelial cell dysfunction↑ Bl d i it↑ Bl d i it↑ Blood viscosity↑ Blood viscosity
ReninRenin--AngiotensinAngiotensin--AldosteroneAldosterone SystemSystem↑ Morning BP surge↑ Morning BP surge↑ Morning BP surge↑ Morning BP surge
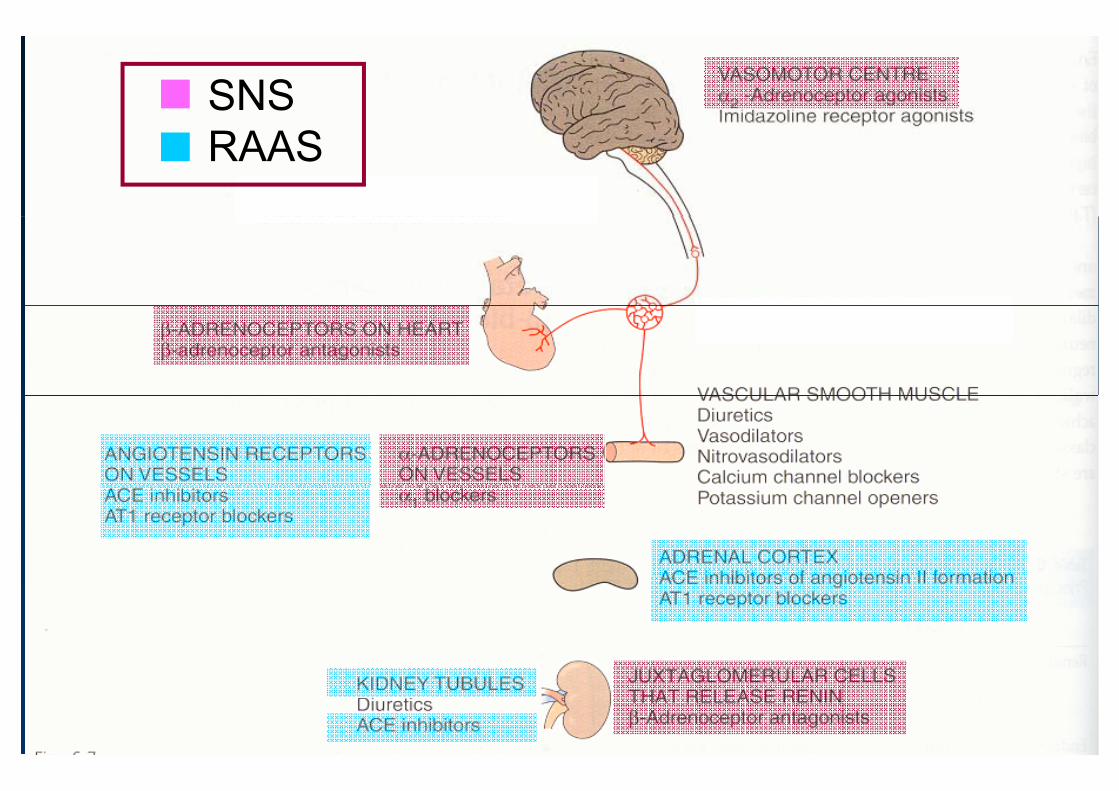
SNS RAAS

Effects of Effects of αα--Blockade on the Blockade on the Effects of Effects of αα Blockade on the Blockade on the Morning Surge of BPMorning Surge of BP
No Rx
Doxazosin
DosingDosing
Kario, Pickering, et al Am J Hypertens 2004;17; 668Kario, Pickering, et al Am J Hypertens 2004;17; 668

Effects of Bedtime Dosing of Effects of Bedtime Dosing of C t ll A ti C t ll A ti 22 i t i t Centrally Acting Centrally Acting αα22--agonists agonists
on Morning HTNon Morning HTNon Morning HTNon Morning HTNGuanabenz
morningmorning
Cl idievening Clonidineevening
U f l f th i hibit ti &/ fUsefulness of sympathoinhibitory action, &/or of night-time dosing in controlling Morning HTN
J HTN 2003;21:805-811
g g g g

Regression of Carotid Regression of Carotid Atherosclerosis by Controlling Atherosclerosis by Controlling
Morning BP by Morning BP by αα1/ß Antagonist1/ß AntagonistMorning BP by Morning BP by αα1/ß Antagonist1/ß Antagonist
Cli i D Ni ht M i C tid IMT
5
0 0
Clinic Day Night Morning Carotid IMT
0
SBP
-10
-5-0.01
SBP mmHg IMT
mm
20
-15 -0.02-0.02NS
NS
-25
-20
MetoprololCarvedilol
-0.03
NS
<0 001<0.02
-30 -0.04-0.04<0.001
Marfella et al, Am J Hypertens 2005: 18: 308Marfella et al, Am J Hypertens 2005: 18: 308

CYT006CYT006--AngQb, a Vaccine Against AngQb, a Vaccine Against Hypertension Targeting Hypertension Targeting Hypertension Targeting Hypertension Targeting
Angiotensin IIAngiotensin IIgg
Lancet 2008;371:821-827

Change of Daytime BPChange of Daytime BPChange of Daytime BPChange of Daytime BP(week 14 vs. Baseline(week 14 vs. Baseline))
Lancet 2008;371:821-827

24h BP P fil t W k 1424h BP P fil t W k 1424hr BP Profile at Week 1424hr BP Profile at Week 14
Lancet 2008;371:821-827

Change of Early Morning BPChange of Early Morning BPChange of Early Morning BPChange of Early Morning BP(week 14 vs. Baseline. 300(week 14 vs. Baseline. 300µg CYT006µg CYT006--AngQb)AngQb)
DBPDBPDBPDBP
SBPSBP
Usefulness of RAAS-inhibitory action, &/or of l T1/2 i t lli M i HTN
Lancet 2008;371:821-827
long T1/2 in controlling Morning HTN

S (I)S (I)Summary (I)Summary (I)
There is a pronounced diurnal rhythm of BP and CV BP and CV eventsevents, with a peakpeak of both in the morning morning hours, and a decrease during the night. DrugsDrugs approved for once daily dose may haveDrugsDrugs approved for once daily dose may have different durations of actiondifferent durations of action, particularly after missed dosesmissed doses.With some antihypertensive drugs the time of dosingtime of dosingmay have significant effects on the diurnal pattern of BP.

S (II)S (II)Summary (II)Summary (II)
Inhibition of SNS or RAASInhibition of SNS or RAAS may be useful for may be useful for controlling MBPScontrolling MBPSggDifferent antihypertensive drugsDifferent antihypertensive drugs may have different effects on the morningdifferent effects on the morning surge of BPdifferent effects on the morningdifferent effects on the morning surge of BP.

C l iC l iConclusionsConclusions
Morning BP surge is an independent risk for Morning BP surge is an independent risk for advancing the atherosclerosis process , TOD advancing the atherosclerosis process , TOD g p ,g p ,and triggering CV events.and triggering CV events.
In addition to strict BP control, In addition to strict BP control, antihypertensive therapy targeting MBPS antihypertensive therapy targeting MBPS could achieve more beneficial effect forcould achieve more beneficial effect forcould achieve more beneficial effect for could achieve more beneficial effect for prevention of CV disease in highprevention of CV disease in high--risk risk hypertensive patientshypertensive patientshypertensive patients.hypertensive patients.

KOALA SymposiumKOALA SymposiumKOALA SymposiumKOALA Symposium

Thank you Thank you Thank you Thank you for your for your for your for your
attention !attention !attention !attention !



Factors Influencing Morning SurgeFactors Influencing Morning SurgeFactors Influencing Morning SurgeFactors Influencing Morning Surge
Brain Sympathetic system
Aging Renin-angiotensin system
Clock gene
Stress
HPA axis
Nitric oxidesStress
Cold temp
Nitric oxides
Cold temp
Morning BPMorning BP

Factors Influencing Exaggerated Morning SurgeFactors Influencing Exaggerated Morning SurgeFactors Influencing Exaggerated Morning SurgeFactors Influencing Exaggerated Morning Surge
AgeAge (( >> 7070 yr)yr)AfricanAfrican--AmericanAmerican EthnicityEthnicityDayDay ofof weekweek (Mon)(Mon) // SeasonSeason ofof yearyear (Winter)(Winter)DayDay ofof weekweek (Mon)(Mon) // SeasonSeason ofof yearyear (Winter)(Winter)TobaccoTobacco // AlcoholAlcohol useuseSodiumSodium // CaffeineCaffeine // MedicationMedication (e(e..gg.. oraloralcontraceptives)contraceptives)contraceptives)contraceptives)

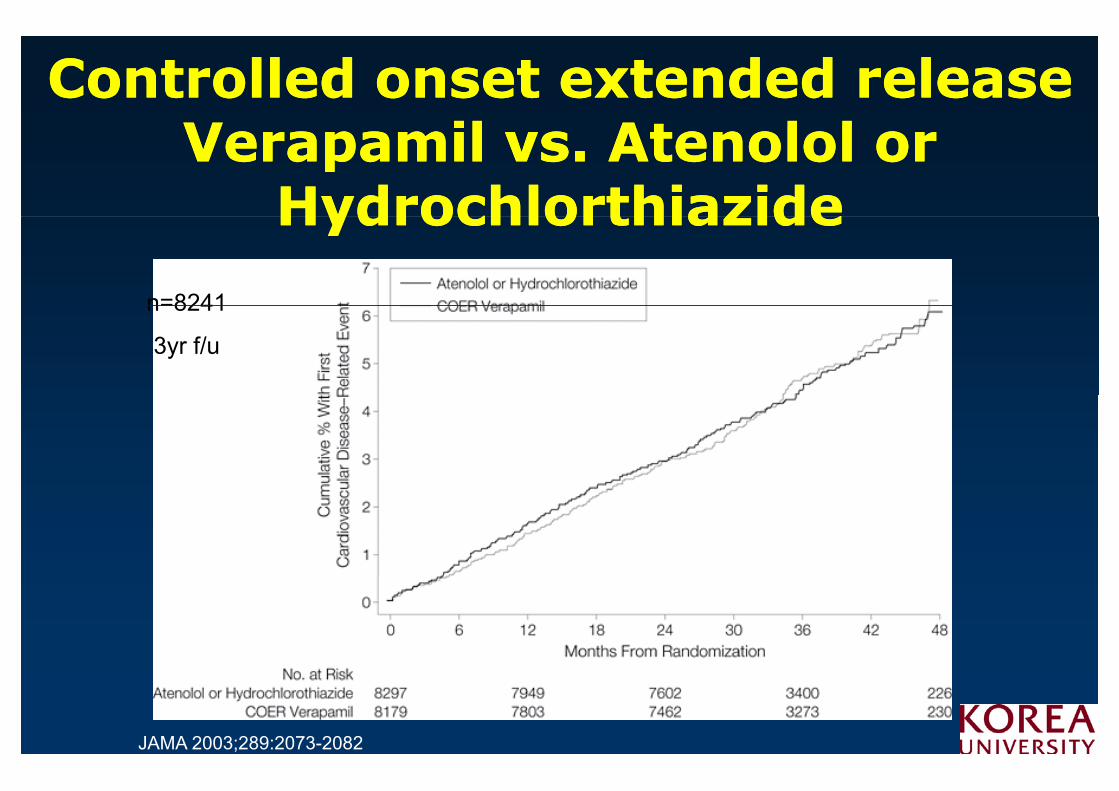
Controlled onset extended release Controlled onset extended release V il At l l V il At l l Verapamil vs. Atenolol or Verapamil vs. Atenolol or
HydrochlorthiazideHydrochlorthiazideHydrochlorthiazideHydrochlorthiazide
n=8241n 8241
3yr f/u
JAMA 2003;289:2073-2082

Reducing targetReducing target--organ damageorgan damageMean arterial pressure (mmHg)
Reduced blood pressure slows the rate of GFR decline
95 98 101 104 107 110 113 116 1190
r = 0.69; P < 0.05
min
/yea
r) -2
-4
GFR
(m
L/m
Untreated
-6
8
eclin
e in
G hypertension-8
-10
De
130/85 140/90-12
-14-14
Bakris et al. Am J Kidney Dis 2000;36:646–661

M i BP SM i BP SMorning BP Surge Morning BP Surge g gg g& CV E t& CV E t& CV Events& CV Events

TargetTarget--organ organ DDamage amage IIncreases ncreases CCardiovascular ardiovascular IIncreases ncreases CCardiovascular ardiovascular
RRiskiskEndothelial dysfunction
EEndotheliumndothelium playsplays aa keykey rolerole inin controllingcontrollingperipheralperipheral arteriolararteriolar resistanceresistance
y
peripheralperipheral arteriolararteriolar resistanceresistanceEndothelialEndothelial dysfunctiondysfunction cancan bebe observedobserved asasyyanan inapropriateinapropriate responseresponse totovasodilators/vasoconstrictorsvasodilators/vasoconstrictorsvasodilators/vasoconstrictorsvasodilators/vasoconstrictors
Nitric oxide is a key endogenous vasodilatorNitric oxide is a key endogenous vasodilatorNitric oxide is a key endogenous vasodilatorNitric oxide is a key endogenous vasodilatorItIt isis oneone ofof thethe earliestearliest markersmarkers forfor targettarget--organorgan damagedamageItIt contributescontributes toto cardiovascularcardiovascular disordersdisorders
Klahr, Morrissey. Kidney Int Suppl 2000;75:S7–S14
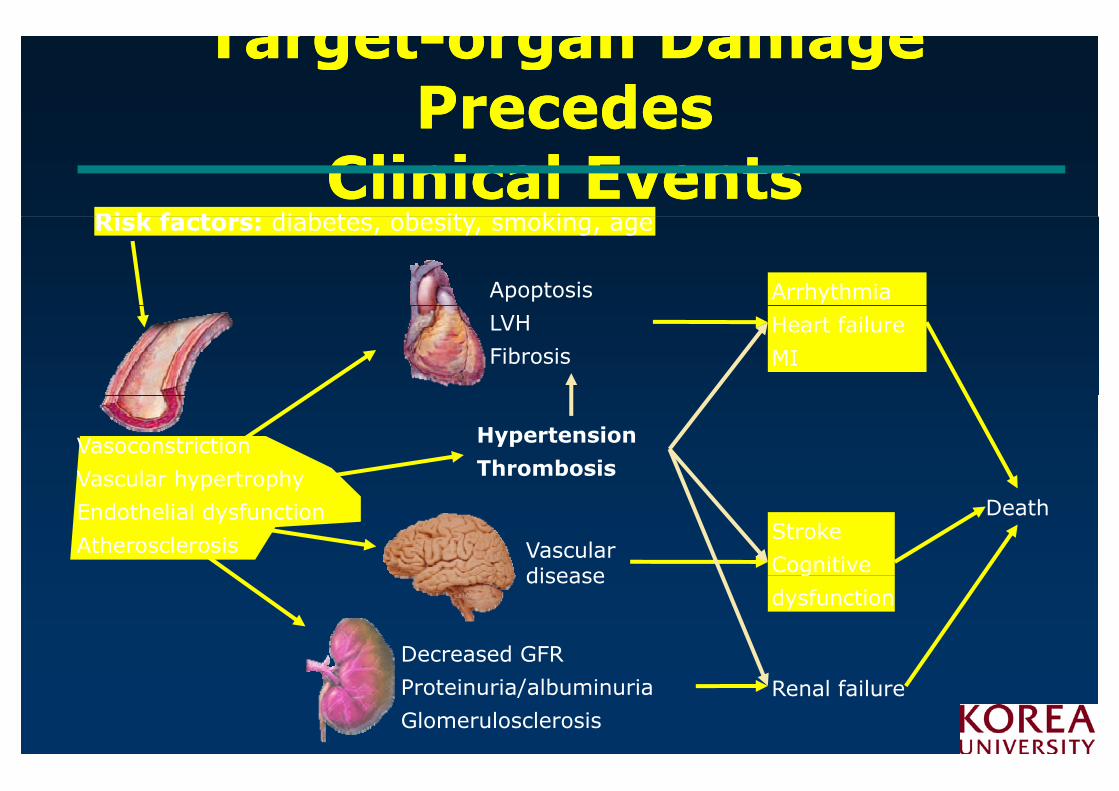
TargetTarget--organ Damage organ Damage Precedes Precedes Precedes Precedes
Clinical EventsClinical EventsRi k f t di b t b it ki
Apoptosis Arrhythmia
Risk factors: diabetes, obesity, smoking, age
LVH
FibrosisHeart failure
MI
Vasoconstriction
Vascular hypertrophy
Hypertension
ThrombosisVascular hypertrophy
Endothelial dysfunction
Atherosclerosis
DeathStroke
Cognitive Vascular disease
Decreased GFR
g
dysfunctiondisease
Proteinuria/albuminuria
GlomerulosclerosisRenal failure

TargetTarget--organ organ DDamage amage IIncreases ncreases IIncreases ncreases
CCardiovascular ardiovascular RRiskiskLeft ventricular hypertrophy120
HypertensionHypertension + LVH
Left ventricular hypertrophy
80
100
nciden
cets
)
Hypertension + LVH
60
80
dju
sted
in
00 p
atie
nt
40
ear
age-
ad(p
er 1
0
202-y
e
0Stroke Heart failure Coronary disease
Kannel. Eur Heart J 1992;13 (Suppl D):82–88

TargetTarget--organ organ DDamage amage IIncreases ncreases CCardiovascular ardiovascular RRiskisk
Carotid IMT
Daniel HO et al. NEJM 1997;340:14–22

TargetTarget--organ organ DDamage amage IIncreases ncreases CVCV RRiskisk
*
14
16
nts
*
Albuminuria (in type 2 diabetes)
10
12
14
ascu
lar ev
en
per
yea
r)
Albuminuria (in type 2 diabetes)
6
8
e of ca
rdio
va
of pat
ients
p
*
2
4
Inciden
ce
(% o
0Normoalbuminuria Microalbuminuria Macroproteinuria
*P<0 05 versus normoalbuminuria
Gimeno Orna et al. Rev Clin Esp 2003;203:526–531
*P<0.05 versus normoalbuminuria after adjusting for other risk markers

Lowering Lowering BPBP reduces reduces CVCVi ki kriskrisk
Meta-analysis of 61 prospective, observational studiesOne million adults, 12.7 million person-years
7% reduction in risk of ischaemic heart disease
2 mmHg decrease in mean SBP
heart disease mortality
mean SBP10% reduction in risk of stroke mortalitymortality
Lewington et al. Lancet. 2002;360:1903–1913

Characteristics of Morning BP Characteristics of Morning BP Characteristics of Morning BP Characteristics of Morning BP Reactivity SubgroupReactivity SubgroupReactivity SubgroupReactivity Subgroup
<<<
Am J Hypertens 2005;18:1528–1533

24h Profiles of SBP & SBP 24h Profiles of SBP & SBP VariationVariation
NormoNormoHTNHTN
Hypertension. 2005;45:505-512.
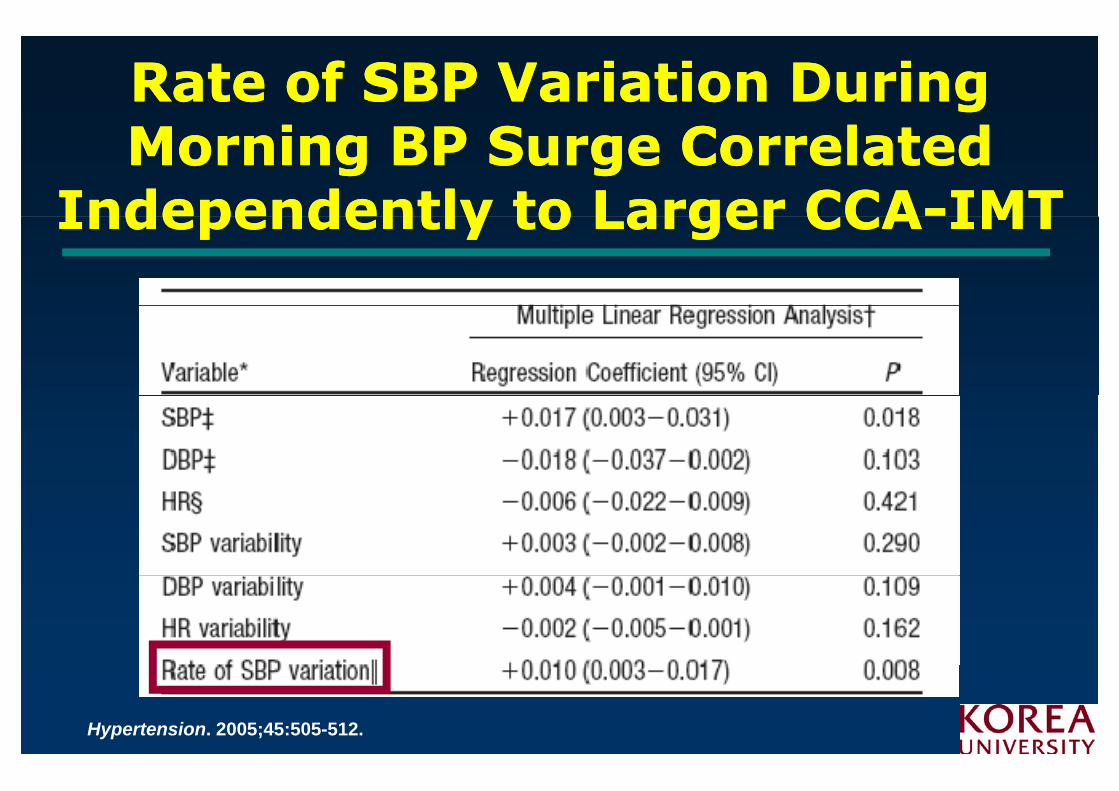
RRate of SBP ate of SBP VVariation ariation DDuring uring ii SS CC l dl dMMorning BP orning BP SSurge urge CCorrelated orrelated
IIndependently to ndependently to LLarger CCAarger CCA--IMTIMTIIndependently to ndependently to LLarger CCAarger CCA IMTIMT
Hypertension. 2005;45:505-512.

A significant increase in physical and A significant increase in physical and l i il i i dj d i h i i dj d i h i i mental activitymental activity––adjusted ischemic time at adjusted ischemic time at
the hour of awakening the hour of awakening gg
Circulation. 1996;93:1364-1371

Telmisartan compared with Telmisartan compared with
P<0 05 24-h mean Telmisartan
Perindopril Perindopril –– last 8 hourslast 8 hours100
Pretreatment
P<0.05 24 h mean Telmisartan versus Perindopril
95
mHg)
P≤0.05
90
DBP (
mm
P≤0.05Telmisartan versus Perindopril
85
D Post-treatment
Telmisartan 80 mg P i d il 4
80208 10 12 14 16 18 22 24 2 4 6 8
Perindopril 4 mg
Double-blind
Time of day (hours) comparative studyNalbantgil et al. Int J Clin Pract 2004;58:50–54

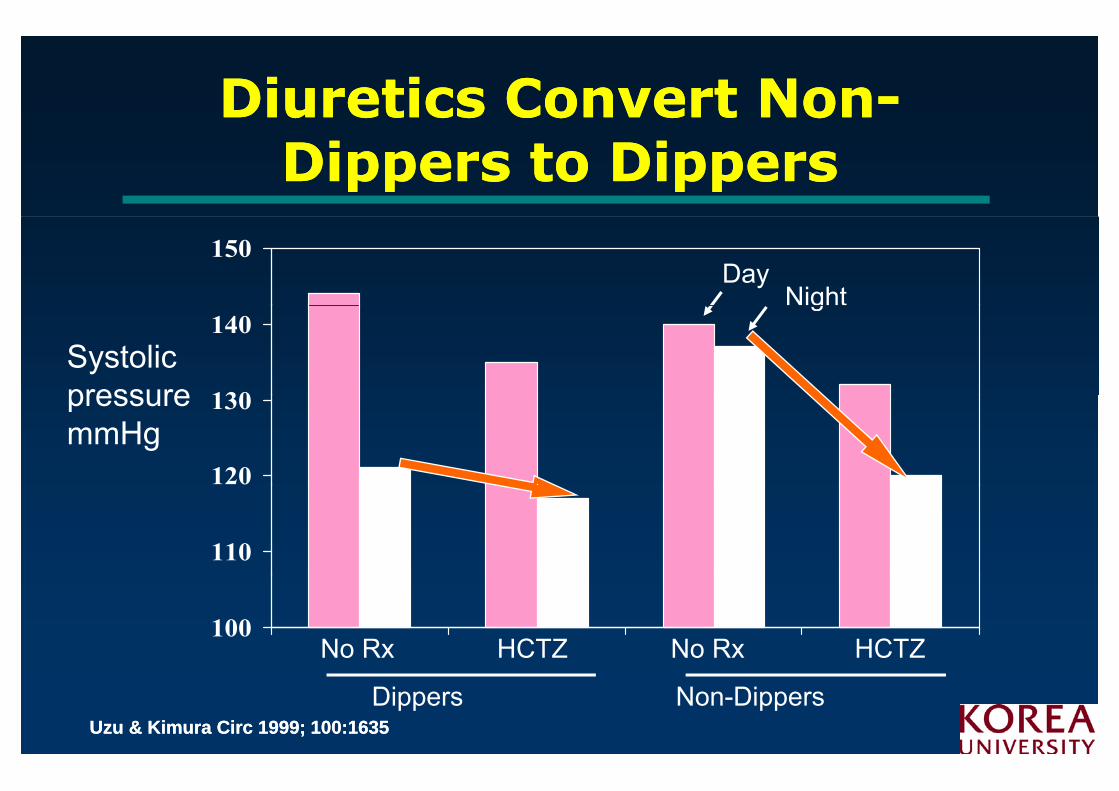
Diuretics Convert NonDiuretics Convert Non--Dippers to DippersDippers to Dippers
1 5 0Day
Ni ht
1 3 0
1 4 0Systolic pressure
Night
1 2 0
1 3 0pressure mmHg
1 1 0
1 0 0No Rx HCTZ No Rx HCTZ
Dippers Non-DippersUzu & Kimura Circ 1999; 100:1635Uzu & Kimura Circ 1999; 100:1635

Telmisartan vs AmlodipineTelmisartan vs Amlodipinei 24i 24 h ABPMh ABPMusing 24using 24--h ABPMh ABPM
Placebo (n=58)
Amlodipine (5-10 mg) (n=65)Telmisartan (40-120 mg) (n=62)
BP (mm Hg) 160
Week 12, SBP
140
120
100100
0
0800 1200 1600 2000 2400 0400 0800
Lacourcière Y et al, in press
0
Time

Relevance of trough:peak Relevance of trough:peak ratios to 24ratios to 24--h h BPBP controlcontrol
)
180
Placebo
e (m
mH
g 160Trough
Drug A
pre
ssure
20
140Peak
ug(T:P ratio =75%)
Blo
od 120
100Drug B
(T:P ratio =45%)
07:00 11:00 15:00 19:00 23:00 03:00 07:00
100Dose
(T:P ratio =45%)Dose
Time of day
Ellioit, Meredith. J Hypertension 1995;13:279–283
Diuretics Convert NonDiuretics Convert Non--Dippers to DippersDippers to Dippers
150Day
Night
130
140Systolic pressure
g
120
130pressure mmHg
110
100No Rx HCTZ No Rx HCTZ
Dippers Non-DippersUzu & Kimura Circ 1999; 100:1635Uzu & Kimura Circ 1999; 100:1635
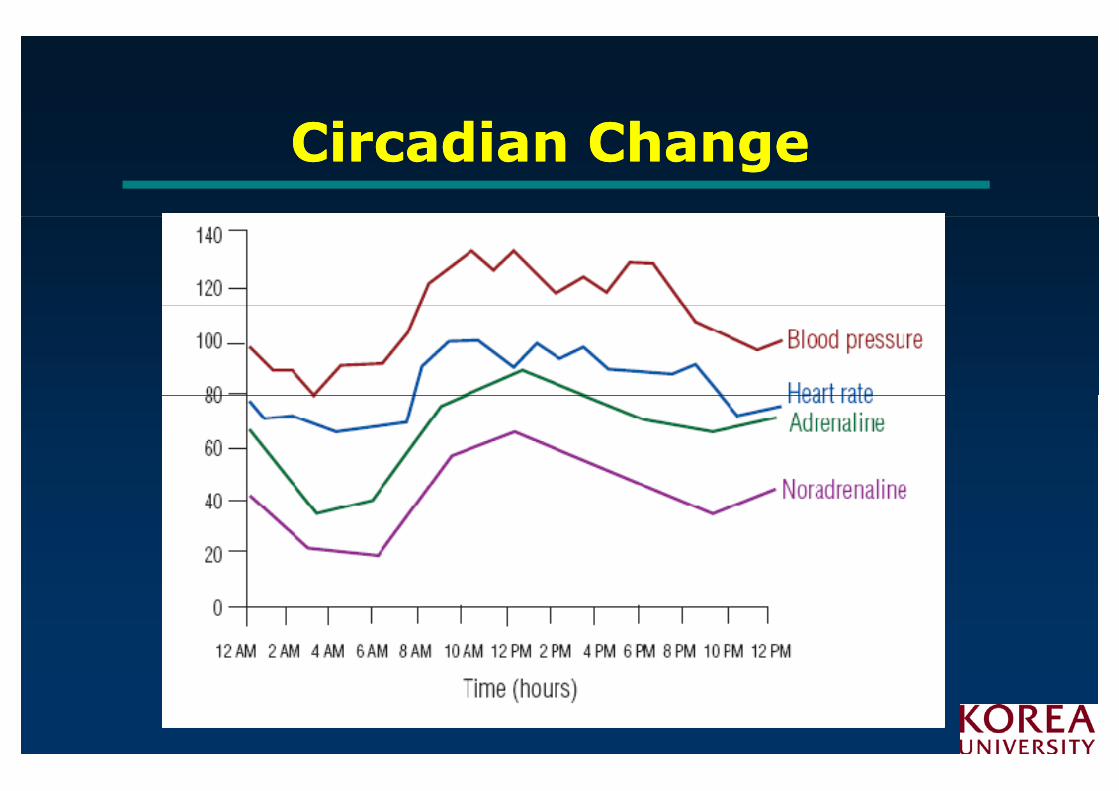
Ci di ChCi di ChCircadian ChangeCircadian Change

Adverse Events of Adverse Events of CYT006CYT006--AngQbAngQb
Placebo 100μg 300μg pPlacebo(n=24)
100μg(n=24)
300μg(n=24)
p
Injection-site 16 (66 7%) 23 (95 8%) 19 (79 2%) 0 045Injection-siteinduration
16 (66.7%) 23 (95.8%) 19 (79.2%) 0.045
Injection-site 8 (33 3%) 18 (75 0%) 21 (87 5%) 0 000Injection-siteedema
8 (33.3%) 18 (75.0%) 21 (87.5%) 0.0003
Headache 8 (33 3%) 6 (25 0%) 15 (62 5%) 0 024Headache 8 (33.3%) 6 (25.0%) 15 (62.5%) 0.024