community resources linda cragin, director massahec network 4-26-2013
TRANSCRIPT
Community Resources
Linda Cragin, Director
MassAHEC Network
4-26-2013

Today’s Objectives
• Understand the importance of care transitions
• Understand the range of community services available.
• Understand how to access community services.
• Understand the important role of informal/family caregivers.


Care Transitions:
• Better coordination of patient transfers among care sites and the community could save money and improve care.
• Care transition describes a continuous process as patient care shifts from one setting to another.
www.healthaffairs.org

Care Transitions:
• Hospitalizations account for approximately 33% of total Medicare expenditures ($524 billion in 2010) and represent the largest program outlay.
• The Medicare Payment Advisory Commission estimated Medicare costs of approximately $15 billion due to readmissions, $12 billion of which is for cases considered preventable.
• Other estimates range from $25 to $45 billion in wasteful spending (2011) due to avoidable complications and unnecessary hospital admissions.
www.cfmc.org, www.healthaffairs.org

Within 30 days of discharge,
19.6 % of Medicare beneficiaries are re-
hospitalized.
Jencks SF, Williams MV, Coleman EA: Rehospitalizations among patients in the Medicare Fee-for-service Program. NEJM 2009 Apr 2; 360(14):1418-28
ACA impact on Transitions
• Effective 10/1/12: - Increase Medicare payments if hospitals
achieve/exceed targets for certain quality measures – including discharge processes and instruction
- Reduce Medicare payments by 1% if readmission rates readmissions rates exceed a target for certain diagnoses.

Care Transitions:Patient and Caregiver Involvement, Medication reconciliation, Handoff communication and Discharge, Preparing patients for Discharge, Teamwork and Interdisciplinary Rounds, etc.
Collaboration between the hospitals and their community partners to effectively co-design better processes of patient transfer.
The Care Transitions Program® - Transition Coaches® work with patients with complex needs and coach them with self-management skills to ensure their needs are met during transition from hospital to home.
So where do patients go?

Rehab Hospital• intensive inpatient rehabilitation
therapy• specialized care (3+ hours of therapy
a day) from a team (MD, RN, PT/OT) • Patient must have improvement
potential: stroke, spinal cord, brain injury
• Less likely: hip fracture, knee replacement unless there are complications
• Coverage: Medicare Part A

Skilled Nursing/Extended Care Facilities:
• Medicare covers skilled care for 1-20-100 days
• Medicaid, long term care insurance and private payment for long term/chronic/extended care.
• Team based care: Nursing, PT, OT, ST, SW, Recreational Therapist, pharmacist consultant, medical director
• Scheduled interprofessional care planning meetings with patient/family involvement.
SNF Medicare Coverage:
• Patient was formally admitted as an inpatient to a hospital for at least three consecutive days in the 30 days prior to admission in a Medicare-certified skilled nursing facility (not ER observation!); and
• Medicare Part A covered the hospital stay
• Patient needs skilled nursing care seven days a week or skilled therapy services at least five days a week.
Critical opportunity for better transitions planning

Home Health Services: Skilled, Intermittent, Homebound
• Max: 8 hours/day and 28 hours/week. • Skilled nursing: performed by a
licensed nurseInjections (and teaching patients to self-inject), tube
feedings, catheter changes, wound care, etc.• Home health aide: if patient requires
skilled services. Includes help with bathing, toileting, dressing, etc. • Skilled therapy: performed by a licensed
therapistPT: gait training, regain/maintain movement and
strengthST: regain and strengthen speech and languageOT: regain/maintain the ability to do ADLs
• Medical social services• Coverage: Medicare Part A, no
deductible/co-insurance

Outpatient PT, OT, ST• Medically necessary • Medicare: if improvement or to
prevent deterioration• Limits! Medicare will cover up to
$1,880 for physical and speech therapy combined, and another $1,880 for occupational therapy.
• If patient approaches the limit and needs more, MD can tell Medicare that it is medically necessary
• Coverage: Medicare Part B

Hospice: • MD: life expectancy is <6 months (ALOS is 7 days!)
• Patient signs electing palliative care• Patient does not need to be
homebound• Comprehensive services delivered
by a team: RN, PT/OT/ST, pastoral care, social work, volunteers, respite, music and art therapists, massage, etc.
• Benefit includes two 90-day benefit periods followed by an unlimited number of 60-day benefit periods.
• Coverage: Part A
Medicare Advantage Plans• Health Maintenance Organizations (HMO)• Preferred Provider Organizations (PPO) • Private Fee-For-Service (PFFS) plans.• Special Needs Plans (SNP)• Provider Sponsored Organizations (PSO)• Medicare Medical Savings Accounts (MSAs)
In Massachusetts:Senior Care Options (SCOs)
Integrated Care Organizations (ICOs)
Program for All Inclusive Care for the Elderly (PACE)
Evercare
Some blend Medicare and Medicaid coverage…

Community Resources

Community Resources:
• Assisted Living and Supportive Housing
• Aging Services Access Points (in MA)
• Social Day Care or Adult Day Health
• Transportation
• Councils on Aging/Senior Centers
• etc.

Family Caregivers• Family caregivers are the foundation of long-term
care nationwide.• More than 65 million people, 29% of the U.S.
population, provide care for a chronically ill, disabled or aged family member or friend during any given year and spend an average of 20 hours per week.
• The value of these “free” services is estimated to be $375 billion a year; almost twice as much as is actually spent on homecare and nursing home services combined ($158 billion).
National Alliance for Caregiving 2009 various studies
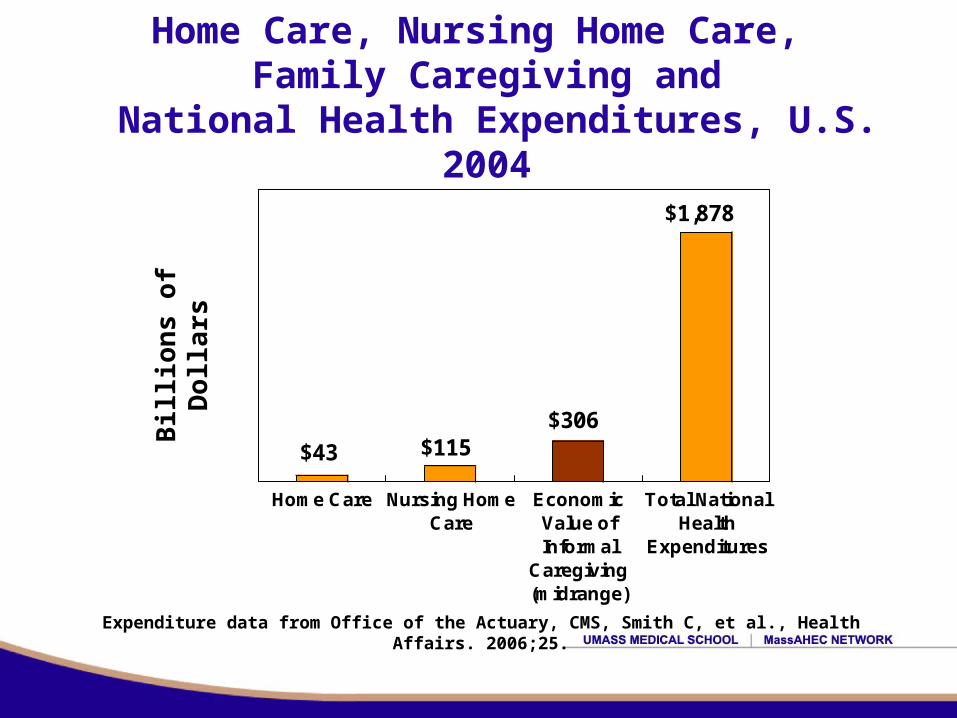
Home Care, Nursing Home Care, Family Caregiving and
National Health Expenditures, U.S. 2004
$43 $115$306
$1,878
Home Care Nursing HomeCare
EconomicValue ofInformal
Caregiving(midrange)
Total NationalHealth
Expenditures
Expenditure data from Office of the Actuary, CMS, Smith C, et al., Health Affairs. 2006;25.
Bill
ion
s o
f D
olla
rs
The typical family caregiver:
• A 49-year-old woman caring for her widowed 69-year-old mother who does not live with her.
• She is married and employed.
• Approximately 66% of family caregivers are women.• More than 37% have children or grandchildren under 18
years old living with them.
National Alliance for Caregiving 2009

Summary:
There are many community resources…
There are skilled, trained, professional staff caring across the spectrum of services…
Communication and coordination is critical…
Patient and family involvement is a must…
And… remember:
1-800-age-info www.800ageinfo.org