complications and management of mucopolysaccharidosis
TRANSCRIPT


Complications and management of Mucopolysaccharidosis
F.Tabatabaei Pediatric endocrinologist

• Until 21 century, supportive treatment • Bone marrow transplantation • Specific enzyme replacement therapy (ERT)

History of ERT
• Concept of ERT introduced in 1964 by Christian de Duve
• At University of Alberta by Mark J. Poznansky and Damyanti Bhardwaj, ERT developed on rats
Wikipedia

supportive treatment

Prevention and management of complications Symptomatic and palliative treatment with multidisciplinary team
Mucopolysaccharidosis I, II, and VI: brief review and guidelines for treatment. Genet. Mol. Biol. vol.33 no.4 São Paulo 2010 Epub Nov 12, 2010

General considerations • Paediatric subspecialties: Cardiology Anaesthesia Orthopaedics ENT Ophthalmology neurosurgery • paramedical groups: Physiotherapy Occupational therapy Audiology Speech therapy Psychology JE Wraith. http://adc.bmj.com/ on August 3, 2016 - Published by group.bmj.com
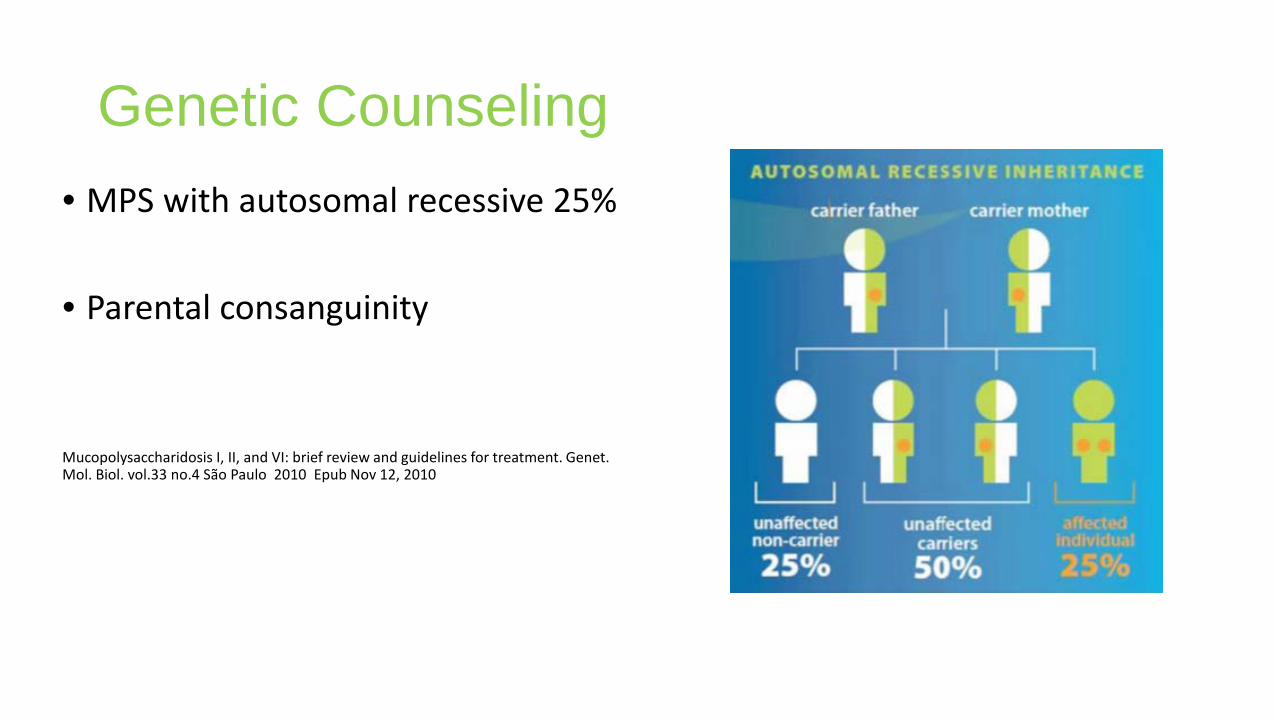
Genetic Counseling • MPS with autosomal recessive 25% • Parental consanguinity
Mucopolysaccharidosis I, II, and VI: brief review and guidelines for treatment. Genet. Mol. Biol. vol.33 no.4 São Paulo 2010 Epub Nov 12, 2010

Genetic Counseling
• MPS II, X-linked, identification of female
carriers very important • Female carrier has 25% risk of an affected
child (50% risk for a male child)
Mucopolysaccharidosis I, II, and VI: brief review and guidelines for treatment. Genet. Mol. Biol. vol.33 no.4 São Paulo 2010 Epub Nov 12, 2010

Prenatal Diagnosis • In first or second trimester Chorionic villus biopsy Amniotic fluid collection • In high gestational age umbilical cord blood cell • Level of enzyme activity in cells • With known mutations in family, diagnosis quickly obtained Mucopolysaccharidosis I, II, and VI: brief review and guidelines for treatment. Genet. Mol. Biol. vol.33 no.4 São Paulo 2010 Epub Nov 12, 2010

COMPLICATIONS MANAGEMENT

RESPIRATORY COMPLICATIONS
• Result from: Airway obstruction Excessive secretions Skeletal restriction Organomegaly Frequent infections Neurologic compromise Up to date 2016
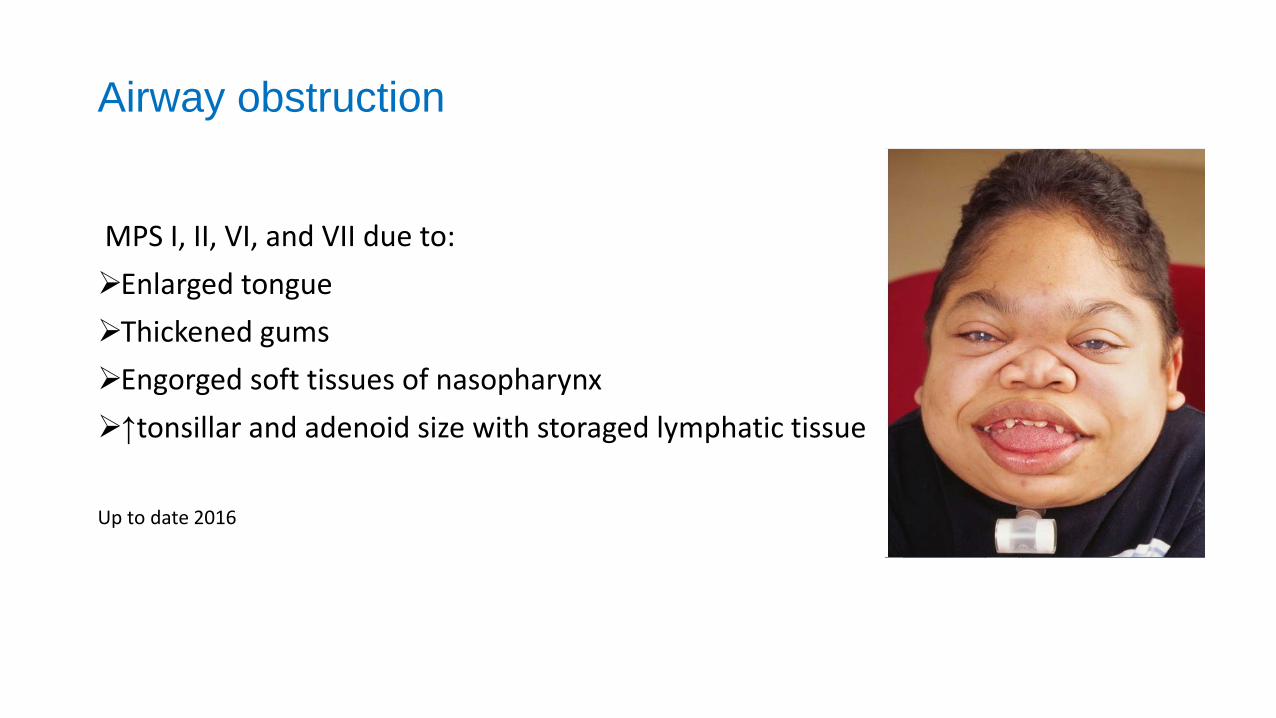
Airway obstruction
MPS I, II, VI, and VII due to: Enlarged tongue Thickened gums Engorged soft tissues of nasopharynx ↑tonsillar and adenoid size with storaged lymphatic tissue
Up to date 2016

Interventions Maintaining a stable airway Removal of tonsils and adenoids Continuous Positive Airway Pressure (CPAP) at night Younger patients adapt better to CPAP Facial dysmorphism difficult to fit of masks
Supplemental oxygen at low flow rates during sleep Oxygen with caution to avoid suppressing hypoxic respiratory drive Up to date 2016

Interventions
Tracheotomy: Severe hypoxemia Hypercapnia Signs of right heart failure Sleep disturbance Severe sleep apnea that not improve with CPAP Critical airway stenosis
Up to date 2016

Central apnea from cord compression
• MPS IV A and IV B: Atlantoaxial instability Odontoid dysplasia • Prophylactic cervical fusion in MPS IV and other patients with cervical
instability
Up to date 2016

Anesthesia • Difficulty in endotracheal intubation : I. Airway obstruction II. Excessive secretions III. Large tongue IV. Abnormal airway anatomy V. Spinal cord injury by extension of neck due to instability of cervical
spine Up to date 2016
Anesthesia management
• Endotracheal tube smaller than patient's age or weight • Intubation with adequate visualization • Extubation very difficult, and glucocorticoids ↓airway edema • If unsuccessfully extubated, tracheotomy must perform Up to date 2016

Sinopulmonary infections Frequent or chronic pulmonary infections Otitis media Sinusitis
Up to date 2016

Mechanism for increased infection
1. Obstruction of Eustachian tubes and sinus ostia 2. Thick and copious secretions →airway obstruction 3. Abnormal immune function 4. Decrease T cell proliferative and antibody production Minor respiratory infections progress to pneumonia with consolidation
Up to date 2016

Sinopulmonary infections management • Antimicrobial management similar to without MPS • Recovery time longer for MPS • Bronchodilators need to treat reactive airway disease • Otitis media difficult to treat and tympanostomy tubes require • Tube placement should consider more readily than other • Preventive influenza vaccine + standard immunizations • Prophylactic antibiotic use, especially winter • Nebulized gentamicin for prophylaxis in patients with tracheotomy Up to date 2016

CARDIAC COMPLICATIONS
Underlying MPS disorder Cardiomyopathy rarely in Hurler and MPS VI Complication of severe pulmonary disease and chronic hypoxemia
Up to date 2016

Valvular disease
Progressive thickening of mitral and aortic valve in types I, II, VI, and less in MPS III A to D Tricuspid and pulmonic valve regurgitation occur and exacerbate by pulmonary HTN Up to date 2016

Management of valvular disease
• Severely affected→ valve replacement
• In valvular insufficiency, HTN and vascular disease should treat • Beneficial prophylactic afterload reduction in moderate regurgitation and without
HTN→ uncertain
Up to date 2016
Vascular disease
Storage cells accumulate in walls of artery →impaired flow and ischemia Unexpected in young children Narrowing of abd aorta→HTN and poor perfusion of lower extremities Renal, mesenteric, and iliac arteries Narrowing can detect by arteriography, ultrasound, and MRI Up to date 2016

Pulmonary hypertension Due to: a. Chronic hypoxemia due to airway obstruction b. Pulmonary disease Therapy : 1. Maintaining a secure airway 2. Avoiding hypoxemia, especially during night
Up to date 2016

SKELETAL AND CONNECTIVE TISSUE COMPLICATIONS
Storage material in connective tissues →abnormalities in bone, joints, ligaments i. Growth failure ii. Dysmorphism iii. Impair mobility iv. Pain
Up to date 2016

Dysostosis multiplex • MPS I, II, IV, VI, and VII, less extensive in MPS III
• Thickened hyperostotic calvarium, with craniosynostosis; a "J" or "shoe-shaped"
sella turcica • Odontoid dysplasia • Ovoid and beaked vertebrae • "oar-shaped" ribs with narrow roots and broadened ends • Tilting of radial and ulnar epiphyses • Long bones with irregular, curved, and expanded diaphyses • Pointed and irregular metacarpals • Irregular or dysplastic femoral capital epiphyses; and a dysplastic pelvis
Up to date 2016
Management of skeletal complications
Dysplastic femoral capital epiphyses
• Deficient ossification of superior acetabulum cause dislocation of hip and erosions of femoral neck
• Joint replacement surgery is possible using a standard prosthesis
Up to date 2016

Odontoid hypoplasia
• In MPS IV A and IV B and in severe forms of MPS I and VII • Due to inadequate ossification • Lead to atlantoaxial instability→C1-C2 subluxation and high spinal
cord compression • MPS IV A and IV B should prophylactic cervical vertebral fusion • Other MPS should evaluate in flexion and extension radiographs If cervical instability is present, fusion should perform Up to date 2016
Spine abnormalities
• Abnormalities of vertebral body occur frequently and can result in spinal instability and kyphoscoliosis
Up to date 2016

gibbus deformity of lumbar spine
• In Hurler • Gibbus deformity is a short-segment thoracolumbar kyphosis
resulting in sharp angulation. • Resulting in a beaked appearance on lateral radiographs • Causes of gibbus formation : Incomplete ossification of abnormal vertebrae Poor truncal tone Anterior disc herniation Weight bearing Up to date 2016

Spondylolisthesis • forward slippage of L5 over S1 • MPS I • Spinal fusion surgery require to stabilize spine • MPS do not heal well and often have complications from surgical procedures
Up to date 2016
Spinal fusion surgery
• Grafts with membranous (skull) rather than endochondral bone • Fusion surgery carefully consider and perform only when absolutely necessary • Often fails and must repeat due to severe osteopenia lead to failure of fixation
Up to date 2016

Pachymeningitis cervicalis • MPS VI, MPS I, II, and VII • Progressive thickening of meninges around cervical spinal cord by MPS storage • Form tight sleeve around spinal cord→ ↓flow of CSF and compress cervical cord • Fatigue in legs and gradually decreased movement and sedentary activities • weakness or sensory loss • Breathing or bowel and bladder control affected
Up to date 2016

Management of Pachymeningitis cervicalis
• Is difficult • Surgical treatment • High surgical and anesthesia risks Up to date 2016
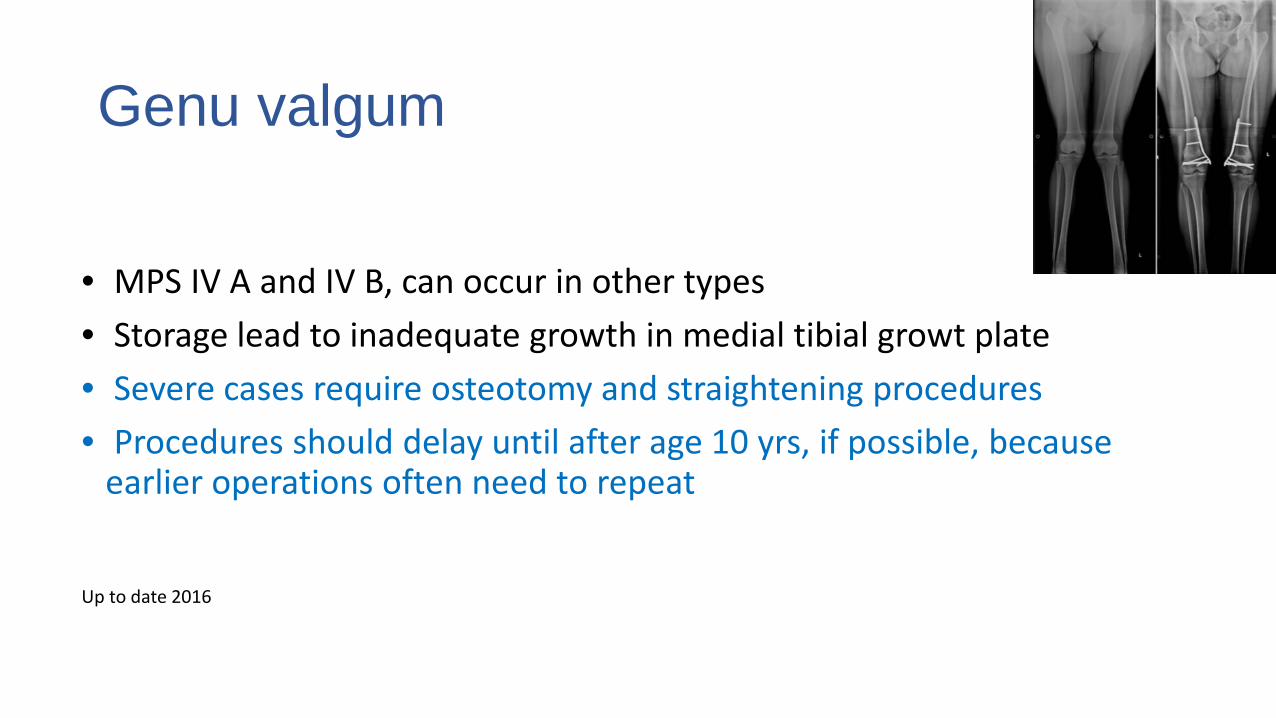
Genu valgum
• MPS IV A and IV B, can occur in other types • Storage lead to inadequate growth in medial tibial growt plate • Severe cases require osteotomy and straightening procedures • Procedures should delay until after age 10 yrs, if possible, because
earlier operations often need to repeat
Up to date 2016

Short stature
• Extensive skeletal abnormalities impair growth • Growth hormone resistance may play a role in MPS I • Severe MPS I may accelerated growth in first year, height <fifth percentile • Less severely may reach normal or near-normal heights • MPS II have accelerated growth first three yrs of life, but subsequently ↓ GV • ERT may improve growth in MPS II, particularly if therapy start <10 yrs Up to date 2016

Joint stiffness • Associated with pain on movement in nearly all MPS • Etiology : I. Inflammatory changes II. Engorgement of synovial and other connective tissues of joint III. Abnormalities of cartilage and epiphyseal bone • Pain and decreased movement lead to contractures • Physical therapy can help maintain function • Wheelchairs often need for mobility due to pain and/or limited endurance • Animal studies possible therapeutic role for TNF-α antagonists Up to date 2016

Ligamentous laxity
• Often in MPS IV A and IV B • Lysosomal storage → joints to be stiff • Mucopolysaccharide accumulation in ligaments can lead to
laxity of joints • Ligamentous laxity contributes to atlantoaxial instability and
kyphoscoliosis.
Up to date 2016
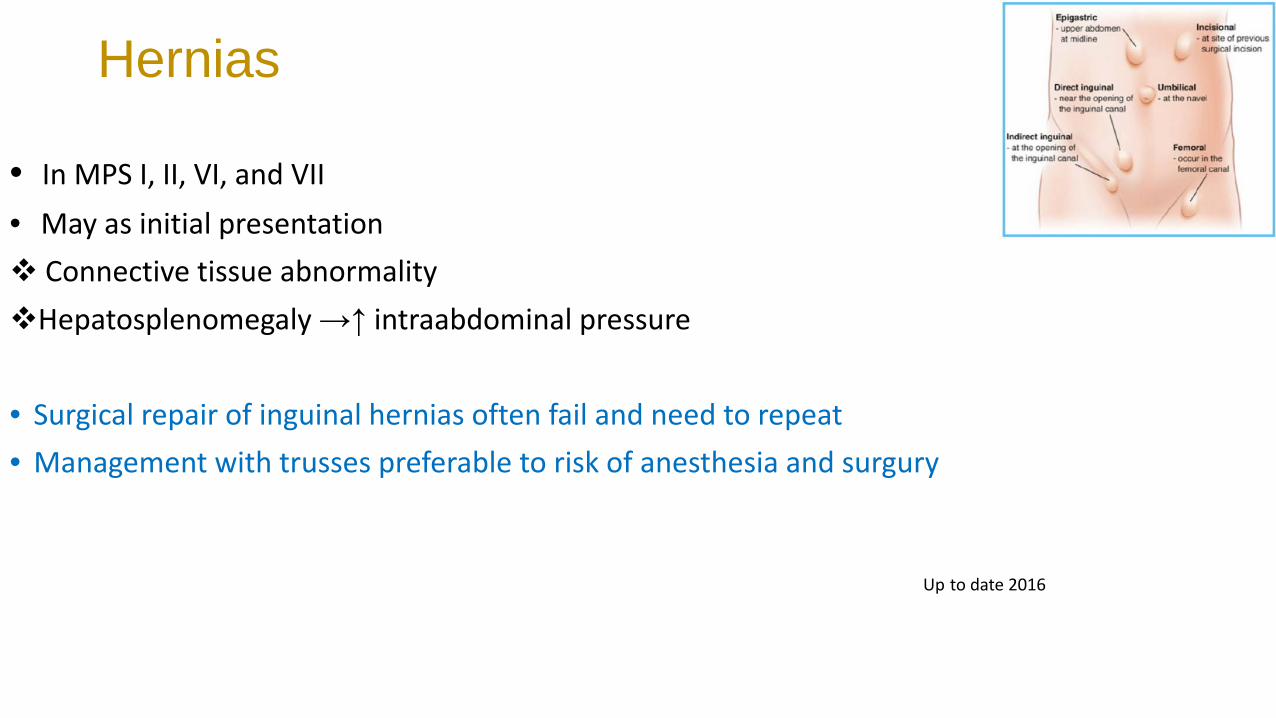
Hernias
• In MPS I, II, VI, and VII • May as initial presentation Connective tissue abnormality Hepatosplenomegaly →↑ intraabdominal pressure • Surgical repair of inguinal hernias often fail and need to repeat • Management with trusses preferable to risk of anesthesia and surgury
Up to date 2016

NEUROLOGIC COMPLICATIONS
• Result from storage in cells: Brain Supporting structures (meninges or spinal column) Sensory organs (eye)
Up to date 2016

NEUROLOGIC COMPLICATIONS
• ↑ICP →significant ventriculomegaly • Imaging findings may not reflect neurologic status
Up to date 2016

Hydrocephalus
• MPS I, II, III, VI, and VII Acute ↑ICP→ severe headaches, visual disturbance, altered mental
status, and rapidly progressive developmental decline Process may insidious and without typical signs • Papilledema not a reliable indicator and is often not present in ↑ ICP • Diagnosis ↑ICP confirm by LP • Manage by placement of a ventriculoperitoneal shunt
Up to date 2016

Developmental delay and neurologic decline • In severe forms of MPS I, II, III, and VII • MPS IV and VI →normal intellectual development • Begin to walk and speak before developmental plateau • Then decline slowly • Average IQ is 50 by 3 to 4 yrs
Up to date 2016
Abnormal behavior
• Hurler →pleasant, good-natured children with excellent behavior→ but become unresponsive in final stages
Up to date 2016
Abnormal behavior
• In severe Hunter and Sanfilippo, developmental delay at 2 to 6 yrs • Hyperactive and aggressive behavior • Short attention, not respond to instructions, and no sense of danger • Aggressive behavior improve with age • Overall function progressively decline→ reach unresponsive in early yrs
Up to date 2016
Abnormal behavior
• MPS II →high-pressure hydrocephalus→ severe headach that may worsen behavior problems
Up to date 2016

Management of abnormal behavior • Ensure home environment is safe • Medications have been limited by their side effects • Medications : Neuroleptics (eg, chlorpromazine, thioridazine, haloperidol), may excessive sedation Benzodiazepines, may increase secretions and respiratory compromise, bulbar palsy,
and ↓ swallowing Tricyclic antidepressants • Fluoxetine and carbamazepine • Fluoxetine avoid in patients with seizures • Methylphenidate is usually not helpful Up to date 2016
Seizures
• Hunter and Sanfilippo , rarely in other MPS • EEG → irregular slow wave activity and typical epileptiform discharge • Seizures manage with anticonvulsant similar to patients without MPS
Up to date 2016

Sleep disturbance
• Common, especially in Sanfilippo
Up to date 2016
• A padded bedroom for keep child and avoid injury during night • Restraints are generally not effective • Medications: melatonin or sedatives • Melatonin successful in 75% within 3 to 4 days • Start dose 2 to 3 mg→↑ after 1 to 2 weeks to 4 to 6 mg (max 10 mg) • Melatonin with regular sleep time and a darkened bedroom • Benzodiazepines or chloral hydrate may be tried
Up to date 2016
Carpal tunnel syndrome
• Very common in MPS • From bone disease and soft tissue storage • Pain, paresthesia, or weakness • Thenar atrophy, decreased sweating, claw hand deformity • Evaluate with nerve conduction study Up to date 2016

Treatment of Carpal tunnel syndrome
• Similar to patients without MPS • Functional improvement with carpal tunnel release • Accumulation of storage material in soft tissues can lead to recurrence Up to date 2016

Diarrhea
• MPS II and III →recurrent or chronic diarrhea • Mechanism → MPS storage in neurons of myenteric plexus→ abnormal motility • Improve with medications that decrease bowel motility (loperamide)
Up to date 2016
OPHTHALMOLOGIC COMPLICATIONS
Corneal cloudingis (uncommon in MPS II) Glaucoma Optic neuropathy Degeneration of retina • Present at time of initial diagnosis
Up to date 2016

SPECIFIC THERAPIES
A. Hematopoietic stem cell transplantation (HCT) B. Enzyme replacement
Up to date 2016

HCT • Successfully in MPS I and under investigation for MPS II and VI • Replacement of enzyme-deficient hematopoietic cells with donor-derived
enzyme-competent cells • Donor cell: bone marrow, peripheral blood stem cells, or umbilical cord blood • Donor: HLA-matched family or HLA-matched unrelated donor • Chemotherapy drug to recipient: ablate host bone marrow and immune system
Up to date 2016
• HCT routinely offered only to Hurler under approximately two yrs • Improve clinical outcome of milder MPS I and II, and MPS VI and VII • Not prevent CNS decline in severe MPS II • MPS III A to D usually do not benefit and may worsen after procedure • HCT not correct bony abnormality in MPS IV A and IV B or MPS I
Up to date 2016

HCT
• With successful engraftment : ↓Hepatosplenomegaly ↑joint mobility ↓airway obstruction Improves cardiac function ↓ CSF pressure Improves or stabilizes hearing Stabilize mental regression, in younger patients Up to date 2016

• Major complications of HSCT 1. Infection 2. Graft-versus-host disease
Wikipedia

ERT approve for MPS I, II, IVA, VI Clinical trials are underway for MPS VII
Up to date 2016

MPS I
• Recombinant human alpha-L-iduronidase (laronidase) • Brand Name: Aldurazyme • IV: 0.58 mg/kg/dose once weekly • Before serious complications • Intrathecal for spinal cord compress in MPS I Up to date 2016
Weekly IV laronidase • Improved: Forced vital capacity (FVC) Walking distance Improved sleep apnea and shoulder flexion Increased height and weight Improved airway size U GAG decreased within first 12 weeks and liver volume within first
year Corneal clouding did not change Infusion reactions generally mild and decreased after six months Up to date 2016

MPS II
• Recombinant human iduronate sulfatase (idursulfase) • Idursulfase (0.5 mg/kg) weekly • ERT is not predicted to cross BBB • Somatic improvements may occur, but cognitive benefits have not seen • ERT started in newly MPS II, not end stage disease
Up to date 2016

MPS II • ERT for at least two years improvement in somatic manifestations : Skeletal disease Joint range of motion Liver/spleen size Respiratory infections Cardiac disease Diarrhea Skin/hair texture Disease-related hospitalizations Up to date 2016
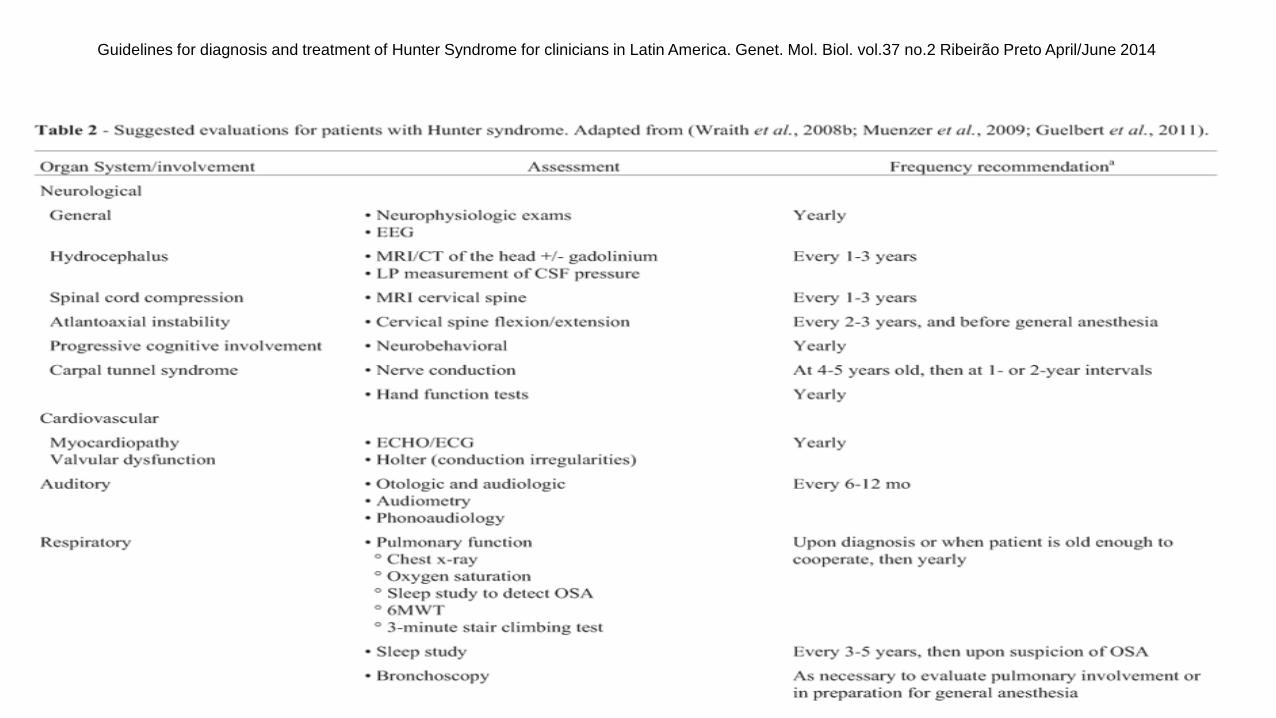
Guidelines for diagnosis and treatment of Hunter Syndrome for clinicians in Latin America. Genet. Mol. Biol. vol.37 no.2 Ribeirão Preto April/June 2014

Guidelines for diagnosis and treatment of Hunter Syndrome for clinicians in Latin America. Genet. Mol. Biol. vol.37 no.2 Ribeirão Preto April/June 2014
MPS IV
• Elosulfase alfa (recombinant human N-acetylgalactosamine-6-sulfate sulfatase) FDA approve for MPS IVA
• IV: 1 mg/kg/dose once weekly • 8 % had anaphylactic reaction • Premedication with antihistamine ± antipyretic recommend Up to date 2016

MPS VI
• Galsulfase (recombinant human N-acetylgalactosamine-4-sulfatase) FDA approve for MPS VI
• 1 mg/kg/dose is administered once weekly • ERT for MPS VI ↓ UGAG and improves patient function and survival
Up to date 2016

Gene therapy
• Gene therapy be associated with benefits in murine models of MPS • However, human studies have not been performed.
Up to date 2016

