co-1 avastin ® (bevacizumab) united states food and drug administration oncologic drugs advisory...
TRANSCRIPT

CO-1
Avastin® (bevacizumab)
United States Food and Drug AdministrationOncologic Drugs Advisory Committee
December 5, 2007

CO-2
Overview
David Schenkein, MD
Senior VP, Clinical Hematology/OncologyGenentech, Inc.

CO-3
Overview Topics
• Indication statement
• Avastin Overview
• E2100 Summary
• Today’s Agenda

CO-4
Indication Statement
Avastin®, in combination with paclitaxel, for the treatment of patients who have not received chemotherapy for their locally recurrent or metastatic HER2-negative breast cancer.

CO-5
Avastin Overview
• Monoclonal antibody specific for VEGF ligand
• Validated antiangiogenesis in cancer therapy
– > 200,000 patients treated worldwide with Avastin
• Clinical validation in numerous settings
– Avastin approved
• Colorectal cancer and non-small cell lung cancer (worldwide)
– Progression-free and overall survival
• Metastatic breast cancer (ex-US)
– Progression-free survival (PFS)

CO-6
Avastin Milestone Developments in Metastatic Breast Cancer
E2100 1st-line MBC
2002 20041989 1997 2000 2005
VEGF-A cloned
IND for Avastin
AVF0776 Phase I/II MBC
AVF21192nd/3rd-line MBC
2001
GNE/NCI Clinical
Research Agreement
Avastin Approved Colorectal
Cancer

CO-7
ECOG Study E2100—Regulatory Milestones
2002 2005 2006 2007 2008
GNE/FDAPresubmission
Meeting
E2100 Ph III FL MBC
First Interim
Agency Request
for More Data
E2100 BLA SupplementResubmitted
E2100 BLA SupplementSubmitted

CO-8
Key Agreements With FDA to Support Resubmission (1)
• Independent Review Facility (IRF) assessment of all 722 patients
• Primary endpoint PFS by IRF review
• Data cut-off in line with ECOG interim analysis applied to final clean database
• Mature survival data

CO-9
Key Agreements With FDA to Support Resubmission (2)
Studies included in sBLA
Efficacy Safety Patient population
E2100 1st-line MBC
AVF2119 Prior anthracycline and taxane treated
AVF0776 Relapsed MBC

CO-10
Study E2100 Summary
• Avastin + paclitaxel associated with compelling treatment effect
• PFS appropriately measured
– Consistency across subsets
– Sensitivity analyses retained benefit
• Objective Response Rate (ORR) improved
• Overall Survival (OS) improved
• Favorable benefit/risk ratio
– No new safety signals observed
• Important advance for women with breast cancer

CO-11
Avastin in Metastatic Breast Cancer
• E2100 demonstrates a robust and clinically meaningful PFS treatment effect
• A PFS effect of this magnitude represents clinical benefit
• Genentech has committed to a full understanding of Avastin’s role in breast cancer

CO-12
David Schenkein, MDGenentech, Inc.
Overview
Kathy Miller, MDIndiana University
Study E2100: Design, Efficacy
Barbara Klencke, MDGenentech, Inc.
Study E2100: Safety
Eric Winer, MDDana-Farber Cancer InstituteHarvard Medical School
MBC and Bevacizumab:Placing ECOG Study 2100 in Context
Chris Bowden, MDGenentech, Inc.
Concluding Remarks
Today’s Agenda

CO-13
ECOG Study E2100:Avastin Added to Weekly Paclitaxel as Initial Chemotherapy for Patients
With Metastatic Breast Cancer
Kathy Miller, MD
Associate ProfessorIndiana University School of Medicine

CO-14
Topics
• Metastatic Breast Cancer Treatment Landscape
• E2100 Study Design Rationale
• E2100 Efficacy Data

CO-15
Metastatic Breast Cancer
• Overt metastatic disease is generally incurable
• Goal of therapy
– Live longer and prosper
• Chemotherapy
– Drug resistance is common
– Substantial toxicity

CO-16
Treatment Landscape 2001
0 5 10 15 20 25 30 35
Months
PFS OS
VATH/CMFVP1
FEC2
Paclitaxel3
EM4
Docetaxel5
DV6
Doxorubicin7
1Aisner. JCO. 1995; 2Brufman. Ann Oncol. 1997; 3Bishop. Sem Oncol. 1997; 4Pacini. Eur J Cancer. 2000; 5Chan. JCO. 1999; 6Norris. JCO. 2000; 7Parideans. JCO. 2000.

CO-17
Treatment Landscape 2007—Little Progress With Chemotherapy
0 5 10 15 20 25 30 35
Months
PFS OS
AT1
AT2
GT3
wkly Paclitaxel4
Docetaxel5
GET6
GV7
1Jassem. JCO. 2001; 2Sledge. JCO. 2003; 3Albain. Proc ASCO. 2004; 4Seidman. Proc ASCO. 2004; 5Jones. JCO. 2005; 6Zielinski. JCO. 2005; 7Martin. Lancet Oncology. 2007.

CO-18
Rationale for E2100
• Importance of angiogenesis
• Taxanes have antiangiogenic activity and are synergistic with Avastin
• AVF0776: Avastin activityas monotherapy
• AVF2119: Ongoing phase III trial in refractory disease
• Greater benefits expected earlier in natural history
Pragmatic
Biologic Clinical
• Intravenous placebo considered barrier to accrual

CO-19
MBC not previously treated with
chemotherapy
(N = 685)
Stratification
- Disease-free interval
- Adjuvant therapy
- ER+, ER–, unknown
- Number of metastatic sites
Paclitaxel: 90 mg/m2 IV infusion over 1 hr every wk for 3 wk followed by 1 wk of rest
Avastin: 10 mg/kg following paclitaxel treatment on Wk 1 and 3 of every cycle
R
A
N
D
O
M
I
Z
E
D
Paclitaxel: 90 mg/m2 IV infusion over 1 hr every wk for 3 wk followed by 1 wk of rest
E2100—Study Design

CO-20
E2100—Endpoints
• Primary endpoint
– Progression-free survival (PFS)
• Secondary endpoints
– Objective response rate (ORR)
– Overall survival (OS)
– Quality of life (QoL)
– Safety

CO-21
Rationale for Progression-Free Survival as the Primary Endpoint for E2100
• Important endpoint in the first-line setting
• Clinical benefit from prolonging PFS
– Maintain disease control
– Prevent symptoms of disease progression
– Prevent toxicities, psychological burden, and uncertainty of disease progression
• PFS endpoint not obscured by subsequent therapy

CO-22
Statistical Considerations
• Primary endpoint: PFS
– N = 685
– 85% power to detect a 33% improvement
• 6 vs 8 mo
– Interim analyses after 50% and 78% events
– Final analysis after 546 events
• Secondary endpoint: OS
– 15% to 25% power to detect 2- to 3-mo improvement

CO-23
E2100—Key Eligibility Criteria
• Disease setting
– Locally recurrent or metastatic breast cancer (mBC)
– HER2+ only if pretreatment with Herceptin or unsuitable
– Measurable or non-measurable disease
• Prior therapy
– No prior chemotherapy for mBC
– Adjuvant taxanes if > 12 mo prior to randomization
• Baseline requirements
– No CNS metastases
– Performance status
• ECOG 0 or 1

CO-24
Assessment Frequency (timing)
Clinical evaluation Every cycle (every 4 wk)
Safety assessment Every cycle (every 4 wk)
Tumor assessment(scan or x-ray)
Every 3 cycles (every 12 wk)Balanced assessments on both arms
QoL (FACT-B) Baseline, Wk 17, and Wk 33
E2100—Assessments

CO-25
Participating Centers
• 10 major cooperative groups participated
• 258 enrolling centers
– US, Canada, Peru, South Africa
– < 10% of patients enrolled ex-US

CO-26
ECOG Study E2100:Efficacy Results

CO-27
E2100 Baseline Characteristics—Balanced
Paclitaxel(n = 354)
Paclitaxel + Avastin(n = 368)
Median age, years (range) 55 (27 - 85) 56 (29 - 84)
≥ 65 years, % 23 23
Measurable disease at baseline, % 77 68
ER+ and/or PR+, % 64 63
HER2+, % 1.7 2.7
Disease-free interval ≤ 24 mo, % 41 41
≥ 3 metastatic sites, % 29 29
Prior adjuvant chemotherapy, % 65 66
Prior adjuvant anthracyclines, % 51 50
Prior adjuvant taxane therapy, % 19 20
Metastatic hormonal therapy, % 36 36

CO-28
Paclitaxel(n = 354)
Paclitaxel + Avastin
(n = 368)
Patients with an event, n (%) 184 (52) 173 (47)
Stratified analysis
HR 0.483
95% CI (0.385, 0.607)
p value
Log-rank 0.0001
PFS, mo
Median 5.8 11.3
95% CI (5.36, 8.15) (10.45, 13.27)
E2100—PFS by Independent Radiology Facility (IRF)

CO-29
0.8
0.6
0.4
0.2
0.0
1.0
3630241260
Pro
port
ion
with
out
even
t
HR = 0.483 (0.385, 0.607)
Log-rank test, p ≤ 0.0001
Paclitaxel (n = 354)
Paclitaxel + Avastin (n = 368)
18
Time, mo
E2100—PFS by IRF (Kaplan-Meier)

CO-30
Exploratory Analyses of PFS
1. PFS in key subsets
2. IRF vs Investigator-assessed progression
3. Sensitivity analyses

CO-31
All Patients Age < 40 yr
Age 40 - 64 yr
Age ≥ 65 yr
< 3 Metastatic sites
≥ 3 Metastatic sites
Measurable disease at baseline
Non-measurable disease at baseline No prior adjuvant chemotherapy Prior adjuvant chemotherapy Prior adjuvant TAXANE therapy
ER+
ER–
E2100—PFS Consistent Across Subgroups
Paclitaxel betterPaclitaxel + Avastin better
0.50.2 521Hazard ratio

CO-32
Exploratory Analyses of PFS
1. PFS in key subsets
2. IRF vs Investigator-assessed progression
3. Sensitivity analyses

CO-33
11.3
0.8
0.6
0.4
0.2
0.0
1.0
18 3630241260
Pro
port
ion
with
out
even
t
HR = 0.483
PAC
PAC + AVA
PFS by IRF
E2100—PFS Consistent Between IRF and Investigator
5.8
11.4
HR = 0.421
PAC
PAC + AVA
PFS by investigator
5.8
Months

CO-34
Exploratory Analyses of PFS
1. PFS in key subsets
2. IRF vs Investigator-assessed progression
3. Sensitivity analyses

CO-35
Median PFS
PFS analysis variationPAC
(n = 354)
PAC + AVA
(n = 368) HR p value
Primary analysis 5.8 11.3 0.48 < 0.0001
Investigator Progression not confirmed by IRF:
• Paclitaxel alone: Censor
• Avastin arm: Assume progression
5.8
9.2 0.60 < 0.0001
Sensitivity Analyses—Significant Benefit Retained Even if Avastin Arm Penalized
CSR Table 15

CO-36
Secondary Analyses
• Objective Response Rate
• Overall Survival
• Quality of Life

CO-37
0
10
20
30
40
50
60
CR PR SD PD UE
PAC
PAC + AVA
* Stratified analysis of CR + PR comparison, p < 0.0001
0%
22%
50%*
44%
34%
26%
12%Be
st r
esp
onse
, %Best Overall Response by IRFPatients With Measurable Disease at Baseline
9%5%

CO-38
0
10
20
30
40
50
60
CR + PR CR + PR
Be
st r
esp
onse
, %
E2100—Objective Response by Investigators and IRFPatients With Measurable Disease at Baseline
Investigator assessment IRF assessment
50%
22%23%
48%
PACPAC + AVA

CO-39
Paclitaxel(n = 354)
Paclitaxel + Avastin
(n = 368)
Patients who died, n (%) 238 (67.2) 243 (66)
Stratified analysis
HR 0.869
95% CI (0.722, 1.046)
p value
Log-rank 0.1374
Overall survival, mo
Median 24.8 26.5
95% CI (21.39, 27.37) (23.72, 29.21)
Note: Data are based on a 21 October 2006 cutoff.
Overall Survival

CO-40
E2100—Overall Survival
PAC+AVA 104103
00
58
2319
344307PAC
4848
193165
No. of patients at risk
249215
368354
297258
HR = 0.869 (0.722, 1.046)
Log-rank test, p = 0.1374
PAC (n = 354): Median OS 24.8 mo
PAC + AVA (n = 368): Median OS 26.5 mo0.8
0.6
0.4
0.2
0.0
1.0
543630 6048420
Pro
por
tion
surv
ivin
g
18 24126
0.8
0.6
0.4
0.2
0.0
1.0
543630 6048420 18 24126
* Post-hoc
Months
p = 0.017*
74.0%
81.4%
50.1%
55.0%
p = 0.191*

CO-41
E2100—Quality of Life: Primary Analysis Favors Avastin Therapy
-24.6
-15.9
-12.7
-6.6
-30
-25
-20
-15
-10
-5
0
Baseline Wk 17 Wk 33
PAC
PAC + AVADecline
Change from baseline for Trial Outcome Index-Breast
Patients with QoL data
PAC N =
PAC + AVA N =
327
347
290
318
296
292
p = 0.0069
p = 0.0002

CO-42
E2100—Efficacy Conclusions for Avastin + Paclitaxel
• Clinically meaningful improvement in PFS
– Magnitude of PFS benefit consistent for all patient subgroups
– Similar PFS results based on IRF or investigator assessments validates ECOG review process
– Robust PFS result verified by sensitivity analyses
• Doubling of ORR, with improvement in 1-year survival and no additional QoL burden

CO-43
ECOG Study E2100:Safety
Barbara Klencke, MD
Associate Group Medical DirectorGenentech, Inc

CO-44
Paclitaxel(n = 342)
Paclitaxel + Avastin (n = 358)
Cycles* received per patient
Median 6 10
Range 1 - 26 1 - 38
25th - 75th percentile 3 - 9 6 - 15
*1 cycle = 4 weeks.
E2100—Treatment Received

CO-45
Status and reason for discontinuation
Paclitaxel(n = 354)
(%)
Paclitaxel + Avastin(n = 368)
(%)
Total(N = 722)
(%)
Not treated 2.3 0.5 1.4
Treatment ongoing 2 11 7
Discontinued protocol therapy 96 89 92
Disease progression 55 45 50
Toxicity/side effects/complications 19 20 20
Death 1.4 1.6 1.5
Other 20 22 21
Reasons for Treatment Discontinuation

CO-46
Paclitaxel(n = 348)
%
Paclitaxel +Avastin
(n = 363)%
Death events 73.6 70.2
Due to MBC 69.3 66.9
Due to protocol therapy 0.3 0.0
Due to other cause 2.0 2.5
Unknown 2.0 0.8
E2100: Investigator-Reported Cause of Death in Safety Population

CO-47
Deaths
Paclitaxel(n = 348)
n (%)
Paclitaxel +Avastin
(n = 363)n (%)
All deaths 256 (73.6) 255 (70.2)
Due to protocol therapy Not assessable by
Genentech6 (1.7)
E2100—Causes of Death:Comprehensive Genentech Clinical Review

CO-48
NCI-CTCAE Term Grade ≥ 3
Paclitaxel (n = 348)
(%)
Paclitaxel + Avastin
(n = 363)(%)
Patients with ≥ 1 event 50.6 71.1
Neuropathy 18.1 25.3
Hypertension 1.4 16.0
Fatigue 5.2 10.7
Infection without neutropenia 4.6 9.1
Neutropenia (Grade 4) 3.2 5.8
Vomiting 2.3 5.5
Grade 3-5 nonhematologic and Grade 4-5 hematologic events included.
Most Frequent Grade 3-5 Adverse Events by Category and Preferred Term (≥ 5% Incidence)

CO-49
Paclitaxel(n = 348)
Paclitaxel + Avastin(n = 363)
Grade 3-5
1.4 16.0
0 3.6
0 3.0
0.3 2.2
0.3 2.2
0 0.6
Gr 3 Gr 4 Gr 5
15.4 0.6 0
1.1 1.9 0.6
1.9 1.1 0
1.7 0.6 0
1.9 0.3 0
0 0 0.6
Selected adverse events
Hypertension
Arterial thromboembolism
Proteinuria
Hemorrhage
Left ventricular dysfunction
GI perforations
E2100—Grade 3-5 Adverse Events: Categories of Special Interest (%) by Grade

CO-50
E2100—Safety Summary for Avastin + Paclitaxel
• Avastin + paclitaxel relatively well tolerated despite longer treatment
• Discontinuation for treatment toxicity equally balanced
• Safety profile consistent with known Avastin toxicity profile

CO-51
AVF2119—Study Design
Metastatic breast cancer • Measurable disease• Prior anthracycline + taxane
therapy required• HER2+ or HER2–
Primary endpoint• PFS by IRF
Stratification• ECOG performance status• Number of prior chemotherapy regimens
Capecitabine2500 mg/m2 q day × 14q 3 wk
Capecitabine2500 mg/m2 q day × 14
Avastin 15 mg/kgq 3 wk
N = 450
RANDOMIZE
1:1
CO-52
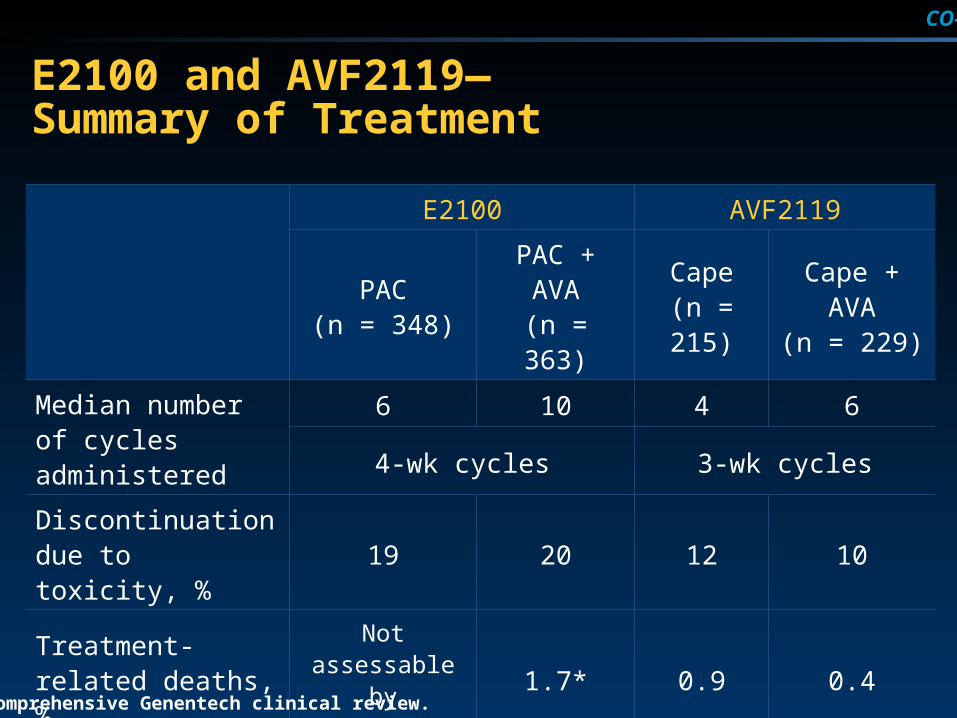
E2100 and AVF2119—Summary of Treatment
E2100 AVF2119
PAC(n = 348)
PAC + AVA(n = 363)
Cape(n = 215)
Cape + AVA(n = 229)
Median number of cycles administered
6 10 4 6
4-wk cycles 3-wk cycles
Discontinuation due to toxicity, %
19 20 12 10
Treatment-related deaths, %
Not assessable by Genentech
1.7* 0.9 0.4
*Comprehensive Genentech clinical review.

CO-53
AVF2119
Cape(n = 215)
Cape + AVA(n = 229)
0.5 20.0
0.5 0.4
0 1.3
0.5 0.4
1.0 3.5
0 0
0.9 0
E2100 and AVF2119g—Grade 3-5 Adverse Events: Categories of Special Interest (%)
Selected adverse events, Grade 3 - 5
E2100
PAC(n = 348)
PAC + AVA(n = 363)
Hypertension 1.4 16.0
Arterial thromboembolic events
0 3.6
Proteinuria 0 3.0
Hemorrhage 0.3 2.2
Left ventricular dysfunction
0.3 2.2
GI perforations 0 0.6
Neuropathy 18.1 25.3

CO-54
Avastin Safety Summary
• E2100 and AVF2119 report side effects consistent with current Avastin labeling
• Overall safety profile and QoL outcomes from E2100 support acceptability of the safety profile for Avastin + paclitaxel

CO-55
Metastatic Breast Cancer and Bevacizumab:Placing ECOG Study 2100 in Context
Eric Winer, MDDirector, Breast Oncology Center
Dana-Farber Cancer Institute
Associate Professor of Medicine Harvard Medical School
Chief Scientific AdvisorSusan G. Komen for the Cure

CO-56
Why Do We Develop New Therapies for Patients With Metastatic Breast Cancer?
• To improve treatment outcomes for women living with the disease today
• To identify promising new therapies that can be applied to the adjuvant setting

CO-57
How Do We Maximize Clinical Benefit forWomen With Metastatic Breast Cancer?
• Goals of treatment are to
– Maximize survival
• Median survival from initiation of first-line chemotherapy in HER2-negative disease is approximately 2 years
– Maintain disease control
– Minimize symptoms from disease
– Minimize toxicity from treatment
QUALITYOF LIFE

CO-58
Agents Approved for Metastatic Breast Cancer Since 2001
Drug Trial Size
Capecitabine Docetaxel + Capecitabine vs
Docetaxel
N = 511
Gemcitabine Paclitaxel + Gemcitabinevs
Paclitaxel
N = 529
Lapatinib Capecitabine + Lapatinib vs
Capecitabine
N = 324
Ixabepilone Capecitabine + Ixabepilonevs
Ixabepilone
N = 752
O’Shaughnessy. JCO. 2002; Melemed. ASCO Breast. 2007; Geyer. NEJM. 2006; Thomas. JCO. 2007.

CO-59
10 mo5 mo
MBC Tx—Recent Major Phase 3 Trials: Efficacy Results
20 mo10 mo
PFS/TTP
OS
1Miller. SABCS. 2005; 2O’Shaughnessy. JCO. 2002; 3Melemed. ASCO Breast. 2007; 4Geyer. NEJM. 2006; 5Thomas. JCO. 2007; NA: Not available.
Not reported yet
XD2
GT3
TyX4
IxX5
XDD
GTT
TvXX
IxXX
XD2
GT3
TyX4
IxX5
XDD
GTT
TvXX
IxXX

CO-60
PFS or TTP, mo
4 6 8 120 2 10
Phase III PFS/TTP Results in First-line Metastatic Breast Cancer Trials Utilizing Taxanes
ATFACJassem 2001
APACBiganzoli 2002
ADACNabholtz 2003
Pq wPq 3wSeidmann 2004
FACMackey 2002
GTTMelemed 2007
ADFACBontenbal 2005
GETFECZielinski 2005
ECETCarmichael 2001
Luck 2000 ETEC
E2100 Paclitaxel + BevacizumabPqw
ATTASledge 2003 T
Experimental arm
Control arm

CO-61
Is Prolonging Progression-Free Survival Meaningful for Patients?
• Improvements in progression-free survival
– Delay the onset of disease-related symptoms and the side effects from a new therapy
– Avoid the psychological consequences associated with disease progression and changing therapy
– Eliminate the uncertainty as to whether new treatment will be effective
Yes, prolonging progression-free survival can be highly meaningful!

CO-62
For Progression-Free Survival to Equal Patient Benefit, Then…
• The improvement in PFS must be
– Substantial in magnitude
– Established with confidence
– Supported by other measures of efficacy
• Survival
• QoL
• Objective response rate

CO-63
Applying These Criteria to the Combination of Paclitaxel + Bevacizumab
Criteria As demonstrated in ECOG 2100
Substantial in magnitude
PFS hazard ratio: 0.48 (p < 0.0001)
Established with confidence
Agreement between investigator and independent review
Sensitivity analyses
Supported by other measures of efficacy
OS hazard ratio: 0.87 (p = 0.14)
QoL favors bevacizumab
Doubling of response rate (p < 0.0001)

CO-64
10 mo5 mo
MBC Tx—Recent Major Phase 3 Trials: Efficacy Results
20 mo10 mo
PFS/TTP
OS
1Miller. SABCS. 2005; 2O’Shaughnessy. JCO. 2002; 3Melemed. ASCO Breast. 2007; 4Geyer. NEJM. 2006; 5Thomas. JCO. 2007; NA: Not available.
Not reported yet
XD2
GT3
TyX4
IxX5
E21001 TAT
XDD
GTT
TvXX
IxXX
XD2
GT3
TyX4
IxX5
E21001 TAT
XDD
GTT
TvXX
IxXX

CO-65
Longerprogression-free
survival
Side effects/risks from treatment
FrequencySeverity
Extent of improvement
The Trade-Off

CO-66
What Side Effects and Risks Must Be Accepted With Paclitaxel and Bevacizumab?
• 20% increase in Grade 3-5 toxicity
– Asymptomatic Grade 3 hypertension and proteinuria were the most common adverse events
• Neuropathy increase due to duration of treatment
• Small increase in severe toxicity
– Arterial thrombotic events
– Congestive heart failure
– GI perforation
– Bleeding
• Added day-to-day toxicity quite limited

CO-67
In Summary
• Progression-free survival is a meaningful endpoint
• The combination of bevacizumab and paclitaxel results in
– Substantial improvement in progression-free survival
– Modest additional toxicity for the majority of patients
• Bevacizumab in combination with paclitaxel is a valuable treatment option for women with metastatic breast cancer

CO-68
Concluding Remarks
Chris Bowden, MD
Senior Group Medical DirectorGenentech, Inc.

CO-69
E2100 Summary
• Benefit
– Clinically meaningful treatment effect on progression-free survival
– PFS supported by all secondary endpoints
• Risk
– Safety profile familiar to prescribing oncologists
• Confidence
– Independent cooperative group study
– Consistency across subsets, IRF vs investigator, multiple sensitivity analyses

CO-70
Indication Statement
Avastin® in combination with paclitaxel is indicated for the treatment of patients who have not received chemotherapy for their locally recurrent or metastatic HER2-negative breast cancer.

CO-71
Avastin®
Supportive Slides

CO-72
TAX(n54)
TAX/AV(n114)
No. of patients with an objective response 54 112 a
No. of patients with an event 22 (40.7%) 56 (50.0%)
Duration of objective response (months)
Median 9.7 9.4
95% CI (7.43, 12.62) (8.38, 13.31)
Unstratified Hazard Ratio (Relative to TAX) 0.838 (0.508, 1.382)
a Two patients (21061 and 29004) have negative durations of objective response because a PD was recorded prior to a PR. For Patient 21061, the PD was retracted in the reader comments; for Patient 29004, the PD date was kept and allowed to be followed by a best response of PR since PD was not assessed as a best response.
Duration of Objective Response Patients with Measurable Disease at Baseline and an Objective Response

CO-73
Subgroup Analysis of PFS (1)
Baseline Risk Factor
Total n n Median
(mo) n Median (mo)
Hazard Ratio (95% Cl)
All Patients 722 354 5.8 368 11.3 0.54 (0.44-0.67)
Age (yrs)
<40 59 32 4.8 27 8.3 0.54 (0.26-1.09)
40-64 496 239 6.1 257 12.1 0.51 (0.39-0.66)
≥65 167 83 6.1 84 10.4 0.67 (0.42-1.05)
Race
White 550 266 6.0 284 12.0 0.54 (0.42-0.69)
Non-White 172 88 5.6 84 10.9 0.55 (0.36-0.86)
Region
North America 663 324 5.8 339 11.2 0.55 (0.44-0.68)
Rest of the World 59 30 6.5 29 12.5 0.43 (0.19-0.94)
Disease Status
Locally recurrent 12 4 - 8 10.9 0.83 (0.09-8.04)
Metastatic 709 349 5.8 360 11.4 0.54 (0.44-0.67)
TAX better
TAX/AV better
0.50.2 521

CO-74
Subgroup Analysis of PFS (2)
Baseline Risk Factor
Total n n Median
(mo) n Median (mo)
Hazard Ratio (95% Cl)
All Patients 722 354 5.8 368 11.3 0.54 (0.44-0.67)
Disease-free intervals (months)
≤24 months 296 146 4.9 150 10.6 0.58 (0.42-0.79)
>24 months 426 208 8.3 218 12.1 0.50 (0.38-0.67)
ER status
Positive 446 223 7.7 223 11.9 0.59 (0.44-0.78)
Negative 265 127 4.9 138 11.1 0.44 (0.31-0.61)
Unknown 11 4 21.3 7 1.70 (0.15-19.07)
ER/PR/HER2 combined
Negative 232 110 5.3 122 10.6 0.49 (0.34-0.70)
All others 490 224 7.4 246 12.5 0.57 (0.44-0.75)
HER2 status
Positive 15 6 2.4 9 11.3 0.00 (0.00- )
Negative 650 316 6.1 334 11.1 0.57 (0.45-0.71)
Unknown 57 32 7.7 25 12.5 0.42 (0.19-0.93)
TAX better
TAX/AV better
0.50.2 521

CO-75
Subgroup Analysis of PFS (3)
Baseline Risk Factor
Total n n Median
(mo) n Median (mo)
Hazard Ratio (95% Cl)
All Patients 722 354 5.8 368 11.3 0.54 (0.44-0.67)
Number of metastatic sites
<3 514 252 6.6 262 13.3 0.53 (0.41-0.69)
≥3 208 102 4.8 106 8.3 0.56 (0.38-0.81)
Measurable Disease at baseline
No 250 111 4.1 139 16.6 0.37 (0.25-0.54)
Yes 472 243 6.7 229 10.7 0.66 (0.51-0.85)
SLD of target lessions (mm)
≤Median (76.00) 238 116 8.6 122 11.1 0.72 (0.50-1.03)
>Median 234 127 5.8 107 8.6 0.63 (0.44-0.91)
Prior adjuvant hormone therapy
Yes 343 175 6.1 168 12.4 0.56 (0.41-0.77)
No 379 179 5.5 200 11.1 0.52 (0.39-0.70)
Metastatic / Recurrence hormone therapy
Yes 262 128 6.0 134 11.9 0.53 (0.37-0.77)
No 460 226 5.8 234 11.1 0.55 (0.43-0.72)
TAX better
TAX/AV better
0.50.2 521

CO-76
Reasons for PFS censoring: Patients censored more than 90 days from data cutoff (%)
TAX
(n=354) TAX/AV
(n=368) Total
(n=722)
Patients censored more than 90 days prior to data cutoff
40 35 37
No scans or pertinent clinical information submitted to IRF
6 6 6
Non-protocol Therapy 15 13 14
Investigator PD not confirmed by IRF
15 9 12
Data cutoff 3 9 5