combined therapy with insulin plus oral agents - codhycombined therapy with insulin plus oral agents...
TRANSCRIPT

Combined Therapy withInsulin Plus Oral Agents
Is there Any Advantage?
Matthew C. Riddle, M.D.
Professor of Medicine
Oregon Health & Science University
Portland, Oregon

Yes !Gewiss! Vraiment!
Most patients with type 2 diabetesneed combination therapy
to reach usual glycemic targets
. . . including those who need insulin
Is there Any Advantage in Combined Therapy?

The Clinical ProblemLoss of Control with Monotherapy in the UKPDS
UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:837-853.
9
8
7
6
00 3 6 9
Years From Randomization
12 18
Conventional (diet)
Intensive (SU or insulin)
Med
ian
Hb
A1
c(%
)

Monotherapy in the UKPDS Obese Substudy
Turner RC et al. UKPDS 49. J Am Med Ass 1999;21:2005
Percent with HbA1c < 7% on monotherapy3 years 6 years 9 years
Diet 23 12 11
Sulfonylurea 45 28 21
Metformin 44 34 13
Insulin 34 37 24

Turner RC et al. UKPDS 49. J Am Med Ass 1999;21:2005
“The majority of patients need
multiple therapies
to attain these target goals in the longer term.”
Monotherapy in the UKPDS Obese Substudy
Why combine oral agents with insulin?
Pharmacology
Physiology
Clinical trials

Why combine oral agents with insulin?
Pharmacology
The ratio of desired to undesired effectsmay be improved

Dose-response Relationships forEffects of Treatments
50 100
Desired effect Undesired effect
50
0
100
50
50
0
100
% of maximal dose
% of maximal effect
100
% incidence

Dose-response Relationships forMetformin
1000 2500
HbA1c reduction GI symptoms
50
0
100
1000
50
0
100
Mg metformin daily
% of maximal effect
2500
% incidence
?20-30%
5%
Garber AJ et al. Am J Med 1997;102:491
h
h
h
hh

Dose-response Relationships forGlimepiride
4 8
HbA1c reduction Hypoglycemia
50
0
100
4
50
0
100
Mg glimepiride daily
% of maximal effect
8
% incidence
2
Goldberg RB et al. Diabetes Care 1996;19: 849
h
h h

Why combine oral agents with insulin?
Physiology
Glycemic variability and hypoglycemiacan be reduced by enhancing
the effectiveness of endogenous insulin

Three Main Oral agent + Insulin Combinations
Sulfonylureas + Insulin
Metformin + Insulin
Thiazolidinediones + Insulin

Smooth Transition to Insulinwhile Continuing Glimepiride
Riddle MC et al. Diabetes Care. 1998;21:1052-57
mg/dL
0
300
*
* *****
*
250
200
150
100
4 8 12 16 20 24
Weeks of treament
FPG
Placebo + 70/30 insulin titrated to 140 mg/dL
Glimepiride + insulin
0
100
75
50
25
04 8 12
Insulin Dosage
16 20 24
Weeks of treament* P <.001 * P <.001† P <.05
Units/Day
†
Quicker control with 37% less injected insulin

Metformin or Glitazone + CSII in T2DMEffect on Plasma Glucose
Yu et al. Diabetes 1999;48:2414-21
0800 1200 1600 2400 0800
Metformin
Continuous insulin infusion
Troglitazone
100
50
0
mg/dL150
0800 1200 1600 2400 0800
Continuous insulin infusion plus metforminContinuous insulin infusion
Continuous insulin infusion plus troglitazone
100
50
0
150
Time of day Time of day
Equivalently excellent glycemic control
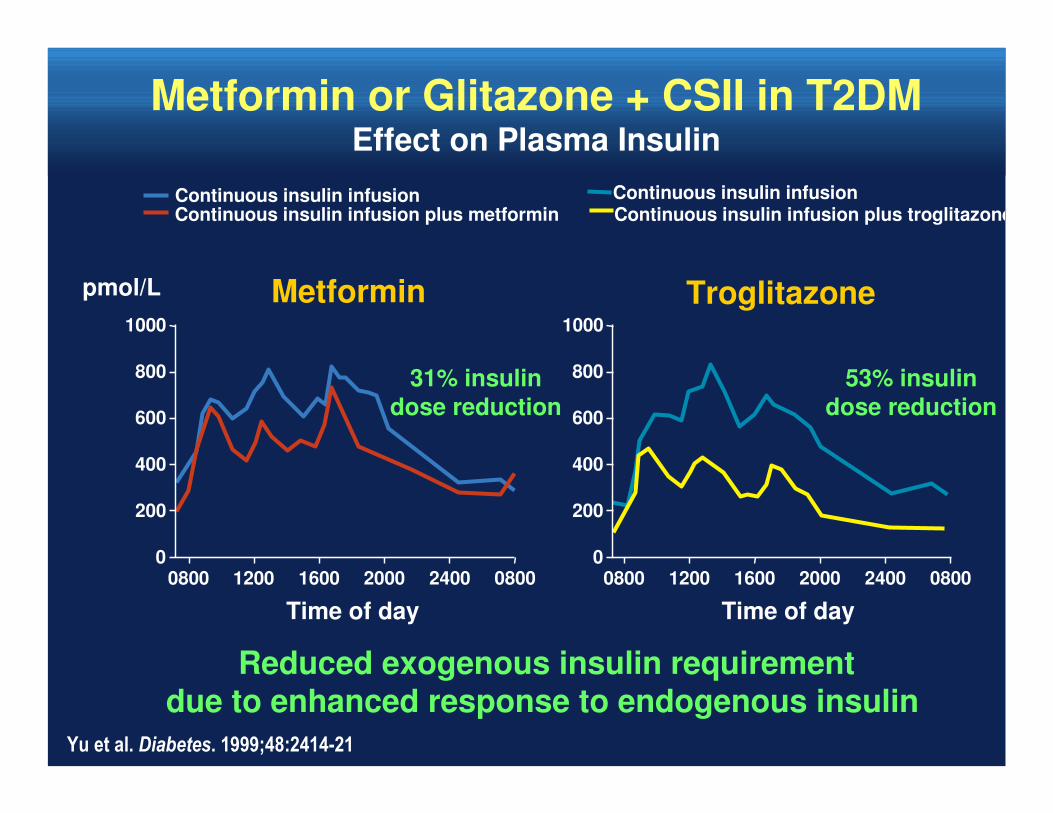
Metformin or Glitazone + CSII in T2DMEffect on Plasma Insulin
0800 1200 1600 2400 0800
Metformin
Continuous insulin infusion
1000
600
400
200
0
Troglitazone
800
1000
600
400
200
0
pmol/L
800
0800 1200 1600 2400 0800
Continuous insulin infusion plus metforminContinuous insulin infusionContinuous insulin infusion plus troglitazone
2000 2000
Time of day Time of day
31% insulindose reduction
53% insulindose reduction
Yu et al. Diabetes. 1999;48:2414-21
Reduced exogenous insulin requirementdue to enhanced response to endogenous insulin

Variability of FPG in 2 Studiesof glibenclamide and evening insulin
Placebo/Ins Glibenclamide/Ins
Bedtime NPH 1.7 ± 0.2 1.1 ± 0.1
Riddle MC et al. P < 0.05
Diabetes Care 1989;12:623-9
Suppertime 70/30 1.4 ± 0.3 0.8 ± 0.1
Riddle MC et al. P < 0.05
Am J Med Sci 1992;:303:151-6
35 and 43% less variability with combination therapy
SD of sequential FPG measurements
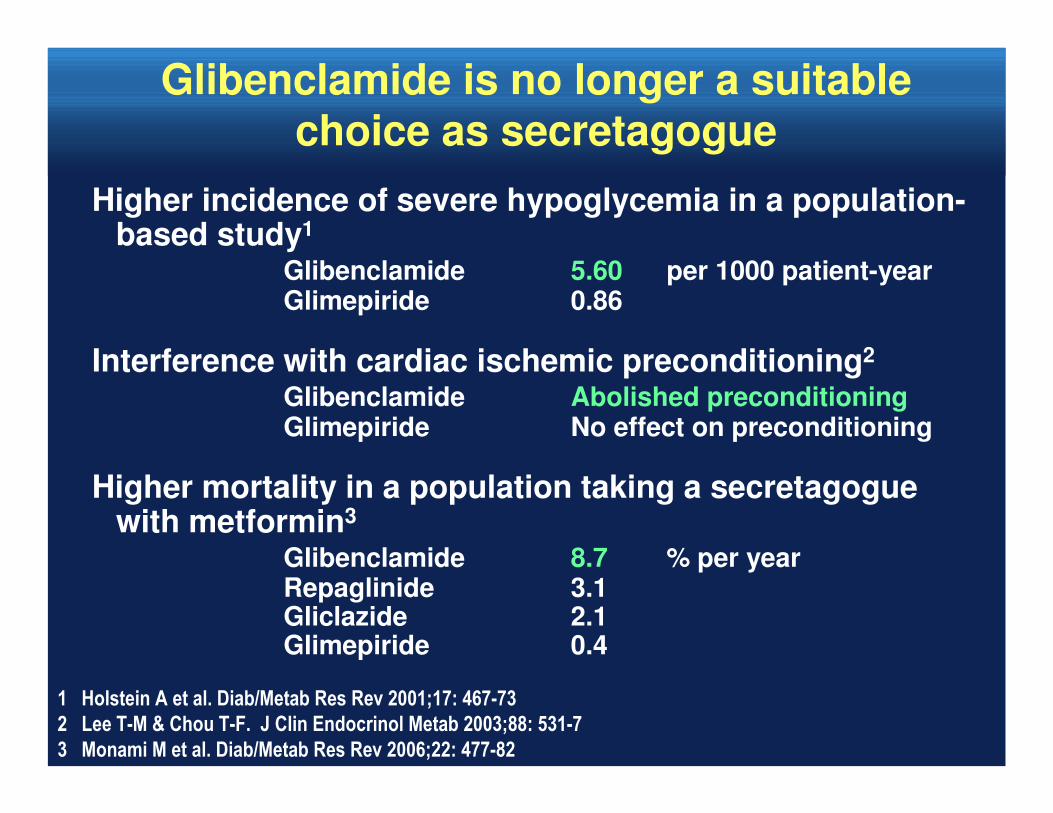
Glibenclamide is no longer a suitable choice as secretagogue
Higher incidence of severe hypoglycemia in a population-based study1
Glibenclamide 5.60 per 1000 patient-yearGlimepiride 0.86
Interference with cardiac ischemic preconditioning2
Glibenclamide Abolished preconditioningGlimepiride No effect on preconditioning
Higher mortality in a population taking a secretagoguewith metformin3
Glibenclamide 8.7 % per yearRepaglinide 3.1Gliclazide 2.1Glimepiride 0.4
1 Holstein A et al. Diab/Metab Res Rev 2001;17: 467-73
2 Lee T-M & Chou T-F. J Clin Endocrinol Metab 2003;88: 531-7
3 Monami M et al. Diab/Metab Res Rev 2006;22: 477-82

Secretagogues increase the proportion of insulin from endogenous secretion
Sensitizers increase the responseto endogenous insulin
Summary of physiologic studies
. . . both improve the effectivenessof remaining endogenous insulin

Why combine oral agents with insulin?
Clinical trials
Better glycemic control achievedLess weight gain

Improvement of Glycemic Controlwith Combination Therapy
Yki-Jarvinen H. Diabetes Care 2001;24: 738-67
Previously insulin-treated T2DM patients
Regimen Glycated Hb reductionvs insulin alone
(despite insulin dose reductions)
Insulin + sulfonylurea - 0.4%7 studies
Insulin + metformin - 1.3%4 studies
Insulin + TZD - 1.3%2 studies

Initiation of Bedtime NPH Insulin ± Glipizide
Shank M et al. Diabetes. 1995;44:165-72
0
100
220
140
248
113
8.6
7.8
8.9
7.1
200
300
6
7
8
9
Baseline on Glipizide 20 mg/d
Bedtime NPH Bedtime NPH
+ glipizide
Bedtime NPH Bedtime NPH
+ glipizide
10FPG HbA1c
After bedtime NPH titrated to FPG 120 mg/dL
mg/dL %
Better control with combination therapy
- 0.7%
N = 18 T2DM

Metformin + Intensified N + R Insulin
Insulin + Placebo Insulin + Metformin
N = 22 N = 21
Insulin dosage (U/d)
Baseline 97 96
6 months 120 92
Weight (kg)
Baseline 107 104
6 months 110 104
HbA1c (%)
Baseline 9.1 9.0
6 months 7.6 6.5
-1.1%
Aviles-Santa et al. Ann Intern Med 1999;131:182-8
-3 kg
Better control and no weight gain with combination therapy

Intensive Insulin Therapy ± Metformin
390 type 2 patients on insulin or insulin + metforminMean age 61 yr, duration 13 yr, BMI 30, A1c 7.9%
Randomized to Insulin 2 to 4 injections + PlaceboInsulin 2 to 4 injections + metformin 850-2550 mg
EndpointsAt 48 months – CV morbidity and mortalityAt 16 weeks – glycemic control
An early report after 16 weeks:“ . . . unexpected favorable effects of metformin”
Wulffele MG et al. Diabetes Care 2002;25: 2133-40

Intensive Insulin Therapy ± Metformin
Insulin + placebo Insulin + metformin
Insulin u/d 71 64Metformin mg/d --- 2163
A1c %Endpoint 7.6 6.9∆ - 0.3 - 0.9Placebo adj ∆ --- - 0.6 <0.0001
Weight kg∆ + 1.2 - 0.4Placebo adj ∆ --- - 1.6 <0.0001
Hypoglycemia/pt-mo 1.12 1.52 NS
Wulffele MG et al. Diabetes Care 2002;25: 2133-40

Unanswered questions
Will limitation of weight-gain accompanyinginsulin treatment improve CV outcomes?
What are the roles of pramlintide and exenatide
combined with insulin?
Will using all available agents to get to A1c 6% improve outcomes?

Pramlintide + Basal-prandial Insulin in T2DM Open-label clinical experience study
130
150
170
190
210
230
acB pcB acL pcL acD pcD hs
*
*
*
*
*
* *
Glucosemg/dL
Baseline
6 Months
*P <0.05
Karl D et al. Diabetes 2005; 54(S1):A12; in press Diab Res Clin Pract

The ACCORD TrialCan we get to 6% A1c and will that improve outcomes?
10,000 type 2 patients -- to be followed ~ 5.5 yr
Primary endpoint -- major cardiovascular events
Double 2x2 factorial design
– Intensive vs standard glycemic policy (n=10,000)
– Intensive vs standard blood pressure policy(n=5800)
– Statin treatment with or without added fibrate(n=4200)
HbA1c target for intensive glycemic arm --
6%, using any combination of agents, including intensive insulin