clinical significance of hiv-1 drug resistance daniel r. kuritzkes, md section of retroviral...
TRANSCRIPT

Clinical Significance of HIV-1 Drug Resistance
Daniel R. Kuritzkes, MDSection of Retroviral Therapeutics
Brigham and Women’s HospitalHarvard Medical School
DRK/Rome IAS/20.07.11
Consequences of ongoing viral replication during HAART
Accumulation of drug resistance mutations Development of cross-resistance within multiple
drug classes Greater difficulty in re-establishing virologic control
with future regimens Decline in CD4 count leading to disease progression
DRK/Rome IAS/20.07.11
Factors contributing to incomplete suppression of virus replication
Inadequate adherence Pharmacologic factors Host factors Inadequate ARV potency Transmitted drug resistance
DRK/Rome IAS/20.07.11
Managing drug-resistant HIV-1
Goal of therapy: complete virologic suppression Use resistance testing to guide regimen selection Combine new drugs with other active agents
– Ritonavir-boosted PI– NRTI without cross-resistance– Newer drugs (2nd-generation NNRTI, integrase
inhibitors, entry inhibitors) Use at least two or three active drugs to
maximize success of 2nd and later ART regimens
ARV Drug Resistance in Resource-Limited Settings
DRK/Rome IAS/20.07.11
South Africa Resistance Cohort Study: Specific aims
Estimate prevalence of drug resistance among patients receiving sub-optimal ART
Estimate prevalence of drug resistance among previously treated patients
Estimate impact of drug resistance on response to national ART program
Marconi et al Clin Infect Dis 2008
DRK/Rome IAS/20.07.11
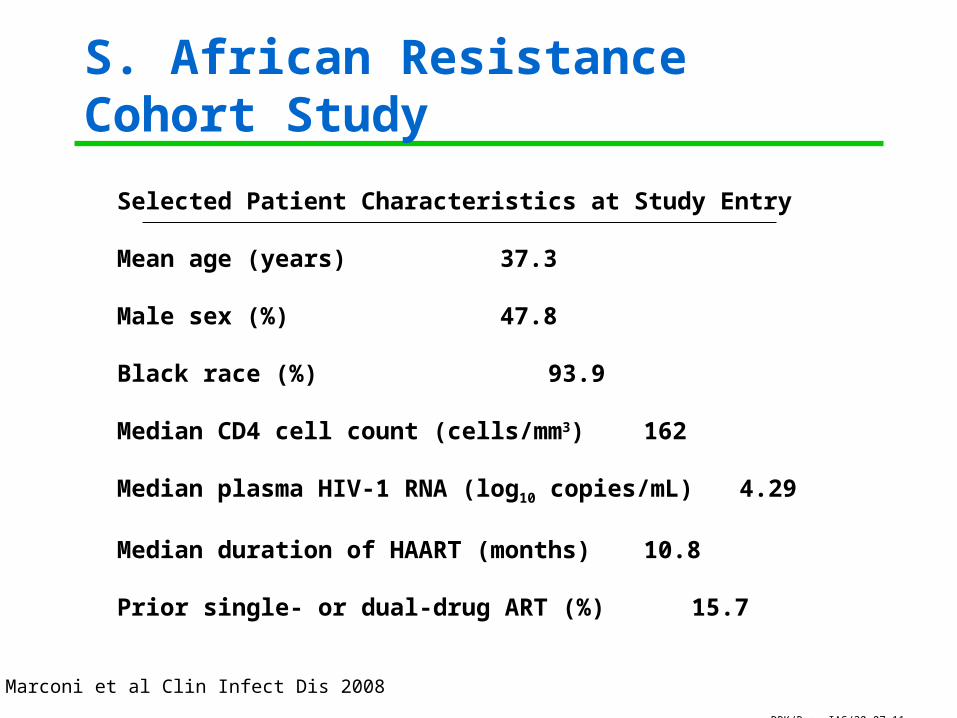
S. African Resistance Cohort Study
Selected Patient Characteristics at Study Entry
Mean age (years) 37.3
Male sex (%) 47.8
Black race (%) 93.9
Median CD4 cell count (cells/mm3) 162
Median plasma HIV-1 RNA (log10 copies/mL) 4.29
Median duration of HAART (months) 10.8
Prior single- or dual-drug ART (%) 15.7
Marconi et al Clin Infect Dis 2008

DRK/Rome IAS/20.07.11
Resistance mutations by regimen
Marconi et al Clin Infect Dis 2008
DRK/Rome IAS/20.07.11
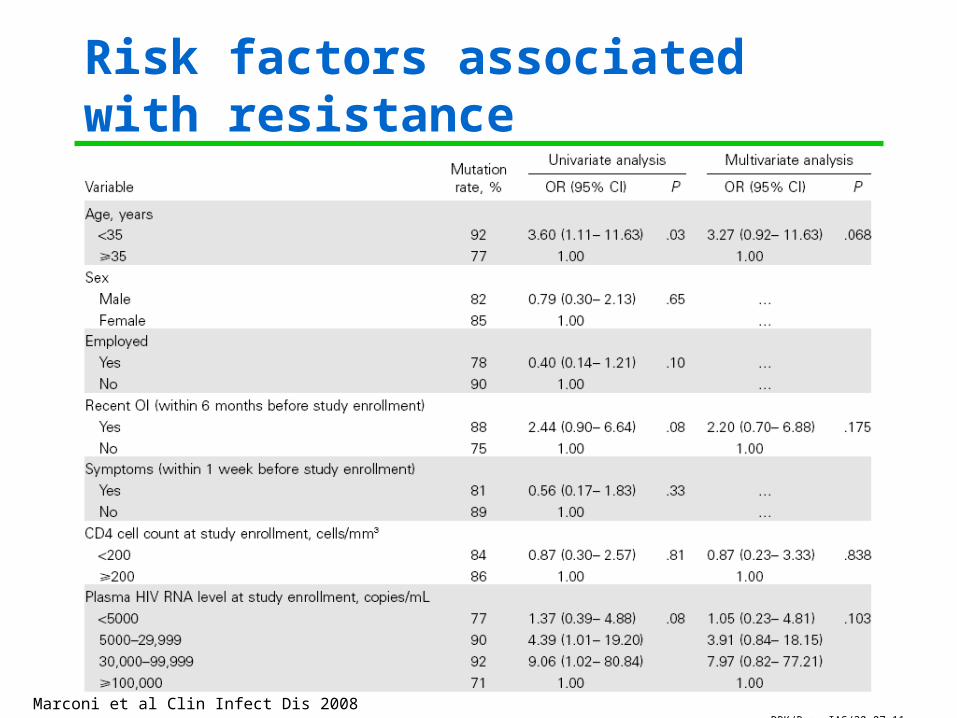
Risk factors associated with resistance
Marconi et al Clin Infect Dis 2008
DRK/Rome IAS/20.07.11
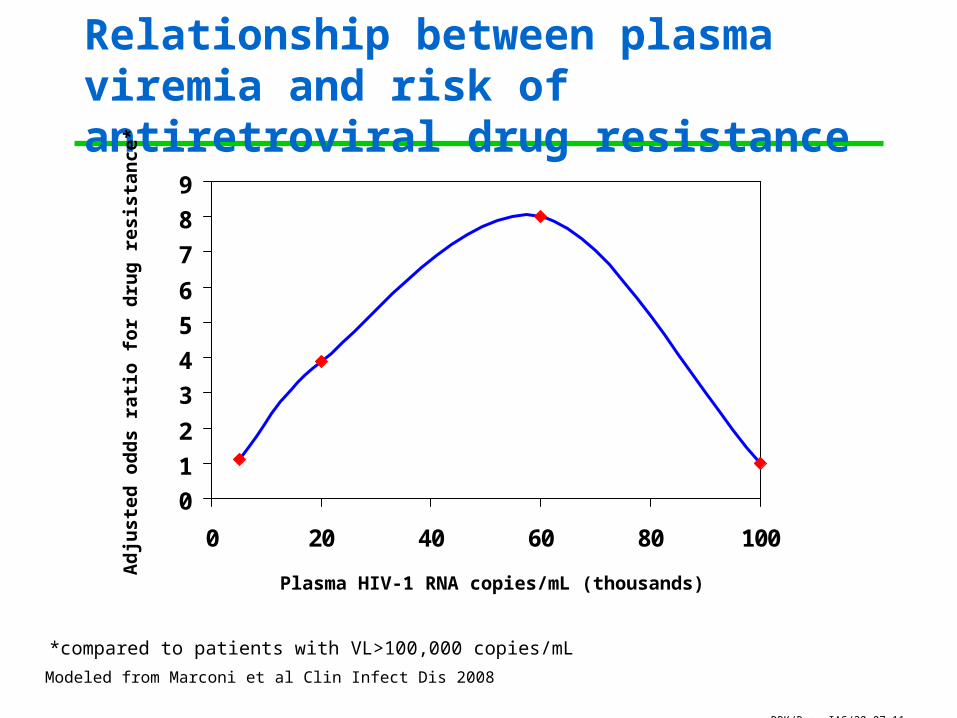
Relationship between plasma viremia and risk of antiretroviral drug resistance
0
1
2
3
4
5
6
7
8
9
0 20 40 60 80 100
Plasma HIV-1 RNA copies/mL (thousands)
Ad
jus
ted
od
ds
rati
o f
or
dru
g r
esis
tan
ce*
Modeled from Marconi et al Clin Infect Dis 2008
*compared to patients with VL>100,000 copies/mL

DRK/Rome IAS/20.07.11
24-week follow-up of SARCS patients
24-Week ITT Viral Suppression (VL<50 c/ml) and Baseline HIV-1 Drug Resistance
65% 69% 37%
0%
25%
50%
75%
100%
% V
iral
Su
pp
ress
ion
(<5
0 c/
ul)
All subjects
>1 Major Mutation
No Drug Resistance
Murphy R et al AIDS 2010; 24:1007-12.
P=.01
DRK/Rome IAS/20.07.11
Resistance after 2nd-line ART failure
302 patients on 2nd-line ART in Gugulethu– Viral sequencing performed on samples from 33 adults with
confirmed virologic failure Mean duration of prior ART 23 months Time from initiating 2nd-line ART to VF ~10 mo
– Plasma obtained 7 mo after VF 22 patients (67%) had wild-type virus at time of
2nd virologic failure– No major PI resistance mutations found
Levinson et al CROI 2011
DRK/Rome IAS/20.07.11
Conclusions
Data suggest non-adherence plays a major role in treatment failure
Adherence interventions rather than regimen switch may be more appropriate for some patients
Resistance testing may help avoid unnecessary switching to expensive 2nd- and 3rd-line regimens
Resistance after Single-Dose Nevirapine

DRK/Rome IAS/20.07.11
NVP resistance in women and infants after sdNVP prophylaxis in HIVNET 012
Eshleman et al AIDS 2001; 15:1951-7.
DRK/Rome IAS/20.07.11
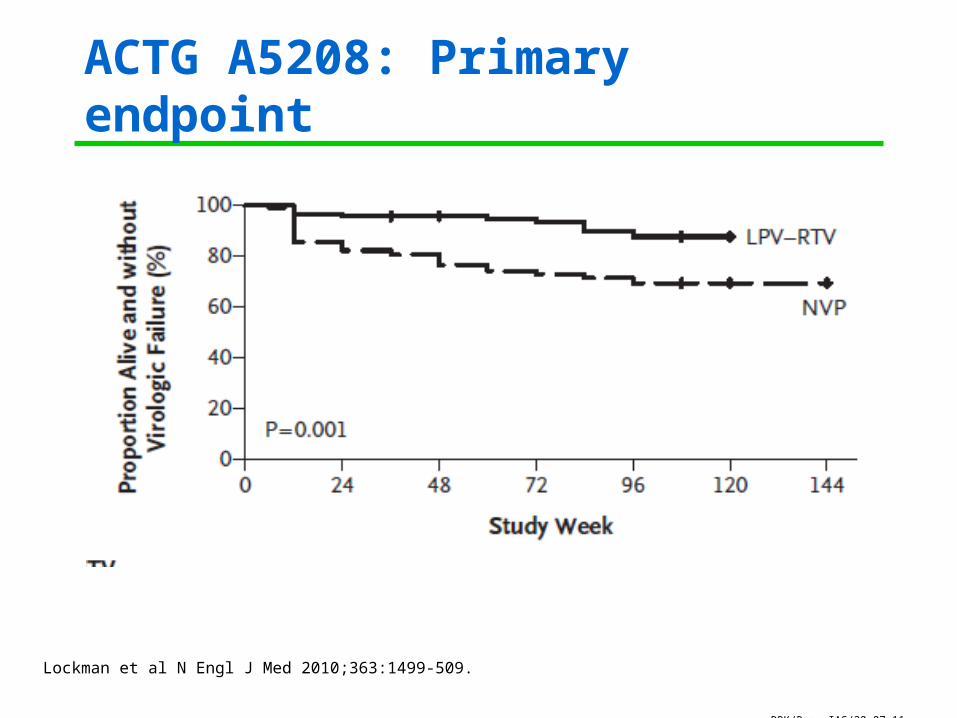
ACTG A5208: Primary endpoint
Lockman et al N Engl J Med 2010;363:1499-509.
DRK/Rome IAS/20.07.11
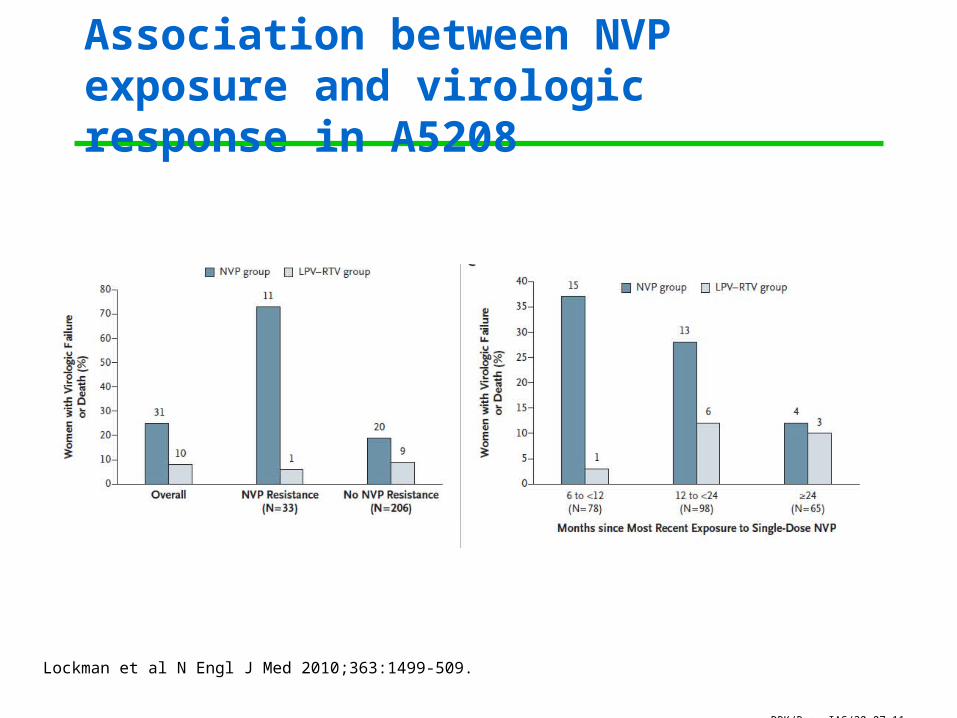
Association between NVP exposure and virologic response in A5208
Lockman et al N Engl J Med 2010;363:1499-509.
DRK/Rome IAS/20.07.11
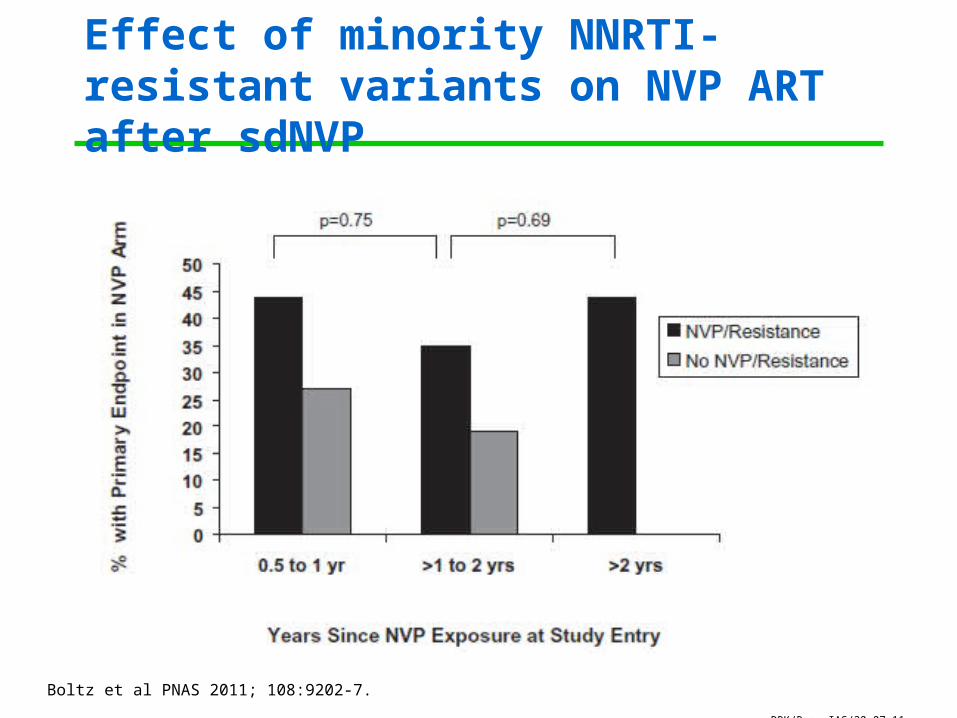
Effect of minority NNRTI-resistant variants on NVP ART after sdNVP
Boltz et al PNAS 2011; 108:9202-7.

DRK/Rome IAS/20.07.11
TOPS: Preventing NNRTI resistance after single-dose NVP for PMTCT
0%
10%
20%
30%
40%
50%
60%
NVP NVP-CBV4 NVP-CBV7
Per
cent
of
wom
en w
ith N
VP
res
ista
nce
at w
eek
6
Overall efficacy of ZDV/3TC “tail” = 85.6%
McIntyre et al PLoS Medicine 2009; 6:e1000172

DRK/Rome IAS/20.07.11
MOMS Study (ACTG A5207)1
Pregnant women who were to receive sdNVP for pMTCT randomized to 7 or 21 days of a post-NVP “tail” consisting of:– AZT/3TC– TDF/FTC– LPV/r
487 women randomized– 422 received study treatment– 63% received ZDV pre-partum
NVP resistance emerged in 5 women (4 in 7-day and 1 in 21-day arms; p=NS)– No difference between regimens– Similar trends observed in minority variant analysis2
1McMahon et al CROI 2011.2Hong et al. Antiviral Ther 2011; 16 (Suppl 1): A15.
DRK/Rome IAS/20.07.11
Conclusions
In the absence of virologic monitoring, failure of 1st-line regimens is associated with a high incidence of ARV resistance
PI resistance at 2nd-line failure is uncommon Absence of resistance suggests non-adherence
and may predict future non-adherence Better regimens are needed to prevent resistance
in the context of pMTCT– PROMISE study is addressing this need

DRK/Rome IAS/20.07.11
Acknowledgments
BWHVince MarconiRichard MurphyRoger ParedesSébastien Gallien
MGHBruce WalkerElena LosinaZhigang LuBingxia WangJulie LevinsonKen Freedberg
McCord HospitalHenry SunpathJane HamptonJanet GiddyHelga Holst
St. Mary’s HospitalDoug RossScott CarpenterKofi Koranteng-Apeagyi
Nelson Mandela School of MedicineMichelle Gordon
University of Cape Town Catherine OrrellRobin Wood
FundingNIAID, Gilead, CDC, Elizabeth Glaser Pediatric AIDS Foundation, Mark Schwartz Global Health Fellowship