comparative nephrotoxicity of gentamicin and ...aac.asm.org/content/19/5/859.full.pdf ·...
TRANSCRIPT

Vol. 19, No. 5ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, May 1981, p. 859-8660066-4804/81/050859-08$02.00/0
Comparative Nephrotoxicity of Gentamicin and Tobramycin:Pharmacokinetic and Clinical Studies in 201 Patients
JEROME J. SCHENTAG,'* MARTIN E. PLAUT,2 AND FRANK B. CERRA3Departments of Pharmaceutics,' Medicine,2 and Surgery,3 Schools ofPharmacy' and Medicine,2'3 State
University ofNew York at Buffalo; Buffalo General Hospital,23; and Clinical PharmacokineticsLaboratory, Millard Fillmore Hospital,' Buffalo, New York 14209
Received 18 November 1980/Accepted 27 February 1981
A total of 201 critically ill patients were studied during 267 courses ofgentamicinor tobramycin treatment (139 gentamicin courses and 128 tobramycin courses).Of these 267 courses, pharmacokinetic and clinical data were obtained for 240(120 gentamicin and 120 tobramycin). The data collected for pharmacokineticanalysis included measurements of serial blood and urine levels, urinary excretionof fl2-microglobulin, protein levels, and granular casts. A two-compartment modelwas used to assess tissue accumulation, and in 89 courses the predicted accumu-lation was confirmed by cumulative urine collection or postmortem tissue analysis.As groups, the patients given gentamicin and tobramycin did not differ in age,weight, creatinine clearance, total dose given, duration of treatment, initialaminoglycoside trough serum levels, number of dosage adjustments, concurrentuse of furosemide, or concurrent cephalosporins. Previous aminoglycoside treat-ment (usually gentamicin) had occurred more frequently in the tobramycin-treated patients (P < 0.01), and more males than females received tobramycin(P < 0.05). Pharmnacokinetic assessments of renal damage were based on bothchanges in glomerular filtration rate (serum creatinine levels, creatinine clearance)and renal tubular damage (,82-microglobin, casts), but only patients with elevatedaminoglycoside tissue levels leading to renal tubular damage and subsequentcreatinine clearance decreases were considered to have experienced aminoglyco-side nephrotoxicity. In the pharnacokinetic analysis of nephrotoxicity, 29 genta-micin courses (24%) and 12 tobramycin courses (10%) were complicated bynephrotoxicity (P < 0.01). The 201 study patients were also evaluated indepen-dently for clinical nephrotoxicity (defined as a serum creatinine level increase of0.5 mg/dl or more). Clinical nephrotoxicity occurred at rates of 37% in thegentamicin-treated group and 22% in the tobramycin-treated group (P < 0.02). Inthese similar groups of critically ill patients, tobramycin was less nephrotoxicthan gentamicin.
Aminoglycoside antibiotics are potentially ne-phrotoxic substances which may cause specificdamage to the lining cells of renal proximaltubules. The incidence of reported nephrotoxicdamage in aminoglycoside-treated patients hasincreased from 5 to almost 40% recently (2, 4, 7,8, 19); the occurrence rate is apparently a func-tion of the type of patients studied, variations inthe methods used to define nephrotoxicity, andintensity of renal monitoring by investigators.The incidence of nephrotoxicity may also vary
with the aminoglycoside used. Animal studiesreadily differentiate these compounds. Genta-micin is more nephrotoxic than tobramycin, ne-tilmicin, or amikacin in animals (3, 5, 6). Inanimal studies elevated aminoglycoside dosesare used, which result in blood levels that mark-edly exceed the levels employed to treat humaninfections. Also, at least one compound must
produce nephrotoxicity in most study animals,so that these animals can serve as a referencepopulation for comparing aminoglycosides. Inhuman trials, nephrotoxicity is much less com-mon, and it may occur for different reasons thanoverdoses.The widespread clinical use of dosing nomo-
grams and the monitoring of serum concentra-tions mean that both overdoses and elevatedblood concentrations are avoided, yet nephro-toxicity still occurs (1, 2, 7, 16, 18, 19). Thus,animals are overdosed until renal failure occurs,whereas patients may experience renal damagedespite the use of recommended doses and ther-apeutic serum concentrations (1, 2, 15, 16, 18).In view of the differences between the nephro-toxic damage produced by overdoses in animalsand clinical aminoglycoside nephrotoxicity,comparative studies in animals may x; t provide
859
on May 11, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

860 SCHENTAG, PLAUT, AND CERRA
relevant models for characterization of compar-ative clinical nephrotoxicity. Furthermore, thebelief that aminoglycoside nephrotoxicity is al-ways dose related might also be challenged, sinceclinical nephrotoxicity has not been abolishedby the use of proper doses.Our pharmacokinetic studies in patients have
provided some insight into the pathogenesis ofrenal damage when appropriate doses are used.An early finding of these studies was that ab-normally high aminoglycoside accumulations inrenal tissue lead to proximal tubular damage,even though aminoglycoside blood levels remainnormal (9, 15). A characteristic pattem of renaltubular damage precedes an eventual increase inserum creatinine levels by 5 to 10 days (15). Inthe patients experiencing aminoglycoside neph-rotoxicity, increases in serum creatinine levelsoccur late in the sequence of events, after evi-dence of abnormally rapid tissue accumulationand proximal damage, as measured by urinesediment changes and excretion of f32-micro-globulin (14). Thus, an increase in the serumcreatinine level may reflect damage to the prox-imal tubules which actually began 5 to 7 daysbefore changes in glomerular filtration.We applied these criteria to a study of the
comparative nephrotoxicities of gentamicin andtobramycin. Our study involved two groups froma homogeneous population of acutely ill olderpatients having similar base-line risks for neph-rotoxicity and similar clinical complications dur-ing hospitalization.
MATERIALS AND METHODSPatients. A total of 201 acutely ill patients were
given 267 courses of aminoglycoside therapy (139 gen-tamicin courses, 128 tobramycin courses). These pa-tients were older adults (average age, 66 years) withserious infections complicating either major medicalor surgical disorders. All but a few of these patientshad abdominal infections, pneumonia, septicemia, ora combination of these diseases. Each was enteredprospectively into the study at the time of request fortherapy and pharmacokinetic monitoring, after gen-tamicin or tobramycin was selected for use by theattending physician. The rates of patient accessionwere similar for the gentamicin-treated and tobramy-cin-treated groups over the 2-year study period.Doses and sample collection. Rates of aminogly-
coside administration were determined individuallyfor all patients according to nomograms and measuredpeak and trough serum concentrations. Blood for as-says was obtained throughout treatment and in mostpatients for 10 to 20 days after aminoglycoside treat-ment was stopped (to quantitate the terminal half-life), as previously described (9, 10, 11-13, 15). Desiredtherapeutic peak concentrations were between 4 and10,ug/ml, and desired trough concentrations were 0.5to 2.0 Lg/ml for both aminoglycosides. Most patientshad been catheterized during their illness, and daily
24-h urine samples were collected to verify tissueaccumulation and to measure indices of renal tubulardamage. Pretreatment renal and pharmnacokinetic pa-rameters were obtained on the day before aminogly-coside administration was begun, or the value on treat-ment day 1 was used as the base-line value if a priorvalue was not available.
Assays. Serum, urine, and postmortem tissue ami-noglycoside concentrations were measured by both amicrobiological assay and a radioimmunoassay, as pre-viously described (12, 13). The lower limit of sensitivityfor the radioimmunoassay was 0.03 pg/ml; thus, thisassay allowed measurement of both serum and urineconcentrations for 10 to 30 days after the last dose.Serum creatinine levels and 24-h creatinine clearancevalues were determined by autoanalyzer methods; 24-h urinary excretion of 82-microglobulin was deter-mined by the radioimmunoassay, and values of morethan 50 mg/24 h were associated with nephrotoxicity(4). Quantitative cast counts were performed daily onrandom urine samples, and values of more than 500casts per mil on 3 consecutive days were associatedwith nephrotoxicity (10).
Pharmacokinetic analysis. Serum concentra-tions (Cp) in the washout phase were fitted to abiexponential equation (Cp = Ae-' + Be-'t) by usingthe NONLIN least-squares regression computer pro-gram. The A and B intercepts were adjusted for theamount of residual drug present from previous dosesto yield intercept values reflecting a single dose. Theslopes and adjusted intercept values were used tocalculate the rate constants and distribution volumesof the two-compartment model. These included thecentral and steady-state volumes of distribution, theintercompartment distribution rate constants, theelimination rate constant, and the body clearance. Thevalues of these parameters were used in another digitalcomputer program (NUMINT), which numerically in-tegrated the differential equations for the model tosimulate serum concentrations from the first dosethrough the final dose and for the washout period.When all computer-simulated serum concentrationvalues agreed within 20% with the measured concen-trations throughout treatment and in the washoutperiod, the calculated parameters of the model wereconsidered to be reliable. The NUMINT programprovided the amount of drug in the central and tissuecompartments of the two-component model duringtherapy and after therapy ended (11-13).
Nephrotoxicity. Nephrotoxicity was determinedin each course of treatment by using two sets ofcriteria. A clinical assessment of nephrotoxicity wasperformed independently of a pharmacokinetic assess-ment in a blind fashion. The clinical criterion fornephrotoxicity was an increase in the serum creatininelevel of 0.5 mg/dl or more during therapy or within 7days of the last dose. Unless another cause of theincrease was clearly apparent, the change was alwaysattributed to aminoglycoside treatment.
In the pharmacokinetic assessment of nephrotox-icity, two essential criteria were used to define neph-rotoxicity. The first was an abnormally high aminogly-coside tissue accumulation, which was defined as anamount more than two standard deviations above themean value for treated patients who did not show an
ANTIMICROB. AGENTS CHEMOTHER.
on May 11, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
NEPHROTOXICITIES OF GENTAMICIN AND TOBRAMYCIN 861
increase in the creatinine level. These abnormal valueswere more than 200 mg for gentamicin and more than175 mg for tobramycin (15). The second criterion ofthe pharmacokinetic assessment was an increase inurine ,I2-microglobin levels and casts occurring beforethe serum creatinine level increase in a specific pat-tern, as previously described (15). In the pharmacoki-netic definition of nephrotoxicity, serum creatininelevel increases of more than 0.5 mg/dl not precededby indices of renal tubular damage or abnormal tissueaccumulation were considered to be caused by some-thing other than aminoglycoside nephrotoxicity (15).
Anlalysis. Each course of aminoglycoside therapywas examined separately even in the same patient,since clinical status and risk factors could changecourse by course. About 25% of the patients werestudied during more than one course of therapy. Aseparate analysis of only those single-course patientswho had not received aminoglycosides prevously ex-amined the influence ofprevious aminoglycoside treat-ments on our findings. Differences between aminogly-cosides were analyzed by using the Student t test andthe chi-square test with the Yates correction. A Pvalue of <0.05 was considered significant.
RESULTSOf the 267 courses of treatment examined, 9
were excluded from the clinical analysis, eitherbecause of failure to determine serum creatininelevels after therapy or because hemodialysis in-validated serial creatinine level measurements.The remaining 258 courses were analyzed byusing clinical criteria.Of the 267 courses, 27 were excluded from the
pharmacokinetic analysis because there were in-adequate data to employ the pharmacokineticcriteria for nephrotoxicity. Of the remaining 240courses, 120 patients were given gentamicin and120 received tobramycin. This report summa-rizes our findings after an analysis of these 240courses of treatment by using the pharmacoki-netic criteria for nephrotoxicity and comparesthe incidence of nephrotoxicity as determinedby pharmacokinetic assessment with the inci-dence as determined by clinical criteria.Analysis of course eliminated due to in-
sufficient pharmacokinetic data. A total of27 courses had inadequate data for analysis bythe pharnacokinetic criteria, but all 27 could beevaluated for creatinine level increases. Of these27 courses, 19 involved gentamicin and 8 in-volved tobramycin. Creatinine level increasesoccurred in 3 of 19 gentamicin courses and in 3of 8 tobramycin courses. If all six of these cre-atinine level increases had been caused by theaminoglycosides, the outcome of this study re-garding gentamicin and tobramycin nephrotox-icities would not have changed (X2 = 5.2;P < 0.02).Nephrotoxicity in 240 courses as deter-
mined by pharmacokinetic analysis. The
120 gentamicin and 120 tobramycin courses oftreatment were administered to patients of simn-ilar age, weight, initial creatinine clearance leveland incidence ofproven infection (Table 1). One-fourth of each group had positive blood cultures.Previous aminoglycoside treatments (usuallywith gentamicin) were given twice as frequentlyto the tobramycin group (P < 0.001), and moremen than women were given tobramycin (P <0.05).During treatment, the two groups had similar
initial trough concentrations, received the sameaverage doses and durations of treatment, andrequired an average of 1.1 dosage changes (usu-ally decreases) to maintain blood levels withinthe therapeutic range. Cephalosporins weregiven concurrently in slightly more tobramycincourses, and diuretics (chiefly furosemide) weregiven in more gentamicin courses (Table 1).Neither of these differences was significant.About 75% of the infections in each group
either were cured or improved by the treatment(Table 2). Approximately 25% of the patients ineach group died, usually as a consequence of anunderlying disease. However, in 11 of the pa-tients (4.5%) who died aminoglycoside-inducedrenal failure was a major contributing factor.By the end of therapy, the gentamicin-treated
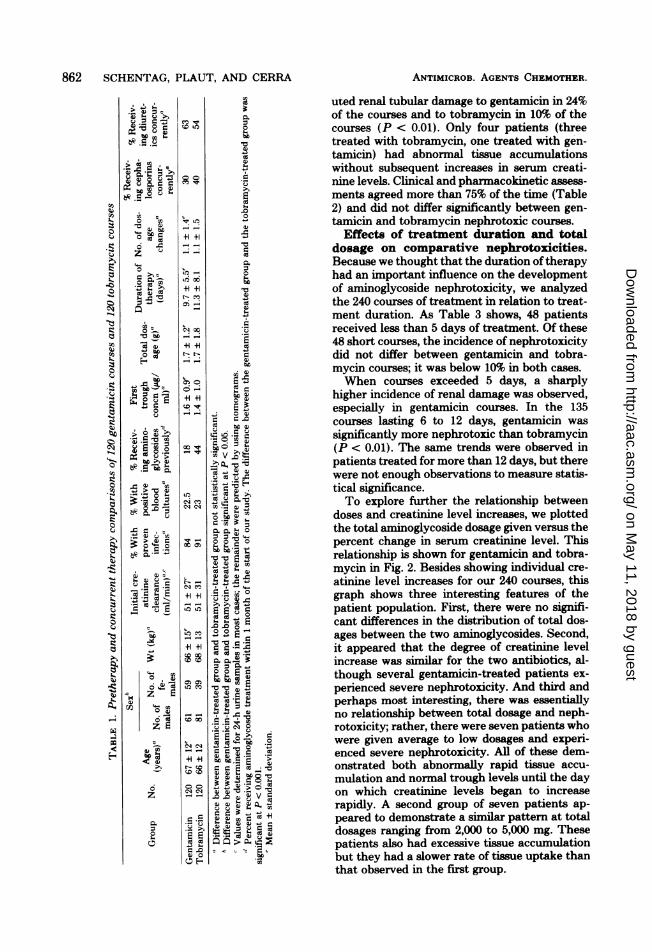
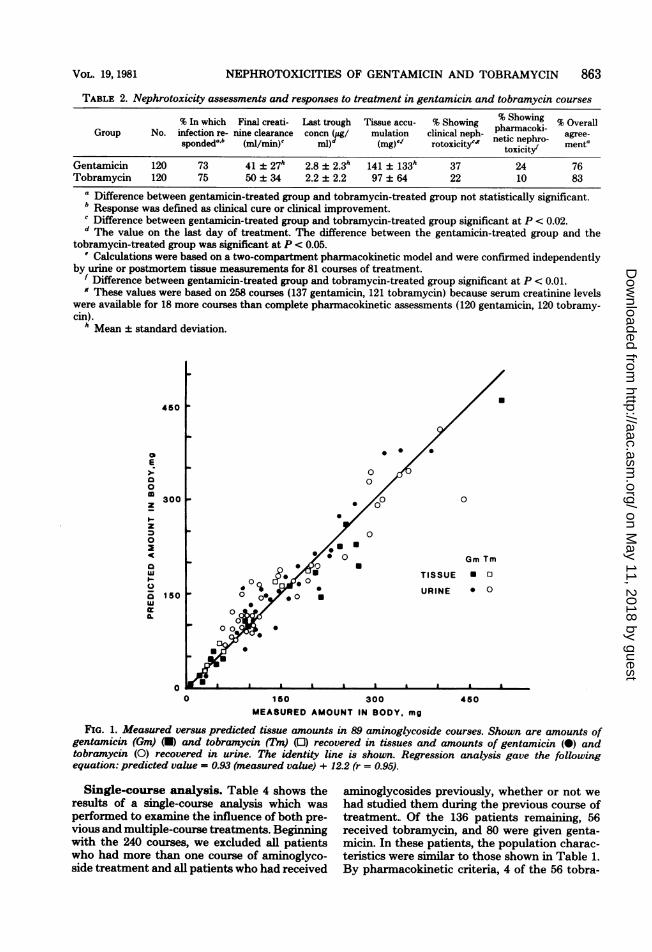
group had a greater mean decrease in creatinineclearance (P < 0.02), a higher final trough con-centration (P < 0.05), and a greater averagetissue accumulation (P < 0.01) than the tobra-mycin-treated group (Table 2). Figure 1 showsthe measured tissue accumulation values andthe values predicted in the patients for whomwe obtained consent for autopsy. This figureshows that the pharmnacokinetic model was ac-curate for both gentamicin and tobramycin overthe entire range of the observed tissue accumu-lation values. Consistent with differences be-tween gentamicin and tobramycin in tissue ac-cumulation, nephrotoxicity occurred in 24% ofthe gentamicin courses and in 10% of the tobra-mycin courses, a significant difference (P <0.01).Comparative nephrotoxicities as deter-
mined by pharmacokinetic assessment andclinical criteria. Clinical criteria identifiednephrotoxicity in 37% of the gentamicin coursesand 22% of the tobramycin courses (P < 0.02).As nearly all patients with creatinine level in-creases were defined clinically as experiencingaminoglycoside nephrotoxicity, clinical nephro-toxicity occurred more often than pharmacoki-netic nephrotoxicity, the latter requiring abnor-mal tissue accumulation and evidence of tubulardamage before creatinine level increases. Phar-macokinetic assessments, which were based pri-marily on abnormal tissue accumulation, attrib-
VOL. 19, 1981
on May 11, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
862 SCHENTAG, PLAUT, AND CERRA
uted renal tubular damage to gentamicin in 24%.uE:^ c. of the courses and to tobramycin in 10% of the:tZ8ECDig , courses (P < 0.01). Only four patients (three
* .5 .E .r treated with tobramycin, one treated with gen-0.3 tamicin) had abnormal tissue accumulations
without subsequent increases in serum creati-nine levels. Clinical and pharmacokinetic assess-ments agreed more than 75% of the time (Table2) and did not differ significantly between gen-
3,rQbDt<.tamicin and tobramycin nephrotoxic courses.oWo<=+1 +1 = Effects of treatment duration and total
ztO = __ =0dosage on comparative nephroto3icities.4. Because we thought that the duration oftherapy
Lqo>< _ ,had an important influence on the developmento..@>~ +1 +1 r of aminoglycoside nephrotoxicity, we analyzed
the 240 courses of treatment in relation to treat-ment duration. As Table 3 shows, 48 patientsreceived less than 5 days of treatment. Of these
ErX__S 48 short courses, the incidence of nephrotoxicityHEZ< > >. = did not differ between gentamicin and tobra-
mycin courses; it was below 10% in both cases.When courses exceeded 5 days, a sharply
XH5H3=i_ OL,higher incidence of renal damage was observed,especially in gentamicin courses. In the 135
>_=CZ Dcourses lasting 6 to 12 days, gentamicin wasox,,._X>g:, Qsignificantly more nephrotoxic than tobramycin
-4aEXXtsOD V;q3(P < 0.01). The same trends were observed in-oeX patients treated for more than 12 days, but there
t 0 ; .o were not enough observations to measure statis-o5 =.> r Q e ;; rEZtical significance.cq3;-Dw> n < <-P^To explore further the relationship between
t a*X : Q. doses and creatinine level increases, we plottedX..) 0. 0.U X; ° the total aminoglycoside dosage given versus the
> 44.)° a C; O 3 3 c percent change in serum creatinine level. ThisO 0
relationship is shown for gentamicin and tobra-CX * Q)@,,mycin in Fig. 2. Besides showing individual cre-
atinine level increases for our 240 courses, thisX4w "+1 +lc c g^=graph shows three interesting features of theLO LOQi< e g c | ;patient population. First, there were no signifi-> -D 0 E cant differences in the distribution of total dos-
laul¢e n w w5ages between the two aminoglycosides. Second,_+1+1 0 0 it appeared that the degree of creatinine leveli3E0 X X n i increase was similar for the two antibiotics, al-a°g , be g3 = though several gentamicin-treated patients ex-~ <:z a z r cE perienced severe nephrotoxicity. And third and
4. H < <perhaps most interesting, there was essentially_ -:w CD 0 : 5 = no relationship between total dosage and neph-X:zE .$!: q: .rotoxicity; rather, there were seven patients who4m. bo>_were given average to low dosages and experi-
F- < | _ _ ba @ rc £ enced severe nephrotoxicity. All of these dem-onstrated both abnormally rapid tissue accu-
O6 O O 3 x ._ 8 " mulation and normal trough levels until the dayz c on which creatinine levels began to increaserapidly. A second group of seven patients ap-
m..5,X3e + peared to demonstrate a similar pattern at total2 e E A i W dosages ranging from 2,000 to 5,000 mg. These03 3 < a: > a. patients also had excessive tissue accumulationD0 but they had a slower rate of tissue uptake than
that observed in the first group.
ANTIMICROB. AGENTS CHEMOTHER.
on May 11, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
NEPHROTOXICITIES OF GENTAMICIN AND TOBRAMYCIN 863
TABLE 2. Nephrotoxicity assessments and responses to treatment in gentamicin and tobramycin courses
% In which Final creati- Last trough Tissue accu- % Showing % Showing % OverallGroup No. infection re- nine clearance concn (ug/ mulation clinical neph- acoki- agree-
spondeda,b (ml/min)c MI)d (mg)'" rotoxicityc' netoxicintero/ menta
Gentamicin 120 73 41 ± 27h 2.8 ± 2.3h 141 ± 133h 37 24 76Tobramycin 120 75 50 ± 34 2.2 ± 2.2 97 ± 64 22 10 83
a Difference between gentamicin-treated group and tobramycin-treated group not statistically significant.b Response was defined as clinical cure or clinical improvement.c Difference between gentamicin-treated group and tobramycin-treated group significant at P < 0.02.d The value on the last day of treatment. The difference between the gentamicin-trea,ted group and the
tobramycin-treated group was significant at P < 0.05.' Calculations were based on a two-compartment pharmacokinetic model and were confirmed independently
by urine or postmortem tissue measurements for 81 courses of treatment.f Difference between gentamicin-treated group and tobramycin-treated group significant at P < 0.01.9 These values were based on 258 courses (137 gentamicin, 121 tobramycin) because serum creatinine levels
were available for 18 more courses than complete pharmacokinetic assessments (120 gentamicin, 120 tobramy-cin).
h Mean ± standard deviation.
450
aE
a0m 300z
z0
a
uJw
0o 150wa.
0
.
* 0*
00
0
0,l00
a
o0 U
0
Gm Tm
TISSUE U 0
URINE 0 0
160 300 450MEASURED AMOUNT IN BODY, mg
FIG. 1. Measured versus predicted tissue amounts in 89 aminoglycoside courses. Shown are amounts ofgentamicin (Gm) (U) and tobramycin (Tm) (0) recovered in tissues and amounts of gentamicin (0) andtobramycin (0) recovered in urine. The identity line is shown. Regression analysis gave the followingequation: predicted value = 0.93 (measured value) + 12.2 (r = 0.95).
Single-course analysis. Table 4 shows theresults of a single-course analysis which wasperforned to examine the influence of both pre-vious and multiple-course treatments. Beginningwith the 240 courses, we excluded all patientswho had more than one course of aminoglyco-side treatment and all patients who had received
aminoglycosides previously, whether or not wehad studied them during the previous course oftreatment.. Of the 136 patients remaining, 56received tobramycin, and 80 were given genta-micin. In these patients, the population charac-teristics were similar to those shown in Table 1.By pharmacokinetic criteria, 4 of the 56 tobra-
VOL. 19, 1981
on May 11, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

864 SCHENTAG, PLAUT, AND CERRA
TABLE 3. Comparative nephrotoxicities ofgentamicin and tobramycin in relation to duration of treatmentDuration of Total no. of courses No. of nephrotoxic courses % of nephrotoxic coursestreatment
(days) Gentamicin Tobramycin Gentamicin Tobramycin Gentamicin Tobramycin
1-5 30 18 2 1 7 66-12 61 74 18 7 29 9a13-52 29 28 9 4 31 14
a Significantly different from the gentamicin value at P < 0.01 (X2 = 7.6).
600t
550
500-
450
400 H
350
300
250
200
150
o00
50
0
-50
10(
IA
o TM
* GM
0
- 10 °
0 0~~~~~
8 < o p °@I 0Ig 0 00
0 (9%4&g- 4 0 0 0
200 500 4000 2000
Total Dosoge Given, mg
FIG. 2. Relationship between total dos(atinine level increase for tobramycin (Cpatients (0) and gentamicin (GM)-treat(0). Reference line A illustrates seven pappeared abnormally sensitive to thesehad severe renal damage. Reference line Ia population ofpatients who were less s
experienced moderate levels of renal dctotal doses of 2,00() to 5,000 mg.
TABLE 4. Comparative nephrotoxicitiescourse patients
No. withoutGroup Total toxic n
no. reactionGentamicin 80 61 ]Tobramycin 56 52 4
' Difference between gentamicin-treatetobramycin-treated group significant at I= 5.37; Yates correction applied to chi-squ
h Values in parentheses are percentageE
mycin-treated patients experienced nephrotox-icity, whereas 19 of the 80 gentamicin-treatedpatients experienced nephrotoxicity (X2 = 5.4; P< 0.02). Thus, the imbalance resulting from themore frequent previous administration of ami-noglycosides to tobramycin-treated patients didnot have a major influence on the study findings.
DISCUSSIONBecause of reliable dosing nomograms and
3 widespread dosage control-based measurementsof serum levels, fewer patients are now over-
dosed with aminoglycosides. Nevertheless,nephrotoxicity does appear to be a growing prob-lem, even despite dosage control. Perhaps ami-noglycoside nephrotoxicity appears more fre-quently because of close observation, or perhapsit was even more frequent before dosage controlwas based on blood levels. Regardless of the
0 reasons for the more frequently reported neph-; ° ° rotoxicity, it is clear that the toxicity now ob-
served clinically is different from overdose tox-
, I,,,,, ..icity and it may be related to factors such as
5000 10,000 individual sensitivity, abnormal renal uptake, or
synergy between aminoglycosides and clinicalage and cre- risk factors. Animal models based on overdoses
TM)-treated and previous human comparative trials in which
ted patients doses were poorly controlled have limited value
atients who either in differentiating comparative nephrotox-drugs and icities or in identifying patients at risk. The
B illustrates appropriate model is critically ill patients.,ensitive but Once blood levels are controlled within the
zmage after therapeutic range, the nephrotoxicities of two
compounds can be studied in a double-blindrandomized fashion by using a clearly definedendpoint as the criterion for differentiation. For
in single- the study of aminoglycosides, serum creatinine
level increases have been the criterion used forNo. with a long time, yet this definition of nephrotoxicityephrotoxic is potentially too nonspecific to reliably identifyreaction' tubular damage in situations where concurrent
19 (31)b renal insults are so frequent. Furthermore, the
4 (8) double-blind trial design precluded any analysis
d group and of data until the final stages and because of this
(X2 did not allow a constant search for new mecha-
uare table). nisms or better criteria for nephrotoxicity. Our
s. investigative plan permitted intensive analysis
r-
EST
cn
c0
a-
ANTIMICROB. AGENTS CHEMOTHER.
10
on May 11, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

NEPHROTOXICITIES OF GENTAMICIN AND TOBRAMYCIN 865
of urine in search of new parameters and thedevelopment and evaluation of new and poten-tially more specific criteria for identifying thesite of aminoglycoside damage. Simultaneousyet blind clinical analyses allowed us to compareany new criterion with standard clinical assess-ments. In the clinical analysis, we attributedessentially all serum creatinine level increase toaminoglycoside nephrotoxicity, fully realizingthe difficulties inherent in using a nonspecifictest to judge toxicity in critically ill patients.The advantage of this approach to our clinicaldefinition was a low dropout rate, whereas thedisadvantage was a high rate of nephrotoxicity.
In our pharmacokinetic analysis, the quanti-tative nature of the criteria used and the factthat they were supported in 89 cases by eithertissue analysis or urine recovery lend validity tothe use of these criteria in nonblind fashion.Tissue accumulation is a highly specific criterionas only 4 of our patients experienced abnormalaminoglycoside tissue accumulation without a
subsequent increase in serum creatinine levels.Finally, the results ofa double-blind randomizedcomparative trial in which nephrotoxicity wasdefined by serum creatinine level increases alsoagreed with our pharmacokinetic assessmentthat gentamicin was more nephrotoxic than to-bramycin (17). The two studies were compli-mentary, as our findings support the use of se-rum creatinine levels in less acutely ill patients,such as those employed in this double-blind trial,whereas the conclusion that gentamicin is morenephrotoxic than tobramycin in a study designedto be free of interpretive bias lends further sup-port to the utility of the pharnacokinetic as-sessment of nephrotoxicity in severely ill pa-tients.
In a group of critically ill patients, the use ofthe pharmacokinetic criteria lowers the overallincidence of nephrotoxicity attributable to bothgentamicin and tobramycin, perhaps becausethese criteria more reliably distinguish the ne-phrotoxic potential of these agents in a mannerconsistent with the known pathogenesis of ami-noglycoside renal damage. However, the abso-lute specificity of the pharmacokinetic criteriacan only be determined when there is a group ofinfected patients at equal risk not given amino-glycosides, an impossible study design until non-nephrotoxic alternatives to aminoglycosides be-come available.
In our 240 courses of treatment, there can beno doubt that older age, concurrent disease,critically ill status, and concurrent multiple-drugtreatments combined to produce an extremelyhigh overall incidence of renal damage. Our pop-ulation was one of the most seriously ill popu-
lations studied to date (average mortality, 25%),yet these patients were representative of thepatients who most often require these agentsand therefore deserved study. We found thatgentamicin-treated and tobramycin-treated pa-tients were at equal risk for renal damage. Therewere no clinical parameters unbalanced againstthe gentamicin-treated group, and thus we couldnot explain the greater occurrence of gentamicinnephrotoxicity on clinical grounds. On the con-trary, the clinical differences which we did findbetween the gentamicin-treated and tobramy-cin-treated groups uniformly favored increasedtobramycin nephrotoxicity. For example, the to-bramycin-treated group had significantly moremales, who are perhaps at greater risk of renaldamage (R. A. Parker, W. M. Bennett, C. E.Plamp, D. C. Houghton, D. N. Gilbert, and G.A. Porter, Program Abstr. Int. Cong. Chemo-ther. 11th, Boston, Mass., abstr. no. 938, 1979).The tobramycin-treated group showed a trendtoward longer duration of treatment. Finally,almost twice as many gentamicin courses wereless than 5 days long, again favoring increasedtobramycin nephrotoxicity.Although there were no differences in dose or
blood levels, the predominant pharmacokineticdifference between the gentamicin-treated andtobramycin-treated groups was an increased tis-sue accumulation in the gentamicin-treatedgroup. Since our prospectively studied genta-micin-treated and tobramycin-treated groupsdid not differ in base-line risk factors or in riskfactors developing during the treatment period,we propose that differences in the rates of renaldamage resulted from differences in the tissueaccumulation-related nephrotoxic potentials ofgentamicin and tobramycin.
ACKNOWLEDGMENTISWe thank G. Calleri, E. DeGlopper, J. Acquard, S. Przy-
wara, D. Chiarnonte, and Ann Krol for assistance throughoutthis study. The attending, nursing, and house staffs of MillardFillmore and Buffalo General Hospitals referred patients andassisted with sample collection.
This work was supported in part by Public Health Servicegrant GM20852 from the National Institute of General Medi-cal Sciences and in part by grants from Eli Lilly & Co., BristolLaboratories, and the Schering Corp.
LITERATURE CITED1. Barza, M., and M. Lauermann. 1978. Why monitor
serum levels of gentamicin? Clin. Pharmacokinet. 3:202-215.
2. Fee, W. E. 1980. Aminoglycoside ototoxicity in the hu-man. Laryngoscope 90:(Suppl. 24):1-19.
3. Gilbert, D. N., C. Plamp, P. Starr, W. M. Bennett, D.C. Houghton, and G. Porter. 1978. Comparativenephrotoxicity of gentamicin and tobramycin in rats.Antimicrob. Agents Chemother. 13:34-40.
4. Hewitt, W. L 1974. Gentamicin: Toxicity in perspective.Postgrad. Med. 50S:55-59.
VOL. 19, 1981
on May 11, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

866 SCHENTAG, PLAUT, AND CERRA
5. Luft, F. C., M. N. Yum, and S. A. Kleit. 1976. Compar-ative nephrotoxicities of netilmicin and gentamicin inrats. Antimicrob. Agents Chemother. 10:845-849.
6. Ormsby, A. M., R. A. Parker, C. E. Plamp, P. Stevens,D. C. Houghton, D. N. Gilbert and W. M. Bennett.1979. Comparison of the nephrotoxic potential of gen-tamicin, tobramycin and netilmicin in the rat. Curr.Ther. Res. 25:335-343.
7. Plaut, M. E., J. J. Schentag, and W. J. Jusko. 1979.Nephrotoxicity with gentamicin or tobramycin. Lancetii:526-527.
8. Plaut, M. E., J. J. Schentag, and W. J. Jusko. 1979.Aminoglycoside nephrotoxicity: comparative asaess-ment in critically ill patients. J. Med. (Cincinnati) 10:257-266.
9. Schentag, J. J., T. J. Cumbo, W. J. Jusko, and IL E.Plaut. 1978. Gentamicin tisaue accumulation and ne-phrotoxic reactions. J. Am. Med. Assoc. 240:2067-2069.
10. Schentag, J. J., F. M. Gengo, M. E. Plaut, D. Danner,A. Mangione, and W. J. Jusko. 1979. Urinary castsas an indicator of renal tubular damage in patientsreceiving aminoglycosides. Antimicrob. Agents Chem-other. 16:468-474.
11. Schentag, J. J., and W. J. Jusko. 1977. Renal clearanceand tissue accumulation of gentamicin. Clin. Pharma-col. Ther. 22:364-370.
12. Schentag, J. J., W. J. Jusko, J. W. Vance, T. J.Cumbo, E. Abrutyn, M. Delattre, and L. M. Ger-bracht. 1977. Gentamicin disposition and tissue accu-mulation on multiple dosing. J. Pharmacokinet. Bio-
ANTIMICROB. AGENTS CHEMOTHER.
pharm. 5:559-577.13. Schentag, J. J., G. L y, M. E. Plaut, W. J.
Jusko, and T. J. Cumbo. 1978. Comparative tissueaccumulation of gentamicin and tobramycin in patients.J. Antimicrob. Chemother. 48:23-30.
14. Schentag, J. J., and ML E. Plaut. 1980. Pattens ofurinary ,2-microglobulin excretion by patients treatedwith aminoglycosides. Kidney Int. 17:654-661.
15. Schentag, J. J., M. E. Plaut, F. B. Cerra, P. B. Wels,P. Walczak, and R. J. Buckley. 1979. Aminoglycosidenephrotoxicity in critically ill surgical patients. J. Surg.Res. 26:270-279.
16. Smith, C. R., K. L Baughman, C. Q. Edwards, J. F.Rogers, and P. S. Lietman. 1977. Controlled compar-ison of amikacin and gentamicin. N. Engl. J. Med. 296:350-353.
17. Smith, C. R., J. J. Lipsky, 0.L Iaskin, D. B. Hellman,E. D. Mellits, J. Longtreth, and P. S. Lietman.1980. Double blind comparison of the nephrotoxicityand auditory toxicity of gentamicin and tobramycin. N.Engl. J. Med. 302:1106-1109.
18. Smith, C. R., R. R. MaxwelL C. Q. Edwards, J. F.Rogers, and P. S. Lletman. 1978. Nephrotoxicityinduced by gentamicin and amikacin. Johns HopkinsMed. J. 142:85-90.
19. Wade, J. C., C. R. Smith, B. G. Petty, J. J. LUpaky, G.Conrad, J. Ellner, and P. S. lietmnan. 1978. Cepha-lothin plus an aminoglycoside is more nephrotoxic thanmethicillin plus an aminoglycoside. Lancet ii:604-606.
on May 11, 2018 by guest
http://aac.asm.org/
Dow
nloaded from