colorectal cancer: what next? neal j. meropol, md chief, hematology and oncology university...
TRANSCRIPT

Colorectal Cancer: What Next?
Neal J. Meropol, MDChief, Hematology and Oncology
University Hospitals Case Medical CenterCase Western Reserve University
January 18, 2014

For our consideration:• Analysis of KRAS/NRAS mutations in the phase 3 20050181
study of panitumumab + FOLFIRI vs FOLFIRI as second-line treatment for metastatic colorectal cancer (Peeters et al)
• Mutations within the EGFR signaling pathway: influence on efficacy in FIRE-3 (Stintzing et al)
• Regular aspirin use improves survival in patients with PIK3CA mutated metastatic colorectal cancer (Kothari et al)
• Maintenance treatment with capecitabine + bevacizumab versus observation after induction treatment with chemotherapy + bevacizumab in metastatic colorectal cancer (Koopman et al)
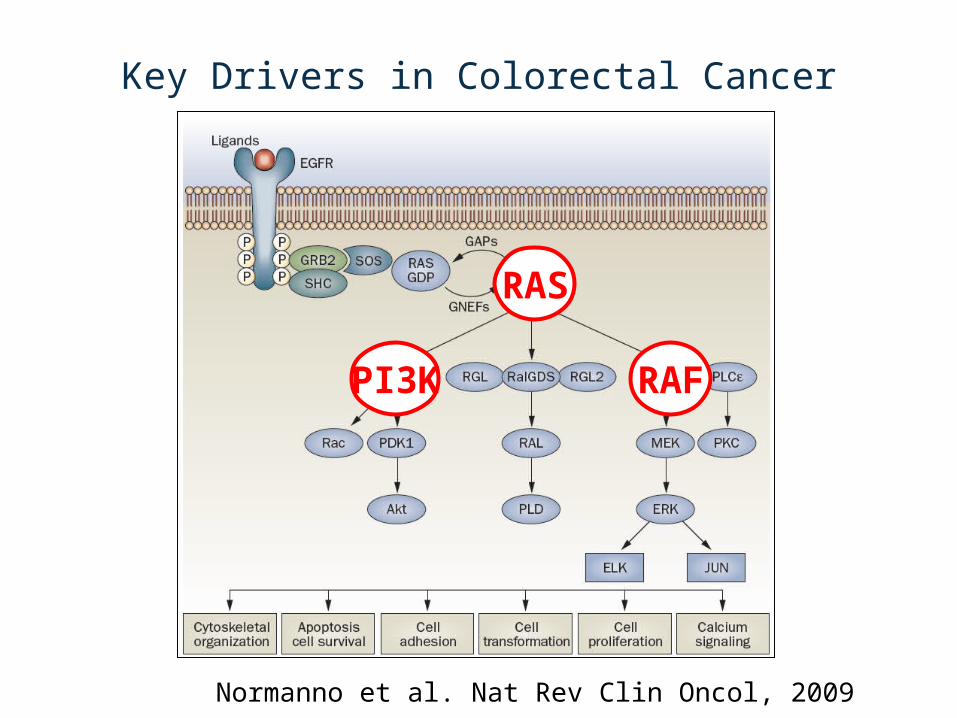
Key Drivers in Colorectal Cancer
Normanno et al. Nat Rev Clin Oncol, 2009
RAS
RAFPI3K

RAS Review• Belongs to a superfamily of
GTPases• Commonly mutated in
human cancer, constitutive activation
• 3 members of the subfamily: N, K, and H-ras
• Different expression patterns and localization in different tumors
• Functional differences not fully delineated Castellano and Santos. Genes and Cancer, 2011

RAS, RAF and PIK3CA Mutations in Colorectal Cancer
• Mutation frequency– KRAS: 40%– NRAS: 3%– BRAF: 5%– PIK3CA: 15%
• BRAF and KRAS/NRAS mutations are mutually exclusive
• KRAS and NRAS mutations are mutually exclusive
De Roock, Lancet Oncol, 2010

EGFR Antibodies in Colorectal Cancer
• 2004 - Regulatory approval initially required EGFR expression by IHC
• 2009 - ASCO Provisional Clinical Opinion: do not administer anti-EGFR antibodies to patients with tumors that harbor codon 12/13 KRAS mutations (Allegra et al. JCO, 2009)

Next Question: What about RAS family mutations other than exon 2 in KRAS?
DatasetsPRIME: FOLFOX +/-panitumumab
(Doulliard, NEJM 2013)First-line
FIRE-3: FOLFIRI + cetuximab or bevacizumab (Stintzing, GI Symp 2014)
First-line
20050181: FOLFIRI +/- panitumumab (Peeters, GI Symp 2014 2014)
Second-line

Reminder – A prospective randomized clinical trial is the gold standard. A
prospective-retrospective study may be adequate if:
• a priori hypothesis and statistical design• biomarker assay validated• samples available from vast majority of
patients• adequate follow up and annotation

PRIME Study: FOLFOX +/- PmabFirst-Line
Douillard J et al. N Engl J Med 2013;369:1023-1034.
PFS
OS
Exon 2 WT-Other Mut
Exon 2 WT-Other Mut

20050181: FOLFIRI +/- PmabSecond-Line
Peeters et al. GI Symp 2014• PFS benefit of Pmab restricted to RAS WT population• RR benefit of Pmab restricted to RAS WT population

FIRE-3 Study: FOLFIRI + cetuximab or bevacizumab first-line
• Favor bevacizumab– Improved PFS and response rate (trend) RAS
mutant– Trend toward improved PFS (but not OS) with
PIK3CA mutant
• Favor cetuximab– Improved OS (but not PFS) with RAS wt (7.5 month
improvement)

What have we learned?
• RAS mutations beyond exon 2 are common (15-18%)• Patients with any RAS mutations do not appear to benefit (at
least no major benefit) from anti-EGFR treatment• Among patients with no RAS mutations, a clinically
meaningful survival benefit is observed with cetux vs bevacizumab (but no difference in PFS)– Results of Alliance 80405 are eagerly awaited!
• Currently, incomplete data regarding potential biologic differences when combining EGFR inhibitors with different chemotherapy backbones, and between different RAS mutations
• A pooled analysis of ALL available studies is encouraged!
Aspirin and PIK3CA

PIK3CA, Prostaglandins, and Colon CancerPIK3CA activating mutations are present in 15-20% of colorectal cancers
Complex interactions exist between PI3K , other signaling pathways, and prostaglandin synthesis which contribute to development and growth of colorectal cancer
Does PIK3CA mutational status influence the response to aspirin?
Markowitz SD. N Engl J Med 2007

Fuchs C S , and Ogino S JCO 2013;31:4358-4361
Aspirin’s affects extend well beyond tumor intracellular signalling

964 Participants in the Nurses’ Health Study and the Health Professionals Follow-up Study with Colorectal
Cancer
Superior colorectal cancer-specific survival (HR=0.18, p<0.001) and overall survival (HR=0.54 , P=0.01) with regular aspirin use in PIK3CA mutants
Liao X, et al. N Engl J Med. 2012;367: 1596-606.

Domingo E et al. JCO 2013;31:4297-4305
No greater benefit of rofecoxib based on PIK3CA mutation status
Regular aspirin use (14%) associated with reduced rate of recurrence in patients with PIK3CA-mutantcancers (HR, 0.11; P .027; but not in patientslacking tumor PIK3CA mutation (HR, 0.92; P .71).
RFS
OS
VICTOR Trial: Adjuvant Study of Rofecoxib vs. Placebo (N=896; 12% PIK3CA mutant)
WT Mutant

Aspirin in PIK3CA Colorectal Cancer(Kothari et al. GI Symp 2014)
• Convenience sample of 185 patients• 49 reported aspirin use• Stage distribution: 1/2/3/4 8/66/67/44• No clear overall survival benefit among ASA
users; trend towards benefit in stage 4

Do the “negative” data provided by Kothari et al refute the underlying hypothesis? NO.
Challenges with current datasets• No randomization between ASA and no ASA• Reliance on patient reporting of ASA use• Variation in dosing among ASA users• Mix of stages included• Small sample sizes of PIK3CA mutants• Potential unmeasured variables that could impact
ASA – PIK3CA relationship, including other treatments received
Prospective evaluation of ASA and COX-2 inhibition in PIK3CA mutant CRC
is needed
Ongoing/Planned randomized trials of ASA and celecoxib in the adjuvant
setting will provide meaningful data

Is maintenance therapy superior to “treatment holiday” after induction? CAIRO3 (Koopman et al)
• N=558, <20% prior adjuvant treatment; ~60% had resection of primary tumor
• Only 60% of patients in obs arm restarted CAPOX-B; most received some treatment
• PFS favors maintenance (HR=.67, p <.0001 ; PFS2 8.5 vs. 11. 7 mo) BUT no clear difference in overall survival (multivariate analysis suggests benefit of M)
• Patients who achieve initial response or have primary tumor removed (in case of synchronous metastasis) may have improved survival with maintenance

What have we learned from CAIRO3?
• It is feasible yet challenging to conduct a “window of opportunity” study after induction (<2 patients per center per year)
• Maintenance treatment clearly will delay progression
• More work is needed to identify those patients who may safely receive a “treatment holiday”

Colorectal Cancer S-CurvePa
tient
Sur
viva
l
Era
Tweaking 5-FU
New Cytotoxics and Antibodies
More Tweaking
1980s 1990s 2000s
We must jump to the next curvePa
tient
Sur
viva
l
Era

How to get there
GenomicsBig data
Public-PrivateBiobanking
Acknowledge that all cancers will be rare diseases
-New clinical trials models-New infrastructure and regulatory models
Technology
Teamwork
Trials
