congenital lobar emphysema - thorax.bmj.com · thorax(1959), 14, 254. congenital lobar emphysema by...
TRANSCRIPT
Thorax (1959), 14, 254.
CONGENITAL LOBAR EMPHYSEMABY
P. G. I. STOVINFrom the Bernhard Baron Institute of Pathology, The London Hospital
(RECEIVED FOR PUBLICATION MARCH 31, 1959)
The term congenital lobar emphysema wasused by Robertson and James (1951) to denoteinfantile emphysema when pulmonary infectionor intrabronchial foreign bodies are absent.Although in most instances only one lobe isaffected, a few patients have emphysema of morethan one lobe or subsequently developemphysema of a second lobe (Kernan, 1944;Ehrenhaft and Taber, 1953; Sloan, 1953; Potts,Holinger and Rosenblum, 1954; Morse andGladding, 1955; Holzel, Bennett, and Vaughan,1956; Nelson, 1957; Contro, Miller, White, andPotts, 1958a and b; Sherman, 1959). However,as these multilobar cases are exceptional and asmany authors have used the term congenital lobaremphysema, its adoption for this relativelyspecific clinical condition seems advisable.
Typical cases clinically exhibit either remittentor progressive dyspnoea and cyanosis, associatedwith severe unilateral emphysema and displace-ment of the mediastinum to the opposite side.Wheezing chest sounds are frequent and thetemperature may be elevated. In several cases thecondition of the infant is so critical that urgentsurgical thoracic decompression by lobectomy isnecessary. The symptoms often arise at orshortly after birth; their onset is rarely delayedbeyond the sixth month.
In the present paper one case is described witha method of histological investigation which wasfound to be useful in elucidating its basicpathology.
CASE REPORTA premature male infant (birth weight 3 lb. 13 oz.,
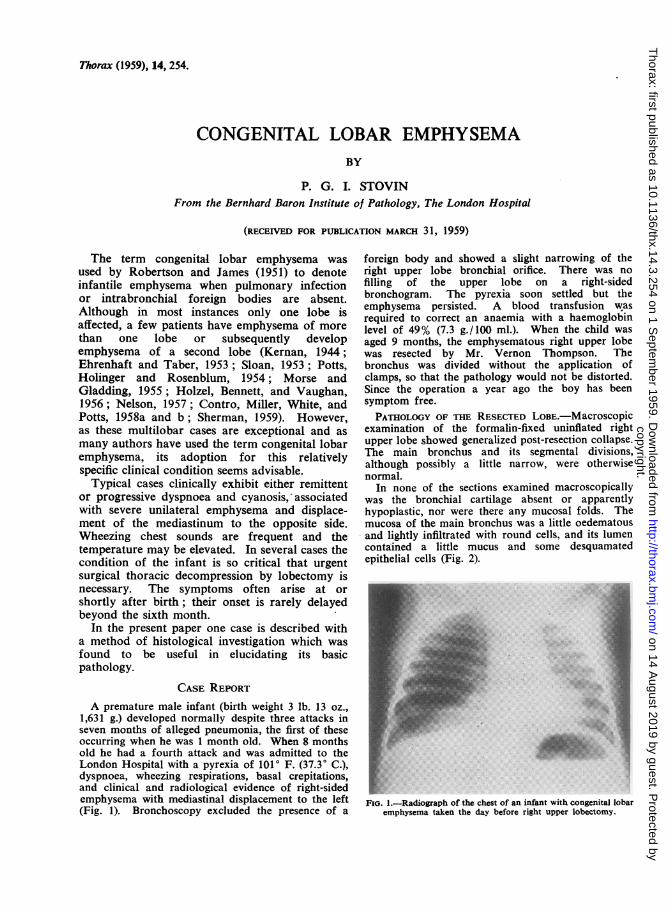
1,631 g.) developed normally despite three attacks inseven months of alleged pneumonia, the first of theseoccurring when he was 1 month old. When 8 monthsold he had a fourth attack and was admitted to theLondon Hospital with a pyrexia of 1010 F. (37.3' C.),dyspnoea, wheezing respirations, basal crepitations,and clinical and radiological evidence of right-sidedemphysema with mediastinal displacement to the left(Fig. 1). Bronchoscopy excluded the presence of a
foreign body and showed a slight narrowing of theright upper lobe bronchial orifice. There was nofilling of the upper lobe on a right-sidedbronchogram. The pyrexia soon settled but theemphysema persisted. A blood transfusion wasrequired to correct an anaemia with a haemoglobinlevel of 49% (7.3 g./100 ml.). When the child wasaged 9 months, the emphysematous right upper lobewas resected by Mr. Vernon Thompson. Thebronchus was divided without the application ofclamps, so that the pathology would not be distorted.Since the operation a year ago the boy has beensymptom free.PATHOLOGY OF THE RESECTED LOBE.-Macroscopic
examination of the formalin-fixed uninflated rightupper lobe showed generalized post-resection collapse.The main bronchus and its segmental divisions,although possibly a little narrow, were otherwisenormal.
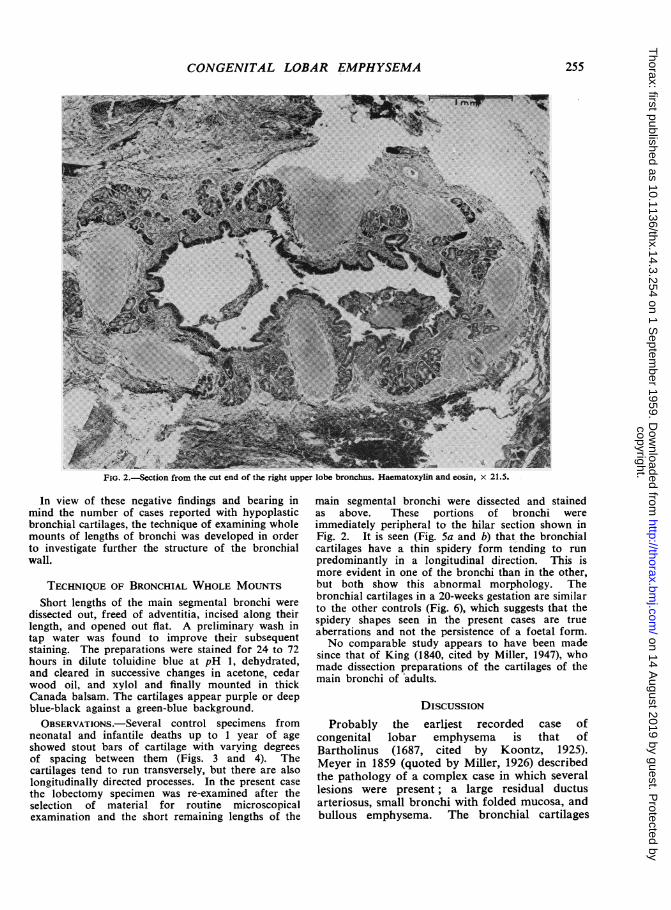
In none of the sections examined macroscopicallywas the bronchial cartilage absent or apparentlyhypoplastic, nor were there any mucosal folds. Themucosa of the main bronchus was a little oedematousand lightly infiltrated with round cells, and its lumencontained a little mucus and some desquamatedepithelial cells (Fig. 2).
FIG. 1.-Radiograph of the chest of an infant with congenital lobaremphysema taken the day before right upper lobectomy.
-i
copyright. on 14 A
ugust 2019 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.14.3.254 on 1 Septem
ber 1959. Dow
nloaded from
CONGENITAL LOBAR EMPHYSEMA;,,SW*k.ji w,t
FIG. 2.-Section from the cut end of the right upper lobe bronchus. Haematoxylin and eosin, x 21.5.
In view of these negative findings and bearing inmind the number of cases reported with hypoplasticbronchial cartilages, the technique of examining wholemounts of lengths of bronchi was developed in orderto investigate further the structure of the bronchialwall.
TECHNIQUE OF BRONCHIAL WHOLE MOUNTSShort lengths of the main segmental bronchi were
dissected out, freed of adventitia, incised along theirlength, and opened out flat. A preliminary wash intap water was found to improve their subsequentstaining. The preparations were stained for 24 to 72hours in dilute toluidine blue at pH 1, dehydrated,and cleared in successive changes in acetone, cedarwood oil, and xylol and finally mounted in thickCanada balsam. The cartilages appear purple or deepblue-black against a green-blue background.OBSERVATIONS.-Several control specimens from
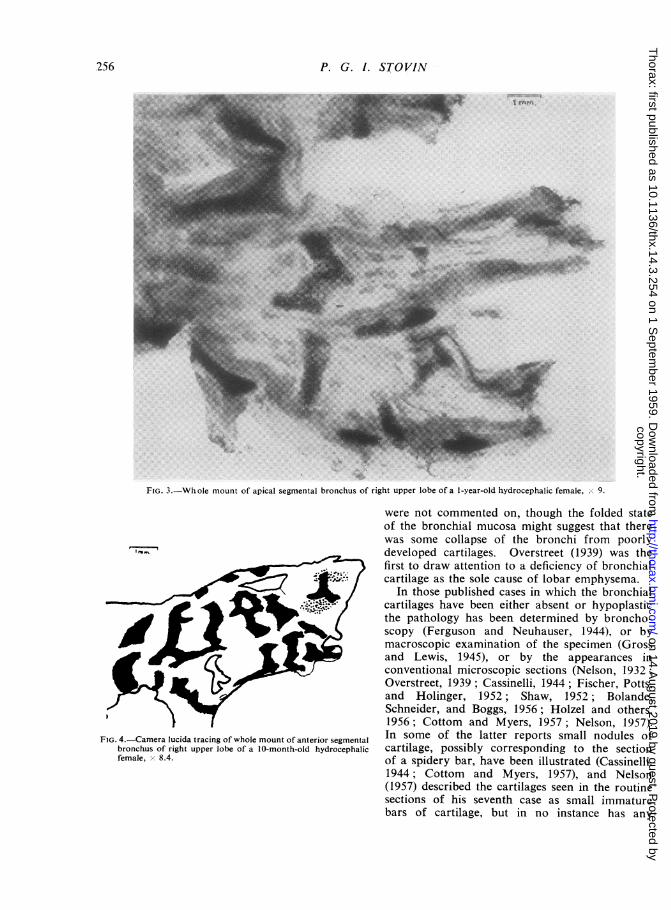
neonatal and infantile deaths up to 1 year of ageshowed stout bars of cartilage with varving degreesof spacing between them (Figs. 3 and 4). Thecartilages tend to run transversely, but there are alsolongitudinally directed processes. In the present casethe lobectomy specimen was re-examined after theselection of material for routine microscopicalexamination and the short remaining lengths of the
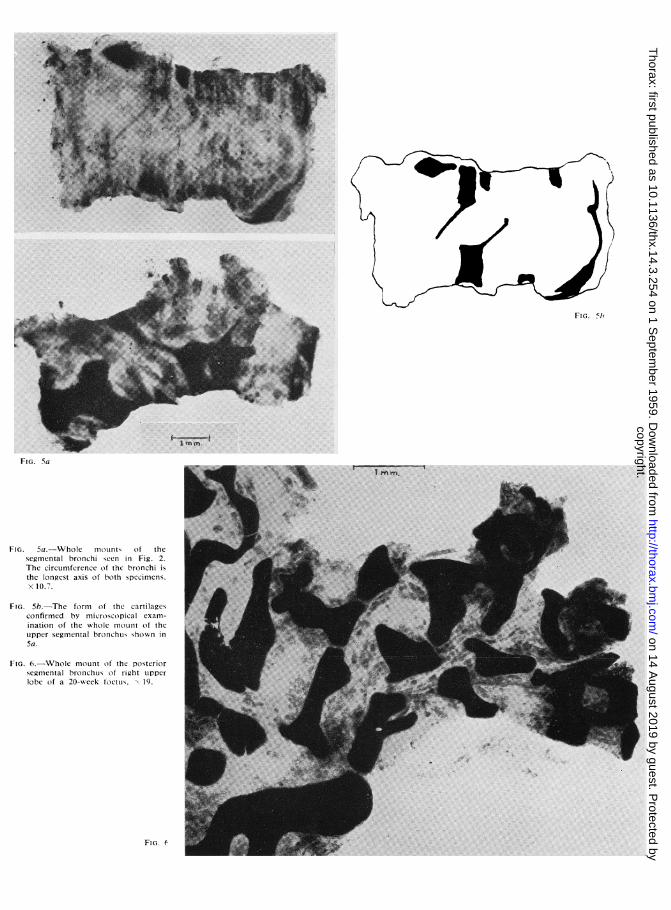
main segmental bronchi were dissected and stainedas above. These portions of bronchi wereimmediately peripheral to the hilar section shown inFig. 2. It is seen (Fig. 5a and b) that the bronchialcartilages have a thin spidery form tending to runpredominantly in a longitudinal direction. This ismore evident in one of the bronchi than in the other,but both show this abnormal morphology. Thebronchial cartilages in a 20-weeks gestation are similarto the other controls (Fig. 6), which suggests that thespidery shapes seen in the present cases are trueaberrations and not the persistence of a foetal form.No comparable study appears to have been made
since that of King (1840, cited by Miller, 1947), whomade dissection preparations of the cartilages of themain bronchi of adults.
DISCUSSION
Probably the earliest recorded case ofcongenital lobar emphysema is that ofBartholinus (1687, cited by Koontz, 1925).Meyer in 1859 (quoted by Miller, 1926) describedthe pathology of a complex case in which severallesions were present; a large residual ductusarteriosus, small bronchi with folded mucosa, andbullous emphysema. The bronchial cartilages
255
copyright. on 14 A
ugust 2019 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.14.3.254 on 1 Septem
ber 1959. Dow
nloaded from
P. G. I. STOVIN
FIG. 3.-Whole mount of apical segmental bronchus of right upper lobe of a 1-year-old hydrocephalic female, 0,9.
were not commented on, though the folded stateof the bronchial mucosa might suggest that therewas some collapse of the bronchi from poorly
am developed cartilages. Overstreet (1939) was thefirst to draw attention to a deficiency of bronchialcartilage as the sole cause of lobar emphysema.
In those published cases in which the bronchialcartilages have been either absent or hypoplasticthe pathology has been determined by broncho-scopy (Ferguson and Neuhauser, 1944), or bymacroscopic examination of the specimen (Grossand Lewis, 1945), or by the appearances inconventional microscopic sections (Nelson, 1932;Overstreet, 1939; Cassinelli, 1944; Fischer, Potts,and Holinger, 1952; Shaw, 1952; Bolande,Schneider, and Boggs, 1956; Holzel and others,1956; Cottom and Myers, 1957; Nelson, 1957).
'amera lucida tracing of whole mount of anterior segmental In some of the latter reports small nodules ofhus of right upper lobe of a 10-month-old hydrocephalic cartilage, possibly corresponding to the sectionx 8.4. of a spidery bar, have been illustrated (Cassinelli.
1944; Cottom and Myers, 1957), and Nelson(1957) described the cartilages seen in the routinesections of his seventh case as small immaturebars of cartilage, but in no instance has any
FIG. 4.-C,broncEfemale
.256
copyright. on 14 A
ugust 2019 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.14.3.254 on 1 Septem
ber 1959. Dow
nloaded from
FI[. 5h
FIG. Sa
FIG. 5a.-Whole mount, of thesegmental bronchi scen in Fig. 2.The circumfcrence of thc bronchi isthe longest axis o1 both specimens.x 107.
FIG. 5b.-The form of the cartilagesconfirmed by microscopical exam-ination of the whole m1oLint of theupper segmental bronchus shown in5a.
FIG. 6.-Whole mount of the posteriorsegmental bronchuLs Of right ulpperlobc of a 20-week foetuLs. \19.
F[o. e
copyright. on 14 A
ugust 2019 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.14.3.254 on 1 Septem
ber 1959. Dow
nloaded from
P. G. 1. STOVIN
reconstruction of the shape or direction of thecartilage been attempted.The present case illustrates the possible
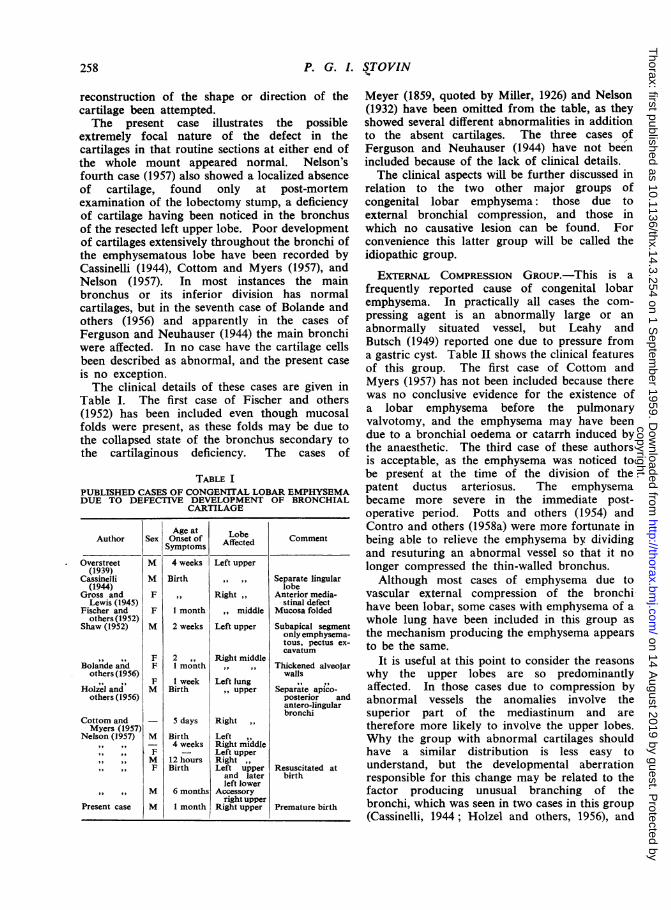
extremely focal nature of the defect in thecartilages in that routine sections at either end ofthe whole mount appeared normal. Nelson'sfourth case (1957) also showed a localized absenceof cartilage, found only at post-mortemexamination of the lobectomy stump, a deficiencyof cartilage having been noticed in the bronchusof the resected left upper lobe. Poor developmentof cartilages extensively throughout the bronchi ofthe emphysematous lobe have been recorded byCassinelli (1944), Cottom and Myers (1957), andNelson (1957). In most instances the mainbronchus or its inferior division has normalcartilages, but in the seventh case of Bolande andothers (1956) and apparently in the cases ofFerguson and Neuhauser (1944) the main bronchiwere affected. In no case have the cartilage cellsbeen described as abnormal, and the present caseis no exception.The clinical details of these cases are given in
Table I. The first case of Fischer and others(1952) has been included even though mucosalfolds were present, as these folds may be due tothe collapsed state of the bronchus secondary tothe cartilaginous deficiency. The cases of
TABLE IPUBLISHED CASES OF CONGEN1TAL LOBAR EMPHYSEMADUE TO DEFECTIVE DEVELOPMENT OF BRONCHIAL
CARTILAGE
Age at LobeAuthor Sex Onset Of Affected Comment
Overstreet M 4 weeks Left upper(1939)
Cassinelli M Birth , , Separate lingular(1944) lobe
Gross and F ,, Right Anterior media-Lewis (1945) , stinal defect
Fischer and F I month middle Mucosa foldedothers (1952)
Shaw (1952) M 2 weeks Left upper Subapical segmentonly emphysema-tous, pectus ex-cavatum
F 2 ,, Right middleBolande and F 1 month ,, . Thickened alveolar
others (1956) walls,, , . F 1 week Left lung , .
Holzel and M Birth upper Separate apico-others (1956) posterior and
antero-lingularbronchi
Cottom and - 5 days RightMyers (1957)
Nelson (1957) M Birth Left- 4 weeks Right middleF - Left upperM 12 hours RightF Birth Left upper Resuscitated at
and later birthleft lower
M 6 months Accessoryright upper
Present case M 1 month Right upper Premature birth
Meyer (1859, quoted by Miller, 1926) and Nelson(1932) have been omitted from the table, as theyshowed several different abnormalities in additionto the absent cartilages. The three cases ofFerguson and Neuhauser (1944) have not beenincluded because of the lack of clinical details.The clinical aspects will be further discussed in
relation to the two other major groups ofcongenital lobar emphysema: those due toexternal bronchial compression, and those inwhich no causative lesion can be found. Forconvenience this latter group will be called theidiopathic group.
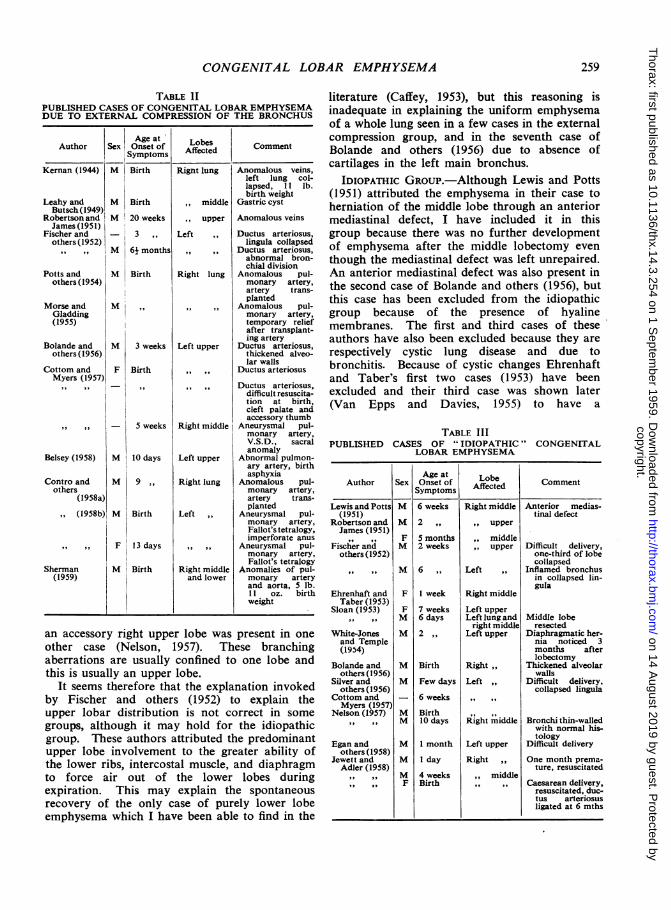
EXTERNAL COMPRESSION GROUP.-This is afrequently reported cause of congenital lobaremphysema. In practically all cases the com-pressing agent is an abnormally large or anabnormally situated vessel, but Leahy andButsch (1949) reported one due to pressure froma gastric cyst. Table II shows the clinical featuresof this group. The first case of Cottom andMyers (1957) has not been included because therewas no conclusive evidence for the existence ofa lobar emphysema before the pulmonaryvalvotomy, and the emphysema may have beendue to a bronchial oedema or catarrh induced bythe anaesthetic. The third case of these authorsis acceptable, as the emphysema was noticed tobe present at the time of the division of thepatent ductus arteriosus. The emphysemabecame more severe in the immediate post-operative period. Potts and others (1954) andContro and others (1958a) were more fortunate inbeing able to relieve the emphysema by dividingand resuturing an abnormal vessel so that it nolonger compressed the thin-walled bronchus.
Although most cases of emphysema due tovascular external compression of the bronchihave been lobar, some cases with emphysema of awhole lung have been included in this group asthe mechanism producing the emphysema appearsto be the same.
It is useful at this point to consider the reasonswhy the upper lobes are so predominantlyaffected. In those cases due to compression byabnormal vessels the anomalies involve thesuperior part of the mediastinum and aretherefore more likely to involve the upper lobes.Why the group with abnormal cartilages shouldhave a similar distribution is less easy tounderstand, but the developmental aberrationresponsible for this change may be related to thefactor producing unusual branching of thebronchi, which was seen in two cases in this group(Cassinelli, 1944; Holzel and others, 1956), and
258
copyright. on 14 A
ugust 2019 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.14.3.254 on 1 Septem
ber 1959. Dow
nloaded from
CONGENITAL LOBAR EMPHYSEMA
TABLE 11PUBLISHED CASES OF CONGENITAL LOBAR EMPHYSEMADUE TO EXTERNAL COMPRESSION OF THE BRONCHUS
Age at LobesAuthor Sex Onset of Affected Comment
Symptoms
M Birth
M Birth
M 20 weeks
3 ,
M 61 months
M Birth
M
M 3 weeks
F Birth
-I- 5 weeks
M 10 days
M 9 .,
M Birth
,, ,9 9 F 13 days
Sherman M Birth(1959)
Right lungI
, middle
, upper
Left ,,
Right lung
Left upper
Right middle
Left upper
Right lung
Left
Right middleand lower
Anomalous veins,left lung col-lapsed, 11 lb.birth weight
Gastric cyst
Anomalous veins
Ductus arteriosus,lingula collapsed
Ductus arteriosus,abnormal bron-chial division
Anomalous pul-monary artery,artery trans-planted
Anomalous pul-monary artery,temporary reliefafter transplant-ing artery
Ductus arteriosus,thickened alveo-lar walls
Ductus arteriosus
Ductus arteriosus,difficult resuscita-tion at birth,cleft palate andaccessory thumb
Aneurysmal pul-monary artery,V.S.D., sacralanomaly
Abnormal pulmon-ary artery, birthasphyxia
Anomalous pul-monary artery,artery trans-planted
Aneurysmal pul-monary artery,Fallot's tetralogy,imperforate anus
Aneurysmal pul-monary artery,Fallot's tetralogy
Anomalies of pul-monary arteryand aorta, 5 lb.11 oz. birthweight
an accessory right upper lobe was present in one
other case (Nelson, 1957). These branchingaberrations are usually confined to one lobe andthis is usually an upper lobe.
It seems therefore that the explanation invokedby Fischer and others (1952) to explain theupper lobar distribution is not correct in somegroups, although it may hold for the idiopathicgroup. These authors attributed the predominantupper lobe involvement to the greater ability ofthe lower ribs, intercostal muscle, and diaphragmto force air out of the lower lobes duringexpiration. This may explain the spontaneousrecovery of the only case of purely lower lobeemphysema which I have been able to find in the
literature (Caffey, 1953), but this reasoning isinadequate in explaining the uniform emphysemaof a whole lung seen in a few cases in the externalcompression group, and in the seventh case ofBolande and others (1956) due to absence ofcartilages in the left main bronchus.
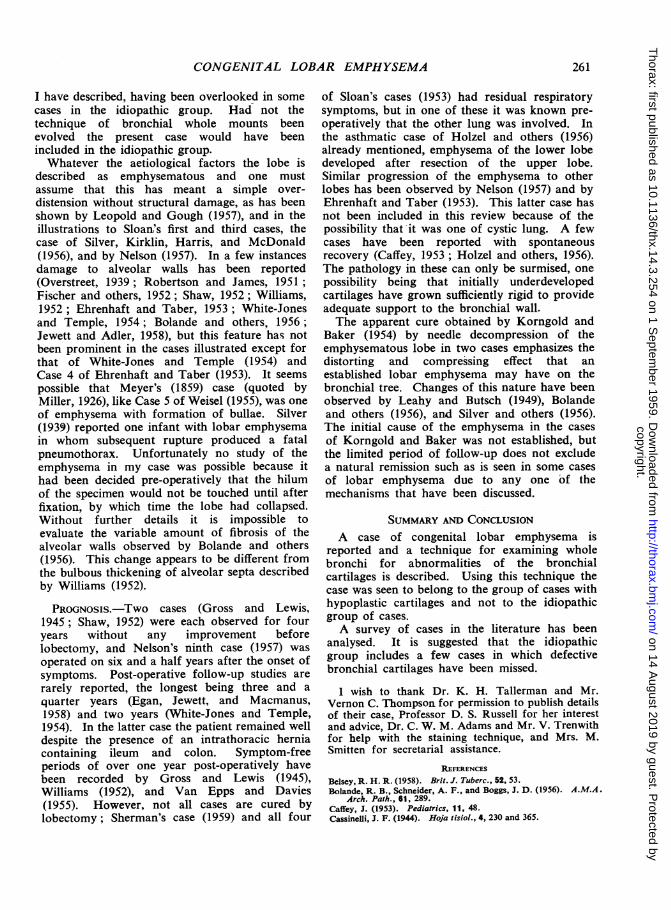
IDIOPATHIC GROUP.-Although Lewis and Potts(1951) attributed the emphysema in their case toherniation of the middle lobe through an anteriormediastinal defect, I have included it in thisgroup because there was no further developmentof emphysema after the middle lobectomy eventhough the mediastinal defect was left unrepaired.An anterior mediastinal defect was also present inthe second case of Bolande and others (1956), butthis case has been excluded from the idiopathicgroup because of the presence of hyalinemembranes. The first and third cases of theseauthors have also been excluded because they arerespectively cystic lung disease and due tobronchitis. Because of cystic changes Ehrenhaftand Taber's first two cases (1953) have beenexcluded and their third case was shown later(Van Epps and Davies, 1955) to have a
TABLE IIIPUBLISHED CASES OF "IDIOPATHIC" CONGENITAL
LOBAR EMPHYSEMA
Age at LbAuthor Sex Onset of Affected CommentSymptoms Afce
Lewis and Potts M 6 weeks Right middle Anterior medias-(1951) tinal defect
Robertson and M 2 ,, ,, upperJames (1951)
,, ,,2I F 5 months ,, middleFischer and M 2 weeks ,, upper Difficult delivery,
others (1952) one-third of lobecollapsed
M 6 ,, Left ,, Inflamed bronchusin collapsed lin-gula
Ehrenhaft and F 1 week Right middleTaber (1953)
Sloan (1953) F 7 weeks Left upperM 6 days Left lung and Middle lobe
right middle resectedWhite-Jones M 2 ,, Left upper Diaphragmatic her-and Temple nia noticed 3(1954) months after
lobectomyBolande and M Birth Right Thickened alveolar
others (1956) wallsSilver and M Few days Left ,, Difficult delivery,
others (1956) collapsed lingulaCottom and - 6 weeksMyers (1957)
Nelson (1957) M BirthM 10 days Right middle Bronchi thin-walled
with normal his-tology
Egan and M I month Left upper Difficult deliveryothers (1958)
Jewett and M 1 day Right ,, One month prema-Adler (1958) ture, resuscitated
M 4 weeks ,, middleF Birth ,, ,, Caesarean delivery,
resuscitated, duc-tus arteriosusligated at 6 mths
Kernan (1944)
Leahy andButsch (1949)
Robertson andJames (1951)
Fischer andothers (1952)
Potts andothers (1954)
Morse andGladding(1955)
Bolande andothers (1956)
Cottom andMyers (1957)
Belsey (1958)
Contro andothers
(1958a),, (1958b)
259
copyright. on 14 A
ugust 2019 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.14.3.254 on 1 Septem
ber 1959. Dow
nloaded from

P. G. 1. STOVIN
complicating lipoid pneumonia. The onset ofSloan's second case (1953) appears to have beendue to the probable inhalation of milk and hastherefore not been included in Table III, whichgives the clinical details of the idiopathic group.OTHER MINOR GRouPs.-These are listed in
Table IV. Robertson and James (1951) are not
TABLE IVPUBLISHED CASES OF CONGENITAL LOBAR EMPHYSEMA
ATTRIBUTED TO VARIOUS RARER CAUSES
Age atGroup Author Sex Onset Lobe Commentof Symp- Affected Comn
toms
Mucosal Robertson M 2 weeks Rightfold and James upper
(1951)M 3 ,, Left upper A little peribron-
chial collapseBronchial Belsey M Birth Right Pin hole orifice
atresia (1958) upper to lobar bron-chus
,, M 51 years Left upper No orifice tolobar bron-chus, hyper-plastic bron-chial carti-lages, abnor-mal pulmonaryarteries to thelobe
Asthma- Williams M Birth Right Mild diffuse in-like (1952) middle flammation ingroup lobe
Sloan M 3 weeks Right(1953) middle
Holzel F 4 ,, Left upperand and laterothers left lower(1956)
the only authors to describe mucosal folds. Onecase (Fischer and others, 1952) has been discussedin the deficient cartilage group above. Mucosalfolds were noticed by Leahy and Butsch (1949),but the patches of collapse noticed histologicallyin the emphysematous lobe must raise thesuspicion that the emphysema was due toinflammation. It is interesting that these authorsconsidered the mucosal folds to be in the natureof a mucosal prolapse secondary to theemphysema.The five cases which Weisel (1955) claimed to
have improved by bronchial dilatation mightbelong to the atretic group, but no histologicalstudies were described. Belsey (1958), besidesgiving details of two atretic cases, mentionsbronchial tumours as a further possible cause oflobar emphysema, some of which might becongenital.There is a small group of cases with evidence
of bronchial neuromuscular dysfunction similarto asthma but of a more localized nature.Williams's case (1952) and Sloan's first case (1953)
both obtained temporary symptomatic relief fromadrenaline, and the former case showed bulbousthickening of the interalveolar septa which mayhave been hypertrophic muscle bundles in therespiratory bronchioles. The second case ofHolzel and others (1956) also probably belongs tothis group and adrenaline was beneficial for therelapse after lobectomy.
Hyaline membranes were present in the secondcase of Bolande and others (1956) and thickenedalveolar walls were mentioned in all their cases,but the clinical details are not suggestive ofhyaline membrane disease. The history ofEhrenhaft and Taber's seventh case (1953) issuggestive of this disease, but no hyalinemembranes were observed. Ehrenhaft and Taberpostulated that traumatic interstitial emphysemamight cause infantile lobar emphysema, but thereis no histological and only slight clinical evidencein favour of this hypothesis. These two possibleaetiological factors therefore do not appear inTable IV.The salient points in the clinical data of the
three main groups are summarized in Table V.
TABLE VSUMMARY OF SOME FEATURES OF THE THREEPRINCIPAL GROUPS OF CONGENITAL LOBAR
EMPHYSEMA
VascularExternal Idiopathic Defective
Compression Group CartilageGroup Group
Sex ratio M/F 11/2 13!4 8/7Age at onset BirBirth- Birth-5 Birth-6
months months months(average (average (average27 days) 26 days) 23 days)
Left upper.. 6 7 6Lobar Left lung 2 2
distri-J Right upper 1 4 5bution Right middle 2 6 4
Right lung.. 5LBilateral I
Though the groups are small there appears to beone feature distinguishing the defective-cartilagegroup from the other two, namely a higherproportion of females. In addition, although theaverage age for the onset of symptoms in thethree main groups is the same, it is much lessfrequent for the symptoms to begin after thefirst month in the defective cartilage group (oneout of 16) than it is in the other groups (one outof four). These differences may be genuine, butthe groups are so small that a definite conclusionmust await the description of many more cases inall groups. Certainly the differences between thegroups are not sufficient to exclude the possibilityof a limited defect in bronchial cartilage, such as
260
copyright. on 14 A
ugust 2019 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.14.3.254 on 1 Septem
ber 1959. Dow
nloaded from
CONGENITAL LOBAR EMPHYSEMA
I have described, having been overlooked in somecases in the idiopathic group. Had not thetechnique of bronchial whole mounts beenevolved the present case would have beenincluded in the idiopathic group.Whatever the aetiological factors the lobe is
described as emphysematous and one mustassume that this has meant a simple over-distension without structural damage, as has beenshown by Leopold and Gough (1957), and in theillustrations to Sloan's first and third cases, thecase of Silver, Kirklin, Harris, and McDonald(1956), and by Nelson (1957). In a few instancesdamage to alveolar walls has been reported(Overstreet, 1939; Robertson and James, 1951;Fischer and others, 1952; Shaw, 1952; Williams,1952; Ehrenhaft and Taber, 1953; White-Jonesand Temple, 1954; Bolande and others, 1956;Jewett and Adler, 1958), but this feature has notbeen prominent in the cases illustrated except forthat of White-Jones and Temple (1954) andCase 4 of Ehrenhaft and Taber (1953). It seemspossible that Meyer's (1859) case (quoted byMiller, 1926), like Case 5 of Weisel (1955), was oneof emphysema with formation of bullae. Silver(1939) reported one infant with lobar emphysemain whom subsequent rupture produced a fatalpneumothorax. Unfortunately no study of theemphysema in my case was possible because ithad been decided pre-operatively that the hilumof the specimen would not be touched until afterfixation, by which time the lobe had collapsed.Without further details it is impossible toevaluate the variable amount of fibrosis of thealveolar walls observed by Bolande and others(1956). This change appears to be different fromthe bulbous thickening of alveolar septa describedby Williams (1952).
PROGNOSIS.-Two cases (Gross and Lewis,1945; Shaw, 1952) were each observed for fouryears without any improvement beforelobectomy, and Nelson's ninth case (1957) wasoperated on six and a half years after the onset ofsymptoms. Post-operative follow-up studies arerarely reported, the longest being three and aquarter years (Egan, Jewett, and Macmanus,1958) and two years (White-Jones and Temple,1954). In the latter case the patient remained welldespite the presence of an intrathoracic herniacontaining ileum and colon. Symptom-freeperiods of over one year post-operatively havebeen recorded by Gross and Lewis (1945),Williams (1952), and Van Epps and Davies(1955). However, not all cases are cured bylobectomy; Sherman's case (1959) and all four
of Sloan's cases (1953) had residual respiratorysymptoms, but in one of these it was known pre-operatively that the other lung was involved. Inthe asthmatic case of Holzel and others (1956)already mentioned, emphysema of the lower lobedeveloped after resection of the upper lobe.Similar progression of the emphysema to otherlobes has been observed by Nelson (1957) and byEhrenhaft and Taber (1953). This latter case hasnot been included in this review because of thepossibility that it was one of cystic lung. A fewcases have been reported with spontaneousrecovery (Caffey, 1953; Holzel and others, 1956).The pathology in these can only be surmised, onepossibility being that initially underdevelopedcartilages have grown sufficiently rigid to provideadequate support to the bronchial wall.The apparent cure obtained by Korngold and
Baker (1954) by needle decompression of theemphysematous lobe in two cases emphasizes thedistorting and compressing effect that anestablished lobar emphysema may have on thebronchial tree. Changes of this nature have beenobserved by Leahy and Butsch (1949), Bolandeand others (1956), and Silver and others (1956).The initial cause of the emphysema in the casesof Korngold and Baker was not established, butthe limited period of follow-up does not excludea natural remission such as is seen in some casesof lobar emphysema due to any one of themechanisms that have been discussed.
SUMMARY AND CONCLUSIONA case of congenital lobar emphysema is
reported and a technique for examining wholebronchi for abnormalities of the bronchialcartilages is described. Using this technique thecase was seen to belong to the group of cases withhypoplastic cartilages and not to the idiopathicgroup of cases.A survey of cases in the literature has been
analysed. It is suggested that the idiopathicgroup includes a few cases in which defectivebronchial cartilages have been missed.
1 wish to thank Dr. K. H. Tallerman and Mr.Vernon C. Thompson for permission to publish detailsof their case, Professor D. S. Russell for her interestand advice, Dr. C. W. M. Adams and Mr. V. Trenwithfor help with the staining technique, and Mrs. M.Smitten for secretarial assistance.
REFERENCESBelsey, R. H. R. (1958). Brit. J. Tuberc., 52, 53.Bolande, R. B., Schneider, A. F., and Boggs, J. D. (1956). A.M.A.
Arch. Path., 61, 289.Caffey, J. (1953). Pediatrics, 11, 48.Cassinelli, J. F. (1944). Hoja tisiol., 4, 230 and 365.
261
copyright. on 14 A
ugust 2019 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.14.3.254 on 1 Septem
ber 1959. Dow
nloaded from

P. G. 1. STOVIN
Contro, S., Miller, R. A., White, H., and Potts, W. J. (1958a).Circulation, 17, 418.
5(1958b). Ibid., 17, 424.Cottom, D. G., and Myers, N. A. (1957). Brit. med. J., 1, 1394.Egan, R. W., Jewett, T. C., and Macmanus, J. E. (1958). A.M.A.
Arch. Surg., 77, 584.Ehrenhaft, J. L., and Taber, R. E. (1953). Surgery, 34, 412.Ferguson, C. F., and Neuhauser, E. B. D. (1944). Amer. J. Roent-
genol., 52, 459.Fischer, H. W., Potts, W. J., and Holinger, P. H. (1952). J. Pediat.,
41, 403.Gross, R. E., and Lewis, J. E. (1945). Surg. Gynec. Obstet., 80, 549.Holzel, A., Bennett, E., and Vaughan, B. F. (1956). Arch. Dis.
Childh., 31, 216.Jewett, T. C., and Adler, R. H. (1958). Surgery, 43, 926.Kernan, J. D. (1944). Ann. Otol. (St. Louis), 53, 818.Koontz, A. R. (1925). Bull. Johns Hopk. Hosp., 37, 340.Korngold, H. W., and Baker, J. M. (1954). Pediatrics, 14, 296.Leahy, L. J., and Butsch, W. L. (1949). Arch. Surg. (Chicago), 59,
466.Leopold, J. G., and Gough, J. (1957). Thorax, 12, 219.Lewis, J. E., and Potts, W. J. (1951). J. thorac. Surg., 21, 438.
Miller, R. T. (1926). Arch. Surg. (Chicago), 12, 392.Miller, W. S. (1947). The Lung, 2nd ed., p. 26. Charles C. Thomas,
Springfield, Illinois.Morse, H. R., and Gladding, S. (1955). Amer. J. Dis. Child., 89, 351.Nelson, R. L. (1932). J. Pediat., 1, 233.Nelson, T. Y. (1957). Arch. Dis. Childh., 32, 38.Overstreet, R. M. (1939). Amer. J. Dis. Child., 57, 861.Potts, W. J., Holinger, P. H., and Rosenblum, A. H. (1954). J.
Amer. med. Ass., 155, 1409.Robertson, R., and James, E. S. (1951). Pediatrics, 8, 795.Shaw, R. R. (1952). Ibid., 9, 220.Sherman, F. E. (1959). J. Pediat., 54, 93.Silver, A. W., Kirklin, J. W., Harris, L. E., and McDonald, J. R.
(1956). Dis. Chest, 30, 456.Silver, H. B. (1939). Amer. J. Dis. Child., 57, 907.Sloan, H. (1953). J. thorac. Surg., 26, 1.
Van Epps, E. F., and Davies, D. H. (1955). Amer. J. Roentgenol.,73, 375.
Weisel, W. (1955). Ann. Surg., 142, 17.White-Jones, R. H., and Temple, L. J. (1954). Arch. Dis. Childh.,
29, 248.Williams, M. H. (1952). J. thorac. Surg., 24, 522.
262
copyright. on 14 A
ugust 2019 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.14.3.254 on 1 Septem
ber 1959. Dow
nloaded from