colony-forming units (cfu) - wydział lekarski
TRANSCRIPT

1
Diagnostic medical microbiology is the discipline that identifies etiologic agents of disease. The job of the clinical microbiology laboratory is to test specimens from patients for microorganisms that are, or may be, a cause of the illness and to provide information (when appropriate) about the in vitro activity of antimicrobial drugs against the microorganisms identified.
The staff of a clinical microbiology laboratory should be qualified to advise the physician as well as process specimens. The physician should supply salient information about the patient, such as age and sex, tentative diagnosis or details of the clinical syndrome, date of onset, significant exposures, prior antibiotic therapy, immunologic status, and underlying conditions. The clinical microbiologist participates in decisions regarding the microbiologic diagnostic studies to be performed, the type and timing of specimens to be collected, and the conditions for their transportation and storage. Above all, the clinical microbiology laboratory, whenever appropriate, should provide an interpretation of laboratory results.
Specimens selected for microbiologic examination should reflect the disease process and be collected in sufficient quantity to allow complete microbiologic examination. The number of microorganisms per milliliter of a body fluid or per gram of tissue is highly variable, ranging from less than 1 to or 1010 colony-forming units (CFU) [a unit used to estimate the number of viable bacterial or fungal cells in a sample].
CFU determine the number of culturable microorganisms (the larger the more microorganisms are present).
Because skin and mucous membranes have a large and diverse indigenous flora, every effort must be made to minimize specimen contamination during collection. Contamination may be avoided by various means. The skin can be disinfected before aspirating or incising a lesion. Alternatively, the contaminated area may be bypassed altogether. It is often impossible to collect an uncontaminated specimen, and
2
decontamination procedures, cultures on selective media, or quantitative cultures must be used. If possible, specimens should be collected before the administration of antibiotics. Above all, close communication between the clinician and the microbiologist is essential to ensure that appropriate specimens are selected and collected and that they are appropriately examined.
Because some pathogens possess characteristic morphologic features, staining properties, or movement, they can be accurately identified by direct microscopic examination of clinical material. For certain infections, microscopic diagnosis is highly sensitive and specific. It is also a rapid technique that sometimes permits the physician to initiate treatment without waiting for the results of a culture. Brightfield microscopy uses visible light as source of illumination. Specimens can be stained to visualize and characterize bacteria more easily using, for example, Gram stain, or the Ziehl-Neelsen technique if mycobacteria are suspected. Gram-stained smears of colonies of bacteria from culture plates can also be examined by this method. Useful information regarding infectious etiology can also often be obtained by histopathologists when they examine tissue specimens by light microscopy using a variety of different ‘special stains’.
Brightfield microscope observation
Darkfield microscopy causes the specimen to appear light against a dark background. This is useful for detecting microorganisms that are not easily seen by brightfield microscopy or cannot be easily stained, such as Treponema pallidum - the cause of syphilis - obtained from primary lesions.
Darkfield microscope observation
Fluorescence microscopy relies on the principle that fluorescent dyes (fluorochromes) absorb invisible short-wavelength (ultraviolet) light and give off visible light. Immunofluorescence uses fluorochrome-labelled antibodies that will bind to specific

3
antigens. This method is particularly useful for the diagnosis of direct tissue fragments containing microorganisms.
Live/dead staining used to assess bacterial viability by observing cells’ color (red - dead and green - live).
Although a species identification is rarely possible, bacterial pathogens may be visualized and assigned to morphologic and functional groups using special stains. The Gram staining is both rapid and simple to perform and can be carried out on virtually any body fluid or tissue sample. It can yield clinically useful information of three kinds:
1. The presence of bacteria in a normally sterile body fluid (e.g., CSF, pleural fluid, urine)
2. Staining properties and morphology of the microorganisms in a sample or culture that can direct the empirical selection of antibiotics for the patient (Gram-positive or Gram-negative)
Gram-negative rods Gram-positive bacilli Gram-negative cocci Gram-positive cocci
3. For certain clinical specimens, a diagnosis. For example, the presence of Gram-
negative diplococci inside the leukocytes of urethral pus is highly specific for gonococci. The same morphologic type seen in samples of CSF is nearly always the meningococcus.
Negative and positive growth of Neisseria meningitidis in the cerebrospinal fluid, respectively.
During observation, Gram-negative diplococci are present inside leukocytes.
Culturing is usually the most specific way to establish the presence of a particular pathogen in a patient sample. However, in many situations, culturing may not be sensitive or clinically practical. Culture is routine for most bacterial and fungal infections. Because Chlamydia and viruses are obligate intracellular pathogens, they can be propagated and

4
identified only in appropriate cell cultures (this method is not used in standard diagnostics). In many instances, the cause of an infection is confirmed by isolating and culturing microorganism either in artificial media or in a living host. Liquid media provide greater sensitivity for the isolation of small numbers of microorganisms; however, identification of mixed cultures growing in liquid media requires subculture onto solid media so that isolated colonies can be processed separately for identification. Growth in liquid media also cannot ordinarily be quantitated. Solid media, although somewhat less sensitive than liquid media, provide isolated colonies that can be quantified if necessary and identified. Some genera and species can be recognized on the basis of their colony morphologies.
Growth of microorganisms in liquid media is characterized by an increase of turbidity, whereas growth on solid media is characterized by the presence of countable colonies of microorganisms.
For quantitative cultures, a specific volume of specimen is spread over the agar surface and the number of colonies per milliliter is estimated. For semiquantitative cultures, an unquantitated amount of specimen is applied to the agar and diluted by being streaked out from the inoculation site with a sterile bacteriologic loop. The amount of growth on the agar is then reported semiquantitatively as many, moderate, or few (or 3+, 2+, or 1+ ), depending on how far out from the inoculum site colonies appear. A microorganism that grows in all streaked areas would be reported as 3+.
Isolation of microorganisms by a streak plate method.
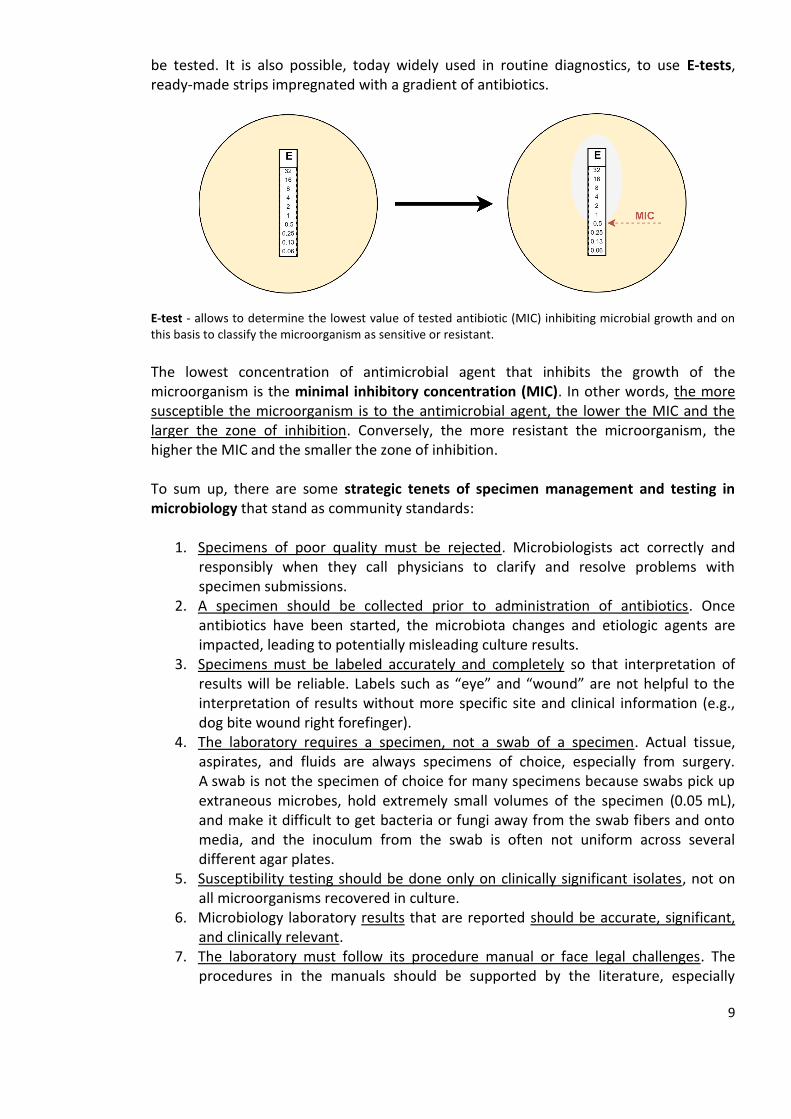
Cultures are generally incubated at 35 to 37°C in an atmosphere consisting of air, air supplemented with carbon dioxide (3-10%), reduced oxygen (microaerophilic conditions), or no oxygen (anaerobic conditions), depending upon requirements of the microorganism. Since clinical specimens from bacterial infections often contain aerobic, facultative anaerobic, and anaerobic bacteria, such specimens are usually inoculated into
5
a variety of general purpose, differential, and selective media, which are then incubated under aerobic and anaerobic conditions.
Types of oxygen requirements of different microorganisms.
The duration of incubation of cultures also varies with the growth characteristics of the microorganism. Most aerobic will grow overnight, whereas anaerobic bacteria require few days to grow. In general, the choices of culture method and medium are tailored to the nature and source of the specimen and the question that the culture is meant to address. For example, when a specimen of pus from a brain abscess is cultured, the implied question is, “What microorganisms are present in the abscess?” The assumption is that any microorganisms present are causative and that chemotherapy directed against them will be beneficial. To look for the etiologic agents, the sample is cultured on a variety of agar-based media and in a broth medium under both aerobic and anaerobic conditions.
As with all diagnostic methods, culture results require interpretation by the physician. In some situations (e.g., meningitis, urinary tract infection), a negative culture is quite reassuring that the etiology of the patient’s problem is not a bacterial or fungal infection. In other situations, the sensitivity of culture diagnosis is relatively poor.

6
Positive cultures always raise the question of whether the isolate is the actual cause of the patient’s illness. In cultures from nonsterile body sites, the problem is whether the isolate represents normal microbiota (colonization) or an etiologic agent (infection). In cultures from normally sterile body sites, contamination can occur when patient samples are obtained using faulty sterile technique.
Some microorganisms, such as Shigella dysenteriae, Coccidioides immitis and Mycobacterium tuberculosis, are always considered clinically significant. Others that ordinarily are harmless components of the indigenous flora of the skin and mucous membranes or that are common in the environment may or may not be clinically significant, depending on the specimen source from which they are isolated.

7
A huge variety of different types of media are used for many different purposes, depending on the type of specimen and the target organism. The ingredients of the media can be manipulated to set the best conditions suited to the purpose. Types of media fall into the following main categories: Enriched cultures Examples include blood agar, to which growth factors are sometimes added, and chocolate blood agar. These media are designed to support the growth of a wide range of bacteria. Enriched media are designed to facilitate the growth of fastidious microorganisms. The primary enrichment component is blood, which provides hemin and other nutrients. Selective cultures These media select for the growth of particular target microorganisms. Inhibitors, often antibiotics, are added to decrease the growth of untargeted microorganisms, while allowing the growth of the suspected pathogen. Such media are particularly useful for specimens from sites of the body with a commensal flora, where a target pathogen has to be picked out from the other bacteria present. Differential cultures These media allow preliminary identification to be made based on the colonial appearance. Some differential media make use of differences in metabolic properties combined with changes in pH to create colonies of different colors, helping the biomedical scientist quickly to distinguish pathogens from non-pathogens. Other media allow direct identification to species level from the colonial appearance.
Culture media used for routine diagnosis of microorganisms.
The first step in microbial identification is the phenotypic assessment of the growing colony. In many cases, the colonial morphology such as color, shape, size, hemolytic reaction, and growth characteristics on various selective and differential media can place an organism in a single family, genus, or even species level. In fact, assessing the ability of an organism to grow in various laboratory media and their oxygen requirement coupled with Gram-stain morphology and a few rapid tests such as catalase, oxidase, coagulase, and indole can provide preliminary identification for most of the clinically significant isolates.
Commercial biochemical identification systems are the backbone of microbial identification in clinical microbiology laboratories. They provide an advantage over

8
conventional identification systems by requiring little storage space, have an extended shelf life, rapid turn-around, low cost, standardized quality control, and ease of use.
The API identification systems consists of series of microcupules on a plastic strip that contain dehydrated substrates for the demonstration of enzymatic activity or the fermentation of carbohydrates. Depending on type of the microorganism and the API strip utilized, it may or may not require microbial growth.
Biochemical API test to determine the specie of the isolated bacterium.
The responsibility of the microbiology laboratory includes not only microbial detection and isolation but also the determination of microbial susceptibility to antimicrobial agents. Perhaps the most important advantage of culturing is that the isolate can be tested for susceptibility to antimicrobial agents, often the most important piece of therapeutically related information to be obtained. Antimicrobial susceptibility tests are performed by either disk diffusion or a dilution method. In the former, a standardized suspension of a particular microorganism is inoculated onto an agar surface to which paper disks containing various antimicrobial agents are applied. Following overnight incubation, any zone diameters of inhibition about the disks are measured and the results are reported as indicating susceptibility or resistance of the microorganism to each antimicrobial agent tested.
Disk-diffusion method - clear zones are measured and on this basis the tested microorganism is classified as sensitive or resistant.
An alternative method is to dilute each antimicrobial agent in broth to provide a range of concentrations and to inoculate each tube or, if a microplate is used, each well containing the antimicrobial agent in broth with a standardized suspension of the microorganism to
9
be tested. It is also possible, today widely used in routine diagnostics, to use E-tests, ready-made strips impregnated with a gradient of antibiotics.
E-test - allows to determine the lowest value of tested antibiotic (MIC) inhibiting microbial growth and on this basis to classify the microorganism as sensitive or resistant.
The lowest concentration of antimicrobial agent that inhibits the growth of the microorganism is the minimal inhibitory concentration (MIC). In other words, the more susceptible the microorganism is to the antimicrobial agent, the lower the MIC and the larger the zone of inhibition. Conversely, the more resistant the microorganism, the higher the MIC and the smaller the zone of inhibition. To sum up, there are some strategic tenets of specimen management and testing in microbiology that stand as community standards:
1. Specimens of poor quality must be rejected. Microbiologists act correctly and responsibly when they call physicians to clarify and resolve problems with specimen submissions.
2. A specimen should be collected prior to administration of antibiotics. Once antibiotics have been started, the microbiota changes and etiologic agents are impacted, leading to potentially misleading culture results.
3. Specimens must be labeled accurately and completely so that interpretation of results will be reliable. Labels such as “eye” and “wound” are not helpful to the interpretation of results without more specific site and clinical information (e.g., dog bite wound right forefinger).
4. The laboratory requires a specimen, not a swab of a specimen. Actual tissue, aspirates, and fluids are always specimens of choice, especially from surgery. A swab is not the specimen of choice for many specimens because swabs pick up extraneous microbes, hold extremely small volumes of the specimen (0.05 mL), and make it difficult to get bacteria or fungi away from the swab fibers and onto media, and the inoculum from the swab is often not uniform across several different agar plates.
5. Susceptibility testing should be done only on clinically significant isolates, not on all microorganisms recovered in culture.
6. Microbiology laboratory results that are reported should be accurate, significant, and clinically relevant.
7. The laboratory must follow its procedure manual or face legal challenges. The procedures in the manuals should be supported by the literature, especially

10
evidence-based literature. To request the laboratory to provide testing apart from the procedure manual places everyone at legal risk.
8. “Background noise” of commensal microbiota must be avoided where possible. Many body sites have normal, commensal microbiota that can easily contaminate the inappropriately collected specimen and complicate interpretation. Therefore, specimens from sites such as lower respiratory tract (sputum), nasal sinuses, superficial wounds, fistulae, and others require care in collection.
11
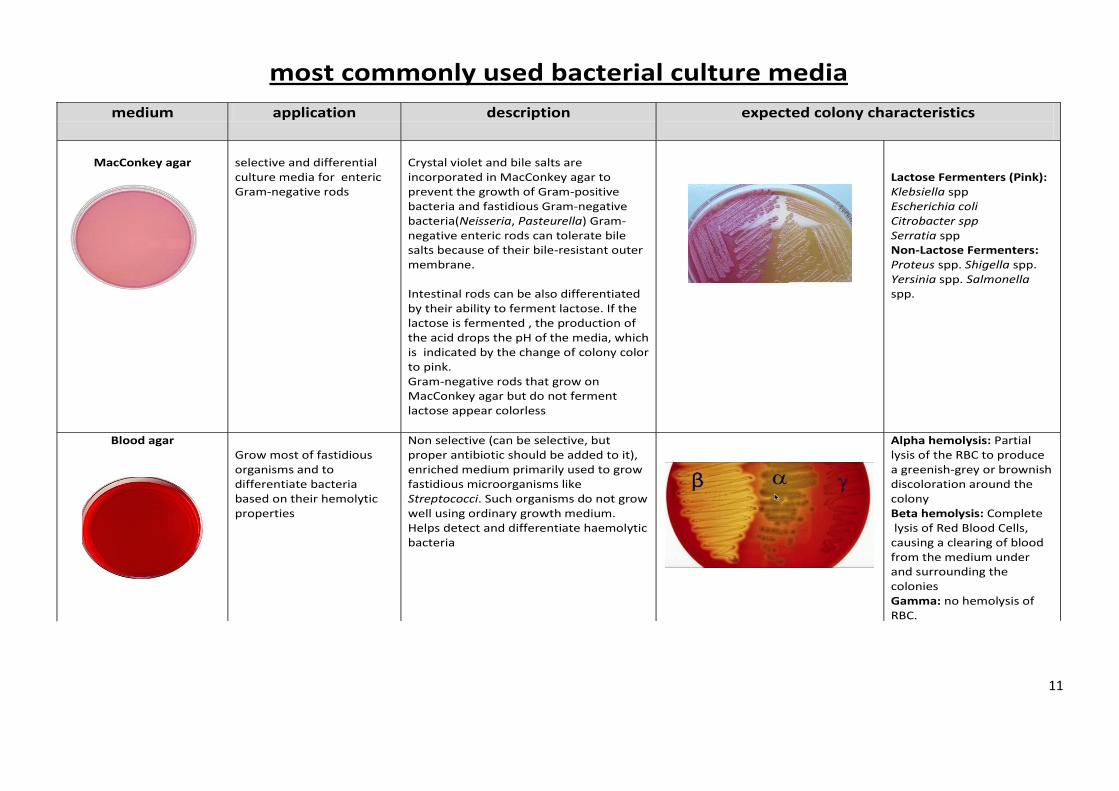
most commonly used bacterial culture media
medium application description expected colony characteristics
MacConkey agar
selective and differential culture media for enteric Gram-negative rods
Crystal violet and bile salts are incorporated in MacConkey agar to prevent the growth of Gram-positive bacteria and fastidious Gram-negative bacteria(Neisseria, Pasteurella) Gram-negative enteric rods can tolerate bile salts because of their bile-resistant outer membrane. Intestinal rods can be also differentiated by their ability to ferment lactose. If the lactose is fermented , the production of the acid drops the pH of the media, which is indicated by the change of colony color to pink. Gram-negative rods that grow on MacConkey agar but do not ferment lactose appear colorless
Lactose Fermenters (Pink): Klebsiella spp Escherichia coli Citrobacter spp Serratia spp Non-Lactose Fermenters: Proteus spp. Shigella spp. Yersinia spp. Salmonella spp.
Blood agar
Grow most of fastidious organisms and to differentiate bacteria based on their hemolytic properties
Non selective (can be selective, but proper antibiotic should be added to it), enriched medium primarily used to grow fastidious microorganisms like Streptococci. Such organisms do not grow well using ordinary growth medium. Helps detect and differentiate haemolytic bacteria
Alpha hemolysis: Partial lysis of the RBC to produce a greenish-grey or brownish discoloration around the colony Beta hemolysis: Complete lysis of Red Blood Cells, causing a clearing of blood from the medium under and surrounding the colonies Gamma: no hemolysis of RBC.
12
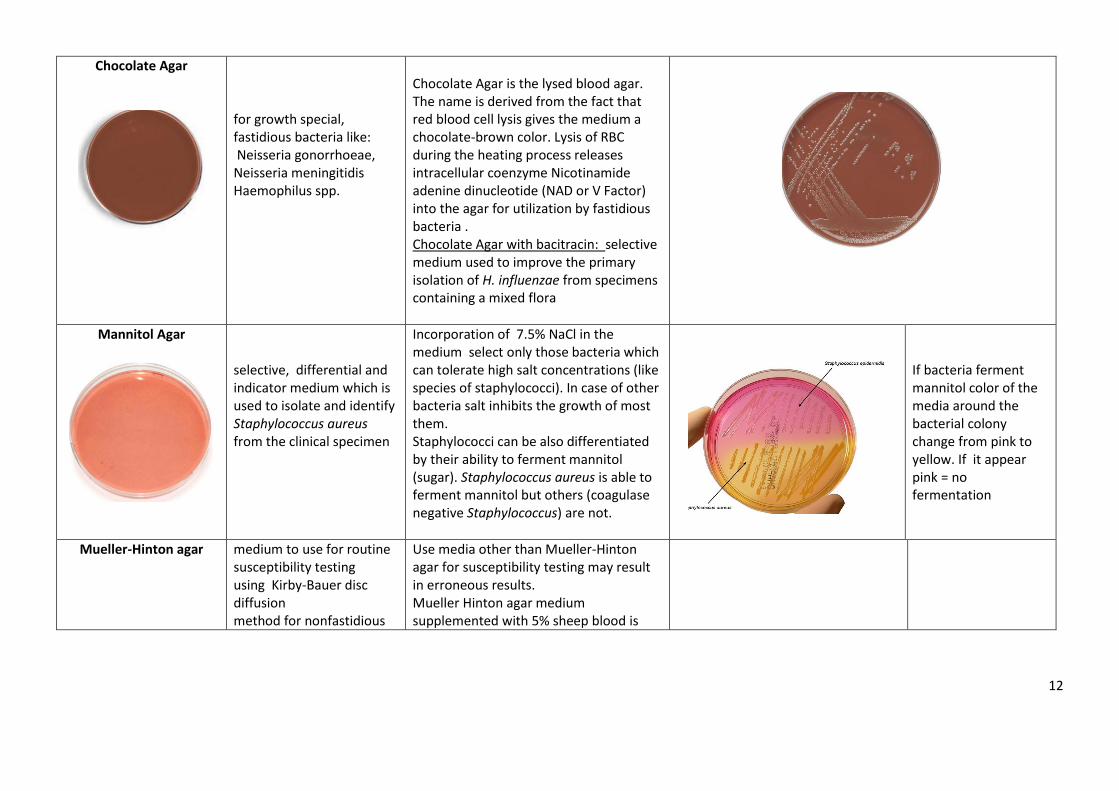
Chocolate Agar
for growth special, fastidious bacteria like: Neisseria gonorrhoeae, Neisseria meningitidis Haemophilus spp.
Chocolate Agar is the lysed blood agar. The name is derived from the fact that red blood cell lysis gives the medium a chocolate-brown color. Lysis of RBC during the heating process releases intracellular coenzyme Nicotinamide adenine dinucleotide (NAD or V Factor) into the agar for utilization by fastidious bacteria . Chocolate Agar with bacitracin: selective medium used to improve the primary isolation of H. influenzae from specimens containing a mixed flora
Mannitol Agar
selective, differential and indicator medium which is used to isolate and identify Staphylococcus aureus from the clinical specimen
Incorporation of 7.5% NaCl in the medium select only those bacteria which can tolerate high salt concentrations (like species of staphylococci). In case of other bacteria salt inhibits the growth of most them. Staphylococci can be also differentiated by their ability to ferment mannitol (sugar). Staphylococcus aureus is able to ferment mannitol but others (coagulase negative Staphylococcus) are not.
If bacteria ferment mannitol color of the media around the bacterial colony change from pink to yellow. If it appear pink = no fermentation
Mueller-Hinton agar
medium to use for routine susceptibility testing using Kirby-Bauer disc diffusion method for nonfastidious
Use media other than Mueller-Hinton agar for susceptibility testing may result in erroneous results. Mueller Hinton agar medium supplemented with 5% sheep blood is
13
bacteria recommended for determining the antimicrobial susceptibility of Str. Pneumonia or N. meningitidis
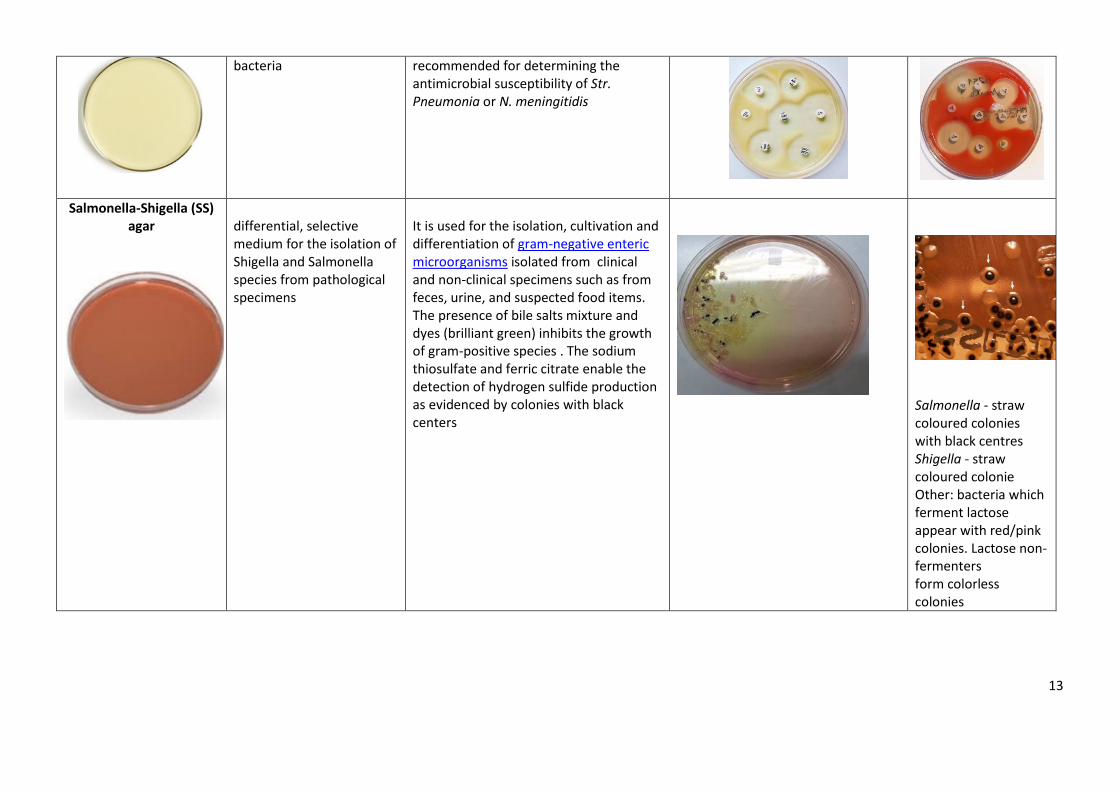
Salmonella-Shigella (SS) agar
differential, selective medium for the isolation of Shigella and Salmonella species from pathological specimens
It is used for the isolation, cultivation and differentiation of gram-negative enteric microorganisms isolated from clinical and non-clinical specimens such as from feces, urine, and suspected food items. The presence of bile salts mixture and dyes (brilliant green) inhibits the growth of gram-positive species . The sodium thiosulfate and ferric citrate enable the detection of hydrogen sulfide production as evidenced by colonies with black centers
Salmonella - straw coloured colonies with black centres Shigella - straw coloured colonie Other: bacteria which ferment lactose appear with red/pink colonies. Lactose non-fermenters form colorless colonies
14
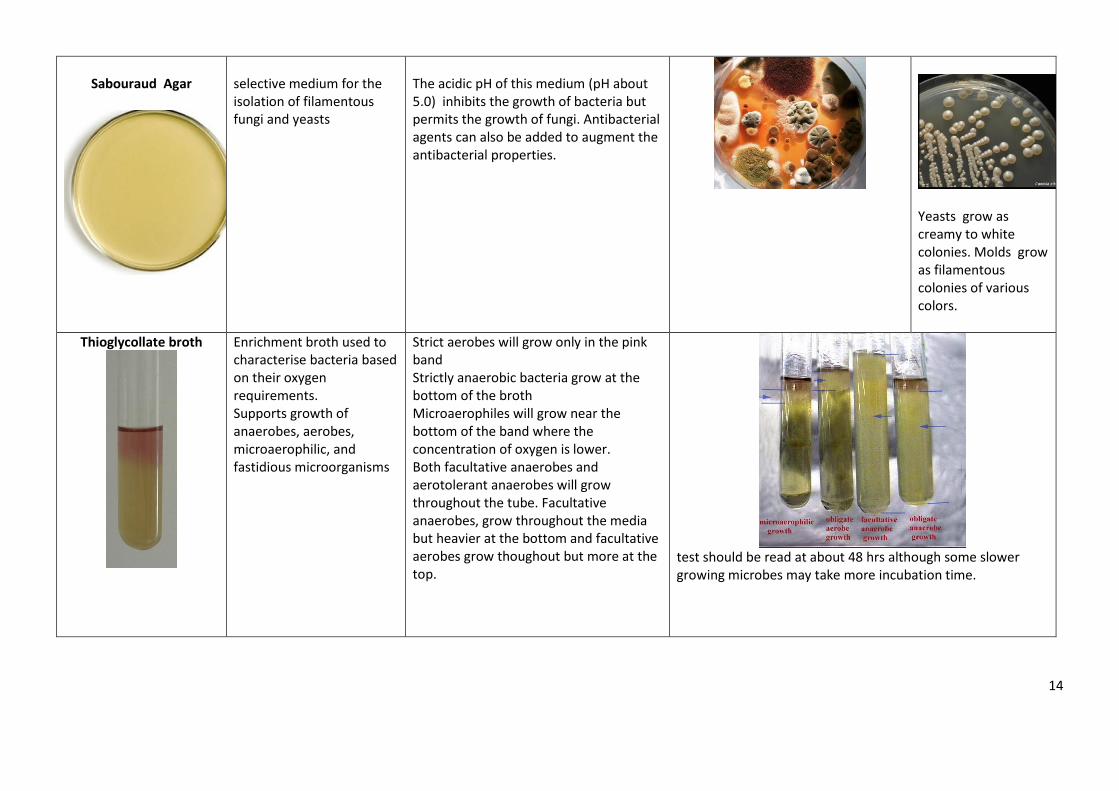
Sabouraud Agar
selective medium for the isolation of filamentous fungi and yeasts
The acidic pH of this medium (pH about 5.0) inhibits the growth of bacteria but permits the growth of fungi. Antibacterial agents can also be added to augment the antibacterial properties.
Yeasts grow as creamy to white colonies. Molds grow as filamentous colonies of various colors.
Thioglycollate broth
Enrichment broth used to characterise bacteria based on their oxygen requirements. Supports growth of anaerobes, aerobes, microaerophilic, and fastidious microorganisms
Strict aerobes will grow only in the pink band Strictly anaerobic bacteria grow at the bottom of the broth Microaerophiles will grow near the bottom of the band where the concentration of oxygen is lower. Both facultative anaerobes and aerotolerant anaerobes will grow throughout the tube. Facultative anaerobes, grow throughout the media but heavier at the bottom and facultative aerobes grow thoughout but more at the top.
test should be read at about 48 hrs although some slower growing microbes may take more incubation time.
15
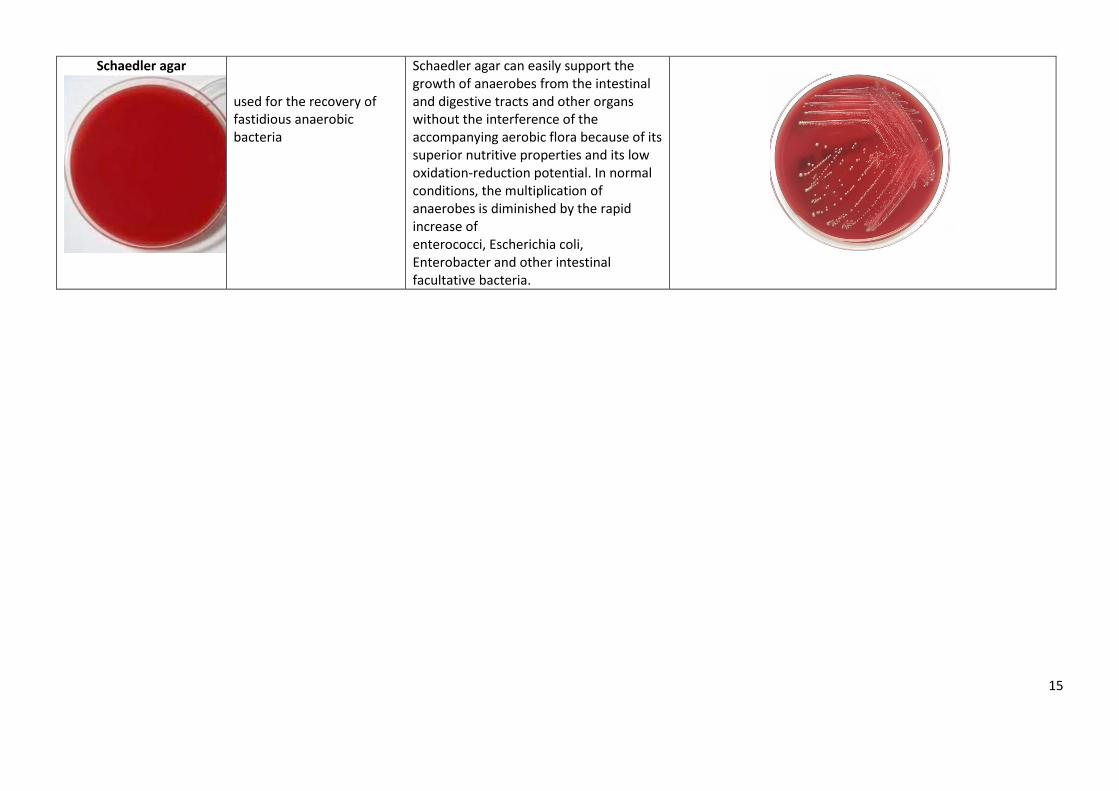
Schaedler agar
used for the recovery of fastidious anaerobic bacteria
Schaedler agar can easily support the growth of anaerobes from the intestinal and digestive tracts and other organs without the interference of the accompanying aerobic flora because of its superior nutritive properties and its low oxidation-reduction potential. In normal conditions, the multiplication of anaerobes is diminished by the rapid increase of enterococci, Escherichia coli, Enterobacter and other intestinal facultative bacteria.

16
SEROLOGIC ASSAYS USED IN MICROBIOLOGY
AGGLUTINATION & HEMAGGLUTINATION
AGGLUTINATION = clumping of cells or particles by specific antibodies (formation of complexes of
antigens and antibodies)
HEMAGGLUTINATION = clumping of red blood cells by specific antibodies; in general, all
serological reactions based on clumping of red blood cells are called hemagglutination
Both these reactions can detect antigens or antibodies depending on what we have (known antigen or known antibody) or what we are looking for:
a) When we look for unknown antigen then we have to use specific antibodies against the antigen
b) When we look for specific antibodies in the patient’s serum than we have to use known antigen
Both agglutination and hemagglutination reactions can be performed on a glass slide, test plate, a
microtiter plate or in tubes.
INDIRECT AGGLUTINATION/HEAMGGLUTINATION
Both, agglutination and hemagglutination reactions can be performed as passive/indirect
reactions when the antigen (particle) is so tiny that the reaction with the antibody will be
invisible. To improve visualization, we use a carrier particle – most commonly latex beads or red
blood cells (they are red so well visible!) and coat them with the antigen. What is important to
remember about, the carrier itself does not, however, participate in the reaction between
antibody and antigen. That is why these reactions are called passive to indicate that the antigen is
on the carrier particle that does not
participate (is passive) in the reaction.
Often, in indirect/passive hemagglutination
the process of antigen coating on red blood
cells is called sensitization to indicate that
red blood cells coated with the antigen are
sensitive to become clumped by specific
antibodies.
Similarly, using indirect reactions of agglutination or hemagglutination we can detect a patient’s
antibody or unknown antigen – everything depends on what we are looking for or what we have.
17
EXAMPLES
DETECTION OF UNKNOWN ANTIGEN USING KNOWN ANTIBODIES
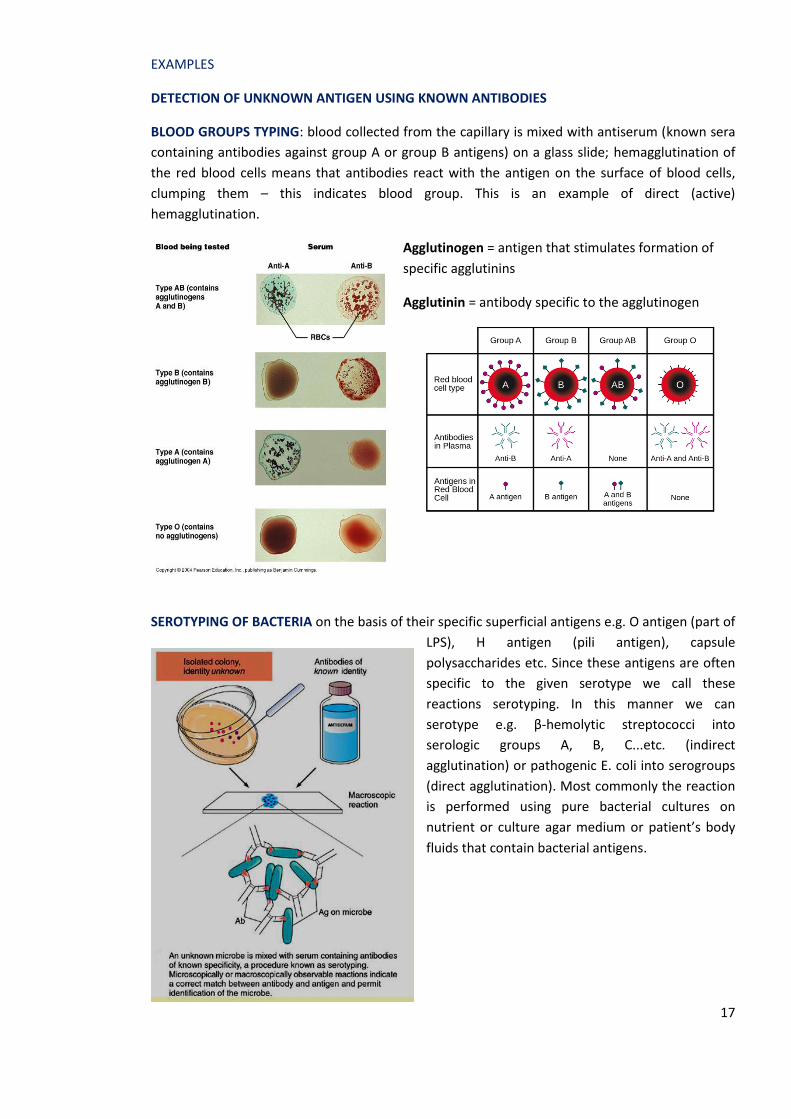
BLOOD GROUPS TYPING: blood collected from the capillary is mixed with antiserum (known sera
containing antibodies against group A or group B antigens) on a glass slide; hemagglutination of
the red blood cells means that antibodies react with the antigen on the surface of blood cells,
clumping them – this indicates blood group. This is an example of direct (active)
hemagglutination.
Agglutinogen = antigen that stimulates formation of
specific agglutinins
Agglutinin = antibody specific to the agglutinogen
SEROTYPING OF BACTERIA on the basis of their specific superficial antigens e.g. O antigen (part of
LPS), H antigen (pili antigen), capsule
polysaccharides etc. Since these antigens are often
specific to the given serotype we call these
reactions serotyping. In this manner we can
serotype e.g. β-hemolytic streptococci into
serologic groups A, B, C...etc. (indirect
agglutination) or pathogenic E. coli into serogroups
(direct agglutination). Most commonly the reaction
is performed using pure bacterial cultures on
nutrient or culture agar medium or patient’s body
fluids that contain bacterial antigens.

18
In the serotyping of β-hemolytic streptococci the carrier is a latex bead coated with antibodies
specific to C polysaccharide antigens on the surface of streptococci
β-hemolytic streptococcus culture on blood agar is taken with loop or plastic stick and mixed on a
test plate with a drop of colored latex particles coated with antibodies specific to groups A, B, C....
Agglutination of latex beads indicates a positive reaction.
Other examples include: Detection of live Leptospira in patient’s fluids e.g. urine sample. Detection of bacterial or fungal antigens (polysaccharides present in the cell wall of Str. pneumoniae, H. influenzae, N. meningitidis or Cryptococcus neoformans) present in patient’s CSF sample, allowing rapid diagnosis of CNS infections. Detection of different viruses in human body fluids, cultures.
DETECTION OF A PATIENT’S ANTIBODY USING KNOW ANTIGEN
WIDAL TEST detects the presence of serum antibodies (agglutinins H and O) in patients serum with typhoid and paratyphoid fever. The Widal test is the reliable and can be of value in the diagnosis of typhoid fevers in endemic areas.
Salmonella antibody starts appearing in serum at the end of first week and rise sharply during the 3rd week of fever. In acute typhoid fever, O agglutinins (antibodies clumping O antigen in the bacterial cell wall) can usually be detected 6–8 days after the onset of fever and H agglutinins
(antibodies that clump flagella on the surface of bacteria) after 10–12 days.
The test is performed in tubes as shown in the picture below.
It is preferable to test two specimens of sera at an interval of 7 to 10 days to demonstrate a rising antibody titer.

19
Patient’s serum is diluted in tubes and then suspensions of antigens O and H are added to each tube and incubated. The result is read on the basis of agglutination of antigens by specific antibodies present in the patient’s serum. The highest dilution of serum indicates the titer of antibodies. In acute enteric fever diagnostic titre of antibodies against O antigen is ≥1:100 whereas titre of antibodies against flagella antigen is ≥ 1:200.
Demonstration of rising titre of four-fold or greater of H and O agglutinins at an interval of 4 to 7 days is the most important diagnostic criterion.
INDIRECT (PASSIVE) HEMAGGLUTINATION
IMPORTANT! Some viruses also bind to red blood cells, and this binding can cause agglutination when the viruses cross-link the red blood cells. For example, influenza viruses have two different types of viral spikes called neuraminidase (N) and hemagglutinin (H), the latter named for its ability to agglutinate red blood cells. Thus, we can use red blood cells to detect the presence of influenza virus by direct hemagglutination assays, in which the virus causes visible agglutination of red blood cells. The mumps and rubella viruses can also be detected using that assay.
Passive hemagglutination assay in the diagnosis of syphilis TPHA has been used as a confirmatory test for the diagnosis of Treponema pallidum infection – this test detects anti-treponemal antibodies (IgG and IgM antibodies) in serum or CSF. TPHA is a good primary screening test for syphilis at all stages beyond the early primary stage – our immune system needs some time to produce specific antibodies. TPHA test is a passive (indirect) hemagglutination assay based on hemagglutination of erythrocytes sensitized with T. pallidum antigen by antibodies found in the patient’s serum or plasma. It is used for both qualitative and semi-quantative detection of anti-treponemal antibodies. The test sample is diluted in absorbing diluent to remove possible cross-reacting heterophile antibody and to remove, block, or absorb potentially cross-reacting, nonpathogenic
treponemal antibodies. Sera containing antibodies to T. pallidum react with erythrocytes (chicken or avian) sensitized with sonicated T. pallidum, Nichols strain (the antigen), to form a smooth mat of agglutinated cells in the microtiter tray well. If antibodies are not present the cells settle to the bottom of the tray well, forming a compact button of unagglutinated cells.

20
Passive hemagglutination assay can be used to determine the titer of antiviral antibodies in patient’s serum. The presence of these antibodies in a patient’s serum will neutralize the virus and block it from agglutinating the red cells, making this a viral hemagglutination inhibition assay (HIA). In this assay, patient serum is mixed with a standardized amount of virus. After a short incubation, a standardized amount of red blood cells is added and hemagglutination is observed. The titer of the patient’s serum is the highest dilution that blocks agglutination.
Other examples include: Detection of antibodies against Leptospira in patient’s serum using alive cultures of leptospiras Detection of specific antibodies against many different bacteria, viruses, fungi in patient’s serum or other body fluids – antigens of many pathogens can be coated on latex beads.
IMMUNOFLUORESCENCE
In a very similar way, the immunofluorescence reaction uses antigens and antibodies against these antigens. However, in immunofluorescence antibodies are conjugated with fluorochorme dyes that absorb ultraviolet light of a defined wavelength, but emits light at a higher wavelength. The emitted light is detected optically with a special microscope equipped with filters specific for the emission wavelength of the fluorochrome – fluorescent microscope.
The fluorochrome can be bound directly to the antigen-specific antibody (direct immunofluorescence) or it can be attached to an anti-immunoglobulin molecule (antibody against antibody) that recognizes the antigen-specific antibody (indirect immunofluorescence).
FTA-ABS Test to diagnose syphilis
Serum from patients suspected of having syphilis because of previous positive VDRL or RPR (description – see below) test is diluted in 1:5 sorbent (patients’ serum is absorbed with treponemes other than Treponema pallidum to remove nonspecific antibodies). In this fluorescence treponemal antibody absorption test the antigen consists of killed Nichols strain. This absorbed serum is layered on a microscope slide which contains fixed T. pallidum subspecies pallidum. If the patient’s serum contains antibody, the antibody will coat the treponeme.
Next, fluorescein isothiocyanate (FITC)-labeled anti-human immunoglobulin is added; this combines with the patient’s IgG and IgM antibodies that are adhering to T. pallidum, and results in a visible test reaction when examined by fluorescence microscopy. FTA-ABS test should not be used as a primary screening procedure. Sensitivity of Fluorescent Treponemal Antibody Test
1. Primary Syphilis: 85% 2. Secondary Syphilis: 100%
21
3. Late Syphilis: 98% Specimen: serum is the most appropriate specimen for the FTA-ABS test; however, spinal fluid may be used.
PRECIPITATION
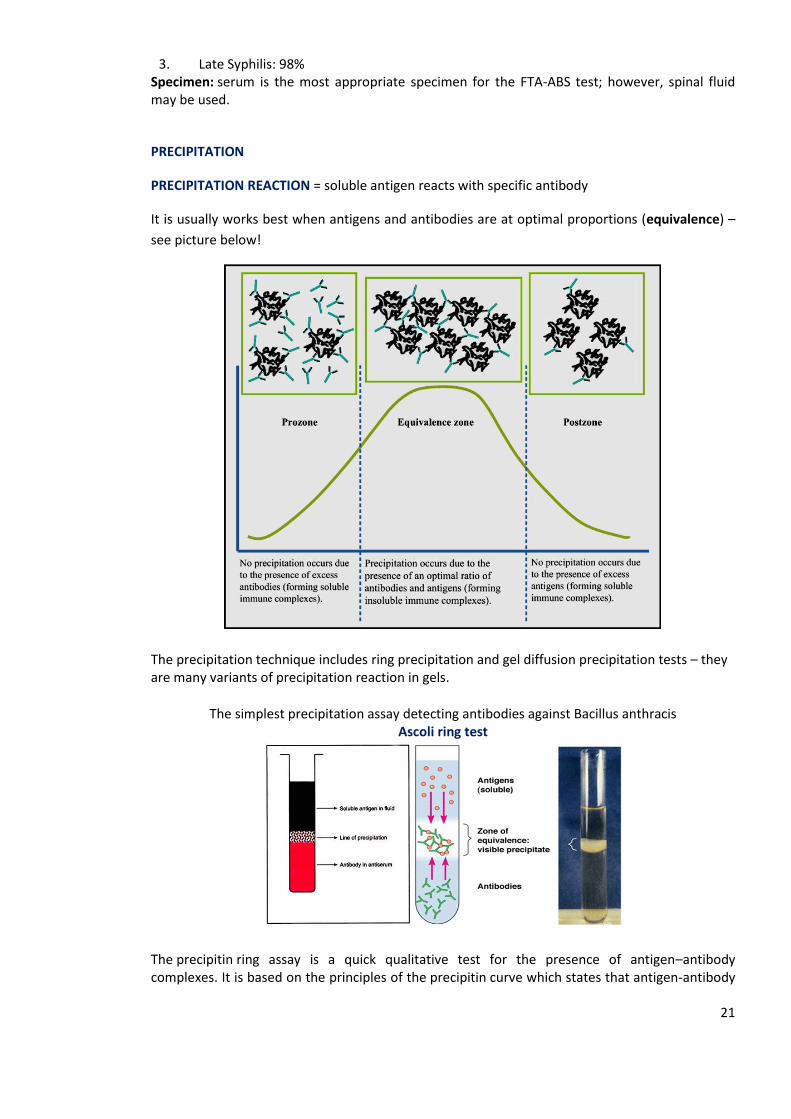
PRECIPITATION REACTION = soluble antigen reacts with specific antibody
It is usually works best when antigens and antibodies are at optimal proportions (equivalence) –
see picture below!
The precipitation technique includes ring precipitation and gel diffusion precipitation tests – they are many variants of precipitation reaction in gels.
The simplest precipitation assay detecting antibodies against Bacillus anthracis Ascoli ring test
The precipitin ring assay is a quick qualitative test for the presence of antigen–antibody complexes. It is based on the principles of the precipitin curve which states that antigen-antibody
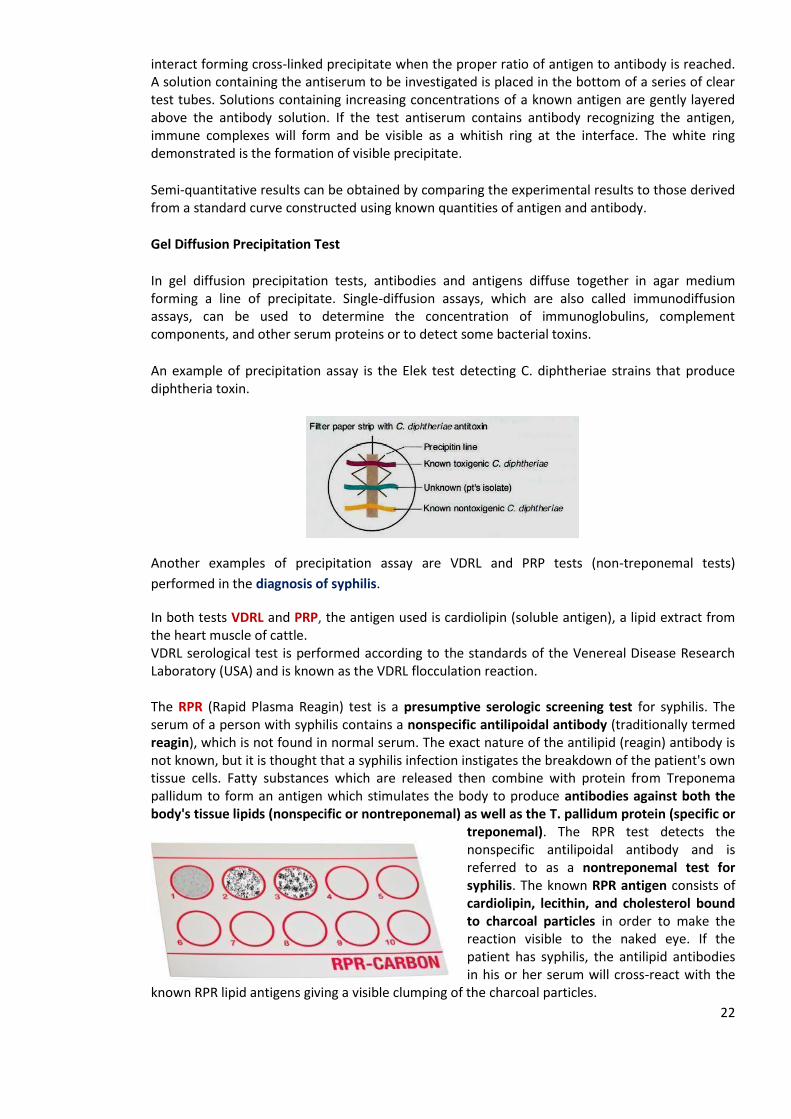
22
interact forming cross-linked precipitate when the proper ratio of antigen to antibody is reached. A solution containing the antiserum to be investigated is placed in the bottom of a series of clear test tubes. Solutions containing increasing concentrations of a known antigen are gently layered above the antibody solution. If the test antiserum contains antibody recognizing the antigen, immune complexes will form and be visible as a whitish ring at the interface. The white ring demonstrated is the formation of visible precipitate.
Semi-quantitative results can be obtained by comparing the experimental results to those derived from a standard curve constructed using known quantities of antigen and antibody.
Gel Diffusion Precipitation Test
In gel diffusion precipitation tests, antibodies and antigens diffuse together in agar medium forming a line of precipitate. Single-diffusion assays, which are also called immunodiffusion assays, can be used to determine the concentration of immunoglobulins, complement components, and other serum proteins or to detect some bacterial toxins.
An example of precipitation assay is the Elek test detecting C. diphtheriae strains that produce diphtheria toxin.
Another examples of precipitation assay are VDRL and PRP tests (non-treponemal tests)
performed in the diagnosis of syphilis.
In both tests VDRL and PRP, the antigen used is cardiolipin (soluble antigen), a lipid extract from the heart muscle of cattle. VDRL serological test is performed according to the standards of the Venereal Disease Research Laboratory (USA) and is known as the VDRL flocculation reaction. The RPR (Rapid Plasma Reagin) test is a presumptive serologic screening test for syphilis. The serum of a person with syphilis contains a nonspecific antilipoidal antibody (traditionally termed reagin), which is not found in normal serum. The exact nature of the antilipid (reagin) antibody is not known, but it is thought that a syphilis infection instigates the breakdown of the patient's own tissue cells. Fatty substances which are released then combine with protein from Treponema pallidum to form an antigen which stimulates the body to produce antibodies against both the body's tissue lipids (nonspecific or nontreponemal) as well as the T. pallidum protein (specific or
treponemal). The RPR test detects the nonspecific antilipoidal antibody and is referred to as a nontreponemal test for syphilis. The known RPR antigen consists of cardiolipin, lecithin, and cholesterol bound to charcoal particles in order to make the reaction visible to the naked eye. If the patient has syphilis, the antilipid antibodies in his or her serum will cross-react with the
known RPR lipid antigens giving a visible clumping of the charcoal particles.
23
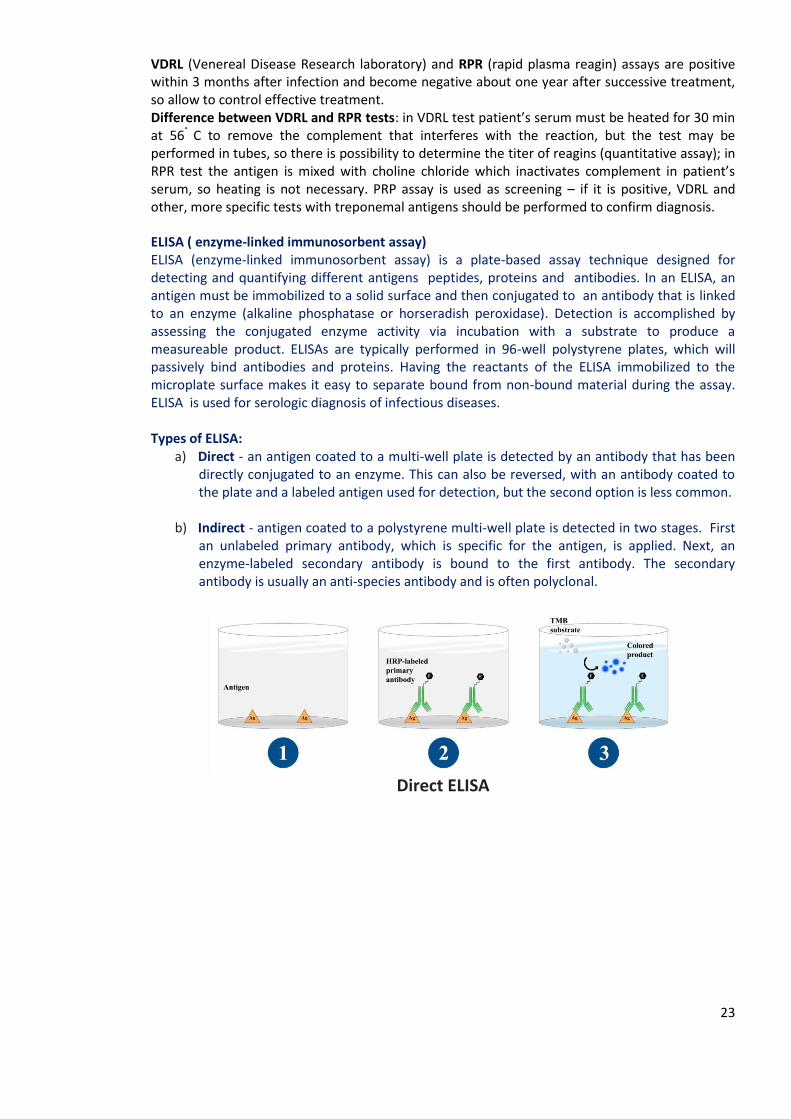
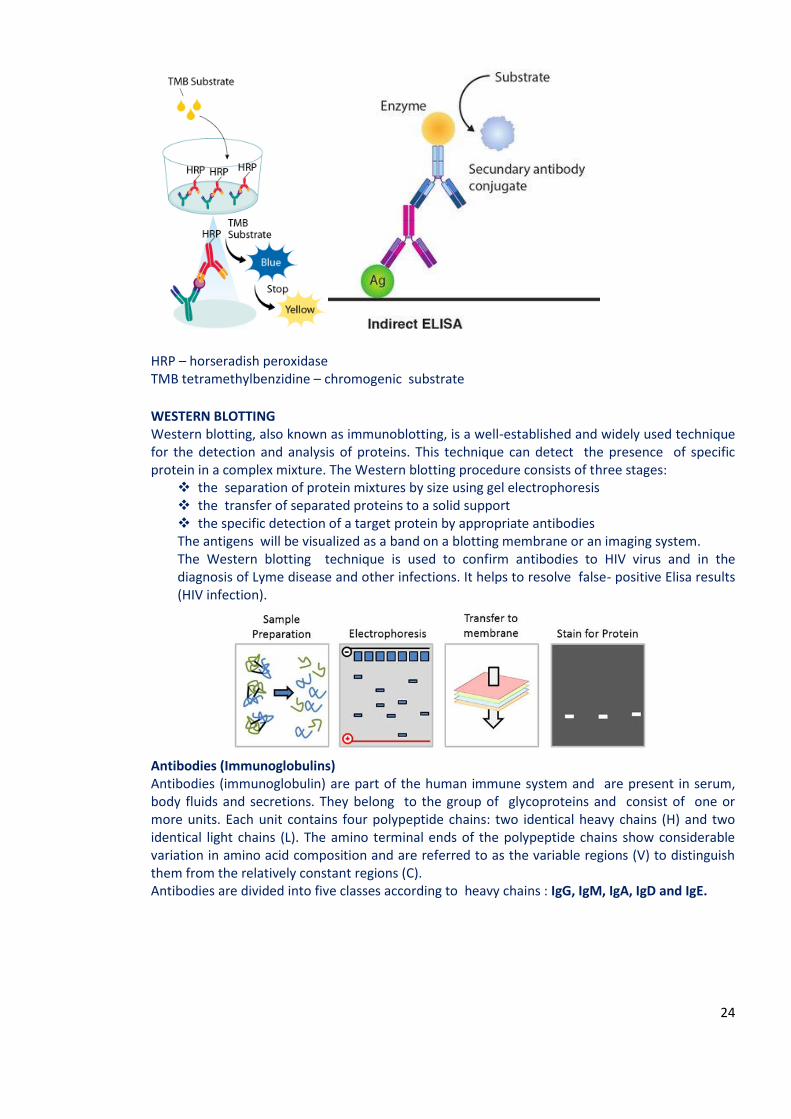
VDRL (Venereal Disease Research laboratory) and RPR (rapid plasma reagin) assays are positive within 3 months after infection and become negative about one year after successive treatment, so allow to control effective treatment. Difference between VDRL and RPR tests: in VDRL test patient’s serum must be heated for 30 min at 56° C to remove the complement that interferes with the reaction, but the test may be performed in tubes, so there is possibility to determine the titer of reagins (quantitative assay); in RPR test the antigen is mixed with choline chloride which inactivates complement in patient’s serum, so heating is not necessary. PRP assay is used as screening – if it is positive, VDRL and other, more specific tests with treponemal antigens should be performed to confirm diagnosis. ELISA ( enzyme-linked immunosorbent assay) ELISA (enzyme-linked immunosorbent assay) is a plate-based assay technique designed for detecting and quantifying different antigens peptides, proteins and antibodies. In an ELISA, an antigen must be immobilized to a solid surface and then conjugated to an antibody that is linked to an enzyme (alkaline phosphatase or horseradish peroxidase). Detection is accomplished by assessing the conjugated enzyme activity via incubation with a substrate to produce a measureable product. ELISAs are typically performed in 96-well polystyrene plates, which will passively bind antibodies and proteins. Having the reactants of the ELISA immobilized to the microplate surface makes it easy to separate bound from non-bound material during the assay. ELISA is used for serologic diagnosis of infectious diseases. Types of ELISA:
a) Direct - an antigen coated to a multi-well plate is detected by an antibody that has been directly conjugated to an enzyme. This can also be reversed, with an antibody coated to the plate and a labeled antigen used for detection, but the second option is less common.
b) Indirect - antigen coated to a polystyrene multi-well plate is detected in two stages. First an unlabeled primary antibody, which is specific for the antigen, is applied. Next, an enzyme-labeled secondary antibody is bound to the first antibody. The secondary antibody is usually an anti-species antibody and is often polyclonal.
Direct ELISA
24
HRP – horseradish peroxidase TMB tetramethylbenzidine – chromogenic substrate
WESTERN BLOTTING Western blotting, also known as immunoblotting, is a well-established and widely used technique for the detection and analysis of proteins. This technique can detect the presence of specific protein in a complex mixture. The Western blotting procedure consists of three stages:
the separation of protein mixtures by size using gel electrophoresis the transfer of separated proteins to a solid support the specific detection of a target protein by appropriate antibodies The antigens will be visualized as a band on a blotting membrane or an imaging system. The Western blotting technique is used to confirm antibodies to HIV virus and in the diagnosis of Lyme disease and other infections. It helps to resolve false- positive Elisa results (HIV infection).
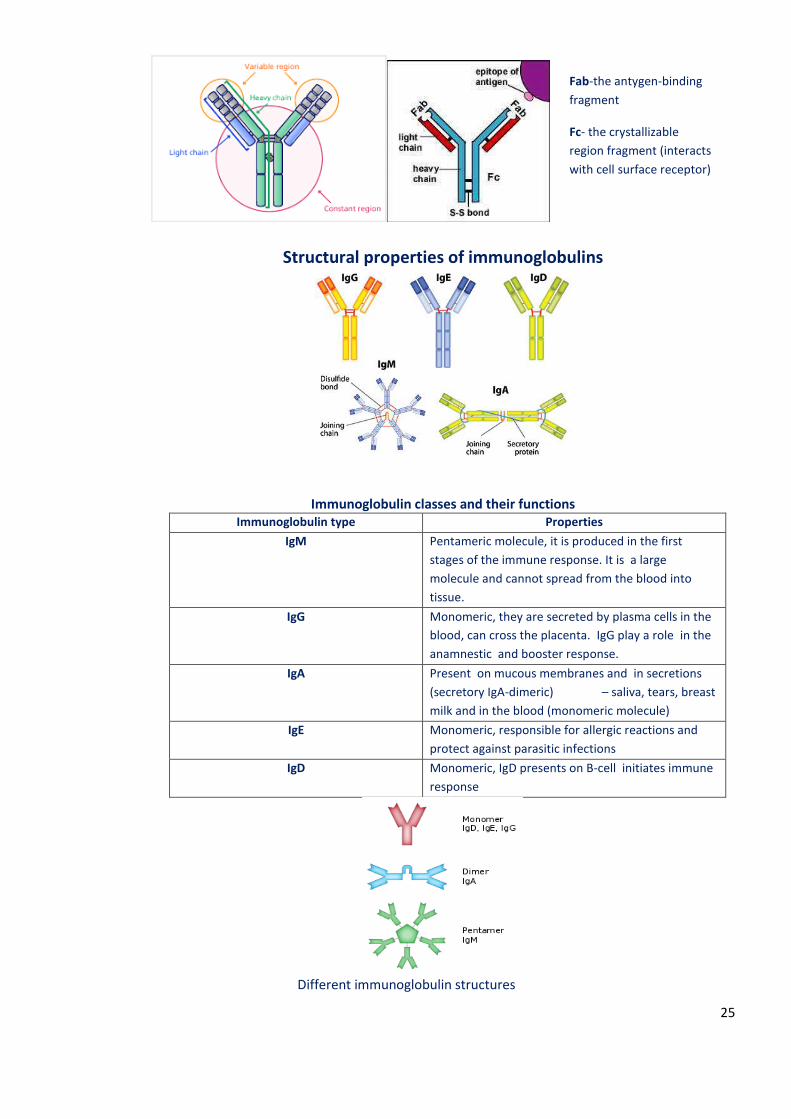
Antibodies (Immunoglobulins) Antibodies (immunoglobulin) are part of the human immune system and are present in serum, body fluids and secretions. They belong to the group of glycoproteins and consist of one or more units. Each unit contains four polypeptide chains: two identical heavy chains (H) and two identical light chains (L). The amino terminal ends of the polypeptide chains show considerable variation in amino acid composition and are referred to as the variable regions (V) to distinguish them from the relatively constant regions (C). Antibodies are divided into five classes according to heavy chains : IgG, IgM, IgA, IgD and IgE.
25
Structural properties of immunoglobulins
Immunoglobulin classes and their functions Immunoglobulin type Properties
IgM
Pentameric molecule, it is produced in the first
stages of the immune response. It is a large
molecule and cannot spread from the blood into
tissue.
IgG Monomeric, they are secreted by plasma cells in the
blood, can cross the placenta. IgG play a role in the
anamnestic and booster response.
IgA Present on mucous membranes and in secretions
(secretory IgA-dimeric) – saliva, tears, breast
milk and in the blood (monomeric molecule)
IgE Monomeric, responsible for allergic reactions and
protect against parasitic infections
IgD Monomeric, IgD presents on B-cell initiates immune
response
Different immunoglobulin structures
Fab-the antygen-binding
fragment
Fc- the crystallizable
region fragment (interacts
with cell surface receptor)