clinical significance of the bcr-abl fusion gene in adult - blood
TRANSCRIPT

Clinical Significance of the BCR-ABL Fusion Gene in Adult Acute Lymphoblastic Leukemia: A Cancer and Leukemia Group B Study (8762)
By Carol A. Westbrook, Arthur L. Hooberman, Cathie Spino, Richard K. Dodge, Richard A. Larson, Frederick Davey, Doris H. Wurster-Hill, Robert E. Sobol, Charles Schiffer, and Clara D. Bloomfield
The Philadelphia (Ph’) chromosome, or its molecular counter- part, the BCR-ABL fusion gene, is a rare but important prognostic indicator in childhood acute lymphoblastic leuke- mia (ALL), but its impact on adult ALL has not been well ascertained. A prospective study of the BCR-ABL fusion gene was begun on patients entered on clinical trials conducted by the Cancer and Leukemia Group B (CALGB). All patients received intensive, multiagent chemotherapy that included daunorubicin. Over 2 years, 56 patients were studied for molecular evidence of a BCR-ABL gene using Southern blot and pulsed-field gel hybridization analysis. Results were compared with cytogenetic detection of a Ph’ chromosome, and clinical features were compared for the BCR-ABL- positive and -negative groups. Molecular methods detected the BCR-ABL gene in 30% of cases compared with cytoge- netic detection of the Ph’ chromosome in only 23%. The majority of cases (76%) showed the p190 gene subtype similar t o pediatric ALL; the BCR-ABL-positive cases dis-
HE BCR-ABL FUSION GENE, usually the result of T the Philadelphia (Ph’) chromosome translocation’ is universally present in cases of chronic myelogenous leuke- mia (CML).* Advances in molecular biology, especially in vivo studies of BCR-ABL gene a~t iv i ty ,~-~ have highlighted the contribution of this gene to the development of acute leukemia as well. Acute lymphoblastic leukemia (ALL) has been of particular interest in this regard because the Ph* chromosome is seen frequently in this disorder, which bears a close similarity to the lymphoid blast phase of CML and yet has molecular features that may differ from those found in CML.7,8
In pediatric ALL, cytogenetic studies have demonstrated that the Ph’ chromosome is an important contributor to mortality though present in only 2% to 3% of ca~es.~-11 Recent studies have underscored this contribution, showing that the Ph’ chromosome continues to carry a poor progno- sis12J3 even within the context of highly intensive, mul- tiagent therapy for childhood ALL that has improved survival in other cytogenetic subgroups.14
In adult ALL, the clinical impact of the Ph’ chromosome has not been as well delineated as it has in childhood ALL, although it is estimated to have a much higher incidence in this age group.9 Earlier studies suggested a poor outcome,11 but there have been no prospective studies that accurately reflect the incidence or prognosis of this abnormality within the context of contemporary therapies. Furthermore, it has been suggested that the BCR-ABL fusion gene of child- hood and adult ALL have a different molecular basis, with the BCR-ABL fusion gene in adult ALL of the “p210” subtype resembling that found in CML, whereas the child- hood subtype is “ ~ 1 9 0 . ” ~ ~ The two subtypes differ in the amount of the BCR gene included in the fusion and may have different biologic activity. Thus, it is difficult to extrapolate from the pediatric experience to adult ALL.
We therefore initiated a prospective study to determine the incidence, molecular subtypes, and clinical outcome of
played a more homogeneous immunophenotype than the BCR-ABL-negative cases and were predominantly CALLA positive (86%) and B-cell surface antigen positive (82%). The rate of achieving complete remission was similar in the BCR-ABL-positive and -negative groups (71 % and 77%, respectively, P = .72). There were more early relapses in the BCR-ABL-positive group, resulting in a shorter remission duration that was especially marked in the CALLA-positive and B-cell antigen-positive populations. These preliminary data suggest that the impact of the BCR-ABL gene on clinical outcome in ALL may be on maintenance of complete remis- sion (CR) rather than achievement of CR when aggressive, multiagent chemotherapy is used. This study identifies the BCR-ABL gene as an important factor in adult ALL and demonstrates the utility of molecular methods for its accu- rate diagnosis. 0 1992 by The American Society of Hematology.
the BCR-ABL fusion gene in newly diagnosed patients with adult ALL enrolled in CALGB clinical trials. We used methods of Southern hybridization and pulsed-field gel (PFG) electrophoresis well-suited to small sample volumes that could reliably detect the BCR-ABL fusion gene, or confirm its absence, in greater than 90% of cases. We compared our results with cytogenetic diagnosis and ana- lyzed associations with clinical and pathologic parameters.
MATERIALS AND METHODS
Fifty-six untreated patients with ALL who were 15 years of age or older were referred for molecular diagnostic studies as part of this prospective study: Cancer and Leukemia Group B (CALGB) 8762-Molecular Genetic Abnormalities in Adult Acute Lympho- blastic Leukemia. Forty-nine of these patients were treated on CALGB treatment protocols; 8 on CALGB 851316 and 41 on CALGB 8811.” The protocols included intensive, five-drug induc-
From the University of Chicago Medical Center, Chicago, 1L; Former Ofice of the CALGB Group Statistician, Boston, MA; CALGB Statistical Ofice, Durham, NC; State University of New York at Syracuse, Ny; Dartmouth Medical School, Hanover, NH; Univer- sity of California at Sun Diego, CA; University of Maryland Cancer Center, Baltimore, MD; and the Department of Medicine, Roswell Park Cancer Institute, Buffalo, Ny.
Submitted April 6, 1992; accepted August 20, 1992. Supported by Grants No. CA04326, CAI 1789, CA21060, CA31983,
CA33601, CA37027, and CA44700; the James F. McDonnell Founda- tion; and a Bristol-MyerslSquibb Cancer Research Fellowship.
Address reprint requests to Carol A . Westbrook, MD, PhD, Section of HematologylOncology, University of Chicago Medical Center, 5841 S MarylandAve, MC 2115, Chicago, 1L 60637-1470.
The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1992 by The American Society of Hematology. 0006-4971 19218012-0021$3.00/0
Blood, Vol80, No 12 (December 15), 1992: pp 2983-2990 2983
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom

2984 WESTBROOK ET AL
tion chemotherapy that included daunorubicin. These 49 patients represent 41% of cases entered on these protocols from October 1, 1987 until February 1, 1990. The other seven patients were included in the molecular, cytogenetic, and immunophenotypic studies but were not treated on CALOB protocols because none were active at the time; all received standard treatment at their home institutions.
The diagnosis of ALL was confirmed by central review of cytologic and cytochemical features according to the French- American-British (FAB) criteria.I8 Cytologic characteristics were examined on Wright-Giemsa-stained smears. Bone marrow or blood smears (or both) were evaluated for myeloperoxidase, using diaminobenzidine substrate at pH 7.6, Sudan Black B, a-napthyl acetate esterase, and with periodic acid-Schiff stain in standard cytochemical assay^.^^.^^ All patients had fewer than 3% myeloper- oxidase-positive blasts. Cases that could be subclassified into the L1 or L2 categories are included; those with L3 morphology, or Burkitt’s type leukemia/lymphoma, were excluded.
Molecular detection of the BCR-ABL fusion gene. Heparinized bone marrow aspirates or blood specimens were obtained before treatment and sent by overnight mail to a central reference laboratory at the University of Chicago Medical Center. Although bone marrow was requested for study on all cases, blood was accepted if marrow could not be provided either because the marrow was inaspirable or the sample was too scanty. A b u w coat was prepared, red blood cells were lysed by hypotonic ammonium chloride, and white blood cells were prepared directly into agarose plugs,21 each containing 1.6 million white blood cells (approximate- ly 10 pg of DNA). The plugs were used for PFG or for standard gel electrophoresis using previously described methods.2112z
Molecular diagnosis of the BCR-ABL fusion gene was per- formed by Southern blot and PFG analysis as described previous- ly.21,22 For every case, Southern blot analysis was performed by hybridization of probes bcr exon 2,2l bcr exon 4,2l and ~ u B 2 . 3 ~ ~ to BumHI, HindII, and Bgl I1 digests; PFG analysis was performed by hybridization of probes bcr exon 2 and pAEB2.3 toNot I digests. Translocation breakpoints are manifest as nongermline restriction bands within the BCR gene that are unique to individual cases. The presence of a new Not I BCR band is considered positive for the BCR-ABL fusion gene of any subtype. The molecular subtype is then specified by Southern blot analysis. Rearrangements detected with bcr exon 2 or bcr exon 4 probes specify the p210 subtype; rearrangement detected with probe pAEB2.3 or the absence of Southern blot rearrangement (in the presence of a positive PFG finding) indicates the p190 subtype. PFG and Southern hybridiza- tion to probes from the ABL genez1 were confirmatory, but isolated rearrangement was not considered positive in the absence of BCR findings.
Cytogenetic analysis was performed as part of CALGB 8461, a prospective study of chromosomes in acute leukemia.23 Analysis of banded chromosomes from bone marrow or, if inaspirable, peripheral blood taken at diagnosis were per- formed in CALGB institutional cytogenetic laboratories. Speci- mens were generally processed using short-term unstimulated cultures (24 to 72 hours). G-banding was usually used. A minimum of 20 cells were analyzed in each case. Two karyotypes demonstrat- ing each abnormal clone, or normal cells if the case lacked a clonal abnormality, were centrally reviewed. Karyotypes were designated according to the ISCN nomen~lature.2~
Immunophenotype determination. Heparinized bone marrow aspirates and blood specimens were used to determine the surface antigen phenotype by means of monoclonal antibodies. The sam- ples were sent by overnight courier to a reference laboratory at University of California, San Diego Cancer Center. Cytofluoromet- ric analysis, as previously described,z4 and a panel of monoclonal
Cytogenetic analysis.
antibodies was used for indirect immunofluorescence. The criteria for surface marker positivity was expression by at least 20% of the leukemic blast population. B-antigen expression was defined as B4 (CD19) or B1 (CD20) positivity; T-antigen expression as TlOl (CD5) or T11 (CD2) reactivity; and myeloid antigen expression as MCS-2 (CD13), My7 (CD13), or MY9 (CD33) positivity. We defined B-lineage as expressing B antigens only (without T or myeloid); T-lineage as expressing T antigens only; myeloid lineage as expressing only myeloid antigens; mixed as being positive for myeloid antigens plus either B, T, or both markers; and miscella- neous as any other combination (B+T+ or no positive markers). CALLA antigen was assessed by J5 (CD10) expression.
The study was designed to analyze the association between the BCR-ABL gene and morphology, immuno- phenotype, karyotype, presenting clinical features, response to therapy, survival, and remission duration and to compare the concordance of molecular and cytogenetic methods.
Survival was defined as the time from study entry until the time of death or last follow-up and was measured for all patients. Remission duration was defined only for those achieving complete response (CR) as time from CR until relapse (either bone marrow or non-bone marrow), death, or last follow-up. Patients were censored for analysis of survival if they were alive at the date of last follow-up, and they were censored for analysis of remission duration if relapse or death had not occurred by the time of last follow-up. Because of possible treatment effects on survival and remission duration, differences in these endpoints between BCR- ABL groups were tested, controlling for treatment study, by using the stratified logrank test.26 Survival and remission duration probabilities were estimated by the Kaplan-Meier method.27 Com- parison of the BCR-ABL groups with respect to surface markers, lineage, sex, organomegaly, lymphadenopathy, mediastinal mass, and response was based on Fisher’s exact test, whereas differences in age, leukocyte count (WBC), and hemoglobin were tested with the Wilcoxon rank sum statistic.28 A comparison of the proportion of BCR-ABL-positive cases found by molecular and cytogenetic detection methods was performed with McNemar’s test.28 All reported P values are based on two-sided tests of significance.
Statistical methods.
RESULTS
The molecular methods used permitted diagnosis of the BCR-ABL fusion and its molecular subtype in 93% of patients (Table 1). The technique was well suited to the analysis of specimens that contained low numbers of cells (as few as 5 million cells) or cells of poor viability resulting from shipping delays, condi- tions that are unavoidable in multi-institutional studies. The BCR-ABL fusion gene was detected as a rearrange- ment within the BCR gene by PFG, and the molecular
Detection of the BCR-ABL fusion gene.
Table 1. Detection of the BCR-ABL Fusion Gene
Total cases studied BCR-ABL positive
bcr positive (p210) bcr negative (p190)
5 PFG only 7 PFG and Southern blot 1 Southern blot only
BCR-ABL negative Not evaluable BCR-ABL positive/evaluable
Molecular No. 1%)
56 17 (30) 4 (24) 13 (76)
35 (63) 4 (7) 0.33
Cytogenetic No. (“4
53 12 (23) - -
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
PHILADELPHIA-POSITIVE ALL IN ADULTS 2985
subtype was specified by Southern analysis. In Phl-positive ALL, chromosome 22 translocation breakpoints occur in one of two regions of the BCR gene7? the 5.8-kb break- point cluster region, which is detected by Southern blot using bcr exon 2 and 4 probes, or the 70-kb first intron of the BCR gene. Translocations within the breakpoint cluster region usually produce the p210 protein, similar to that seen in CML, whereas the latter produces the p190 protein.
The results of molecular studies are summarized in Table 1. Of 56 cases enrolled on CALGB study 8762,52 had all molecular tests successfully completed. This included 36 bone marrow and 16 peripheral blood specimens. Seven- teen cases (30% of the total cases, or 33% of evaluable cases) were BCR-ABL positive. Of these 17, only one- fourth showed findings consistent with the p210 subtype; the remainder were of the p190 subtype.
Of the molecular methods used, PFG was the single most successful, detecting 15 of the 17 cases (88%), whereas Southern blot analysis detected 12 of 17 cases (71%), including 2 that were missed by PFG (one p210 and one p190). Of interest, Southern hybridization with pAEB2.3 detected 8 of the 13 p190 cases, further confirming that these breakpoints tend to cluster within this region. An ABL rearrangement was detected in 10 of the BCR-ABL- positive cases (59%), as well as in one BCR-ABGnegative case that had a cytogenetic Phl chromosome (see below); no other ABL rearrangements were detected, although extensive ABL analysis was not performed.
Of 53 cases sent for cytoge- netic analysis, 44 were specimens of bone marrow and 9 were peripheral blood. Complete karyotypes with adequate banding could be obtained on 40 cases (71%). A higher cytogenetic success rate was obtained when the analysis was limited only to the presence or absence of a Phl chromo- some. When reviewed in this manner, 45 of 53 cases (85%) produced evaluable metaphases, and the results are shown in Table 1. Of the 53 cases, 12 (23%) were Phl positive. If only the evaluable cases are considered, the incidence of Phl chromosome is 12 of 45 (27%). Cytogenetic analysis was more likely to fail in peripheral blood (4 failures of 9 specimens) than in marrow (4 failures of 44 specimens).
We directly compared molecular and cytogenetic meth- ods by analyzing the 53 cases that had samples sent for both studies. Molecular methods detected 16 BCR-ABL- positive cases, about one-third more than did cytogenetics (12 cases). When both methods were completely evaluable (43 cases), agreement was good (P = .18), but there were five discrepancies. Four of these discrepancies were the result of a BCR-ABL fusion that was missed by cytogenet- ics, and one was a Phl-positive case that was missed by molecular analysis.
These five discrepant cases were analyzed in detail. Of the four cases with negative cytogenetic studies, there were two in which no cytogenetic abnormality was reported. One case (41081) had a marrow sample analyzed. Although banding was poor and the karyotype was incomplete, a Ph' chromosome was not present. The other case (43419) had a normal karyotype, but only peripheral blood was available for cytogenetics. Because the total white blood count was
Cytogenetic detection of Ph'.
low (only 3.3 x 109/L) it is possible that the only met- aphases obtained actually originated in residual normal cells. On molecular evaluation, both cases showed a South- ern blot rearrangement with pAEB2.3 (Fig 1A and B) as well as a positive PFG result (not shown).
Two other cases demonstrated the BCR-ABL fusion, but did not show the Phl chromosome, although cytogenetic studies were adequate. Case 44503 had the karyotype 46,XY,t(9;13) (q34;q12), suggesting a breakpoint on chro- mosome 9 at the ABL locus, but because both chromo- somes 22 were normal, it could not be classified as Phl positive. Molecular results demonstrate a bcr rearrange- ment (Fig 2C), suggesting that the BCR-ABL fusion oc- curred by a mechanism other than the standard 9;22 translocation. The other case (42265) had two abnormal clones detected by cytogenetic analysis of peripheral blood: 46,XX, t(4;8)(q21;q22), t( 1 1;14)( ql3;q32) and 47,XX, + 2. All Southern blot data were negative, but PFG showed the same pattern with probes a (bcr exon 4; Fig 2D) and c (pAEB2.3, not shown), and the rearranged bands were faint, consistent with their presence in a minor clone that was missed by cytogenetics. This case was also interesting in that it was positive for surface K light chains. Translocations at 14q32 have been reported in association with the Phl in pediatric ALL,12 but surface Ig is distinctly uncommon. This case is difficult to classify clinically as well as molecu- larly and cannot be confirmed as a true BCR-ABL positive or as a false positive.
Lastly, case 43217 was BCR-ABL negative but cytogenet- ically positive, with a variant Phl chromosome that resulted from a translocation between chromosomes 16 and 22, t( 16;22)(q24;qll). Molecular analysis revealed a PFG rear- rangement with the ABL probe (Fig 2E) but no BCR rearrangement with either Southern or PFG analysis, and thus did not meet the criteria for BCR-ABL fusion. By our choice of probes and enzymes, an ABL rearrangement is not consistently demonstrated when a BCR-ABL fusion is present, so we have not included it in our criteria. On the other hand, we have never observed an ABL rearrange- ment in normal cells or in leukemia cells that are Phl or BCR-ABL negative by other criteria. This case remains unconfirmed for a BCR-ABL gene but, if present, it would represent a false negative of molecular analysis and would support an expansion of our diagnostic criteria.
Of 52 submitted cases, 46 were evaluable for immunophenotyping, and the results are shown in Table 2. Twenty-nine of 46 (63%) expressed B antigens, including 14 of 15 BCR-ABL-positive cases. Expression of T antigens was less common in the BCR-ABL- positive than in the -negative cases and never occurred in the absence of B antigens. Ten of the 14 B-antigen-positive cases with the BCR-ABL gene expressed only B antigens, resulting in a B-lineage phenotype; 4 showed a mixed lineage phenotype that included B antigens (2 My+ B+ and 2 My+ B+ T+), and 1 had no surface markers positive. There were no pure myeloid-lineage or T-lineage cases of BCR-ABL-positive ALL. Viewed from another perspec- tive, the BCR-ABL gene is present in half of the cases of adult ALL with B-cell surface markers, but it is found in
Immunophenotype and FAB class.
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
2986 WESTBROOK ET AL
1 2 1 2 1 2
t
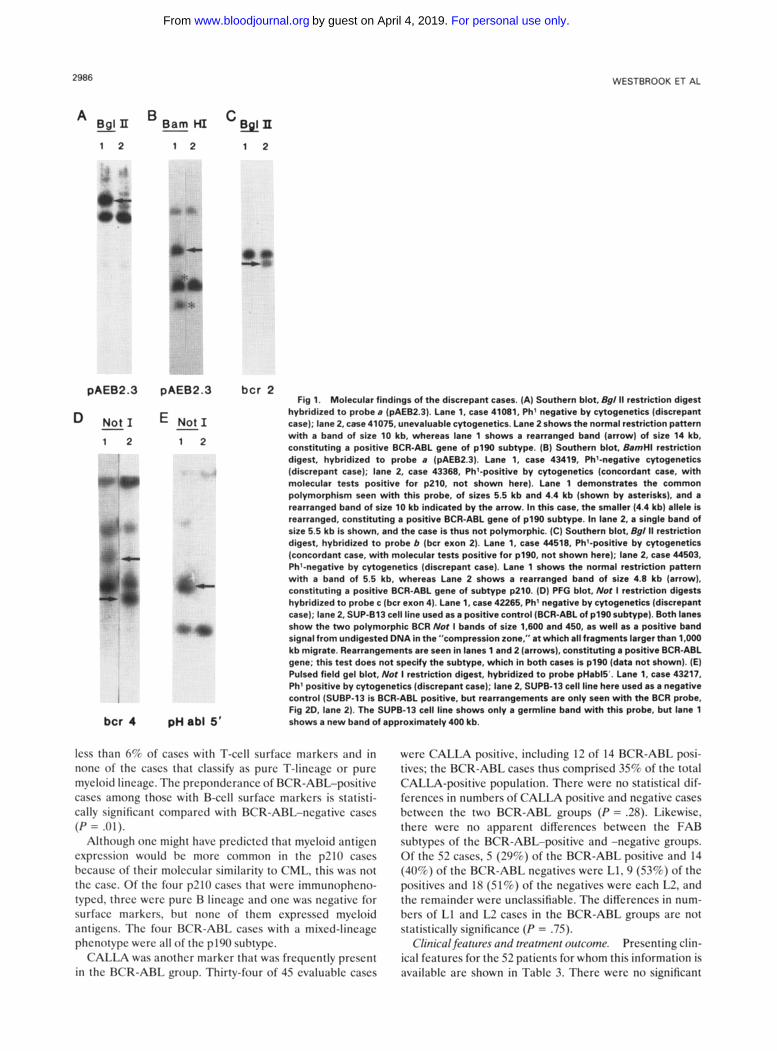
pAEB2.3 pAEB2.3 bcr 2 Fig 1. Molecular findings of the discrepant cases. (A) Southem blot, l?g/ II restridon digest
hybridlzed to probe a (pAEB2.3). Lane 1, case 41081, Ph' negative by cytogenetics (discrepant case); lane 2, cese 41075, unevaluable cytogenetics. Lane 2 shows the normal restriction pattern with a band of size 10 kb, whereas lane 1 shows a rearranged band (arrow) of size 14 kb, constituting a positive BCR-ABL gene of p190 subtype. (B) Southern blot, BamHl restriction digest, hybridized to probe a (pAEB2.3). Lane 1, caw 43419, Ph'-negative cytogenetics (discrepant case); lane 2, case 43368, Phi-positive by cytogenetics (concordant case, with molecular tests positive for p210, not shown here). Lane 1 demonstrates the common polymorphism seen with this probe, of sizes 5.5 kb and 4.4 kb (shown by asterisks), and a rearranged band of size 10 kb indicated by the arrow. In this case, the smaller (4.4 kb) allele Is rearranged, Constituting a posttive BCR-ABL gene of p190 subtype. In lane 2, a single band of size 5.5 kb is shown, and the case is thus not polymorphic. (C) Southern blot, Bg/ II restriction digest, hybridized t o probe b (bcr exon 2). Lane 1, case 44518. Phl-positive by cytogenetics (concordant case, with molecular tests positive for p190, not shown here); lane 2, case 44503, Phl-negative by cytogenetics (discrepant case). Lane 1 shows the normal restriction pattern with a band of 5.5 kb, whereas Lane 2 shows a rearranged band of size 4.8 kb (arrow). constituting a positive BCR-ABL gene of subtype p210. (0) PFG blot, Nor I restriction digests hybridized to probe c (bcr exon 4). Lane 1, case 42265, Ph' negative by cytogenetics (discrepant case); lane 2. SUP-613 cell line used as a positive control (BCR-ABL of p190 subtype). Both lanes show the two polymorphic BCR Nor I bands of size 1.600 and 450, as well as a positive band signal from undigested DNA in the "compression zone," at which all fragments larger than 1,OOO kb migrate. Rearrangements are seen in lanes 1 and 2 (arrows), constituting a positive BCR-ABL gene; this test does not specify the subtype, which in both cases is p190 (data not shown). (E) Pulsed field gel blot, Nor i restriction digest, hybridized to probe pHabl5'. Lane 1, case 43217, Ph' positive by cytogenetics (discrepant case); lane 2, SUPB-13 cell line here used as a negative control (SUBP-13 is BCR-ABL positive, but rearrangements are only seen with the BCR probe, Fig 2D. lane 2). The SUPB-13 cell line shows only a germline band with this probe, but lane 1 shows a new band of approximately 400 kb.
- Not1 E - Not1 1 2 1 2
bcr 4 pHab l 5'
lcss than 6% of cascs with T-ccll surfricc markcrs and in nonc of thc cascs that cl;issify as purc T-lincilgc or purc mycloid lincagc. Thc prcpondcrancc of BCR-ARL-positivc C;ISCS among thosc with R-ccll surfacc markcrs is statisti- cally significant comparctl with RCR-ARL-ncgativc C ~ S C S
Although onc might havc prcdictcd that mycloid antigcn cxprcssion would hc morc common in thc p210 c;iscs hccausc of thcir molccular similarity t o CMI,. this was not thc ciisc. Of thc four p210 CBSCS that wcrc immunophcno- typcd. thrcc wcrc purc R lincagc and onc was ncgativc for surfacc mwkcrs, hut nonc o f thcm cxprcsscd mycloid antigens. Thc four RCR-ABL CBSCS with ii mixcd-lincagc phcnotypc wcrc ;ill o f thc pllM) suhtypc.
CALLA was anothcr markcr that was frcqucntly prcscnt in thc RCR-ARL group. Thirty-four of 45 cvaluahlc caws
( P = . ( ) I ) .
wcrc CALLA positivc, including 12 of 14 RCR-ABL psi- tivcs: thc RCR-ARL cascs thus compriscd 3SC$ of thc total CALLA-positivc population. Thcrc wcrc no statistical dif- fcrcnccs in numbcrs of CALLA positivc and ncgativc caws bctwccn thc two RCR-ARL groups (P = .2X). Likcwisc. thcrc wcrc n o apparcnt diffcrcnccs hctwccn thc FAB suhtypcs of thc RCR-ABL-positive and -ncgativc groups. Of thc S2 cascs. S ( 2 S C 6 ) of thc RCR-ARL positivc and 14 ( 4 W ) of thc RCR-ARL ncgativcs wcrc LI. 0 (SY>) of thc psitivcs and 1% (SIC$) of thc ncgativcs wcrc cach L2, and thc rcmaindcr wcrc unclassifiahlc. Thc diffcrcnccs in num- hcrs of LI and L2 C ~ S C S in the RCR-ARL groups arc not statistically significilncc (P = .75).
Prcscnting clin- ical fcaturcs for thc 52 paticnts for whom this information is availahlc arc shown in Tahlc 3. Thcrc wcrc no significant
Clinical fe(itrin*s and trratmmr oiircome.
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
PHILADELPHIA-POSITIVE ALL IN ADULTS
1 .o-
0.8-
C .- o 0.6- e 0 n E 0.4-
2987
...... 'hi .... .-
L, ................ +
.-.-I BCR-ABL-/CALLA+
- - J BCR-ABL.
I I I I
0 1 2 3 4
Years
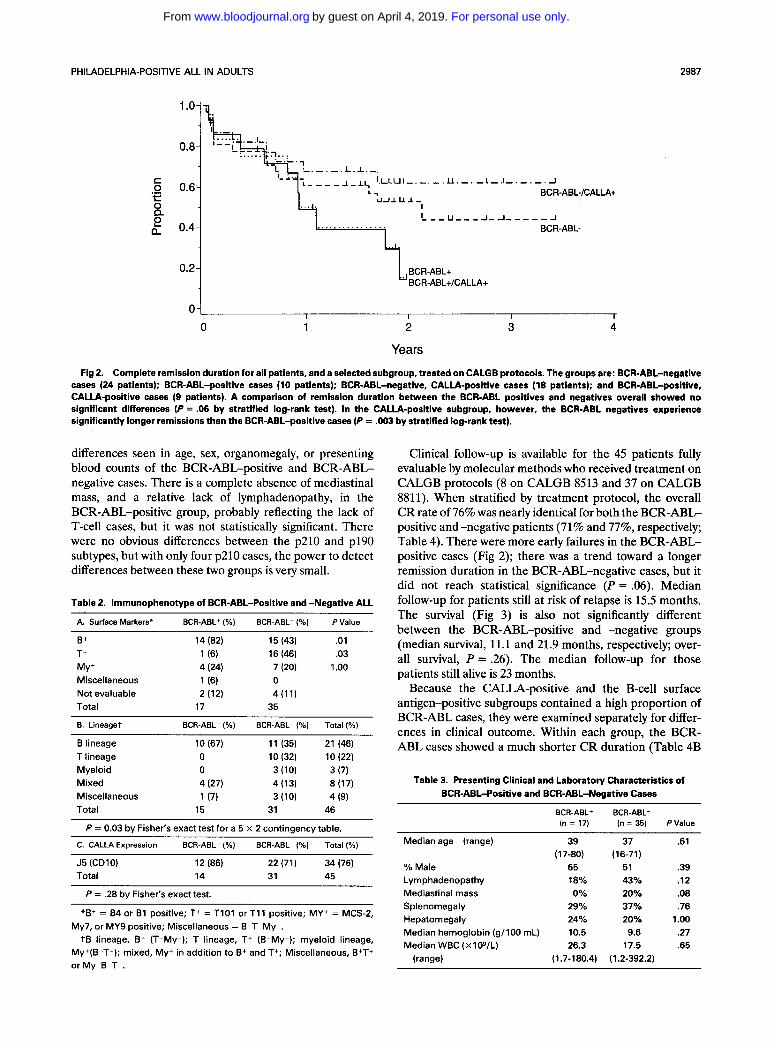
Fig 2. Complete remission duration for all patients, and a selected subgroup, treated on CALGB protocols. The groups are: BCR-ABL-negative cases (24 patients); BCR-ABL-positive cases (10 patients); BCR-ABL-negative, CALLA-positive cases (18 patients); and BCR-ABL-positive, CALLA-positive cases (9 patients). A comparison of remission duration between the BCR-ABL positives and negatives overall showed no significant differences (P = .06 by stratified log-rank test). In the CALLA-positive subgroup, however, the BCR-ABL negatives experience significantly longer remissions than the BCRABL-positive cases (P = .003 by stratified log-rank test).
differences seen in age, sex, organomegaly, or presenting blood counts of the BCR-ABGpositive and BCR-ABL- negative cases. There is a complete absence of mediastinal mass, and a relative lack of lymphadenopathy, in the BCR-ABL-positive group, probably reflecting the lack of T-cell cases, but it was not statistically significant. There were no obvious differences between the p210 and p190 subtypes, but with only four p210 cases, the power to detect differences between these two groups is very small.
Table 2. lmmunophenotype of BCR-ABL-Positive and -Negative ALL ~~
A. Surface Markers" BCR-ABL+ ( O h ) BCR-ABL- ( O h ) P Value
B+ 14 (82) 15 (43) .01 T+ 1 (6) 16 (46) .03 MY+ 4 (24) 7 (20) 1 .oo Miscellaneous 1 (6) 0 Not evaluable 2 (12) 4(11) Total 17 35
B. Lineaget BCR-ABL+ ( O h ) BCR-ABL- ( O h ) Total (%)
B lineage 10 (67) 11 (35) 21 (46) T lineage 0 10 (32) 10 (22) Myeloid 0 3 (10) 3 (7) Mixed 4 (27) 4 (13) 8 (17) Miscellaneous 1 (7) 3 (10) 4 (9) Total 15 31 46
P = 0.03 by Fisher's exact test for a 5 x 2 contingency table.
C. CALLA Expression BCR-ABL+ (%I BCR-ABL- ( O h ) Total (%)
J5 (CDIO) Total
12 (86) 22 (71) 34 (76) 14 31 45
P = .28 by Fisher's exact test. ~~
*B+ = 84 or B1 positive; T+ = TlOl or T11 positive; MY+ = MCS-2, My7, or MY9 positive; Miscellaneous = B-T-My-.
t B lineage, B+ (T-My-); T lineage, T+ (6-My-); myeloid lineage, My+(B-T-); mixed, My+ in addition to B+ and T+; Miscellaneous, B+T+ or My-B-T-.
Clinical follow-up is available for the 45 patients fully evaluable by molecular methods who received treatment on CALGB protocols (8 on CALGB 8513 and 37 on CALGB 8811). When stratified by treatment protocol, the overall CR rate of 76% was nearly identical for both the BCR-ABG positive and -negative patients (71% and 77%, respectively; Table 4). There were more early failures in the BCR-ABG positive cases (Fig 2); there was a trend toward a longer remission duration in the BCR-ABGnegative cases, but it did not reach statistical significance (P = .06). Median follow-up for patients still at risk of relapse is 15.5 months. The survival (Fig 3) is also not significantly different between the BCR-ABL-positive and -negative groups (median survival, 11.1 and 21.9 months, respectively; over- all survival, P = .26). The median follow-up for those patients still alive is 23 months.
Because the CALLA-positive and the B-cell surface antigen-positive subgroups contained a high proportion of BCR-ABL cases, they were examined separately for differ- ences in clinical outcome. Within each group, the BCR- ABL cases showed a much shorter CR duration (Table 4B
Table 3. Presenting Clinical and Laboratory Characteristics of BCR-ABL-Positive and BCR-ABL-Negative Cases
BCR-ABL+ BCR-ABL- (n = 17) (n = 35) PValue
Median age (range)
% Male Lymphadenopathy Mediastinal mass Splenomegaly Hepatomegaly Median hemoglobin (g/lOO mL) Median WBC (xIOg/L)
(range)
39 (1 7-80)
65 18% 0%
29% 24% 10.5 26.3
(1.7-180.4)
37 (1 6-71)
51 43% 20% 37% 20% 9.6
17.5 (1.2-392.2)
.61
.39
.12
.08
.76 1 .oo 2 7 .65
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom

2988 WESTBROOK ET AL
Table 4. Clinical Outcome for Patients Treated on CALGB Protocols 8513and8811
BCR-ABL+ BCR-ABL- A. All Cases (n = 14) (n = 31) PValue"
Complete remission (number) 10 (71%) 24 (77%) .72 Median remission duration (mo) 10.0 18.4 .06 Median survival (mo) 11.2 21.8 .26
BCR-ABL+ BCR-ABL- B. CALLA-Positive Cases (n = 12) (n = 22) PValue
Complete remission 9 (75%) 18 (81%) Median remission duration (mo) 9.5 NAt .003 Median survival (mo) 11.1 NAt .15
BCR-ABL' BCR-ABL- C. B Antigen-Positive Cases (n = 14) (n = 15) PValue
~ ~
Complete remission 9 (65%) 10 (67%) Median remission duration (mo) 9.1 NAt .03 Median survival (mo) 11.4 12.5 .64
*Logrank, stratified by treatment. tMedian not vet achieved.
and C). The CALLA-positive subgroup, which comprised 82% of the entire study population, showed especially striking differences. Remission duration was considerably longer in the BCR-ABL-negative cases (P = .003); median CR duration in BCR-ABL positives was 9.5 months, whereas 60% of the negative cases are still in CR at 2 years (Fig 3). It is clear from Figs 2 and 3 that the observed differences are primarily the result of better outcome in the comparison group. These results suggest that the CALLA-positive, BCR-ABL-negative subgroup may be a subgroup of adult ALL that does considerably better than others; this observa- tion warrants confirmation in a larger study.
DISCUSSION
The present study is an accurate portrayal of the inci- dence of BCR-ABL-positive cases in an unselected popula-
tion of adult ALL. Molecular analysis allowed the accurate specification of BCR-ABL-negative as well as BCR-ABL- positive groups, which facilitated clinical comparisons. Although the population is small and follow-up is short, there are intriguing differences in clinical outcome that warrant further investigation.
The BCR-ABL fusion gene appears to be a common finding in adult ALL, being present in one-third of all cases and fully one-half of cases with B-cell surface markers. Previous studies suggested a 20% in~idence,~Jl but these were based on cytogenetics, which, as we have shown, tends to underestimate the prevalence of this abnormality. Not surprisingly, these BCR-ABL cases present a more homoge- neous phenotype than the comparison BCR-ABGnegative groups. The majority of BCR-ABL-positive cases demon- strated B-cell markers and were CALLA positive, with a notable lack of T-lineage cases and myeloid cases. This is similar to findings in pediatric ALL, in which T-cell cases made up only 9% of Phl-positive cases.l2 There were no other important differences in presentation except for a complete absence of mediastinal mass in the BCR-ABL- positive group, also noted in pediatric ALL,I2 again reflect- ing the lack of T-cell phenotype.
An unexpected result is that the majority of cases show a molecular rearrangement consistent with the p190 subtype. Because of the small number of p210 cases, it was not possible to determine if there are clinical differences between these two subgroups; this question will require a larger study to answer it. It had previously been assumed that the p210 is more common in adult ALL, and the p190 more common in children,15 but these rates have never been examined prospectively. The distribution of 23% p210 and 77% p190 in adults reported here is similar to 15% and 85%, respectively, reported in pediatric ALL by Sury- anarayan et al using PCR.29 These molecular and clinical findings underscore the similarities of adult and pediatric
c .- 0 0.6- - .L. -.-I BCR-ABL-/CALLA+ r 0 p.
BCR-ABL- 2 a 0.4-
BCR-ABL+/CALLA+
I I I
0 1 2 3
Years
Fig 3. Survival for all patients, and for a selected subgroup, treated on CALGB protocols. The groups are: BCR-ABL-negative cases (31 patients), BCR-ABGpositive cases (14 patients); BCR-ABL-negative, CALLA-positive cases (22 cases); BCR-ABL-positive, CALLA-positive cases (12 cases). There are no significant differences in survival between the BCR-ABL positives and negatives either overall (P = .26) or within the CALLA-positive subgroup (P = .15).
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom

PHILADELPHIA-POSITIVE ALL IN ADULTS 2989
Phl-positive ALL, which share more features with each other than with other types of ALL in the same age groups, supporting a view that BCR-ABL-positive ALL is a single clinical entity with a broad age range.
and p e d i a t r i ~ * ~ J ~ ALL show that the presence of a Phl chromosome is associated with low remission rates and shortened survival; these findings have been especially marked in pediatric ALL, in which long-term survival is frequent among the Phl-negative cases. The results of the present study differ somewhat, as the aggressive, multiagent chemotherapy that was used produced a high overall remission rate of greater than 70% in both the BCR-ABGpositive and BCR-ABGnegative groups. Despite this, the BCR-ABL cases showed a trend toward shorter remission duration that was especially marked in certain subgroups; in the CALLA-positive cases; in particular, the BCR-ABL marker identified cases with a short remission duration among those that otherwise would appear to do extremely well. This observation warrants further study, as the CALLA-positive cases make up a sizable majority of adult ALL cases. The shortened remis- sion duration has not yet translated into statistically signifi- cant survival differences, but follow-up is still early.
The present study underscores the limitations of cytoge- netics for the diagnosis of the BCR-ABL gene in ALL; adequately banded metaphases are difficult to obtain and, even when adequate, may fail to detect a Ph* chromosome. The finding of a positive molecular test for the BCR-ABL fusion in the face of Phl-negative cytogenetics has been well documented in CML? and this emphasizes the importance of confirmatory molecular analysis. Several molecular meth- ods have been used to detect the BCR-ABL fusion in ALL,8 including PFG,22 polymerase chain reaction (PCR),29,32-33 and fluorescence in situ h y b r i d i ~ a t i o n . ~ ~ - ~ ~ Southern blot analysis as used in CML7 is inadequate because breakpoints occur outside of the 5.8-kb breakpoint cluster region, in an area much larger than can be surveyed by standard meth- ods. Results obtained with any acceptable molecular method should be similar and allow comparisons with other clinical trials. Although PCR is now the preferred method for speed and cost considerations, the PFG approach used here has been shown to be ~ o m p a r a b l e . ~ ~
In summary, this study demonstrates that the BCR-ABL fusion gene is a common finding in adult ALL, and defines a group of pre-B-cell ALL with similar features in all age
Previous studies in
groups. The effect on clinical outcome depends somewhat on the comparison group, but these preliminary results suggest that the BCR-ABL cases are easily induced into remission with aggressive chemotherapy and fail because of early relapse. If so, this group might benefit by early intensification, such as allogeneic bone marrow transplanta- tion. It will be necessary to test this hypothesis with a larger population, ideally combined with close monitoring by molecular methods to elucidate the effects of treatment and the extent of residual disease, to confirm remission, and to predict relapse.
ACKNOWLEDGMENT
We thank A. Bliznik, K. Hallsworth, and M. Rosen for expert technical assistance, and R. Mick for helpful discussions on statistical analysis. The following CALGB principal investigators, cytogeneticists, and institutions participated in this study: Univer- sity of Chicago, Chicago, IL-Nicholas Vogelzang and Michelle Le Beau (Grant No. CA 41287); Dartmouth-Hitchcock Medical Cen- ter-Gibbons Cornwell, 111, and Doris Wurster-Hill (Grant No. CA 04236); Duke University, Durham, NC-Donald Trump and Sandra H. Bigner (Grant No. CA 47577); University of Iowa, Iowa City, IA-Gerald Clamon and Shivanand R. Patil (Grant No. CA 47642); Long Island Jewish Medical Center, New Hyde Park, NY-Kanti Rai and Prasad R.K. Koduru (Grant No. CA 11028); University of Maryland Cancer Center, Baltimore, MD-Joseph Aisner and Stuart Schwartz (Grant No. CA 31983); McGill Cancer Center, Montreal, Canada-Bernard Cooper and Jacqueline Emond (Grant No. CA 31809); University of Minnesota, Minneap- olis, MN-Bruce Peterson and Diane Arthur (Grant No. CA 16450); University of Missouri, Little Rock, AR-Michael Perry and Jeffrey Sawayer (Grant No. CA 12046); Mt. Sinai School of Medicine, New York, NY-James F. Holland and Vesna Najfeld (Grant No. CA 04457); New York Hospital-Cornell Medical Center, New York, NY-Richard T. Silver and Ram S. Verma (Grant No. CA 07968); University of North Carolina, Chapel Hill, NC-Howard Ozer and Kathleen W. Rao; Island Hospital, Provi- dence, RI-Louis Leone, Hon Fong, and Louie Mark (Grant No. CA 39097); Roswell Park Cancer Institute, Buffalo, NY-Clara Bloomfield. AnneMarie Block (Grant No. CA 37027); State University of New York Health Science Center at Syracuse, Syracuse, NY-David Duggan and Constance K. Stein (Grant No. CA 21060); University of Tennessee, Memphis, TN-Alvin Mauer and Sugandhi A. Tharapel (Grant No. CA 47555); Walter Reed Army Medical Center, Washington, DC-Raymond Weiss and Rawatmal Surana (Grant No. CA 26806); Washington University Medical Center, St. Louis, MO-Alan Lyss and Michael Watson (Grant No. CA 47546).
REFERENCES 1. Heisterkamp N, Stephenson JR, Groffen J, Hansen PF, de
Klein A, Bartram CR, Grosveld G: Localization of the c-ab1 oncogene adjacent to a translocation breakpoint in chronic myelo- cytic leukemia. Nature 306:765, 1983
2. Nowell PC, Hungerford DA: A minute chromosome in human chronic granulocytic leukemia. J Natl Cancer Inst 25:85, 1960
3. Daley GQ, Van Etten RA, Baltimore D: Induction of chronic myelogenous leukemia in mice by the p210bcr'ab' gene of the Philadelphia chromosome. Science 247:824,1990
4. Kelliher MA, McLaughlin J, Witte ON, Rosenberg N: Induc- tion of chronic myelogenous leukemia-like syndrome in mice with v-ab1 and BCR/ABL. Proc Natl Acad Sci USA 87:6649,1990
5. Elefanty AG, Hariharan IK, Cory S: Bcr-abl, the hallmark of chronic myeloid leukaemia in man, induces multiple haematopoi- etic neoplasms in mice. EMBO J 9:1069,1990
6. Heisterkamp N, Jenster G, ten Hoeve J, Zovich D, Pattengale PK, Groffen J: Acute leukemia in bcr/abl transgenic mice. Nature 344:251,1990
7. Kurzrock R, Gutterman JU, Talpaz M: The molecular genet- ics of Philadelphia chromosome-positive leukemias. N Engl J Med 319:990,1988
8. Hooberman AL, Westbrook CA. Molecular diagnosis of the Philadelphia chromosome in acute lymphoblastic leukemia. Leuke- mia Lymphoma 1:3,1989
9. Bloomfield CD, Rowley JD, Goldman AI, Alimena G, Berger
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
2990 WESTBROOK ET AL
R, Borgstrom GH, Brandt L, Catovsky D, de la Chapelle A, Dewald GW, Garson OM: Third International Workshop on Chromosomes in Leukemia: Chromosomal abnormalities and their clinical significance in acute lymphoblastic leukemia. Cancer Res 435368,1983
10. Ribiero RC, Abromowitch M, Raimondi SC, Murphy SB, Behm F, Williams DL: Clinical and biologic hallmarks of the Philadelphia chromosome in childhood acute lymphoblastic leuke- mia. Blood 70:948, 1987
11. Bloomfield CD, Goldman AI, Alimena G, Berger R, Borg- strom GH, Brandt L, Catousky D, de la Chapelle A, Dewald GW, Garson OM, Garwicz S, Golumb HM, Hossfeld DK, Lawler SD, Mitelman F, Nilsson P, Pierre RV, Phillip P, Prigogina E, Rowley JD, Sakurai M, Sandberg AA, Walker LMS, Tricot G, Van Den Berghe H, Van Orshoven A, Vuopio P, Whang-Peng J: Chromo- somal abnormalities identify high-risk and low-risk patients with acute lymphoblastic leukemia. Blood 67:415, 1986
12. Crist W, Carroll A, Shuster J, Jackson J, Head D, Borowitz M, Behm F, Link M, Steuber P, Ragab A, Hirt A, Bvork B, Land V, Pullen J: Philadelphia chromosome positive childhood acute lym- phoblastic leukemia: Clinical and cytogenetic characteristics and treatment outcome. A Pediatric Oncology Group Study. Blood 76:489,1990
13. Fletcher JA, Lynch EA, Kimball VM, Donnelly M, Tantra- vahi R, Sallan SE: Translocation (9;22) is associated with extremely poor prognosis in intensively treated children with acute lympho- blastic leukemia. Blood 77:435,1991
14. Fletcher JA, Kimball VM, Lynch E, Donnelly M, Pavelka K, Gelber RD, Tantravahi R, Sallan SE: Prognostic implications of cytogenetic studies in an intensively treated group of children with acute lymphoblastic leukemia. Blood 74:2130, 1989
15. Bartram CR: Rearrangement of the c-ab1 and bcr genes in Ph-negative CML and Ph-positive acute leukemias. Leukemia 263, 1988
16. Cuttner J, Mick R, Budman DR, Mayer RJ, Lee EJ, Henderson ES, Weiss RB, Paciucci PA, Sobol R, Davey F: Phase 111 trial of brief intensive treatment of adult acute lymphocytic leukemia comparing daunorubicin and mitoxantrone. Leukemia 5:425,1991
17. Larson R A Acute leukemia in adults, in Rake1 RE (ed): Conn’s Current Therapy. Philadelphia, PA, Saunders, 1991, p 352
18. Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DA, Gralnick HR, Sultan C: The French-American-British (FAB) Cooperative Group. The morphologic classification of acute lym- phoblastic leukemia. Concordance among observers and clinical correlations. Br J Hematol47:553,1981
19. Catovsky D, de Salvo Cardullo L, O’Brien M, Morilla R, Costello C, Galton D, Ganeshaguru K, Hofirand V: Cytochemical markers of differentiation in acute leukemia. Cancer Res 41:4824, 1981
20. Williams WJ, Beutler E, Erslev AJ, Lichtman M A Hematol- ogy (ed 4). New York, McGraw-Hill, 1990, p 1745
21. Westbrook CA, Rubin CM, Carrino JJ, Le Beau MM, Bernards A, Rowley JD: Long-range mapping of the Philadelphia chromosome using pulsed-field gel electrophoresis. Blood 71:697, 1989
22. Hooberman AL, Rubin CM, Barton KP, Westbrook CA:
Detection of the Philadelphia chromosome in acute lymphoblastic leukemia by pulsed-field gel electrophoresis. Blood 74:1101,1989
23. Bloomfield CD, Wurster-Hill D, Peng G, Le Beau MM, Tantravahi R, Testa J, Davey FR, Ellison RR, Cuttner J, Schiffer C, Sobol RE, Lunghofer B, Carey M, Mick R, Arthur D: Prognostic significance of the Philadelphia chromosome in adult acute lympho- blastic leukemia, in Gale RP, Hoelzer D (eds): Acute Lympho- blastic Leukemia. UCLA Symposia on Molecular and Cellular Biology, New Series, vol 108. New York, NY, Wiley-Liss, 1990,
24. International System for Cytogenetic Nomenclature (1985): An International System for Human Cytogenetic Nomenclature. Harnden DG, Klinger HP (eds); published in collaboration with Cytogenet Cell Genet, Basel, Switzerland, Varger, 1985
25. Sobol RE, Mick R, Royston I, Davey FR, Ellison RR, Newman R, Cuttner J, Griffin JD, Collins H, Nelson DA: Clinical importance of myeloid antigen expression in adult acute lympho- blastic leukemia. N Engl J Med 316:1111-1117, 1987
26. Kalbfleisch JD, Prentice R L The Statistical Analysis of Failure Time Data. New York, NY, Wiley, 1980
27. Kaplan EL, Meier P: Nonparametric estimation from incom- plete observations. J Am Stat AssoC 53:457,1958
28. Snedecor GW, Cochran WG, Statistical Methods (ed 7). Ames, IA, Iowa State University, 1980
29. Suryanarayan K, Hunger SP, Kohler S, Carroll AJ, Crist W, Link MP, Cleary ML: Consistent involvement of the BCR gene by 9;22 breakpoints in pediatric acute leukemias. Blood 77:324, 1991
30. Radford JE Jr, Burns CP, Jones MP, Gingrich RD, Kemp JD, Edwards RW, McFadden DB, Dick FR, Wen BC: Adult Acute Lymphoblastic Leukemia: Results of the Iowa HOP-L Protocol. J Clin Oncol7:58,1989
31. Kantarjian HM, Walters RS, Keating MJ, Smith TL, O’Brien S, Estey EH, Huh YO, Spinolo J, Dicke K, Barlogie B: Results of the vincristine, doxorubicin, and dexamethasone regimen in adults with standard and high-risk acute lymphoblastic leukemia. J Clin Oncol8:994,1990
32. Kawasaki ES, Clark SS, Coyne MY, Smith SD, Champlin R, Witte ON, McCormick FP: Diagnosis of chronic myeloid and acute lymphocytic leukemias by detection of leukemia-specific mRNA sequences amplified in vitro. Proc Natl Acad Sci USA 85:5698, 1988
33. Hooberman AL, Carino JJ, Leibowitz D, Rowley JD, LeBeau MM, Arlin ZA, Westbrook C A Unexpected heterogeneity of BCR-ABL fusion mRNA detected by polymerase chain reaction in Philadelphia chromosome-positive acute lymphoblastic leukemia. Proc Natl Acad Sci USA 86:4259,1989
34. Tkachuk DC, Westbrook CA, Andreeff M, Donlon TA, Cleary ML, Suryanarayan K, Homge M, Redner A, Gray J, Pinkel D: Detection of bcr-ab1 fusion in chronic myelogenous leukemia by in situ hybridization. Science 250:539,1990
35. Arnoldus EPJ, Weigant J, Noordermeer IA, Wessels JW, Beverstock GC, Grosveld GC, van de Ploeg M, Raap AK: Detec- tion of the Philadelphia chromosome in interphase nuclei. Cyto- genet Cell Genet 54:108,1990
36. Yaremko ML, Westbrook CA, Hooberman A L Rapid diagnosis of the Philadelphia chromosome in acute lymphoblastic leukemia by direct DNA fluorescence in situ hybridization. Am Assoc Cancer Res 32:164,1991 (abstr)
p 101
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom
1992 80: 2983-2990
Sobol, C Schiffer and CD BloomfieldCA Westbrook, AL Hooberman, C Spino, RK Dodge, RA Larson, F Davey, DH Wurster- Hill, RE
(8762)lymphoblastic leukemia: a Cancer and Leukemia Group B Study Clinical significance of the BCR-ABL fusion gene in adult acute
http://www.bloodjournal.org/content/80/12/2983.full.htmlUpdated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
For personal use only.on April 4, 2019. by guest www.bloodjournal.orgFrom