coordinator: dr. anca negovan author: andreea bianca stoica co-authors: drd. monica pantea adrian...
TRANSCRIPT

Investigation of ulcer and bleeding sings in patients with non-steroidal anti-inflammatory drugs and low-dose aspirin consumption: a case-
control study Coordinator: Dr. Anca Negovan
Author: Andreea Bianca StoicaCo-authors: Drd. Monica Pantea
Adrian Stoica
Roxana Spac
Gavriela Radoiu

INTRODUCTIONNon-steroidal anti-inflammatory drugs
(NSAID) and low-dose aspirin (LDA) are well known to cause gastrointestinal mucosal injury.
The gastrointestinal side effects of NSAIDs and antiplatelet therapy are important causes of patients’ addressability to the gastroenterologist in a population with a high prevalence of Helicobacter pylori infection.

BackgroundLow-dose aspirin (ASA) is frequently used in
primary and secondary prevention of cardio-vascular and cerebro-vascular events due to the clinical evidence of benefits in decreasing mortality.
Long term treatment has some benefits such as reducing myocardial infarction, cerebro-vascular events and death caused by vascular disease, but it also has disadvantages: it can cause a higher prevalence of endoscopic upper gastrointestinal lesions.Kim C, et al. Am J Prev Med 2004
Pirmohamed M, BMJ 2004, 329:15-19

THE AIM
To determine the prevalence and severity of endoscopic upper gastrointestinal lesions in patients taking low-dose aspirin and non-aspirin non-steroidal anti-inflammatory drugs in a population with a high prevalence of H. pylori infection

METHODS (1)We perform a longitudinal descriptive study
of upper gastrointestinal endoscopy and medical records (including medication) in patients referred for endoscopy in III-rd Medical Clinic Targu-Mures during a period of three years (2011-2013).
We matched patients who were taking NSAIDs (n=111), aspirin (226) with control patients (n=750) who were reportedly not taking any of these medications

METHODS (2)Including criteria were: patients referred for
UDE presenting dyspeptic symptoms (heartburn, abdominal pain, vomiting), melaena, haematemesis, unexplained anemia or patients evaluated for unexplained weight loss, or evaluated before cardiac surgery.
Excluding criteria were: portal hypertension, Mallory-Weiss tears, neoplastic lesions, therapeutic maneuver, alcohol intake more than 20U weekly.
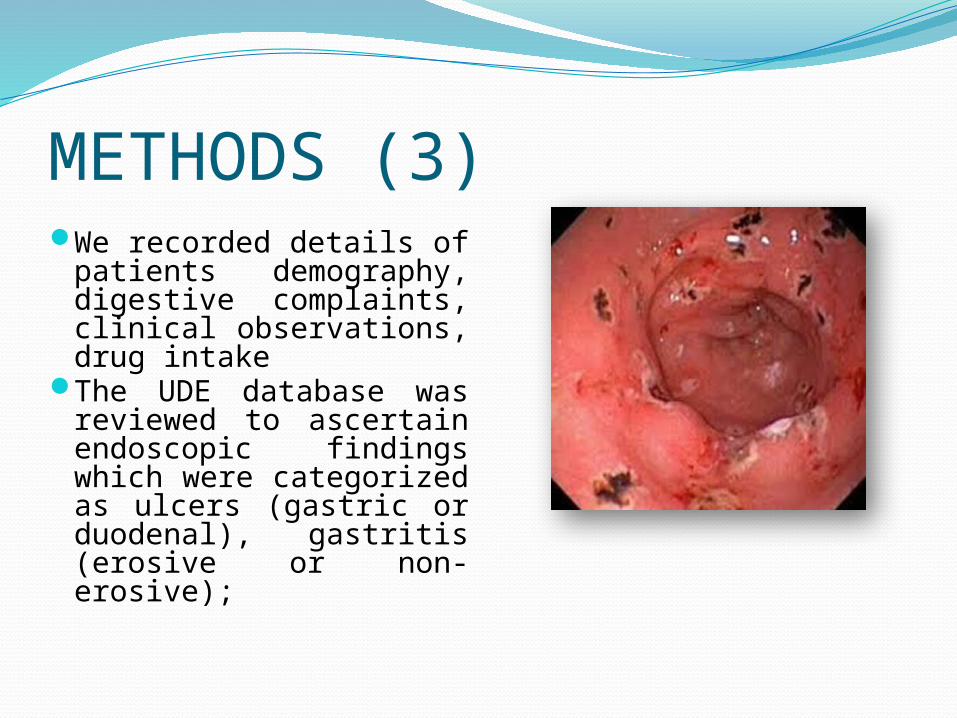
METHODS (3)We recorded details of
patients demography, digestive complaints, clinical observations, drug intake
The UDE database was reviewed to ascertain endoscopic findings which were categorized as ulcers (gastric or duodenal), gastritis (erosive or non-erosive);

RESULTSA total number of 1421 patients, 740 men and
681 women (mean age 60,6 years) were referred for UDE because symptoms (heartburn, pain), bleeding signs, unexplained anemia or weight loss and pre-surgery clinical evaluation during 3 years.
The patients were classified into three groups based on current exposure to medications of interest: ASA=aspirin, NSAIDs=non-steroidal anti-inflammatory drugs and control group.

RESULTS The most frequent NSAIDs used were
diclofenac and ketoprofen.Low-dose aspirin represented 75 or 100
or 125 mg daily.We excluded patients taking combinations
of these.

Demographical characteristics of studied group
681; 47.92%740; 52.08%
Feminin
Masculin
< 20 years 21 - 40 years
41 - 60 years
61 - 80 years
> 80 years0
100
200
300
400
500
600
700
2
312
649
428
30
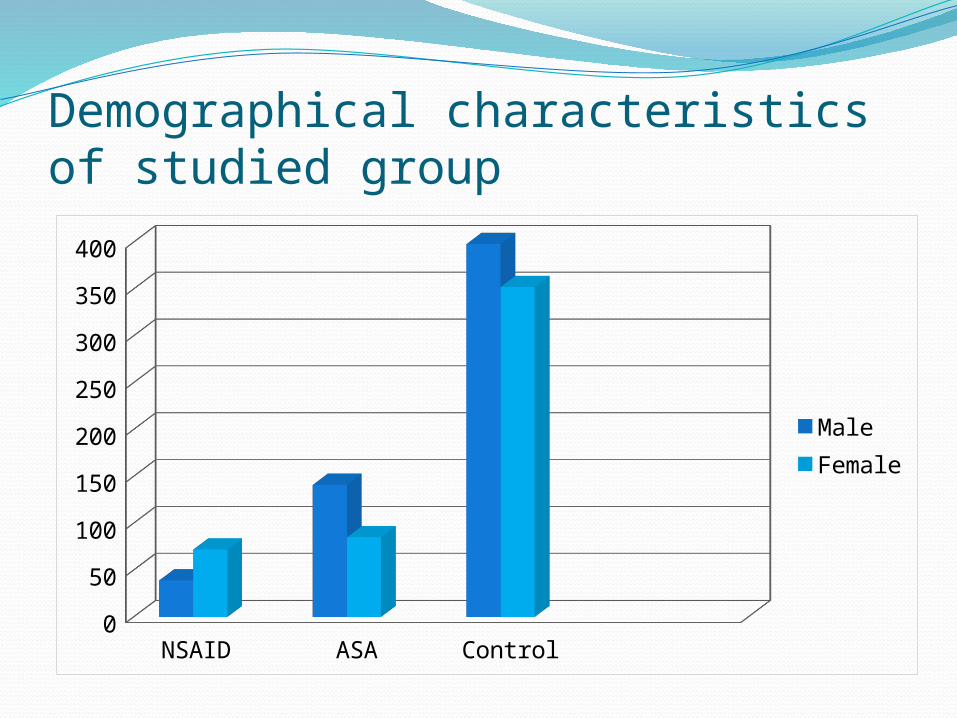
Demographical characteristics of studied group
NSAID ASA Control0
50
100
150
200
250
300
350
400
MaleFemale

SYMPTOMS NSAIDs groupN=111
p ASA groupN=226
p Control groupN=750
Epigastric pain
65,7% 0,02 45,1% 0,020 54%
Heartburn 37,8% 0,05 21,2% 0,03 28,5%
Nausea/vomiting
23,4% 0,07 14,6% 0,6 16%
Melaena 8,1% 0,06 4,4% 0,7 3,7 %
Anemia 35,1% <0,0001
16,3% 0,2 13,3%
Epigastric pain Heartburn Nausea/vomiting Melena Anemia0
50
100
150
200
250
300
350
400
450
7342 26 9
39
102
48 3310
37
405
214
120
28
100
NSAIDs group N=111ASA group N=226Control group N=750

Endoscopic findingsNSAIDs group N=111
p ASA group N=226
p Control group N=750
Gastric and/or duodenal ulcers
17,1% 0,02 12,3% 0,2 9,4%
Bleeding signs 18,% 0,008 8,8% 0,6 7,7%
Erosive gastritis 24,3% <0,0001
23,4% <0,0001
10,2%
NSAIDs group N=111 ASA group N=226 Control group N=7500
10
20
30
40
50
60
70
80
19
28
71
20 20
58
27
53
77Gastric and/or duodenal ulcersBleeding signsErosive gastritis

Histological aspectsNSAIDs groupN=111
ASA groupN=226
Control groupN=750
H. pylori infection 44,1%; p=0,01
34%; p=0,6 32,2%
Chronic gastritis 23,4% 21,6% 22,6%
Gastric atrophy/intestinal metaplasia
9,9%; p=0,02
20,3%; p=0,7
19%
H. pylori infection Chronic gastritis Gastric atrophy/intestinal metaplasia
0
50
100
150
200
250
4926
11
7749 46
242
170143
NSAIDs group N=111
ASA group N=226

CONCLUSION Long-term therapy with aspirin is very frequent in patients
referred for endoscopic evaluation, but the patients have less frequent digestive symptoms.
Patients treated with NSAID therapy have more frequent digestive symptoms and anemia comparative with patients not taking gastrotoxic medication.
Gastrointestinal toxicity was higher in patients taking NSAID who presented more frequent ulcer and bleeding signs on endoscopy, possibly correlated with high prevalence of H. pylori infection in this group.
The aspirin consumers do not have in our population more severe endoscopic lesions than control group, may due to selection criteria (patients screened before surgery without symptoms)

Thank you for your attention!