congenital lung abnormalities
TRANSCRIPT

Congenital lung abnormalitiesDr Aftab Qadir

1.TRACHEOBRONCHIAL ABNORMALITIES•Tracheal agenesis•Tracheal stenosis•Tracheomalacia•Tracheo-oesophageal fistula (TOF)•Bronchial atresia•Tracheal bronchus (PIG bronchus)

2.PULMONARY UNDER DEVELOPMENT•Lung agenesis•Lobar under development•Scimitar syndrome

3.Bronchopulmonary foregut malformation•Bronchogenic cysts•Enteric cysts•Neuroenteric cysts•CCAM•Pulmonary sequestration

5.DIAPHRAGMATIC ABNORMALITIES•Congenital diaphragmatic hernia•Congenital eventeration of the diaphragm
Tracheal agenesis•Rare •Commonly associated with maternal
polyhydramnios•Presentation is immediate and acute with
severe respiratory distress, absent cry and inability to intubate the airway.
•There are three main forms of tracheal agenesis:


Tracheal stenosis•Congenital stenosis due to complete
cartinogenous rings is rare. •50% focal, 30% generalised ,20% funnel
shaped•90% of affected children present in the
first year of life with biphasic stridor. •CT is useful in assessing the anatomy and
has the added advantage of angiographic capabilities.
•MRI and bronchoscopy






Tracheomalacia•Softening of the tracheal wall, due to
cartilaginous abnormalities. •Commonest type is secondary to
tracheostomy, oesophageal atresia/TOF •Chronic inflammation(associated with
cystic fibrosis, recurrent aspiration, immuno-deficiency)
•Extrinsic compression (vascular rings, slings or aberrancy)
•Neoplasia

Causes expiratory wheeze•Fluoroscopy shows an exaggerated
decrease in the sagital width of the trachea during expiration.
•Dynamic CT can be useful to assess the cross-sectional anatomy and compliance of the trachea.


Tracheo-oesophageal fistula (TOF)•Majority of cases are associated with the
presence of oesophageal atresia. •May present with choking, cyanosis,
coughing at the time of feeding.•Contrast oesophagram is used to
demonstrate the presence of a fine hair-like structure connecting the oesophagus and trachea with linear opacification of the posterior tracheal wall





Bronchial atresia•The upper lobe bronchi are more
frequently affected by congenital atresia of lobar or segmental bronchi.
•May be associated abnormalities such as bronchogenic cyst, intralobar sequestration or cystic adenomatoid malformation.



Tracheal bronchus ( Pig bronchus)•Incidence is 1 % of the normal population•Right upper lobe bronchus arises directly
from the trachea



PULMONARY UNDER DEVELOPMENT•Agenesis, aplasia and hypoplasia.•Agenesis is complete absence of a lung
or lobe with absent bronchi •Aplasia is absence of lung tissue but the
presence of a rudimentary bronchus•Hypoplasia is the presence of both
bronchi and alveoli in an underdeveloped lobe



Lung agenesis•Recognizable with a small opaque
hemithorax, displacement of mediastinal structures towards that side.
•Bronchography or bronchoscopy confirms the absent main stem bronchus
•Angiography shows no pulmonary or bronchial arterial circulation.





Scimitar syndrome• Unique form of lobar agenesis or aplasia• Common feature hypoplasia or aplasia of one or
more lobes of the right lung. • The hemithorax is small, with obscuration of the
heart border and a retrosternal soft-tissue density
• Anomalous vein has the appearance of a Turkish scimitar, which normally drains to the IVC
• The right pulmonary artery may be absent• Systemic vessel arising from the lower thoracic
or upper abdominal aorta supplying the right lower lobe.






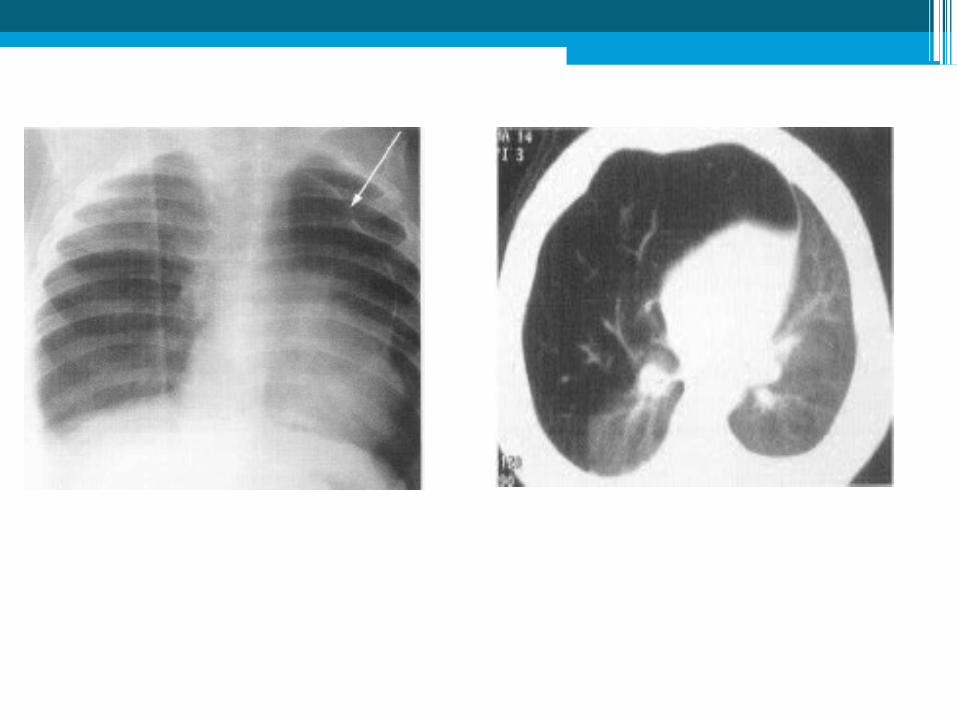
Congenital lobar over inflation/emphysema
•Characterised by progressive over distension of a lobe
•Aetiology is unknown in 50% of cases•Male to female ratio is 3:1 •Associated anomalies include the patent
ductus arteriosus, ventricular septal defect and tetralogy of Fallot
•The upper lobes, or right middle lobe, are commonly involved.


Bronchopulmonary foregut malformation•Bronchogenic cysts •Enteric and •Neurenteric cysts•Cystic hamartomatous (adenomatous)
malformation •Pulmonary sequestration.

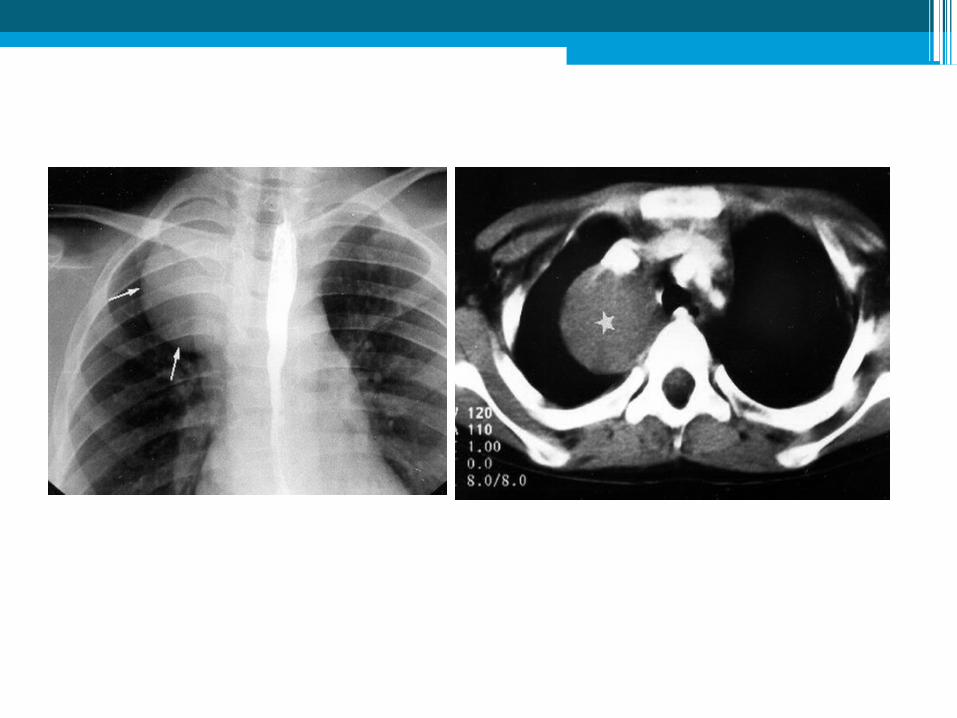
Bronchogenic cysts•50% of all congenital thoracic cysts •May be intrapulmonary or mediastinal
bronchogenic •Can be paratracheal (usually right sided,
carinal or hilar) •Carinal location is most common. •Bronchogenic cysts do not usually
communicate with the tracheobronchial tree





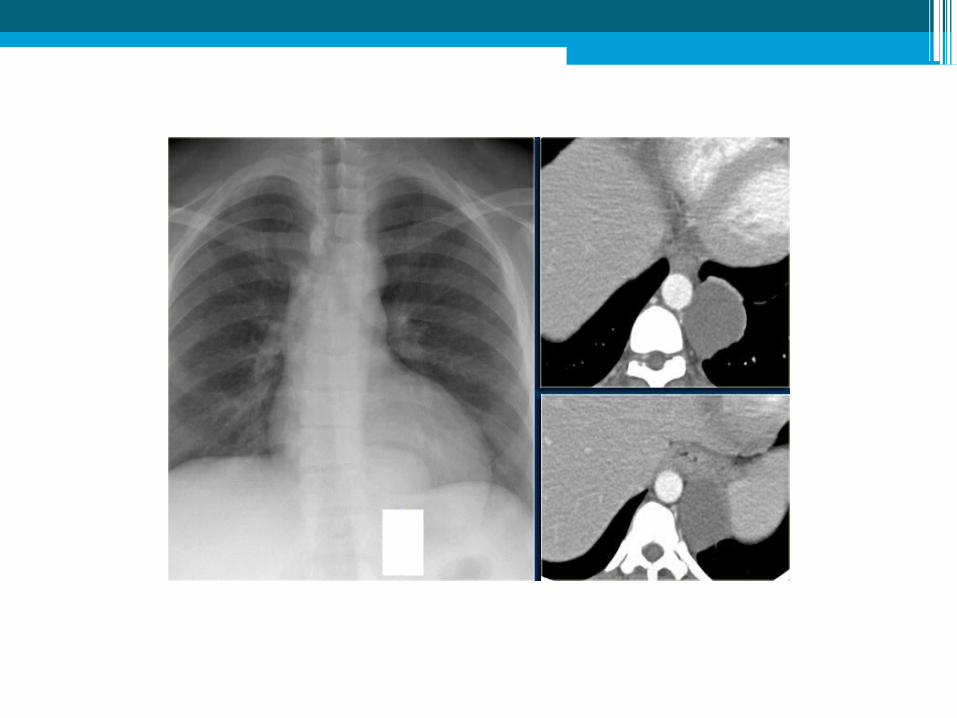
Enteric cysts•Located in the posterior mediastinum. •If present in the oesophageal wall these
are referred to as oesophageal cysts or duplication cysts.
•Mediastinal uptake of 99 Tc-MDP (pertechnetate)contain gastric mucosa.


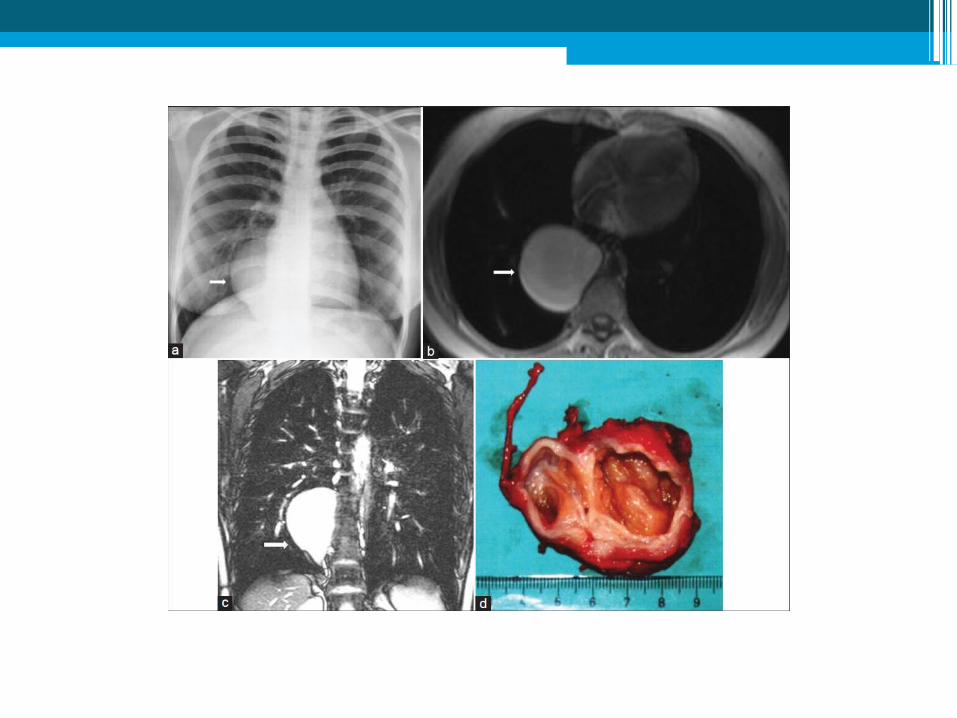
Neuroenteric cysts•Present as posterior mediastinal masses
with associated vertebral abnormalities.•MRI is the most useful tool for evaluating
the thoracic and spinal components of neuroenteriec cysts


CCAM•Hamartomatous proliferation of terminal
bronchioles •Composed of both solid and cystic tissue. •Malformations are classified on the basis
of clinical, radiographic and histological features:
•Type 1,2 and 3






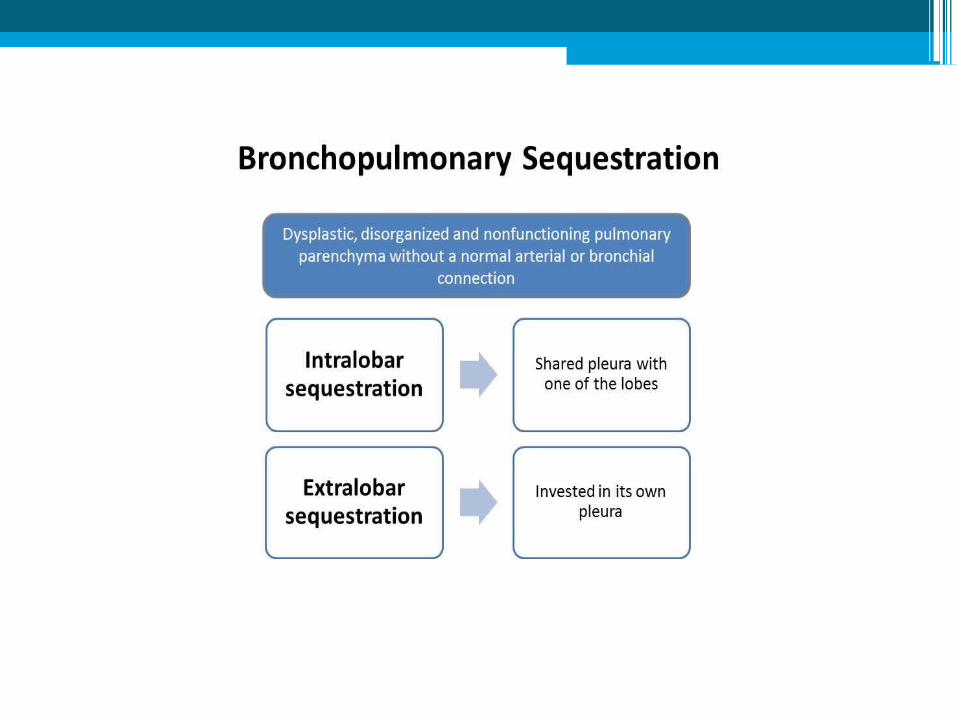
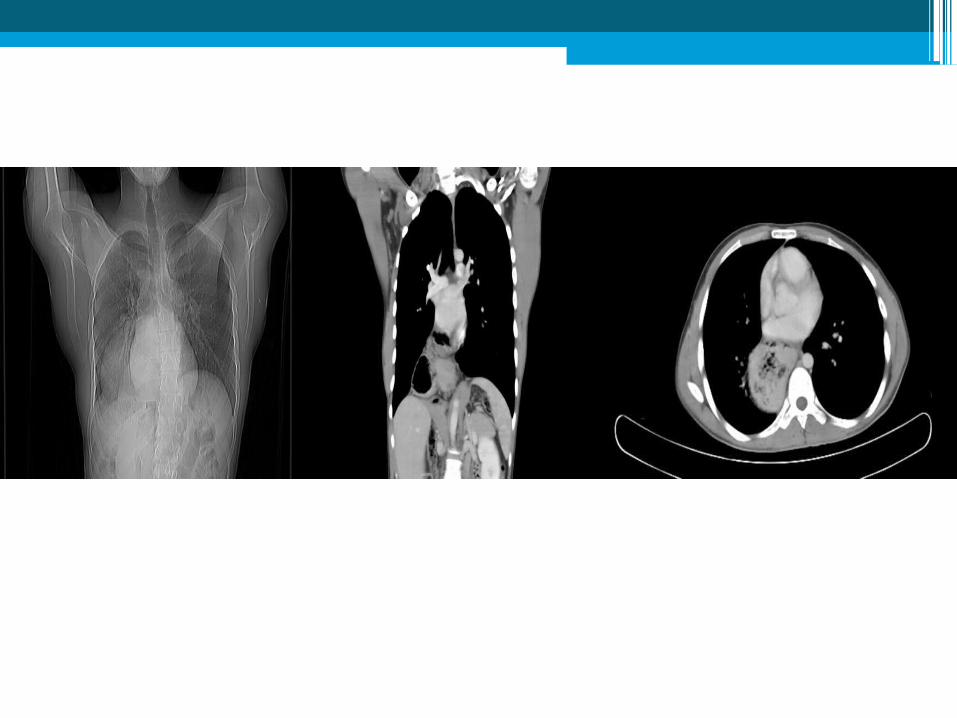
Pulmonary sequestration•Congenital mass of aberrant pulmonary
tissue•No normal connection with the bronchial
tree or with the pulmonary arteries.•Usually located in one of the basal
segments of the lower lobe. •Intralobar sequestration (ILS) is
contained within the lung with no separate pleural covering


CHARACTERSTIC
INTRALOBAR
EXTRALOBAR
Incidence More common ( 75 %) Less common( 25 %)
Gender predisposition Equal Men 4: 1
Pleural investment Shares visceral pleura of parent lobe
Separate visceral pleura
Location Posterior basal segments(Approx. 60% on left)
Above, below or withindiaphragm(Approx. 90% on left)
Venous Drainage Pulmonary venous Systemic venous (azygos, IVC, portal)
Presentation Early adulthood with a history of pulmonary infection, chronic cough, or asthma.Asymptomatic mass (15%)
Mostly present during first 6 months of lifedue to respiratory orfeeding problems
RadiographicFeatures
Homogeneousconsolidation withirregular margins oruniformly dense masswith smooth or lobulatedcontours.
Single well defined,homogeneous, triangularshaped opacity in the lowerthorax. May presentelse where in the thoraciccavity.





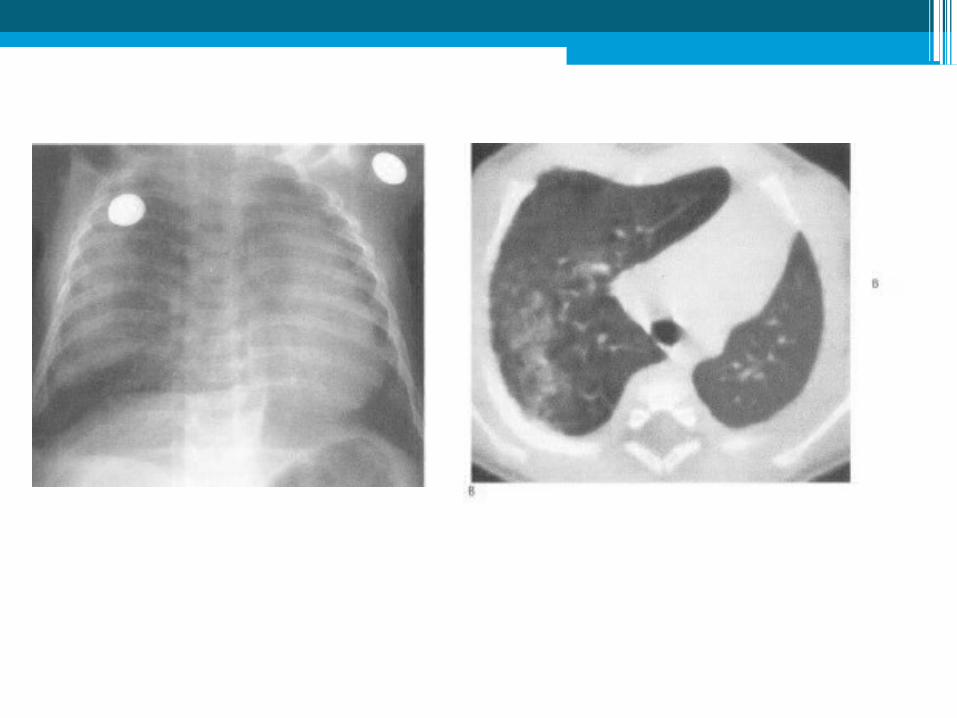
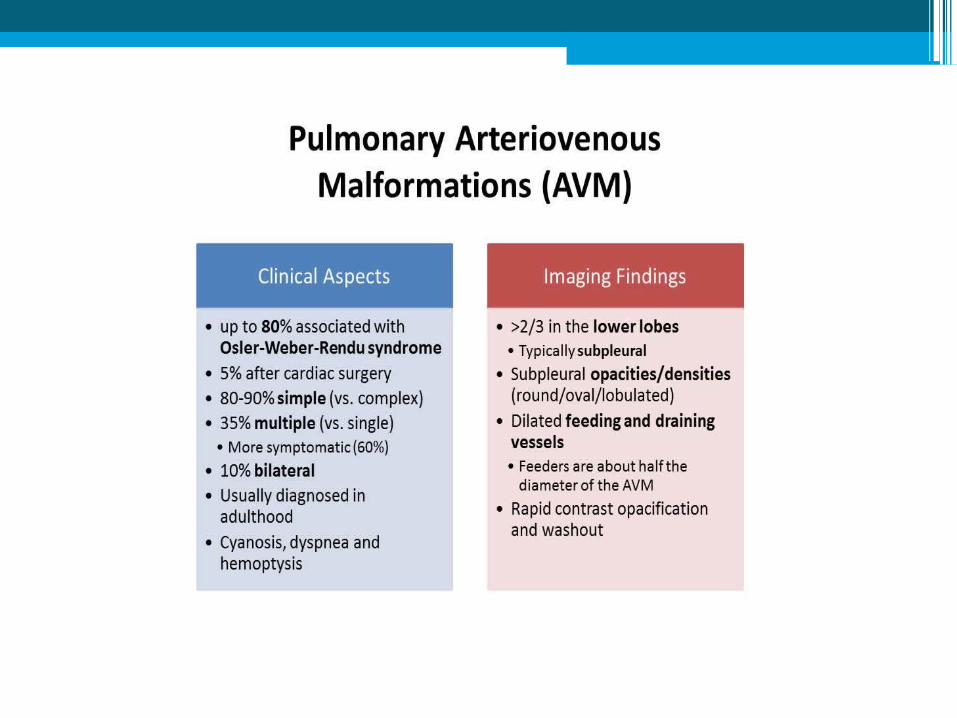
Pulmonary arteriovenous malformations• Congenital or acquired. • The acquired connections arc called
pulmonary fistulas. • Congenital arteriovenous malformations are
abnormal communications between pulmonary arteries and veins
• No intervening capillary bed and are often clinically silent,
• 60% are in the lower lobes• Typical appearances are of a well-defined
pulmonary mass which is often lobulated.



DIAPHRAGMATIC ABNORMALITIES•Hernia •Eventeration •Agenesis
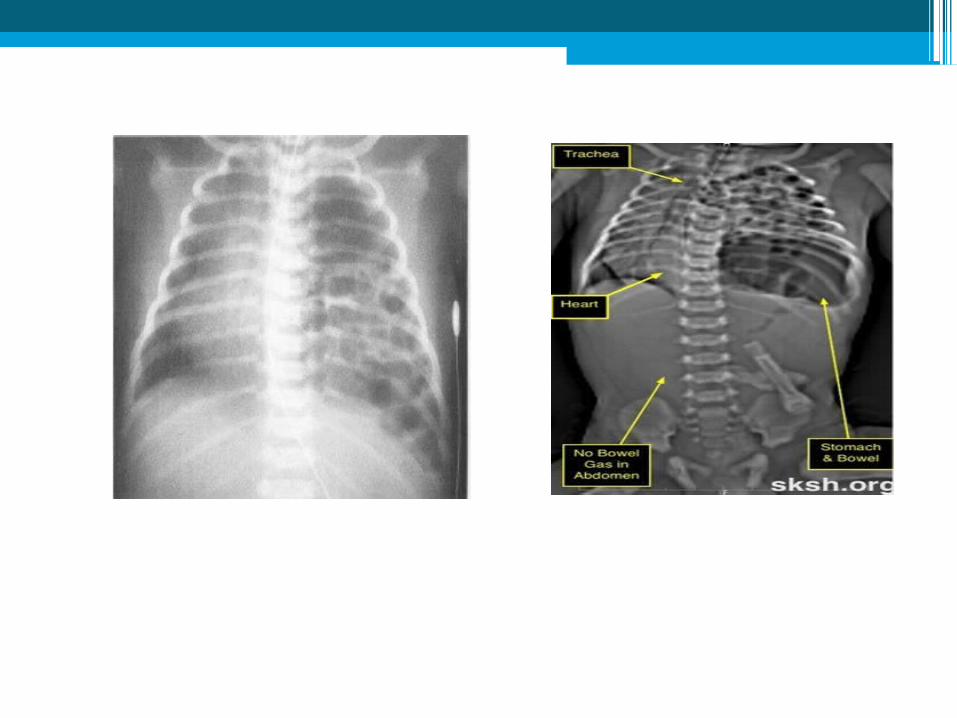
Congenital diaphragmatic hernia•Boakdalek hernia-Posteropleuoperitoneal
foramen•Causes severe respiratory distress in the
neonate •Involves the left pleuroperitoneal foramen
in 75 % of cases.•The prognosis correlates with the degree
of underlying lung hypoplasia

•Neonatal radiograph shows a left-sided large intrathoracic mass of soft-tissue density
•There is absence of the normal gas-containing bowel in the abdomen.



Congenital eventeration of the diaphragm•Either partial or complete •Often right sided, due to hypoplasia of the
diaphragmatic muscle. •Most eventerations are minor, transitory,
local diaphragmatic elevations found incidentally within the first few years of life
•Disappear with age.


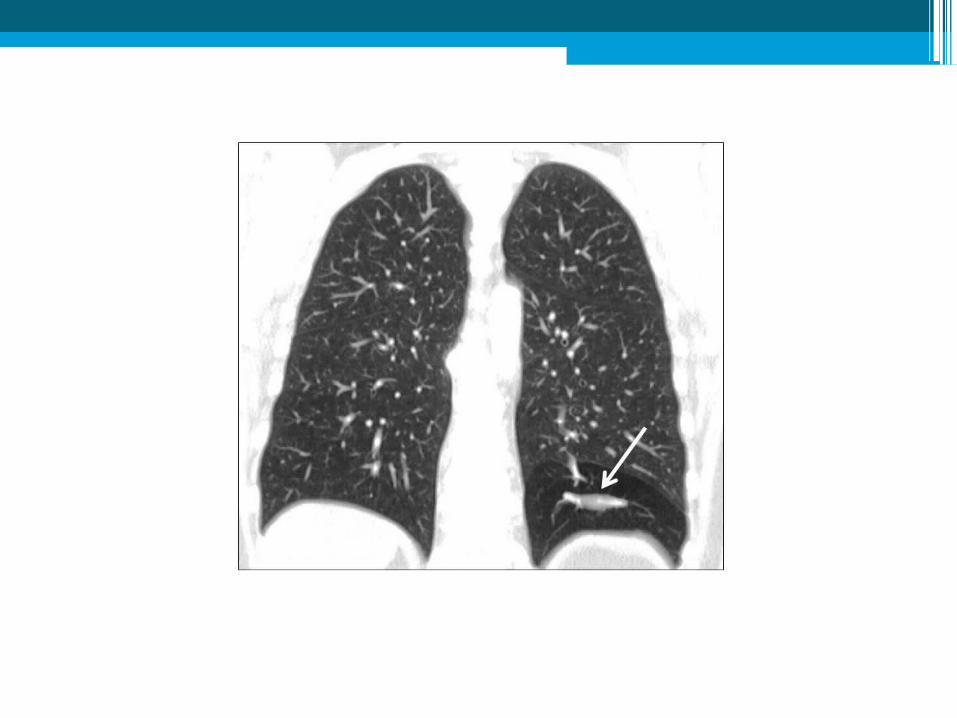
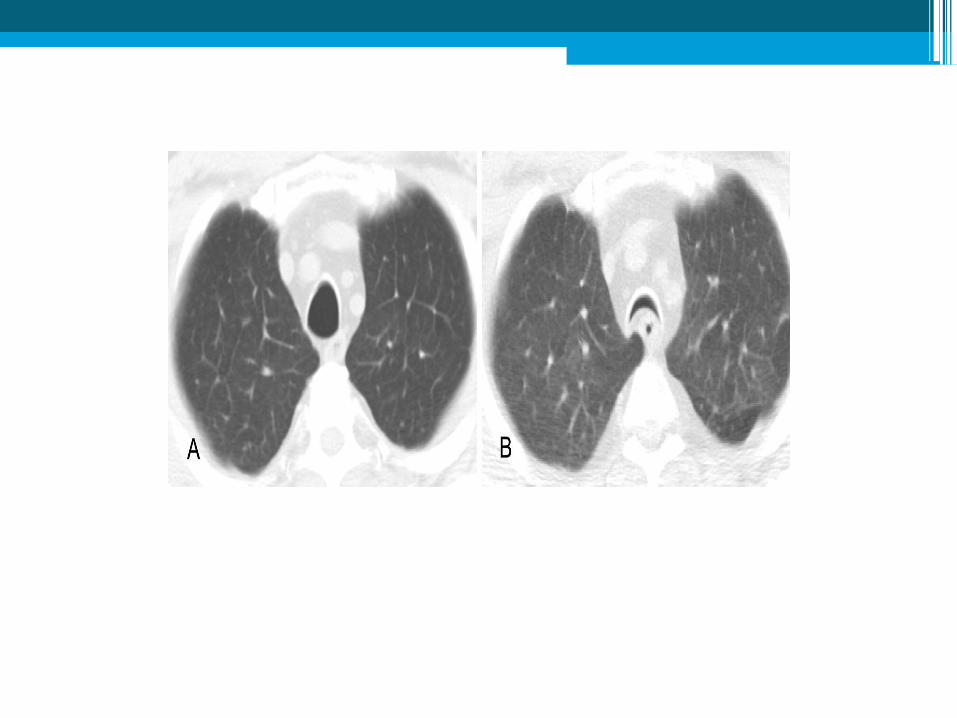
CYSTIC FIBROSIS•Autosomal recessive trait •Prevalence of approximately 1 in 2500. •Chronic respiratory illness


Imaging • Atelectasis• Mucoid impaction• Focal or generalized overinflation• Cylindrical or cystic bronchiectasis• Bronchial wall thickening • Hilar adenopathy• Pulmonary arterial hypertension and cor
pulmonale• Recurrent pneumonias• Hypertrophic osteoarthropathy • Recurrent pneumothorax is common




Few cases







Thank You