clinical policy title: cognitive rehabilitation for ... · clinical policy title: cognitive...
TRANSCRIPT
1
Clinical Policy Title: Cognitive rehabilitation for traumatic brain injury
Clinical Policy Number: 15.02.02
Effective Date: December 1, 2013
Initial Review Date: July 17, 2013
Most Recent Review Date: July 20, 2016
Next Review Date: July 2017
Related policies:
None.
ABOUT THIS POLICY: Keystone First has developed clinical policies to assist with making coverage determinations. Keystone First’s clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by Keystone First when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. Keystone First’s clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. Keystone First’s clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, Keystone First will update its clinical policies as necessary. Keystone First’s clinical policies are not guarantees of payment.
Coverage policy
Keystone First considers the use of cognitive rehabilitation to be clinically proven and, therefore, medically
necessary when all of the following criteria are met:
There has been a traumatic brain injury.
Meets criteria for admission to a rehabilitation facility or for outpatient rehabilitation treatment.
Responsive to verbal or visual stimuli and demonstrates ability or potential to make progress and
achieve goals (i.e., not comatose or in a vegetative state).
No current substance abuse or acute psychiatric disorders.
Scores at least Level III or evolving to Levels IV – VI on the Rancho Los Amigos Level of Cognitive
Function Scale (pages 3 – 4).
Specific short- and long-term goals and an anticipated discharge/completion date are documented.
In adults ages 21 and over, the injury occurred no more than six months from date of request.
Policy contains:
Cognitive rehabilitation.
Traumatic brain injury (TBI).
Mild TBI (mTBI)/concussion.
Multidisciplinary rehabilitation.

2
Limitations:
All other uses of cognitive rehabilitation are not medically necessary. Furthermore, cognitive
rehabilitation in the following settings is not eligible for coverage of the following services, whose
effectiveness and medical necessity has not been established in the peer-reviewed literature:
Transitional living.
Day or community-based programs.
Vocational rehabilitation.
Structured adult education.
Community re-entry programs.
Behavioral training.
Employment counseling.
Work hardening.
Music, recreation or art therapies.
Intelligence testing.
Alternative Covered Services:
None.
Background
Cognitive rehabilitation includes therapies (delivered by speech, occupational or neuropsychological
therapists) that are designed to improve intellectual, perceptual and behavioral skills after damage to
the central nervous system. These therapies intend ultimately to increase levels of self-management
and independence, through the recovery of lost abilities or development of compensatory strategies.
Interventions include retraining in abilities to think, use judgment and make decisions. The focus is on
correcting deficits in memory, concentration and attention, perception, learning, planning and the
sequencing of tasks. Interventions are further classified as restorative/remedial (using a variety of
repetitive approaches) and compensatory/adaptive (adaptive devices and/or modification of the
environment).
Burden of disease — Head injury is the most common cause of death in young adults in the Western
world, accounting for up to two-thirds of in-hospital deaths and for a much larger proportion of lifelong
disability after trauma. Because head injury can affect neurological, cognitive and muscle abilities,
individuals may face physical, cognitive, behavioral and emotional injuries.
Outcomes and potential for successful rehabilitation depends on the primary brain damage and quality
of early management, adequate referral policy, prompt diagnosis and treatment of mass lesions, as well

3
as preventing, limiting and treating processes leading to secondary damage. Challenges in providing care
for individuals with TBIs include the variety of presentation and complexity surround the various
cognitive rehabilitation interventions.
Evaluation — Since its introduction in 1974, the Glasgow Coma Scale (GCS) has been widely adopted as
an initial measure of the severity of brain injury. The GCS score summarizes responses in three domains:
eye opening, verbal and motor. GCS is established as a predictor of both immediate and long-term
outcome after traumatic brain injury. TBI can be categorized as severe, moderate or mild, based on the
presenting GCS. A GCS of ≤ 8 is considered representative of severe brain injury (3 – 8 indicating coma);
9 – 3 moderate brain injury and 14 – 15 mild brain injury or concussion. Patients presenting with severe
brain injury have the highest mortality rate, typically reported in the range of 39 percent to 51 percent.
These patients are also at the highest risk for the development of intracranial hypertension and thus are
most likely to benefit from intervention to control intracranial pressure. Therefore, these groups of
patients will most likely benefit from early intervention, to minimize secondary brain injury. The Rancho
Los Amigos Cognitive Scale (below) further refines outcome prediction and monitoring for rehabilitation
settings.
Study types used in preparing this policy — Systematic reviews for cognitive rehabilitation are listed in
Table 1. These reviews pool results from multiple studies to achieve larger sample sizes and greater
precision of effect estimation, than in smaller primary studies. Other policies are listed in Table 2.
Systematic reviews use predetermined transparent methods to minimize bias, and are therefore rated
highest in evidence grading hierarchies. Economic analyses (cost-effectiveness, benefit or utility studies
report both costs and outcomes but not simple cost studies), sometimes known as efficiency studies,
also rank near the top of evidence hierarchies.
Since searches for primary studies included in systematic reviews often cover several decades, a list of
published reviews provides a “snapshot” of the literature, along with gaps in the evidence base. Table 1
lists systematic reviews for cognitive rehabilitation, along with diagnoses addressed in the reviews, years
of literature covered and major conclusions. Table 2 lists professional association guidelines and other
clinical policies.
Ranchos Los Amigos Cognitive Scale — Describes and monitors a patient’s level of functioning and
progress over extended periods:
Level Classification Definition
I No response. Unresponsive to all stimuli.
II Generalized. Inconsistent, non-purposeful reaction to stimuli.
Responds to pain, but may be delayed.
III Localized. Inconsistent reaction directly related to type of stimulus.
Response to some commands.
May respond to discomfort.
IV Confused Disoriented and unaware of present.

4
Level Classification Definition
Occasional agitation with frequent bizarre or inappropriate
responses.
Short attention span and impaired information processing.
V Confused, inappropriate, non-
agitated.
Non-purposeful, fragmented or random responses to complex
tasks.
Appears alert and responds to commands.
Performs previous learned tasks, but unable to learn new ones.
VI Confused appropriate. Goal-directed behavior.
Responses to situation appropriate.
Incorrect responses due to memory difficulties.
VII Automatic appropriate. Robot-like correct routine responses.
Oriented to setting.
Poor insight, judgment and problem-solving.
VIII Purposeful appropriate (stand by
assist).
Consistent person, place and time orientation.
Recalls and integrates past with present.
Depressed, irritable, low frustration tolerance, angry and
argumentative.
IX Purposeful appropriate (may request
stand by assist).
Independently shifts among tasks and completes accurately for
at least two consecutive hours.
May be agitated and depressed.
Self-monitors appropriateness.
X Purposeful and appropriate (modified
independence).
Multi-tasks regardless of environment.
May need periodic breaks.
Irritable and intolerant of frustration in case of illness, fatigue or
stress.
Table 1: Other guidelines/coverage
Citation Content, Methods, Recommendations
CMS ( NMP 129;
2013)
Cognitive rehabilitation post TBI:
≤ three hours per day inpatient rehab following TBI and all of the following:
o Patient meets criteria for rehab admission.
o Patient requires intensive interdisciplinary services ≤ three hrs/day, five – seven
days/week of ≤ two different types of therapy (physical, occupational, speech, cognitive
and pulmonary).
o Specific short- and long-term goals and anticipated discharge date are documented.
o Injury occurred ≤ six months from date of request.
o Patient is responsive to verbal or visual stimuli and demonstrates ability or potential to
make progress and achieve goals.
o Absence of substance abuse or acute psychiatric disorders.
o Rancho Los Amigos Level of Cognitive Function Scale Level III and evolving, or Rancho
IV – VI.
Outpatient:
≤ three hrs/day individualized neuro-cognitive rehab for diagnosed impairments, when part of a
multidisciplinary program with ≤ two types of therapy, no contraindications and all of the following:

5
Citation Content, Methods, Recommendations
o Documented specific short- and long-term goals, anticipated discharge date.
o Cognitive interventions are structured, systematic, individualized and restorative.
o Injury ≤ six months from date of request.
o Active in-home setting before injury.
o Responsive to verbal or visual stimuli.
o Ability or potential to progress and achieve goals.
o No substance abuse or acute psychiatric disorders.
Service setting exclusions:
Transitional living.
Day or community-based programs.
Non-medical settings (e.g., clubhouses for socialization).
Social skill development programs.
Supported living programs.
Independent living centers.
Service exclusions:
Vocational rehabilitation.
Structured adult education.
Community re-entry programs.
Behavioral training.
Compensatory devices (e.g., memory or date books, electronic paging and computer-assisted
training).
Employment counseling.
Work hardening.
Music, recreation and art therapies.
Intelligence testing.
Table 2: Glasgow Coma Scale (GCS)
Published by the Centers for Disease Control. Centers for Disease Control and Prevention website.
http://www.cdc.gov/masstrauma/resources/gcs.pdf. May 9, 2003. Accessed Jun. 11, 2015.
Glasgow Coma Scale (GCS)
Eye opening response:
• Spontaneous; open with blinking at baseline — four points.
• To verbal stimuli, command and speech — three points.
• To pain only (not applied to face) — two points.
• No response — one point.
Verbal response:
• Oriented — five points.
• Confused conversation, but able to answer questions — four points.
• Inappropriate words — three points.
• Incomprehensible speech — two points.
• No response — one point.

6
Motor response:
• Obeys commands for movement — six points.
• Purposeful movement to painful stimulus — five points.
• Withdraws in response to pain — four points.
• Flexion in response to pain (decorticate posturing) — three points.
• Extension response in response to pain (decerebrate posturing) — two points.
• No response — one point.
Categorization: Coma — No eye opening, no ability to follow commands and no word verbalizations (3 –8 points).
Head Injury Classification:
Severe head injury — GCS score of eight or less;
Moderate head injury — GCS score of nine to 12;
Mild head injury — GCS score of 13 — 15.
(Adapted from Advanced Trauma Life Support: Course for Physicians, American College of Surgeons, 1993).
Searches
Keystone First searched PubMed and the databases of:
UK National Health Services Centre for Reviews and Dissemination.
Agency for Healthcare Research and Quality’s Guideline Clearinghouse and evidence-based
practice centers.
The Centers for Medicare & Medicaid Services (CMS).
We conducted searches on June 8, 2016. Search terms were “traumatic,” “brain injuries,” “cognition”
neuropsychological tests all MESH and “rehabilitation.”
We included:
Systematic reviews, which pool results from multiple studies to achieve larger sample
sizes and greater precision of effect estimation than in smaller primary studies. Systematic
reviews use predetermined transparent methods to minimize bias, effectively treating the
review as a scientific endeavor, and are thus rated highest in evidence-grading hierarchies.
Guidelines based on systematic reviews.
Economic analyses, such as cost-effectiveness, and benefit or utility studies (but not
simple cost studies), reporting both costs and outcomes — sometimes referred to as
efficiency studies — which also rank near the top of evidence hierarchies.
Findings
Cognitive deficits are a common consequence of traumatic brain injury. Although such deficits are
amenable to rehabilitation, methods for individualizing cognitive interventions are still unrefined.
Functional neuroimaging methods such as positron emission tomography and functional magnetic

7
resonance imaging are emerging as possible technologies for measuring and monitoring the cerebral
consequences of plasticity associated with brain injury and for evaluating the effectiveness of
rehabilitation interventions. Functional neuroimaging may even enable more customized and efficient
selection, design, or adaptation of individual cognitive rehabilitation programs. We review the current
literature on functional neuroimaging after traumatic brain injury, relating these findings to cognitive
rehabilitation. Overall, functional neuroimaging after traumatic brain injury has shown reliable
differences in brain activity within several regions of frontal cortex, partly but not uniformly consistent
with neuropsychological and structural findings in traumatic brain injury. We also outline a number of
promising research opportunities for applying functional neuroimaging in traumatic brain injury settings,
along with associated challenges.
Policy updates:
Added statement in the findings section. Updated the clinical trials section.
Summary of clinical evidence:
Citation Content methods, recommendations
SIGN (2013) Key points: Brain injury rehabilitation in adults
Randomized controlled trials (RCTs) or systematic reviews, 1990 ‒ 2011.
Memory impairment after TBI — compensatory memory strategies with clear focus on daily functioning: o Mild-moderate impairment; external aids and internal strategies (visual imagery). o Severe impairment; external compensation focused on function.
Attention deficits post TBI — strategies relevant to personal function.
Executive functioning — meta-cognitive strategies focused on personally relevant problems with planning, problem-solving, and goal management.
Comprehensive/holistic programs should involve multidisciplinary team using goal-focused cognitive, emotional, and behavioral therapies.
Brasure (AHRQ; 2012)
Key points: Multidisciplinary post-acute rehab for moderate to severe TBI in adults
Prospective cohort studies and RCTs, 1980-2012.
Productivity outcomes; heterogeneity among studies precluded overall summary.
Community integration outcomes — one RCT with moderate risk of bias and one cohort with unadjusted results — no summary feasible.
Key overall finding — complexity of TBIs and incompletely defined interventions; heterogeneity of populations precluded pooling results.
No clear benefit of one approach over another.
Hayes (annotated bibliography; 2012)
Key points: Cognitive rehabilitation for TBI
2011 ‒ 2012, study types not specified.
Some evidence for efficacy in memory or social skills.
Comprehensive-holistic cognitive rehab may improve community integration vs. standard neuro-rehabilitation.
No studies report safety.
Variation among studies in targeted domains and rehab protocols; for TBI firm conclusions are difficult.

8
Marshall (2012) Key points: CPGs for mTBI with persistent symptoms
Systematic review of available guidelines with consensus recommendations; published guidelines in English or French, 1997 -2008.
Persisting cognitive complaints
Screen for: attention and concentration; processing speed; and memory (Rivermead Post-concussion Symptoms Questionnaire; provided in appendix to full-text article).
Assess for co-morbid conditions that may influence cognition (anxiety, depression, post-traumatic stress disorder (PTSD), pain, fatigue, sleep disturbance, acute stress disorder).
Refer to neuropsychologist experienced with TBI.
Spontaneous cognitive improvement can be expected in most cases of mTBI. Cognitive rehabilitation should be initiated when:
o Cognitive impairments persist on formal evaluation. o Compensatory strategies are needed for resumption of functional activities/work or safety
concerns (self and/or others). o Electronic external memory devices (computers, paging devices, organizers) are effective for
improving function post-mTBI.
Cincinnati Children’s Hospital (2011)
Key points: Speech therapist-directed computer assisted cognitive rehabilitation for acquired brain injury, ages 3 ‒ 21 years
TBI; tumors; arteriovenous malformations (AVMs); seizure disorders; meningitis; encephalitis; cerebrovascular accidents( CVAs); hydrocephalus.
Systematic reviews or analytic primary studies, 1995 – 2011.
Recommended for impairments in processing speed; attention; memory/working memory; inhibition; problem solving.
WLDI (2011) Key points: Head (trauma, headaches, not including stress and mental disorders)
1993 – Study types not specified.
Recommendations for physical therapy but cognitive rehab not specifically addressed.
Lane-Brown (Cochrane; 2009)
Key points: Interventions for apathy after TBI
VA/DoD (2009) Key points: Management of concussion/mTBI Does not include cognitive rehab.
Goliscz (2009) Key points: Occupational therapy for adults with TBI Does not specifically include cognitive rehab.
Kumar (Cochrane protocol; 2009)
Key points: Occupational outcomes after TBI
Turner-Stokes (2006)
Key points: Specialist rehabilitation for reducing dependency and costs for adults with complex acquired brain injuries
Before-and-after data from 297 patients admitted to UK rehab service, 1999 – 2005.
Changes in dependency status were associated with substantial savings in direct costs of ongoing care, especially for high-dependency patients.
Chesnut (AHRQ; Key points:

9
1999)
Rehabilitation for TBI
Controlled studies, 1976 ‒1997. Key question 3: Cognitive rehabilitation — Mixed results, but best evidence supported prosthetic aids for memory.
o One study indicates cognitive rehabilitation reduces anxiety; improves self-concept and relationships.
o Two studies support use of computer-assisted cognitive rehab in improving immediate recall.
Cicerone (2011) Key points: Clinical Recommendations for Cognitive Rehabilitation after TBI
Included 112 studies 2003 ‒2008
Defines practice standards, guidelines, and options in 6 areas of therapy: o Attention. o Visio-spatial and praxic deficits. o Language and communication deficits. o Memory deficits. o Executive function deficits. o Comprehensive-holistic neuropsychological rehabilitation.
INCOG (2014) Key points: Guidelines for Cognitive Rehabilitation post TBI
Compilation of previous guidelines and literature focused on assessment of moderate to severe TBI.
Cognitive rehabilitation focuses on those younger than 65, medically stable, without psychiatric illness, and awareness of condition.
Individualized care which is tailored to individuals’ goals and condition (both pre and post injury) is an emerging strategy.
Cha (2013) Key points: Computer-based cognitive rehab for stroke.
Chung (Cochrane; 2013)
Key points: Executive dysfunction in stroke or other adult non-progressive acquired brain damage.
Loetscher (Cochrane; 2013)
Key points: Attention deficits following stroke.
Arends (Cochrane; 2012)
Key points: Return to work in adults with adjustment disorders.
Hoffmann (Cochrane; 2010)
Key points: Cognitive impairment in stroke.
Thomas (Cochrane; 2009)
Key Points: Multiple sclerosis.
O’Brien (2008) Key points: Multiple sclerosis.
Glossary
Aneurysm — Section in the wall of a blood vessel weakened, bulging or otherwise at risk of rupture and
bleeding into surrounding tissues.

10
Anoxia — Lack of oxygen.
Coma — State of profound unconsciousness caused by disease, injury or poison.
Traumatic brain injury (TBI) — TBI is an alteration in function or other evidence of brain pathology
caused by external force.
References
Professional society guidelines/others:
Bayley MT, Tate R, Douglas JM, et al. INCOG guidelines for cognitive rehabilitation following traumatic
brain injury: methods and overview. J Head Trauma Rehabil. 2014; 29(4): 290 – 306.
Riechers RG, Care of the patient with mild traumatic brain injury. Glenview (IL): American Association of
Neuroscience Nurses, Association of Rehabilitation Nurses; 2011. p. 35.
Colorado Division of Workers' Compensation. Traumatic brain injury medical treatment guidelines.
Denver (CO): Colorado Division of Workers' Compensation; 2012 Nov 26. p.119.
Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for
management of concussion/mild traumatic brain injury (mTBI). Washington (DC): Department of
Veteran Affairs, Department of Defense; 2009 Apr. p.112.
Golisz K. Occupational therapy practice guidelines for adults with traumatic brain injury. Bethesda (MD):
American Occupational Therapy Association (AOTA); 2009. p.258.
Peer-reviewed references:
Arends I, Bruinvels DJ, Rebergen DS, et al. Interventions to facilitate return to work in adults with
adjustment disorders. Cochrane Database Syst Rev. 2012. Issue 12.
Borg J, Holm L, Cassidy JD, et al. Diagnostic procedures in mild traumatic brain injury. Results of the
WHO Collaborating Centre Task Force on mild traumatic brain injury. J Rehabil Med. 2004a; 43(Suppl):
61 – 75.
Brasure M, Lamberty GJ, Sayer NA, et al. Multidisciplinary postacute rehabilitation for moderate to
severe traumatic brain injury in adults. Comparative effectiveness review number 72. AHRQ Publication
No. 12-EHC101-EF. June 2012.
Bulger EM, Nathens AB, Rivara FP, Moore M, et al. Management of severe head injury: Institutional
variations in care and effect on outcome. Crit Care Med, 2002; 30(8): 1870 – 1876.

11
Cha YJ, Kim H. Effects of computer-based cognitive rehabilitation (CBCR) for people with stroke: A
systematic review and meta-analysis. Neurorehabilitation. 2013; 32(2): 359 – 68.
Chung CSY. Pollock A, Campbell T, Durward BR, et al. Cognitive rehabilitation for executive dysfunction
in adults with stroke or other adult non-progressive acquired brain damage. Cochrane Database Syst
Rev. 2013. Issue 4.
Cicerone KD, Langenbahn DM, Braden C, et al. Evidence-based cognitive rehabilitation: updated review
of the literature from 2003 through 2008. Arch Phys Med Rehabil. 2011; 92(4): 519 – 30.
Dunning J, Stratford-Smith P, Lecky F, et al. for the Emergency Medicine Research Group. A meta-
analysis of clinical correlates that predict significant intracranial injury in adults with minor head trauma.
J Neurotrauma, 2004; 21(7): 877 – 885.
Hayes, Inc. Cognitive rehabilitation for traumatic brain injury (TBI). Medical Technology Directory Pocket
Summary. Hayes, Inc. Lansdale, Pa. June 2011.
Hoffmann T, Bennett S, Koh CL, McKenna KT. Occupational therapy for cognitive impairment in stroke
patients. Cochrane Database Syst Rev. 2010. Issue 9.
Kumar KS, Kamalesh KS, Macadan AS. Cognitive rehabilitation for occupational outcomes after
traumatic brain injury. Cochrane Database Syst Rev. (protocol).2009. Issue 3.
Lamontagne ME, Gagnon C, Allaire AS, Noreau L. Effect of rehabilitation length of stay on outcomes in
individuals with traumatic brain injury or spinal cord injury: a systematic review protocol. Syst Rev. 2013;
2:59.
Lane-Brown A, Tate R. Interventions for apathy after traumatic brain injury. Cochrane Database Syst.
Rev. 2009. Issue 2.
Loetscher T., Lincoln NB. Cognitive rehabilitation for attention deficits following stroke. Cochrane
Database Syst. Rev. 2013. Issue 5.
Marshall S, Bayley M, McCullagh S, Velikonja D, et al. Clinical practice guidelines for mild traumatic brain
injury and persistent symptoms. Can Fam Physician. 2012; 58: 257-67.
Mower WR, Hoffman JR, Herbert M, Wolfson AB, et al. for the NEXUS II Investigators. Developing a
clinical decision instrument to rule out intracranial injuries in patients with minor head trauma:
methodology of the NEXUS II investigation. Ann Emerg Med, 2002; 40(5): 505 – 514.
O’Brien AR, Chiaravalloti N, Groverover Y, DeLuca J, et al. Evidence-based cognitive rehabilitation for
persons with multiple sclerosis: a review of the literature. Arch Phys Med Rehabil. 2008; 89(4): 761 – 9.

12
Sommer JB, Norup A, Poulsen I, et al. Cognitive activity limitations one year post-trauma in patients
admitted to sub-acute rehabilitation after severe traumatic brain injury. J Rehabil Med. June 2013;
45(8) 778 – 784.
Thomas PW, Thomas S, Hilier C, Galvin K, Baker R. Psychological interventions for multiple sclerosis.
Cochrane Database Syst. Rev. 2009. Issue 1.
Turner-Stokes L, Paul S, Williams H. Efficiency of specialist rehabilitation in reducing dependency and
costs of continuing care for adults with complex acquired brain injuries. J Neurol Neurosurg Psychiatry.
2006. 77(5): 634 – 9.
Clinical trials:
Searched clinicaltrials.gov on June 13, 2016 using terms “traumatic,” “brain,” “injury,” “cognitive” and
“rehabilitation.” | Open Studies. 47 studies found, two relevant.
VA Boston Healthcare System Recruiting Boston, Massachusetts . Combining Cognitive Treatment With
Noninvasive Brain Stimulation in Blast TBI. https://clinicaltrials.gov// ct2/show/NCT01596569?
Published May 7, 2012. Updated March 2016. Accessed June 13, 2016.
North Florida/South Georgia Veterans Health System, Gainesville, FL. Cognitive Rehabilitation & Brain
Activity of Attention-Control Impairment in TBI. https://clinicaltrials.gov/ct2/show/NCT02589509?
Published October 13, 2015. Updated December 2015. Accessed June 13, 2016.
CMS National Coverage Determinations (NCDs):
No NCDs identified as of the writing of this policy.
However, there are Medicare Benefit Policy Manuals for cognitive rehabilitation post traumatic brain
injury. National medical policy NMP129. Effective 4/2004.
Medicare Benefit Policy Manual, Chapter 12 - Comprehensive Outpatient Rehabilitation Facility
(CORF) Coverage: http://www.cms.gov/manuals/Downloads/bp102c12.pdf. Revised December
2012. Accessed June 13, 2016
Medicare Benefit Policy Manual, Chapter 1 - Inpatient Hospital Services Covered Under Part A:
http://www.cms.gov/manuals/Downloads/bp102c01.pdf. Revised June 27, 2014. Accessed
June 13, 2016.
Local Coverage Determinations (LCDs):
No LCDs identified as of the writing of this policy.

13
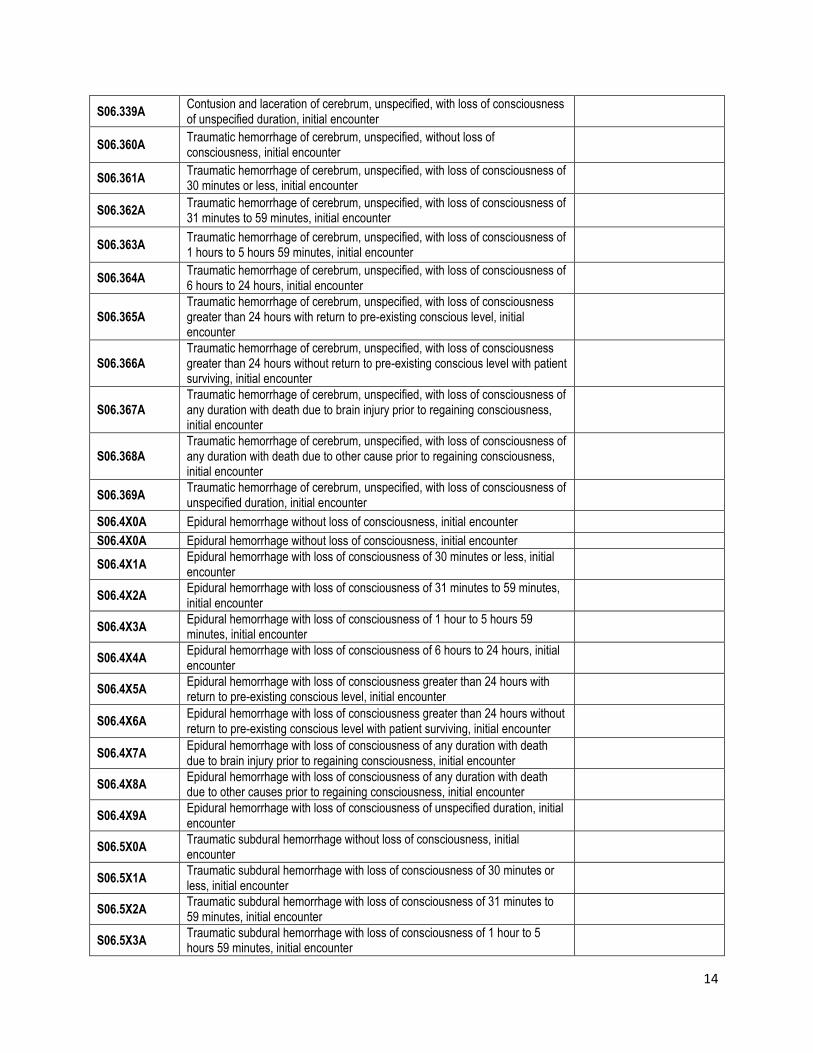
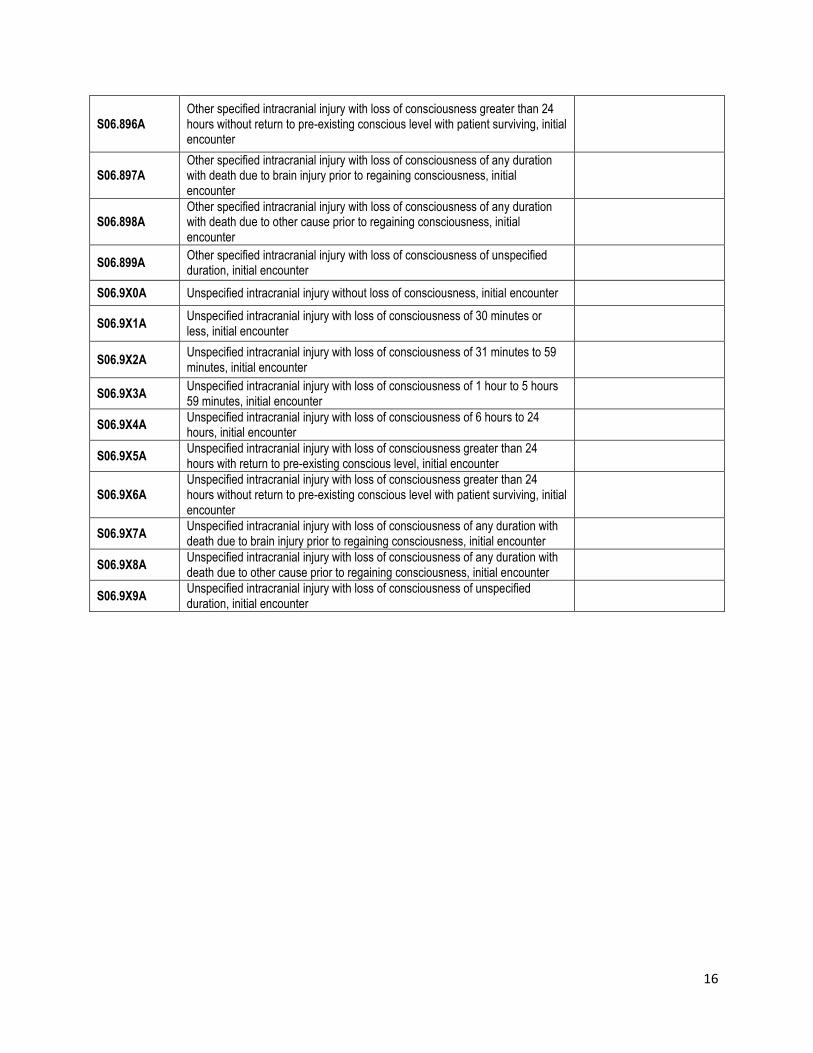
Commonly submitted codes
Below are the most commonly submitted codes for the service(s)/item(s) subject to this policy. This is
not an exhaustive list of codes. Providers are expected to consult the appropriate coding manuals and
bill accordingly.
CPT Code
Description Comment
97532 Development of cognitive skills: attention, memory, problem solving each 15 minutes one-on-one patient contact.
ICD-10 Code Description Comment
S06.300A Unspecified focal traumatic brain injury without loss of consciousness, initial encounter
S06.301A
Unspecified focal traumatic brain injury with loss of consciousness of 30 minutes or less, initial encounter
S06.302A
Unspecified focal traumatic brain injury with loss of consciousness of 31 minutes to 59 minutes, initial encounter
S06.303A
Unspecified focal traumatic brain injury with loss of consciousness of 1 hour to 5 hours 59 minutes, initial encounter
S06.304A
Unspecified focal traumatic brain injury with loss of consciousness of 6 hours to 24 hours, initial encounter
S06.305A
Unspecified focal traumatic brain injury with loss of consciousness greater than 24 hours with return to pre-existing conscious level, initial encounter
S06.306A
Unspecified focal traumatic brain injury with loss of consciousness greater than 24 hours without return to pre-existing conscious level with patient surviving, initial encounter
S06.309A
Unspecified focal traumatic brain injury with loss of consciousness of unspecified duration, initial encounter
S06.330A
Contusion and laceration of cerebrum, unspecified, without loss of consciousness, initial encounter
S06.331A
Contusion and laceration of cerebrum, unspecified, with loss of consciousness of 30 minutes or less, initial encounter
S06.332A
Contusion and laceration of cerebrum, unspecified, with loss of consciousness of 31 minutes to 59 minutes, initial encounter
S06.333A
Contusion and laceration of cerebrum, unspecified, with loss of consciousness of 1 hour to 5 hours 59 minutes, initial encounter
S06.334A
Contusion and laceration of cerebrum, unspecified, with loss of consciousness of 6 hours to 24 hours, initial encounter
S06.335A
Contusion and laceration of cerebrum, unspecified, with loss of consciousness greater than 24 hours with return to pre-existing conscious level, initial encounter
S06.336A
Contusion and laceration of cerebrum, unspecified, with loss of consciousness greater than 24 hours without return to pre-existing conscious level with patient surviving, initial encounter
S06.337A
Contusion and laceration of cerebrum, unspecified, with loss of consciousness of any duration with death due to brain injury prior to regaining consciousness, initial encounter
S06.338A
Contusion and laceration of cerebrum, unspecified, with loss of consciousness of any duration with death due to other cause prior to regaining consciousness, initial encounter
14
S06.339A
Contusion and laceration of cerebrum, unspecified, with loss of consciousness of unspecified duration, initial encounter
S06.360A
Traumatic hemorrhage of cerebrum, unspecified, without loss of consciousness, initial encounter
S06.361A
Traumatic hemorrhage of cerebrum, unspecified, with loss of consciousness of 30 minutes or less, initial encounter
S06.362A
Traumatic hemorrhage of cerebrum, unspecified, with loss of consciousness of 31 minutes to 59 minutes, initial encounter
S06.363A
Traumatic hemorrhage of cerebrum, unspecified, with loss of consciousness of 1 hours to 5 hours 59 minutes, initial encounter
S06.364A
Traumatic hemorrhage of cerebrum, unspecified, with loss of consciousness of 6 hours to 24 hours, initial encounter
S06.365A
Traumatic hemorrhage of cerebrum, unspecified, with loss of consciousness greater than 24 hours with return to pre-existing conscious level, initial encounter
S06.366A
Traumatic hemorrhage of cerebrum, unspecified, with loss of consciousness greater than 24 hours without return to pre-existing conscious level with patient surviving, initial encounter
S06.367A
Traumatic hemorrhage of cerebrum, unspecified, with loss of consciousness of any duration with death due to brain injury prior to regaining consciousness, initial encounter
S06.368A
Traumatic hemorrhage of cerebrum, unspecified, with loss of consciousness of any duration with death due to other cause prior to regaining consciousness, initial encounter
S06.369A
Traumatic hemorrhage of cerebrum, unspecified, with loss of consciousness of unspecified duration, initial encounter
S06.4X0A Epidural hemorrhage without loss of consciousness, initial encounter
S06.4X0A Epidural hemorrhage without loss of consciousness, initial encounter
S06.4X1A
Epidural hemorrhage with loss of consciousness of 30 minutes or less, initial encounter
S06.4X2A
Epidural hemorrhage with loss of consciousness of 31 minutes to 59 minutes, initial encounter
S06.4X3A
Epidural hemorrhage with loss of consciousness of 1 hour to 5 hours 59 minutes, initial encounter
S06.4X4A
Epidural hemorrhage with loss of consciousness of 6 hours to 24 hours, initial encounter
S06.4X5A
Epidural hemorrhage with loss of consciousness greater than 24 hours with return to pre-existing conscious level, initial encounter
S06.4X6A
Epidural hemorrhage with loss of consciousness greater than 24 hours without return to pre-existing conscious level with patient surviving, initial encounter
S06.4X7A
Epidural hemorrhage with loss of consciousness of any duration with death due to brain injury prior to regaining consciousness, initial encounter
S06.4X8A
Epidural hemorrhage with loss of consciousness of any duration with death due to other causes prior to regaining consciousness, initial encounter
S06.4X9A
Epidural hemorrhage with loss of consciousness of unspecified duration, initial encounter
S06.5X0A
Traumatic subdural hemorrhage without loss of consciousness, initial encounter
S06.5X1A
Traumatic subdural hemorrhage with loss of consciousness of 30 minutes or less, initial encounter
S06.5X2A
Traumatic subdural hemorrhage with loss of consciousness of 31 minutes to 59 minutes, initial encounter
S06.5X3A
Traumatic subdural hemorrhage with loss of consciousness of 1 hour to 5 hours 59 minutes, initial encounter

15
S06.5X4A
Traumatic subdural hemorrhage with loss of consciousness of 6 hours to 24 hours, initial encounter
S06.5X5A
Traumatic subdural hemorrhage with loss of consciousness greater than 24 hours with return to pre-existing conscious level, initial encounter
S06.5X6A
Traumatic subdural hemorrhage with loss of consciousness greater than 24 hours without return to pre-existing conscious level with patient surviving, initial encounter
S06.5X7A
Traumatic subdural hemorrhage with loss of consciousness of any duration with death due to brain injury before regaining consciousness, initial encounter
S06.5X8A
Traumatic subdural hemorrhage with loss of consciousness of any duration with death due to other cause before regaining consciousness, initial encounter
S06.5X9A
Traumatic subdural hemorrhage with loss of consciousness of unspecified duration, initial encounter
S06.5X9A
Traumatic subdural hemorrhage with loss of consciousness of unspecified duration, initial encounter
S06.6X0A
Traumatic subarachnoid hemorrhage without loss of consciousness, initial encounter
S06.6X1A
Traumatic subarachnoid hemorrhage with loss of consciousness of 30 minutes or less, initial encounter
S06.6X2A
Traumatic subarachnoid hemorrhage with loss of consciousness of 31 minutes to 59 minutes, initial encounter
S06.6X3A
Traumatic subarachnoid hemorrhage with loss of consciousness of 1 hour to 5 hours 59 minutes, initial encounter
S06.6X4A
Traumatic subarachnoid hemorrhage with loss of consciousness of 6 hours to 24 hours, initial encounter
S06.6X5A
Traumatic subarachnoid hemorrhage with loss of consciousness greater than 24 hours with return to pre-existing conscious level, initial encounter
S06.6X6A
Traumatic subarachnoid hemorrhage with loss of consciousness greater than 24 hours without return to pre-existing conscious level with patient surviving, initial encounter
S06.6X7A
Traumatic subarachnoid hemorrhage with loss of consciousness of any duration with death due to brain injury prior to regaining consciousness, initial encounter
S06.6X8A
Traumatic subarachnoid hemorrhage with loss of consciousness of any duration with death due to other cause prior to regaining consciousness, initial encounter
S06.6X9A
Traumatic subarachnoid hemorrhage with loss of consciousness of unspecified duration, initial encounter
S06.890A
Other specified intracranial injury without loss of consciousness, initial encounter
S06.891A
Other specified intracranial injury with loss of consciousness of 30 minutes or less, initial encounter
S06.892A
Other specified intracranial injury with loss of consciousness of 31 minutes to 59 minutes, initial encounter
S06.893A
Other specified intracranial injury with loss of consciousness of 1 hour to 5 hours 59 minutes, initial encounter
S06.894A
Other specified intracranial injury with loss of consciousness of 6 hours to 24 hours, initial encounter
S06.895A
Other specified intracranial injury with loss of consciousness greater than 24 hours with return to pre-existing conscious level, initial encounter
16
S06.896A
Other specified intracranial injury with loss of consciousness greater than 24 hours without return to pre-existing conscious level with patient surviving, initial encounter
S06.897A
Other specified intracranial injury with loss of consciousness of any duration with death due to brain injury prior to regaining consciousness, initial encounter
S06.898A
Other specified intracranial injury with loss of consciousness of any duration with death due to other cause prior to regaining consciousness, initial encounter
S06.899A
Other specified intracranial injury with loss of consciousness of unspecified duration, initial encounter
S06.9X0A Unspecified intracranial injury without loss of consciousness, initial encounter
S06.9X1A
Unspecified intracranial injury with loss of consciousness of 30 minutes or less, initial encounter
S06.9X2A
Unspecified intracranial injury with loss of consciousness of 31 minutes to 59 minutes, initial encounter
S06.9X3A
Unspecified intracranial injury with loss of consciousness of 1 hour to 5 hours 59 minutes, initial encounter
S06.9X4A
Unspecified intracranial injury with loss of consciousness of 6 hours to 24 hours, initial encounter
S06.9X5A
Unspecified intracranial injury with loss of consciousness greater than 24 hours with return to pre-existing conscious level, initial encounter
S06.9X6A
Unspecified intracranial injury with loss of consciousness greater than 24 hours without return to pre-existing conscious level with patient surviving, initial encounter
S06.9X7A
Unspecified intracranial injury with loss of consciousness of any duration with death due to brain injury prior to regaining consciousness, initial encounter
S06.9X8A
Unspecified intracranial injury with loss of consciousness of any duration with death due to other cause prior to regaining consciousness, initial encounter
S06.9X9A
Unspecified intracranial injury with loss of consciousness of unspecified duration, initial encounter