combined hemodynamic effects dopamine...
TRANSCRIPT

Combined Hemodynamic Effects of Dopamineand Dobutamine in Cardiogenic Shock
C. RICHARD, M.D., J. L. RICOME, M.D., A. RIMAILHO, M.D.,G. BOTTINEAU, M.D. , AND P. AUZEPY, M.D.
SUMMARY In eight mechanically ventilated patients in cardiogenic shock, we assessed the hemodynamiceffects of an infusion ofdopamine and dobutamine and evaluated its role in preventing the deleterious effectsof administering each amine alone. Each patient received three infusions in a randomly assigned order:dopamine, 15 ,.tg/kg/min; dobutamine, 15 ,tg/kg/min; and a combination of dopamine, 7.S ,g/kg/min, anddobutamine, 7.5 ,ug/kg/min. Stroke volume index increased similarly with the three infusions, but dopaminealone increased oxygen consumption (p < 0.05 vs dobutamine alone and dopamine-dobutamine combined).The dopamine-dobutamine combination increased mean arterial pressure (p < 0.05 vs dobutamine),maintained pulmonary capillary wedge pressure within normal limits (p < 0.05 vs dopamine), andprevented the worsening of hypoxemia induced by dopamine (p < 0.05). The dopamine-dobutaminecombination appears to be useful in the management of mechanically ventilated patients in cardiogenicshock.
THE HEMODYNAMIC PICTURE of heart failure ischaracterized by a decrease in stroke volume and anincrease in ventricular filling pressures. When acutepump failure is so severe that an adequate cardiacoutput cannot be maintained, hypotension supervenesdespite the elevated peripheral resistance, and cardio-genic shock ensues. In this setting, diuretics and vaso-dilators cannot be used alone, and the therapeutic useof sympathomimetic amines such as dopamine anddobutamine is required.
Dopamine, a precursor in the endogenous synthesisof norepinephrine, is a potent inotropic agent.I-1 Itincreases stroke volume both by a direct action andthrough the release of norepinephrine stores.4 Whendopamine is used at a dose of 10-15ig/kg/min, va-sopressor effects appear. These effects are of particularvalue in patients with hypotension.5 However, an im-portant side effect limits its use in cardiogenic shock:At a dose of 10 to 15 ,ug/kg/min, it may induce anincrease in pulmonary capillary wedge pressure(PCWP). As a result, its use may be associated withpulmonary vascular congestion, arterial desaturationand increase in venous admixture.6
Dobutamine is also a potent inotropic agent that actsdirectly on adrenergic myocardial receptors withoutany release of norepinephrine from nerve endings.' Inthe treatment of severe heart failure, dobutamine in-duces an increase in cardiac output and stroke volumewith a reduction of PCWP.6 In contrast to dopamine,dobutamine probably has minimal direct vascular ac-tivity even when it is used at higher dosages. However,a reduction in systemic arterial resistance (SAR), fre-quently accompanied by a slight fall in mean arterialpressure (MAP), generally occurs during dobutamineinfusion in patients with chronic, low-output cardiacfailure.8 This decrease in SAR may be due to a reduc-
From the Service de Reanimation Medicale, Hopital de Bicetre, LeKremlin Bicetre, France.
Address for correspondence: C. Richard, M.D., Service de Reanima-tion Medicale, Hopital de Bicetre, 78, rue du General Leclerc, 94270 LeKremlin Bicetre, France.
Received April 30, 1982; revision accepted September 20, 1982.Circulation 67, No. 3, 1983.
tion in compensatory vasoconstriction secondary to animprovement in stroke volume index (SVI).The aim of this study was to assess the efficacy of a
combined dopamine-dobutamine infusion, 7.5 Ag/kglmin each, in the treatment of cardiogenic shock and inthe prevention of the deleterious effects of each sym-pathomimetic amine used alone.
MethodsWe studied eight patients in cardiogenic shock who
required continuous mechanical ventilation. Mechani-cal ventilation was instituted when drug treatment ofpulmonary edema with hypotension by diuretics, digi-talis glycosides or vasodilators was insufficient orineffective.The group consisted of five men and three women,
ages 60-75 years (mean 65 years). Before the onset ofcardiogenic shock, patients were in congestive heartfailure (New York Heart Association class III or IV)controlled by conventional treatment with digitalis,diuretics and vasodilators. The cause of heart failurewas coronary artery disease in four patients and idio-pathic cardiomyopathy in four. The etiology of ische-mic heart disease did not affect the clinical findings.Three patients were in chronic atrial fibrillation. Nopatient had suffered acute myocardial infarction withinthe 7 preceding days.Hemodynamic studies were performed on the sec-
ond day of assisted ventilation. A constant tidal vol-ume (15 ml/kg) with a I/E of /2 was delivered with avolume-controlled ventilator (Siemens servo ventilator900 B). Positive end-expiratory pressure (PEEP) wasnever used.Two days before the study, arterial and thermistor-
tipped Swan Ganz catheters were inserted. Cardiacoutput was measured in triplicate by the thermodilu-tion method (Edwards model 9510) after injecting 10ml of isotonic glucose at 0°C into the right atrium.Right atrial pressure (RAP), mean pulmonary arterialpressure (MPAP), PCWP and MAP were monitoredusing Bentley-Trantec transducers connected to the ar-terial and Swan Ganz catheters. Cardiac index (CI),stroke index (SI), left ventricular stroke work index(LVSWI) and SAR were calculated from standard for-
620
by guest on May 14, 2018
http://circ.ahajournals.org/D
ownloaded from
HEMODYNAMICS OF DOPAMINE AND DOBUTAMINE/Richard et al.
mulas. Blood gas tensions in arterial (Pao2 and Paco2)and mixed venous blood (Pvo2 and Pvco2) were deter-mined by standard electrode technique (ABL 1 Radi-ometer) and corrected for the patient's temperature.An OSM2 radiometer was used to measure hemoglobinand hemoglobin oxygen saturation (SaO2 and SvO2).From these measurements, arterial and mixed venousoxygen contents (CaO2 and CvO2), arteriovenous oxy-gen content difference (avDO2), venous admixture(Qva/Qt) with a respiratory quotient of 0.8 and oxygenconsumption (VO2) were calculated by standardformulas.
Each patient received three infusions in a randomlyassigned order: dopamine, 15 ,g/kg/min; dobutamine,15 ,ug/kg/min; and dopamine, 7.5 ,ug/kg/min, with
404 P A
/fIJi:t14
W90
80-
10-
60-
50-
40-
90-
80-
/0-
60-
50-
40-
io
10
f'CWf'
30-
25-
20-
15-
10-
5
c I
\v -0,<
.)--~
30-
25-
20-
15-
10-
5-
C I
30-
25-
20
15-
10-
5-
--0U
tfg
0 .- - 0
S,,40-
35-
30-
25-
20-
15-
c f
40-
35-
30-
25-
20-
15
c I
40-
I
35
30
25-
20-
151-4- I-sC
dobutamine, 7.5 ,g/kg/min. All other treatments,such as digitalis glycosides, diuretics and vasodilators,were stopped during the 6-8 hours of the study. Be-tween each infusion, a 1-hour interval was allowed forvariables to return to baseline levels. Patients wereventilated (FiO2 = 1) at all times of measurement.PCWP was always measured during the tele-expira-
tory phase. All measurements were performed 30 min-utes after the onset of each infusion. Patients weresedated with diazepam and anesthetized, if necessary,with pancuronium bromide during the study. Body tem-perature did not change significantly during the study.
ResultsThe measurements during the control and drug infu-
UREbmnn
145-
1301
115-
100
85
70
c I
145-
130-
115-
100-
85-
70-
*Cc
I
145-
130-
115-
100-
85-
70-A
0 I
CI
c I
c I
U
C i
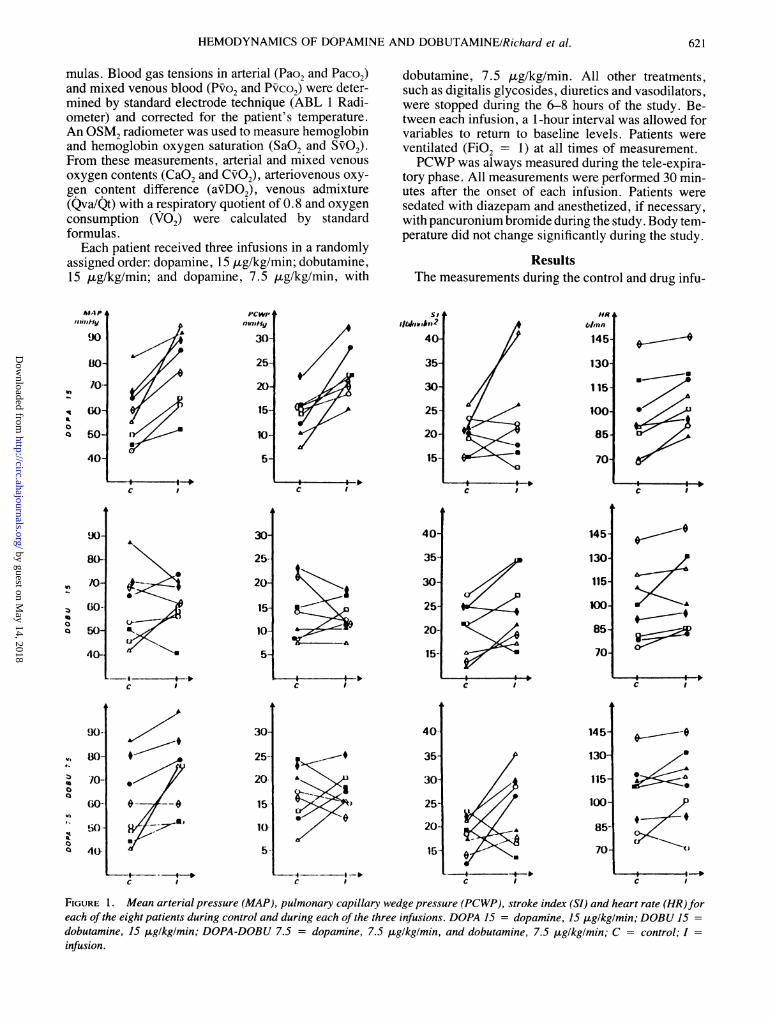
FIGURE 1. Mean arterial pressure (MAP), pulmonary capillary wedge pressure (PCWP), stroke index (SI) and heart rate (HR)foreach of the eight patients during control and during each of the three infusions. DOPA 15 = dopamine, 15 uiglkglmin; DOBU 15 =
dobutamine, 15 ,ug/kglmin; DOPA-DOBU 7.5 = dopamine, 7.5 gglkglmin, and dobutamine, 7.5 ,uglkglmin; C = control; I =
infusion.
to
0a
0
a
v,
zo0a
'4
a
621
by guest on May 14, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 67, No 3, MARCH 1983
TABLE 1. Hemodynamic Values During Control and Drug Infusion Periods
HR SI SARMAP MPAP PCWP RAP CI (beats/ (1/beats/ LVSWI (mm H/I/
Pt Order Treatment (mm Hg) (mm Hg) (mm Hg) (mm Hg) (1/minm2) min) m2) (g_m/M2) min/m)Ml 3 C
Dopa1 C
Dobu2 C
Dopa-dobuGR 2 C
Dopa1 C
Dobu
3 CDopa-dobu
FO 2 CDopa
3 CDobu
I CDopa-dobu
DA 3 CDopa
I CDobu
2 CDopa-dobu
VE 1 CDopa
2 CDobu
3 CDopa-dobu
BO 3 CDopa
2 CDobu
1 CDopa-dobu
CA 1 CDopa
3 CDobu
2 CDopa-dobu
LE 1 CDopa
3 CDobu
2 CDopa-dobu
55 21 7 5 2.3 90 26 18 219541604075
82928670
86985065
4557
48754652504044524362
52555052658564736878
6075
68606060668969688086
381816202626292625
39312831
2028212925342527
2825
262625182523243917263240263432232624294030282935
2177715
10151010
2015
1422
814
1320
1622
1517
241815181412
1715
1228
811
1217
16202111
16122232
23182325
1264S12710
10687S14
35
510
1215
1015
181479
33
107714461610711
97106161914121314
4.5
1.82.02.32.81.52.2
1.52.11.92.3
1.61.3
1.72.31.71.61.71.9
2.11.9
2.11.71.61.9
1.92.91.51.9
1.92.12.02.81.52.92.13.01.92.81.92.41.94.02.22.21.92.7
110
1181201101157084110100
112120
85100
8085741001181231001301101306790
7385
80701001208082
118110142146
14014614114591929293
9092
41
1517213521261221171919132127231615162115
19132322
273418282018
253412261521
1319141721432524
2229
43713103022281318
1623108
1117
1112
67
105
56914
1521
91515152030723916914
911133516171826
19
28201522
5138523141392839252325412020
20131322
23272518282330333024
5624
2521311926232618
25253427
Abbreviations: MAP = mean arterial pressure; MPAP = mean pulmonary arterial pressure; PCWP = pulmonary capillary wedge pressure;RAP = right atrial pressure; CI = cardiac index; HR = heart rate; SI = stroke index; LVSWI = left ventricular stroke work index; SAR =
systemic arterial resistance; Pao2 = arterial blood gas tension; Pfio2 = mixed venous blood gas tension; Qva/Qt = venous admixture; aI)Do2= arteriovenous oxygen content difference; V02 = oxygen consumption; Dopa = dopamine, 15 gug/kg/min; Dobu = dobutamine, 15 gg/kg/min; Dopa-dobu = dopamine, 7.5 ,ug/kg/min, and dobutamine, 7.5 ,ug/kg/min.
sion periods for each patient are listed in table 1. CI,SVI, LVSWI and heart rate (HR) increased to a similarextent during dopamine, dobutamine and dopamine-dobutamine. There were no significant intertreatment
differences for the four variables (table 2). MAP wassignificantly higher (p < 0.001) during dopamine anddopamine-dobutamine infusions than during dobuta-mine infusion (table 3, fig. 1). An increase in MAP
CIRCULATION622
by guest on May 14, 2018
http://circ.ahajournals.org/D
ownloaded from

HEMODYNAMICS OF DOPAMINE AND DOBUTAMINE/Richard et al.
TABLE 1. (Continued)
Pao2378335364369403365347339365298
359287352321286268197338240167210207167224296155
238268271180418336
45937539134637615640638140939112172
98918764
Pi'o23741333535363747
3540
39464231394338343228302931302936
2934
2635373636402440
394337443742
273030332930
Qva/Qt182114161416212719282131221627282717
2021
191921201731
20221429152412201020173314201418283935403447
aiDo2(ml/dl)4.44.15.85.1
5.55.04.12.94.13.13.92.73.85.8
3.53.44.25.45.46.06.36.35.85.96.03.85.64.57.94.24.54.35.03.98.44.14.53.65.13.75.04.04.83.73.63.24.13.0
V02(ml/mini
m2)
104183103101120142
606360657561607559687185951171291231211009473
109131115818891101110
122117961079610297979114781707981
was observed in eight patients during dopamine infu-sion, in six during the dopamine-dobutamine infusion,and in three during dobutamine infusion.SAR was significantly lower (p < 0.05) during
dobutamine infusion than during dopamine and do-pamine-dobutamine infusions (table 3). PCWP was
significantly higher (p < 0.001) during dopamine in-fusion than during dobutamine and dopamine-dobuta-
mine infusions (table 4, figs. 1, 2). In patients in whomMAP increased, there was no deleterious increase inPCWP (i.e., > 20 mm Hg) in three patients duringdopamine infusion, five during dopamine-dobutamineinfusion and three during dobutamine infusion.The Pao2 was significantly lower (p < 0.05) during
dopamine infusion than during dobutamine and dopa-mine-dobutamine infusions. Q ia/Qt increased to asimilar extent during each of the three infusions. Theincrease in PvO2 during dobutamine and dopamine-dobutamine infusions was smaller than during dopa-mine infusion (NS) (table 5). V02 was significantlyhigher (p < 0.05) during dopamine infusion than dur-ing dobutamine and dopamine-dobutamine infusions(table 5).
DiscussionAll our patients in cardiogenic shock received inter-
mittent positive pressure ventilation (IPPV) withoutPEEP. Mechanical ventilation was instituted whendrug treatment of pulmonary edema with hypotensionproved ineffective with diuretics, digitalis glycosides,vasodilators and dobutamine. Under these circum-stances we measured tele-expiratory PCWP and be-lieve that this measurement gave a good estimation oftransmural pressures. This was assumed because dur-ing the passive expiratory phase of IPPV, intrathoracicpressure (i.e., intrapleural or intraesophageal pressure)is near atmospheric pressure, since passive expirationin sedated patients is only affected by the elastic recoilpressure of the lung. This estimation was considered tobe accurate, as PEEP was not used and sympathomi-metic amines have no known effects on chest wall andlung compliance. Mechanical ventilation can induce adecrease in tele-expiratory PCWP by increasing intra-thoracic pressure and reducing venous return.9 An in-crease in intrathoracic pressure is also associated witha decrease in cardiac output and in systemic arterialpressure. '0Our results clearly indicate that an improvement in
hemodynamic status occurs during infusion of the do-pamine and dobutamine, 7.5 ug/kg/min each. MAP,CI and SVI increase, while PCWP remains normal. Nosevere hypoxemia and no dramatic change in SARappear. To our knowledge, these findings have notbeen previously reported.The three infusions have a similar effect on cardiac
output, but this effect is associated with a higher V02with dopamine infusion than with dopamine-dobuta-mine combined. Moreover, in two of our patients incardiogenic shock, the capacity of dopamine alone toimprove cardiac output was reduced. This reduced andoften unpredictable effect of dopamine in patients inheart failure has been reported previously."' 12 Thecause is a depletion of endogenous noradrenalinestores rather than an increase in SAR."' 12 The hemo-dynamic effects of dopamine decrease after 72 hours ofinfusion, and a transient cardiocirculatory deteriora-tion could appear after withdrawal of dopamine. I3 Theassociation of dobutamine, a potent inotropic agentthat acts directly on myocardial /3, adrenergic recep-
623
by guest on May 14, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 67, No 3, MARCH 1983
tors, can prevent this deleterious effect. Our resultsindicate a similar increase in venous admixture afterthe three treatments. An increase in Qva/Qt is the con-sequence of improvement in cardiac output. When car-
diac output increases, a recruitment mechanism is ob-served with opening of capillaries in unventilated areasof the lung.'4 However, dopamine increases hypox-emia, probably as a consequence of increasing PCWP
TABLE 2. Cardiac Index, Stroke Index, Left Ventricular Stroke Work Index and Heart Rate Before and 30 Minutes AfterEach Infusion
Dopamine, Dobutamine, Dopamine-dobutamine,15 Ag/kg/min 15 ,ug/kg/min each 7.5 ,ug/kg/min0 30 0 30 0 30 p
CI (1/mn/M2) 1.8+0.1 2.6±0.4 1.9+0.1 2.4±0.2 1.8±0.1 2.3 ±0.2 NSSI (ml/beat/m2) 20+1.3 25±4 20+2 24±2.6 18±1.4 23+2.7 NSLVSWI (g-m/m2) 13+2 20±5 13+2 17±3 11±2 18±3 NSHR (beats/min) 96±9 109+7 99±8 105+9 105±6 110+8 NS
Values are mean ± SEM.Comparison between the three treatments using A (30-0) index and two-way analysis of variance.Abbreviations: CI = cardiac index; SI = stroke index; LVSWI = left ventricular stroke work index; HR = heart rate.
TABLE 3. Mean Arterial Pressure and Systemic Arterial Resistance Before and 30 Minutes After Each InfusionDopamine, Dobutamine, Dopamine-dobutamine,
15 ,ug/kg/min 15 ,ug/kg/min each 7.5 ,ug/kg/min0 30 0 30 0 30
MAP (mm Hg) 58±4.6 77±5.7t 59±5.3 60+4 60±6 72±5.7tSAR (mm Hg/l/min/m2) 28 3.5 27± 3. 1* 29 + 3.6 22 ± 2.1 30± 5 28 + 2.8*
Values are mean ± SEM.Comparison of dopamine and dopamine-dobutamine vs dobutamine using A(30-0) index and two-way analysis of
variance and Newman-Keuls test:*p < 0.05.tp < 0.01.
TABLE 4. Right Atrial Pressure, Mean Pulmonary Arterial Pressure and Pulmonary Capillarv Wedge Pressure Beforeand 30 Minutes After Each Infusion
Dopamine, Dobutamine, Dopamine-dobutamine,15 ,ug/kg/min 15 gg/kg/min each 7.5 4g/kg/min
0 30 0 30 0 30RAP (mm Hg) 8±1.4 13±1.1* 7±1.4 7±1.5 11.7±1.7 10±1.1MPAP (mm Hg) 26±0.9 34±1.8t 24±1.9 24±1.6 27+2.2 29±2.1PCWP (mm Hg) 14±1.6 23±1.9t 14±2.2 12±1.3 16±2.1 17±1.4
Values are mean ± SEM.Comparison of dopamine vs dobutamine and vs dopamine-dobutamine using A(30-0) index and two-way analysis of
variance and Newman-Keuls test:*p < 0.01.tp < 0.001.
TABLE 5. Arterial Blood Oxygen Pressure, Mixed Venous Blood Oxygen Pressure, Venous Admixture, ArteriovenousOxygen Content Difference and Oxygen Consumption Before and 30 Minutes After Each Infusion
Dopamine, Dobutamine, Dopamine-dobutamine,15 gg/kg/min 15 jug/kg/min each 7.5 ,g/kg/min
0 30 0 30 0 30PaO2 (mm Hg) 316 ± 34 235 ± 38* 303 + 42 282 ± 35 285 ±-44 274 ± 39Pv2 (mm Hg) 35± 1.8 37±2.4 32±2 37±2 34± 1.3 37±+1.9Qva/Qt 19.7 ± 1.4 26.5 2.6 20.0 ± 2.7 24.1 ± 2.7 19.4 ± 2.8 24.7 ± 3.7aiDO2 (ml/dl) 4.7 ±0.3 4.3 ±0.4 4.9 ±0.4 4.2±0.4 5.6±0.6 4.3 ±0.4O2 (ml/min/m2) 86±6 110± 14* 92±9 96±9 101 ±8 96±9Values are mean ± SEM.Comparison of dopamine vs dobutamine and vs dopamine-dobutamine using A(30-0) index and two-way analysis of
variance and Newman-Keuls test:*p < 0.05.Abbreviations: See table 1.
624 CIRCULATION
by guest on May 14, 2018
http://circ.ahajournals.org/D
ownloaded from
HEMODYNAMICS OF DOPAMINE AND DOBUTAMINE/Richard et al.
31'ml/mn-m2
25-
20-
10 20
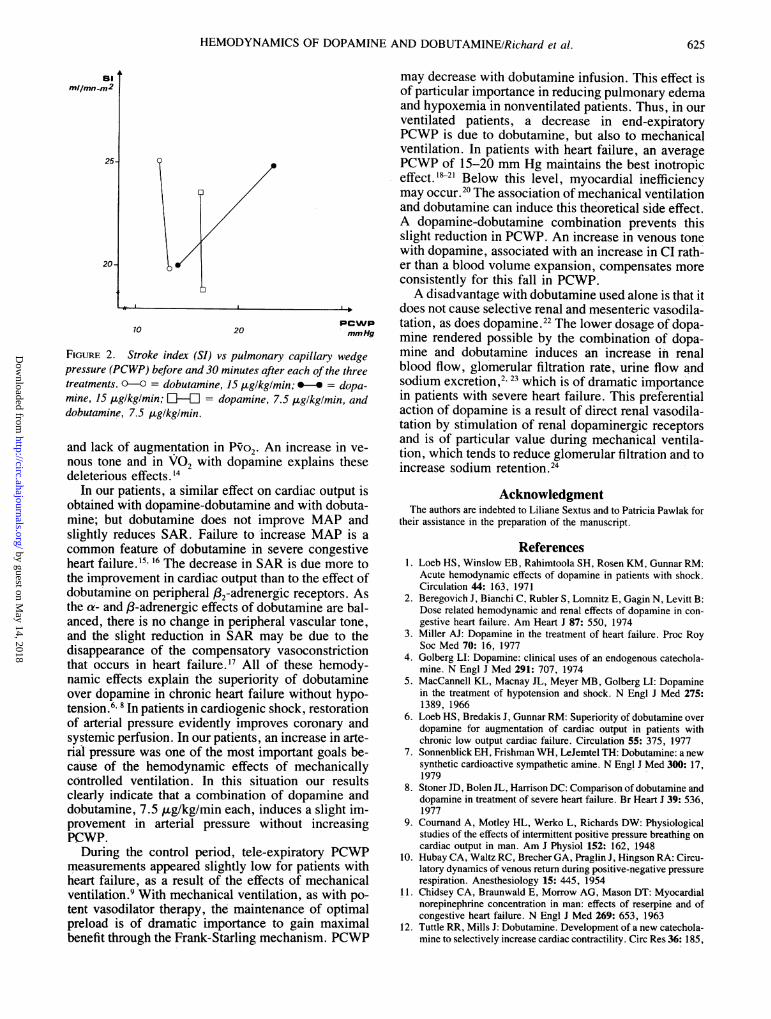
FIGURE 2. Stroke index (SI) vs pulmonary capillary wedgepressure (PCWP) before and 30 minutes after each of the threetreatments. 0-C = dobutamine, 15 ,uglkg/min; *-* = dopa-mine, 15 ,uglkglmin; Ll-LIE = dopamine, 7.5 gglkglmin, anddobutamine, 7.5 lzglkglmin.
and lack of augmentation in Po2. An increase in ve-nous tone and in V02 with dopamine explains thesedeleterious effects.'4
In our patients, a similar effect on cardiac output isobtained with dopamine-dobutamine and with dobuta-mine; but dobutamine does not improve MAP andslightly reduces SAR. Failure to increase MAP is acommon feature of dobutamine in severe congestiveheart failure.'5 16 The decrease in SAR is due more tothe improvement in cardiac output than to the effect ofdobutamine on peripheral ,82-adrenergic receptors. Asthe a- and ,B-adrenergic effects of dobutamine are bal-anced, there is no change in peripheral vascular tone,and the slight reduction in SAR may be due to thedisappearance of the compensatory vasoconstrictionthat occurs in heart failure.17 All of these hemody-namic effects explain the superiority of dobutamineover dopamine in chronic heart failure without hypo-tension.6' 8 In patients in cardiogenic shock, restorationof arterial pressure evidently improves coronary andsystemic perfusion. In our patients, an increase in arte-rial pressure was one of the most important goals be-cause of the hemodynamic effects of mechanicallycontrolled ventilation. In this situation our resultsclearly indicate that a combination of dopamine anddobutamine, 7.5 ,ug/kg/min each, induces a slight im-provement in arterial pressure without increasingPCWP.
During the control period, tele-expiratory PCWPmeasurements appeared slightly low for patients withheart failure, as a result of the effects of mechanicalventilation.9 With mechanical ventilation, as with po-tent vasodilator therapy, the maintenance of optimalpreload is of dramatic importance to gain maximalbenefit through the Frank-Starling mechanism. PCWP
may decrease with dobutamine infusion. This effect isof particular importance in reducing pulmonary edemaand hypoxemia in nonventilated patients. Thus, in ourventilated patients, a decrease in end-expiratoryPCWP is due to dobutamine, but also to mechanicalventilation. In patients with heart failure, an averagePCWP of 15-20 mm Hg maintains the best inotropiceffect.'-2' Below this level, myocardial inefficiencymay occur.20 The association of mechanical ventilationand dobutamine can induce this theoretical side effect.A dopamine-dobutamine combination prevents thisslight reduction in PCWP. An increase in venous tonewith dopamine, associated with an increase in CI rath-er than a blood volume expansion, compensates moreconsistently for this fall in PCWP.A disadvantage with dobutamine used alone is that it
does not cause selective renal and mesenteric vasodila-tation, as does dopamine.22 The lower dosage of dopa-mine rendered possible by the combination of dopa-mine and dobutamine induces an increase in renalblood flow, glomerular filtration rate, urine flow andsodium excretion,2 23 which is of dramatic importancein patients with severe heart failure. This preferentialaction of dopamine is a result of direct renal vasodila-tation by stimulation of renal dopaminergic receptorsand is of particular value during mechanical ventila-tion, which tends to reduce glomerular filtration and toincrease sodium retention.24
AcknowledgmentThe authors are indebted to Liliane Sextus and to Patricia Pawlak for
their assistance in the preparation of the manuscript.
References1. Loeb HS, Winslow EB, Rahimtoola SH, Rosen KM, Gunnar RM:
Acute hemodynamic effects of dopamine in patients with shock.Circulation 44: 163, 1971
2. Beregovich J, Bianchi C, Rubler S, Lomnitz E, Gagin N, Levitt B:Dose related hemodynamic and renal effects of dopamine in con-gestive heart failure. Am Heart J 87: 550, 1974
3. Miller AJ: Dopamine in the treatment of heart failure. Proc RoySoc Med 70: 16, 1977
4. Golberg LI: Dopamine: clinical uses of an endogenous catechola-mine. N Engl J Med 291: 707, 1974
5. MacCannell KL, Macnay JL, Meyer MB, Golberg LI: Dopaminein the treatment of hypotension and shock. N Engl J Med 275:1389, 1966
6. Loeb HS, Bredakis J, Gunnar RM: Superiority of dobutamine overdopamine for augmentation of cardiac output in patients withchronic low output cardiac failure. Circulation 55: 375, 1977
7. Sonnenblick EH, Frishman WH, LeJemtel TH: Dobutamine: a newsynthetic cardioactive sympathetic amine. N Engl J Med 300: 17,1979
8. Stoner JD, Bolen JL, Harrison DC: Comparison of dobutamine anddopamine in treatment of severe heart failure. Br Heart J 39: 536,1977
9. Cournand A, Motley HL, Werko L, Richards DW: Physiologicalstudies of the effects of intermittent positive pressure breathing oncardiac output in man. Am J Physiol 152: 162, 1948
10. Hubay CA, Waltz RC, Brecher GA, Praglin J, Hingson RA: Circu-latory dynamics of venous return during positive-negative pressurerespiration. Anesthesiology 15: 445, 1954
11. Chidsey CA, Braunwald E, Morrow AG, Mason DT: Myocardialnorepinephrine concentration in man: effects of reserpine and ofcongestive heart failure. N Engl J Med 269: 653, 1963
12. Tuttle RR, Mills J: Dobutamine. Development of a new catechola-mine to selectively increase cardiac contractility. Circ Res 36: 185,
,v No
625
by guest on May 14, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 67. No 3, MARCH 1983
197513. Leier CV, Heban PT, Huss P, Bush CA, Lewis RP: Comparative
systemic and regional hemodynamic effects of dopamine and dobu-tamine in patients with cardiomyopathic heart failure. Circulation58: 466, 1978
14. Jardin F, Eveleigh MC, Gurdjian F, Margairaz A: Venous admix-ture in human septic shock. Circulation 60: 155, 1978
15. Andy JJ, Curry CL, Ali N, Mehrotra PP: Cardiovascular effects ofdobutamine in severe congestive heart failure. Am Heart J 94: 175,1977
16. Leier CV, Webel J, Bush CA: The cardiovascular effects of thecontinuous infusion of dobutamine in patients with severe cardiacfailure. Circulation 56: 468, 1977
17. Herber P, Tinker J: Inotropic drugs in acute circulatory failure. IntCare Med 6: 101, 1980
18. Mason DT: Symposium on vasodilatator and inotropic therapy ofheart failure. Am J Med 65: 101, 1978
19. Miller RR, Palomo AR, Brandon TA, Hartley CJ, Quinones MA:Combined vasodilator and inotropic therapy of heart failure. Ex-
perimental and clinical concepts. Am Heart J 102: 500, 198120. Miller RR, Vismara LA, Zelis R, Amsterdam EA, Mason DT:
Clinical use of sodium nitroprusside in chronic ischemic heartdisease. Effects on peripherical vascular resistance and venous toneand on ventricular volume, pump and mechanical performance.Circulation 51: 328, 1975
21. Miller DC, Stinson EB, Oyer PE: Postoperative enhancement ofleft ventricular performance by combined inotropic vasodilatortherapy with preload control. Surgery 88: 108, 1980
22. Vatner JF, McRitcher RJ, Braunwald E: Effects of dobutamine onleft ventricular performance, coronary dynamics and distributionof cardiac output in conscious dogs. J Clin Invest 53: 1265, 1974
23. Golberg LI, MacDonald RH, Zimmerman AM: Sodium diuresisproduced in patients with congestive heart failure. N Engl J Med269: 1060, 1963
24. Marquez JM, Douglas ME, Downs JB, Wenhsein W, Mantini EL,Kuck EJ, Calderwood HW: Renal function and cardiovascularresponses during positive airway pressure. Anesthesiology 50:393, 1979
Late Sudden Death After Repair of Tetralogy of Fallot:A Clinicopathologic Study
JOHN E. DEANFIELD, M.R.C.P., SIEW-YEN Ho, M.PHIL., ROBERT H. ANDERSON, M.D.,WILLIAM J. MCKENNA, M.D., SALLY P. ALLWORK, PH.D., AND KATHARINE A. HALLIDIE-SMITH, M.R.C.P.
SUMMARY Retrospective analysis was performed to determine the likely cause of death in six patientswho died suddenly 1-9 years after repair of tetralogy of Fallot. The integrity of the atrioventricularconduction system and myocardium was examined in three hearts at necropsy. Two of three patients whocomplained of palpitation or syncope had frequent premature ventricular complexes on routine ECGs. Allthe patients had complete right bundle branch block and one had left-axis deviation after repair. Postoper-ative cardiac catheterization (four patients) showed no residual ventricular septal defects, but right ventric-ular pressure was elevated in all.At necropsy, the atrioventricular conduction tissue was related to the margin of perimembranous ventric-
ular septal defect in two patients, but was well posterior in one patient with an infundibular musculardefect. Histologic examination showed that in all cases the atrioventricular node, atrioventricular bundleand left bundle branch were undamaged. There was, however, extensive fibrosis of the right ventricularmyocardium in the ventriculotomy site (three patients), septum (one patient) and outflow tract (onepatient).
These clinical and necropsy findings suggest that ventricular arrhythmia rather than atrioventricularblock was responsible for sudden death in these patients after repair of tetralogy of Fallot.
SUDDEN DEATH is a recognized late event afterrepair of tetralogy of Fallot, with a reported incidenceof as high as 4.6%. 1-3 These deaths are assumed to bedue to cardiac arrhythmia, but the precise mechanismis controversial. Attention was focused initially on thepossibility of late complete atrioventricular block from
From the Royal Postgraduate Medical School, Hammersmith Hospi-tal, and the Cardiothoracic Institute, Brompton Hospital, London,England.
Dr. Deanfield was supported by the Medical Research Council (Unit-ed Kingdom), Dr. Ho, Prof. Anderson and Dr. Allwork by the BritishHeart Foundation, and Dr. McKenna by the Medical Research Council(Canada).
Address for correspondence: John E. Deanfield, M.R.C.P., Divisionof Cardiology, Royal Postgraduate Medical School, HammersmithHospital, Du Cane Road, London W12 OHN, England.
Received July 14, 1982; revision accepted October 21, 1982.Circulation 67, No. 3, 1983.
progressive damage to the proximal conduction sys-tem. This concept arose when the electrocardiographicpattern of right bundle branch block and left-axis devi-ation was found in a proportion of patients after intra-cardiac repair.4 A poor prognosis was reported for pa-tients with these conduction defects,5 but has not beenconfirmed by others..3', Recently, a high incidence ofventricular arrhythmia has been demonstrated afterradical correction, and has been associated with sud-den death in retrospective series.2'," Despite this con-troversy regarding the mechanism for sudden death,there have been no pathologic studies of the conduc-tion system in patients who died suddenly after repairof tetralogy of Fallot. We therefore examined the in-tegrity of the conduction system and myocardium innecropsy specimens from such patients to ascertain theanatomic correlates related to sudden death.
CIRCULATION626
by guest on May 14, 2018
http://circ.ahajournals.org/D
ownloaded from

C Richard, J L Ricome, A Rimailho, G Bottineau and P AuzepyCombined hemodynamic effects of dopamine and dobutamine in cardiogenic shock.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1983 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.67.3.620
1983;67:620-626Circulation.
http://circ.ahajournals.org/content/67/3/620the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 14, 2018
http://circ.ahajournals.org/D
ownloaded from