correlation between p53, c-erbb-2, and topoisomerase ii? expression, dna ploidy, hormonal receptor...
TRANSCRIPT

J. Pathol. 187: 207–216 (1999)
CORRELATION BETWEEN p53, c-erbB-2, ANDTOPOISOMERASE IIá EXPRESSION, DNA PLOIDY,
HORMONAL RECEPTOR STATUS ANDPROLIFERATION IN 356 NODE-NEGATIVE BREAST
CARCINOMAS: PROGNOSTIC IMPLICATIONS
1*, ̊ 2, 3, 1, 1, 2,̊ ̈2, 1 2
1Departments of Pathology and Haematopathology, University of Kiel, Kiel, Germany2South Swedish Breast Cancer Group, Departments of Pathology and Oncology, University Hospital, Lund, Sweden
3Department of Gynaecology, University of Kiel, Kiel, Germany
SUMMARY
Various new prognostic indicators have been identified for mammary carcinomas, but the issue of their significance remains unsettled.The prognostic impact of p53, c-erbB-2, and topoisomerase IIá expression was investigated in relation to standard prognostic factors forcarcinomas of the breast and to the tumour cell growth fraction. Paraffin-embedded specimens of 356 node-negative infiltrating ductalcarcinomas were stained immunohistochemically using a polyclonal antiserum to c-erbB-2, and the monoclonal antibodies DO-1 (p53),Ki-S4 (topoisomerase IIá), and Ki-S5 (Ki-67). The patients were followed for a median duration of 99 months. Both p53 and c-erbB-2were significantly associated with high tumour grade, large tumour size, DNA aneuploidy, lack of steroid hormone receptors, young age,and increased topoisomerase IIá and Ki-67 expression levels. The correlation of p53 and c-erbB-2 was not significant. TopoisomeraseIIá and Ki-67 scores closely paralleled each other, indicating that both reflect the proliferative activity of tumour cells. A univariateanalysis of overall (OS), specific (SS), and disease-free survival (DFS) revealed all the above-mentioned parameters to be statisticallysignificant except patient age, which was relevant only to overall survival. Multivariate analysis with inclusion of all covariates selectedtumour size and proliferation (topoisomerase IIá and Ki-67) indices as independent predictors of survival in all three models. Noadditional information was gained by p53 or c-erbB-2. It is concluded that the proliferative activity, as assessed by topoisomerase IIáor Ki-67 immunostaining, is the most useful indicator of breast cancer prognosis, except for tumour size. Copyright ? 1999 John Wiley& Sons, Ltd.
KEY WORDS—breast cancer; prognosis; proliferation; p53; c-erbB-2; Ki-67; topoisomerase IIá
INTRODUCTION
Molecular markers, notably p53 and c-erbB-2, andproliferation characteristics (reviewed in ref. 1) haverecently received growing attention as prognostic indi-cators for breast carcinoma. Mutations and deletionsof the p53 gene are relatively common in mammarycarcinomas2 and appear to occur early in carcino-genesis.3 Most of them result in abrogation of thegrowth inhibitory or apoptotic potential of the encodedprotein and thus facilitate unrestrained proliferation andprogressive genomic instability (reviewed in refs 4 and5). HER-2/neu, the gene coding for c-erbB-2, a tyrosinekinase receptor sharing sequence homologies with theepidermal growth factor receptor (EGFR),6 is frequentlyamplified in ductal carcinomas of the breast,7,8 whichappears to be associated with a more aggressive behav-iour of the tumours.6,9–11 The HER-2/neu gene is locatedon chromosome 17q2112,13 near the locus encoding fortopoisomerase IIá,14 and co-amplifications of both geneshave been reported.15 This is of dual interest in breastcancer pathology. High topoisomerase IIá expression
*Correspondence to: Pierre Rudolph, MD, Department ofPathology, University of Kiel, Michaelisstrasse 11, 24105 Kiel,Germany. E-mail: [email protected]
CCC 0022–3417/99/020207–10$17.50Copyright ? 1999 John Wiley & Sons, Ltd.
levels have been found to correlate with rapid tumourprogression and adverse prognosis.16 The enzyme is alsothe target of a group of cytotoxic drugs includingepirubicin, doxorubicin, and mitomycin C, which areincreasingly applied in breast cancer chemotherapy,17
and its expression might serve to predict the success ofadjuvant cytotoxic therapy.18
By means of immunohistochemistry, rapid screeningfor these three proteins is possible. The antibody DO-1recognizes both wild-type and mutant p53. The wild-type protein is rapidly degraded due to complexing withMdm2, for which it acts as a transactivator.19 In thisway, the levels of wild-type p53 generally remain belowthe threshold of immunoreactivity, whereas mutantforms tend to accumulate. p53 immunopositivity,although not necessarily linked to a gene mutation,2may therefore be indicative of an impaired transcrip-tional activity, or a deficiency of downstream effectors.Similarly, c-erbB-2 overexpression does not equate toHER-2/neu amplification, but the biological effect ofc-erbB-2 is likely to depend on the actual protein con-tent.20 Topoisomerase IIá expression may be monitoredby means of recently characterized monoclonal anti-bodies,21 of which Ki-S4 has been found to yield theclearest and best reproducible immunostaining results.
Received 19 March 1998Revised 3 July 1998
Accepted 21 August 1998
208
Our study was designed to compare these parameterswith standard prognostic indicators for invasivecarcinomas of the breast, and DNA ploidy and theproliferation fraction as additional covariates. The latterwas assessed by means of the monoclonal antibodyKi-S5 (Ki-67).22,23 Node-negative cases exclusively wereconsidered the most informative because these are thepatients who stand to benefit most from a refinement ofprognostic criteria.24 All parameters were evaluated inunivariate analysis with respect to overall (OS), specific(SS), and disease-free survival (DFS), and a multi-variate analysis was performed to identify independentprognostic indicators and to determine their hierarchy.
MATERIALS AND METHODS
From a series of consecutive infiltrating carcinomas ofthe breast diagnosed between March 1970 and January1986 in the health-care region of southern Sweden,410 cases with histologically confirmed axillary nodenegativity were initially selected for this study. Tumoursize was defined as the maximum tumour diametermeasured on the unfixed resection specimen. All patientshad received local treatment consisting either ofmodified radical mastectomy with axillary dissection, orof conservative breast surgery with axillary dissectionand post-operative irradiation of the breast (n=131).Adjuvant endocrine treatment (30 mg of tamoxifen perday) was given in 106 cases; patients treated withadjuvant chemotherapy (n=19) were excluded from thisstudy. Further exclusion criteria were recurrent node-negative breast cancer (n=13), occurrence of distantmetastases within 2 months after primary surgery (n=3),metastasis to the breast from another primary tumour(n=1), and bilateral breast cancer with subsequent sys-temic disease (n=3). Table I lists the clinico-pathologicalcharacteristics of the 356 patients finally remaining inthe study.
Copyright ? 1999 John Wiley & Sons, Ltd.
All patients were examined clinically at least once ayear; the routine follow-up evaluations includedlaboratory analyses, radiography and mammography.The median follow-up time was 99 months (24–208months), the last update including all details being 15January 1993.
Histology
Haematoxylin and eosin (H&E)-stained sections werereviewed to select the best preserved and most represen-tative tumour areas for further analysis. Each tumourwas graded histologically according to the modifiedBloom and Richardson grading system.25 The mitoticcount (MC) was determined as described elsewhere.26
Only invasive ductal carcinomas without particularhistological subtype (NOS) were included in the study;special carcinoma types were disregarded, which mayexplain the high prevalence of grade 2 tumours in ourseries.
Steroid receptor assay
Hormone receptor analyses were performed by meansof the dextran-coated charcoal assay and Scatchardanalysis.27 In the event of improper processing, thevalues obtained were disregarded.
DNA measurements
Tissues were prepared as previously described.28 Afterpropidium iodide staining, the DNA content of indi-vidual cell nuclei was analysed by flow cytometry usingan Ortho 50H counter.29 Tumours were defined as eitherdiploid (one stemline in the G0/G1 region) or aneuploid(two or more stem-cell populations).
Immunohistochemistry
Immunohistochemical staining was performed aspreviously described.22 Antigen retrieval was effected by
Table I—Characteristics of the 356 patients with node-negative breast cancer
Median age, years (range) 62 (23–91)Menstrual status, n (%)
Premenopausal 104 (29·2)Post-menopausal 252 (70·8)
Surgical treatment, n (%)Modified radical mastectomy with axillary dissection 318 (89·3)
With post-operative radiotherapy 101 (31·8)Conservative breast surgery with axillary dissection 38 (10·7)
With post-operative radiotherapy 29 (76·3)Adjuvant endocrine therapy, n (%) 88 (24·7)Bilateral breast cancer, n (%) 18 (5·1)Median tumour diameter, mm (range) 20 (5–180)Median number of axillary lymph nodes examined (range) 9 (4–57)Median length of follow-up, months (range) 99 (24–108)No. of patients surviving without evidence of disease, n (%) 238 (66·7)Total number of events
Death due to or with advanced breast cancer, n (%) 61 (17·1)Death without clinically confirmed breast cancer, n (%) 42 (11·8)Survival with local or distant recurrence, n (%) 15 (4·2)
P. RUDOLPH ET AL.
J. Pathol. 187: 207–216 (1999)

209PROGNOSTIC INDICATORS FOR BREAST CARCINOMA
heating the slides immersed in 0·01 citric acid, pH 6·0,for 45 min in a microwave oven at maximum power. Allantibodies were incubated on the sections for 30 minat room temperature. The antibody DO-1 (p53,Dianova, Hamburg, Germany) was diluted 1:50 andKi-S4 (topoisomerase IIá) and Ki-S5 (Ki-67) were usedundiluted as lyophilized cell culture supernatantsreconstituted with 5 ml of H2O. c-erbB-2 expressionwas assessed by means of a polyclonal anti-peptideantiserum (DAKO) at a 1:100 dilution. The immuno-reactions were enhanced by means of the streptavidin–biotin–peroxidase technique with a rabbit anti-mouseantibody, followed by counterstaining with Mayer’shaematoxylin.
A colonic carcinoma specimen with known p53immunoreactivity served as a positive control for p53immunostaining. Tonsil samples from our routinefiles were used as positive controls for Ki-67 and topo-isomerase IIá, and as negative controls for p53 andc-erbB-2.
Evaluation of immunoreactivity scores
All slides were read by two experienced pathologists.Only unequivocal nuclear staining was accepted as apositive reaction for p53, topoisomerase IIá, or Ki-67.For c-erbB-2, staining of the cell membranes was con-sidered exclusively.30 p53 reactivity was assessed in asemi-quantitative manner using the following categories:", <10 per cent positive nuclei; +, 10–50 per centpositive nuclei; + +, 51–80 per cent positive nuclei; and+ + +, >80 per cent positive nuclei. Membrane-boundc-erbB-2 staining was classified analogously. Topoi-somerase IIá and Ki-67 scores were determined bycounting a minimum of 1000 tumour cells. The labellingindex was expressed as the percentage of positive cells.
Statistical analysis
The SPSS statistical software package was used forall calculations. All covariates were analysed as bothcontinuous and discrete variables whenever possible.Correlations were computed by means of the Spearmanrank-correlation coefficient, the Kruskal–Wallis non-parametric analysis of variance, or the chi-square test.
Survival was expressed as the number of months fromthe date of primary surgery to the occurrence of an eventand was analysed in three ways: an overall survival (OS),based on all deaths regardless of their cause; as specificsurvival (SS), based on deaths due to or with advancedbreast cancer; and as disease-free survival (DFS), basedon the clinical confirmation of distant, regional, or localrecurrence. Cumulative survival probabilities werecomputed by means of the Kaplan–Meier method. Dif-ferences between the survival functions were assessed bythe Mantel–Haenszel log-rank test.
Oestrogen and progesterone receptor expression wasconsidered negative if the protein content was below10 fmol/mg. p53 was assumed to be overexpressed ifthere were §10 per cent positive nuclei, as proposed ina previous study.31 Tumours were classified as eithernegative or positive for c-erbB-2, regardless of the
Copyright ? 1999 John Wiley & Sons, Ltd.
staining intensity and the percentage of reactive cells.For topoisomerase IIá and Ki-67 scores, cut-off pointswere selected at 20 and 25 per cent, respectively, accord-ing to the median values rounded off to the nearest 5 percent. As to patient age, three groups corresponding to<50, 50–74, and §75 years were formed in accordancewith earlier studies.32,33
Multivariate analysis was performed using the Coxmultiple hazards model. Covariates were selected in astepwise (forward conditional) fashion with use of themaximum likelihood ratio. A p value of 0·05 in theunivariate analysis was adopted as the limit for inclusionas a covariate in the multivariate model. Cases with anymissing values were excluded.
RESULTS
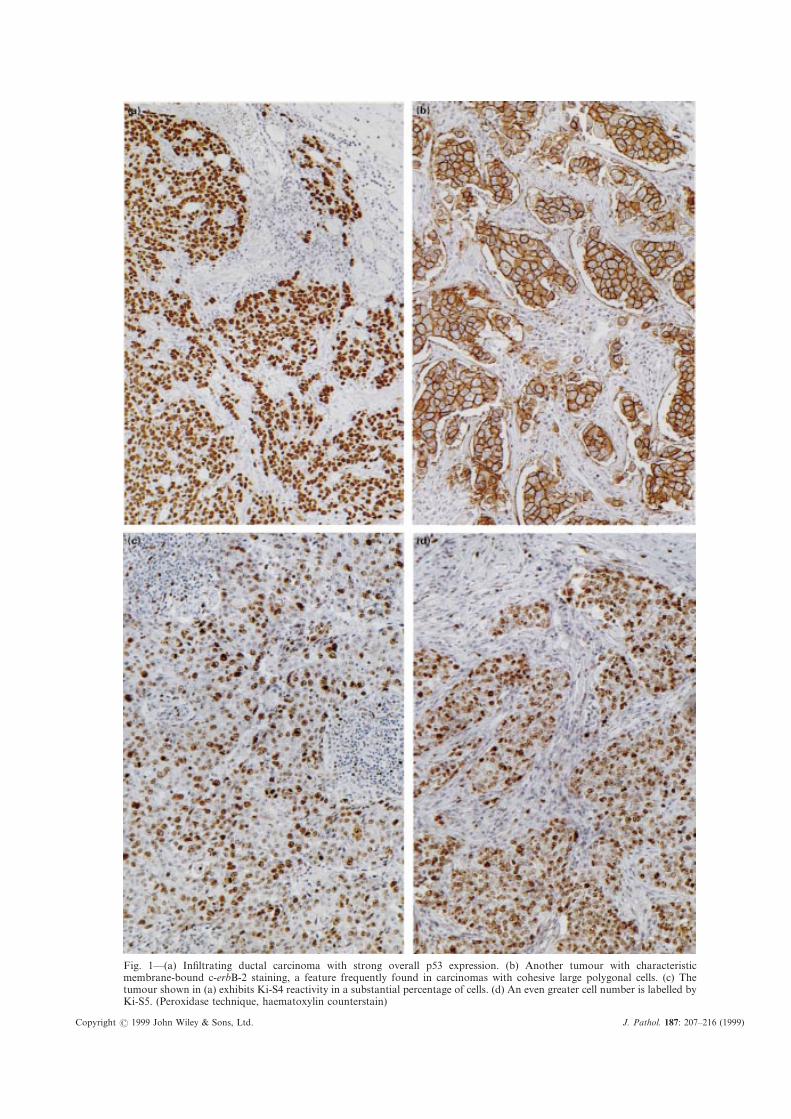
Intra-observer and inter-observer reproducibility inthe evaluation of immunostaining was at least 95 percent. One hundred and six cases (29·8 per cent) stainedpositively for p53 (Fig. 1a) and 132 (37·1 per cent) forc-erbB-2. Whereas there were few variations in theintensity of p53 immunolabelling, the staining forc-erbB-2 was, as a rule, more intense in tumours with ahigh percentage of positive cells (Fig. 1b). The meanimmunolabelling index for topoisomerase IIá (Fig. 1c)was 18·7&13·4 per cent (median 18, range 1·5–84 percent), and for Ki-67 (Fig. 1d) 24·7&16·4 per cent(median 23, range 3–93 per cent). One hundred andseventy-five tumours were DNA diploid and 167aneuploid.
Correlation of covariates
p53 overexpression strongly correlated with hightumour grade (p<0·00005), high MC (p<0·00005), largetumour size (p=0·00007), DNA aneuploidy (p=0·0005),increased topoisomerase IIá expression (p<0·00005,Table II) and high Ki-67 scores (p<0·00005, Table II),and to a lesser extent with premenopausal status(p=0·0138). An inverse relationship was found withpatient age (p=0·0071) and steroid hormone receptor
Table II—Mean values and standard deviations of topo-isomerase IIá and Ki-67 immunoreactivity scores in tumourswith different degrees of c-erbB-2 and p53 reactivity (" =<10per cent; + =10–50 per cent + + =51–80 per cent; + + + =>80per cent positive cells). The differences between individualsubgroups are statistically significant (p<0·001)
Topoisomerase IIá Ki-67
c-erbB-2 " 15·7&13·1 20·0&14·9erbB-2 + 17·5&10·9 24·1&14·4erbB-2 + + 19·8&14·1 26·8&17·1erbB-2 + + + 25·9&11·0 32·8&13·9
p53 " 15·4&11·5 20·4&14·2+ 21·7&12·1 29·3&16·4+ + 26·0&14·7 32·2&12·7+ + + 29·2&12·8 39·4&14·4
J. Pathol. 187: 207–216 (1999)
Copyright
Fig. 1—(a) Infiltrating ductal carcinoma with strong overall p53 expression. (b) Another tumour with characteristicmembrane-bound c-erbB-2 staining, a feature frequently found in carcinomas with cohesive large polygonal cells. (c) Thetumour shown in (a) exhibits Ki-S4 reactivity in a substantial percentage of cells. (d) An even greater cell number is labelled byKi-S5. (Peroxidase technique, haematoxylin counterstain)
? 1999 John Wiley & Sons, Ltd. J. Pathol. 187: 207–216 (1999)
211PROGNOSTIC INDICATORS FOR BREAST CARCINOMA
content (p<0·00005), whereas there was no associationwith c-erbB-2 expression (p=0·38).
c-erbB-2 immunoreactivity was associated with hightopoisomerase IIá and Ki-67 labelling indices(p<0·00005, Table II), high MC (p=0·0001), hightumour grade (p=0·0061), increased tumour size(p=0·0351), and DNA aneuploidy (p=0·0361), but notwith patient age (p=0·13) or menopausal status (p=0·9).There was a negative correlation with oestrogen(p=0·0042) and progesterone (p=0·0011) receptorcontent.
Topoisomerase IIá and Ki-67 scores were closelycovariant (r=0·88, p<0·0000005). Both were positivelyassociated with MC (p<0·00005), tumour grade(p<0·00005), DNA ploidy status (p<0·00005), andtumour size (r=0·21 and 0·19, p=0·000075 and0·000429, respectively), and negatively with patient age(r= "0·32, p<0·00005), menopausal status (p¦0·0002),oestrogen (r= "0·35, p<0·00005) and progesteronereceptor content (r= "0·22, p=0·000048 and 0·00043,respectively).
Oestrogen and progesterone receptors were intimatelyassociated with one another (r=0·6, p<0·0000005). Bothwere inversely correlated with tumour size (r= "0·14and "0·11, p=0·0059 and 0·0324, respectively) andtumour grade (p¦0·00009). However, whereas theoestrogen receptor content was significantly associatedwith patient age (r=0·29, p<0·0000005) and menopausalstatus (p<0·00005), progesterone receptor expressionshowed no such correlation (p=0·7 and 0·35, respect-ively). Neither oestrogen nor progesterone receptorsshowed an association with ploidy status (p>0·25).
DNA aneuploidy was associated with higher tumourgrades (p=0·0005) and higher MCs (p<0·00005), but notwith tumour size, menopausal status or patient age(p>0·15). Tumour grade was weakly associated withtumour size (p=0·0121) and premenopausal status(p=0·0356), and showed a strong inverse correlationwith patient age (p=0·0002).
In addition, the ratio of topoisomerase IIá to Ki-67expression was calculated for each tumour as thequotient of the first labelling index divided by thesecond. When this new variable was broken down byany of the other parameters, notably p53 and c-erbB-2,the means and medians of the so-formed subgroups werevirtually identical.
Survival analysis
As of the last follow-up, 61 patients (17·1 per cent)had died of breast cancer, 42 (11·8 per cent) of othercauses, and 15 (4·2 per cent) were alive with residualdisease.
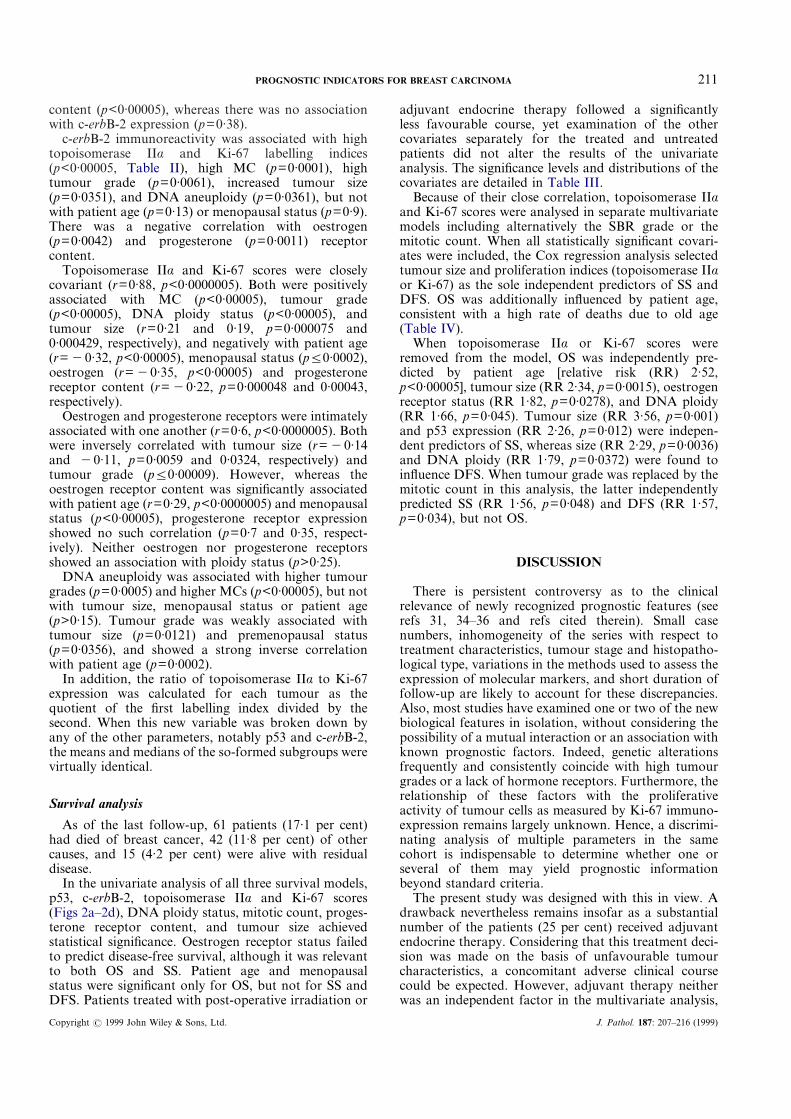
In the univariate analysis of all three survival models,p53, c-erbB-2, topoisomerase IIá and Ki-67 scores(Figs 2a–2d), DNA ploidy status, mitotic count, proges-terone receptor content, and tumour size achievedstatistical significance. Oestrogen receptor status failedto predict disease-free survival, although it was relevantto both OS and SS. Patient age and menopausalstatus were significant only for OS, but not for SS andDFS. Patients treated with post-operative irradiation or
Copyright ? 1999 John Wiley & Sons, Ltd.
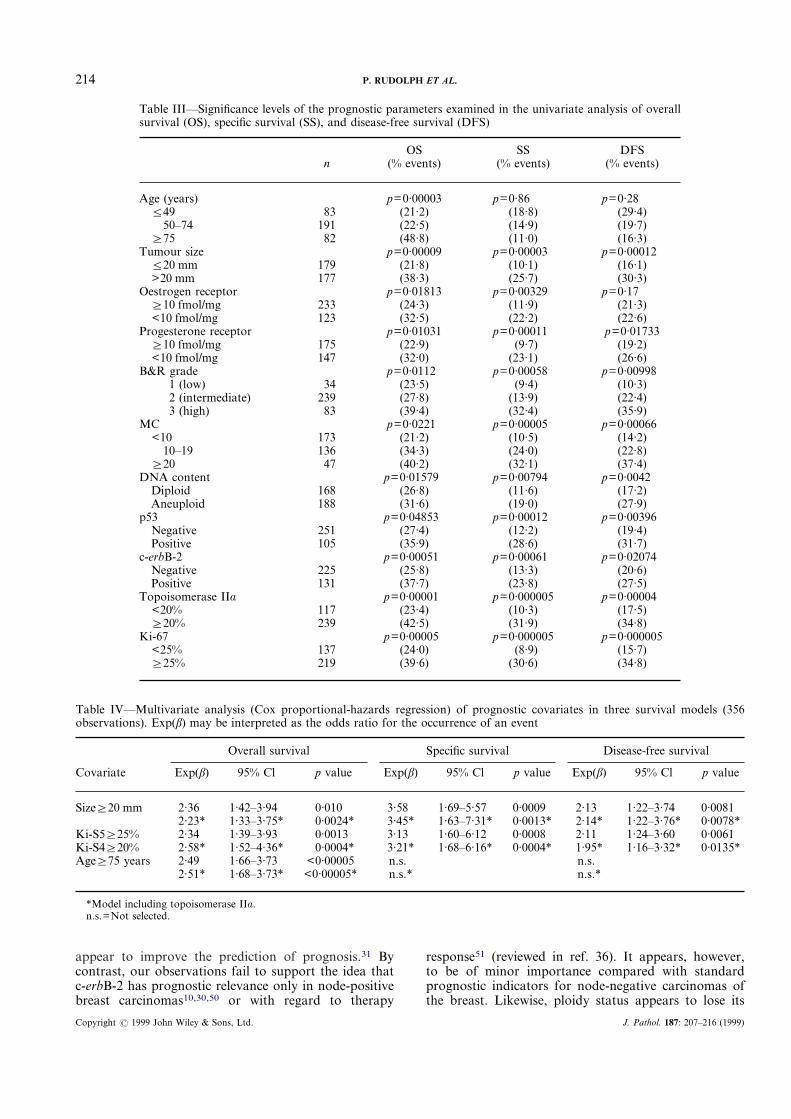
adjuvant endocrine therapy followed a significantlyless favourable course, yet examination of the othercovariates separately for the treated and untreatedpatients did not alter the results of the univariateanalysis. The significance levels and distributions of thecovariates are detailed in Table III.
Because of their close correlation, topoisomerase IIáand Ki-67 scores were analysed in separate multivariatemodels including alternatively the SBR grade or themitotic count. When all statistically significant covari-ates were included, the Cox regression analysis selectedtumour size and proliferation indices (topoisomerase IIáor Ki-67) as the sole independent predictors of SS andDFS. OS was additionally influenced by patient age,consistent with a high rate of deaths due to old age(Table IV).
When topoisomerase IIá or Ki-67 scores wereremoved from the model, OS was independently pre-dicted by patient age [relative risk (RR) 2·52,p<0·00005], tumour size (RR 2·34, p=0·0015), oestrogenreceptor status (RR 1·82, p=0·0278), and DNA ploidy(RR 1·66, p=0·045). Tumour size (RR 3·56, p=0·001)and p53 expression (RR 2·26, p=0·012) were indepen-dent predictors of SS, whereas size (RR 2·29, p=0·0036)and DNA ploidy (RR 1·79, p=0·0372) were found toinfluence DFS. When tumour grade was replaced by themitotic count in this analysis, the latter independentlypredicted SS (RR 1·56, p=0·048) and DFS (RR 1·57,p=0·034), but not OS.
DISCUSSION
There is persistent controversy as to the clinicalrelevance of newly recognized prognostic features (seerefs 31, 34–36 and refs cited therein). Small casenumbers, inhomogeneity of the series with respect totreatment characteristics, tumour stage and histopatho-logical type, variations in the methods used to assess theexpression of molecular markers, and short duration offollow-up are likely to account for these discrepancies.Also, most studies have examined one or two of the newbiological features in isolation, without considering thepossibility of a mutual interaction or an association withknown prognostic factors. Indeed, genetic alterationsfrequently and consistently coincide with high tumourgrades or a lack of hormone receptors. Furthermore, therelationship of these factors with the proliferativeactivity of tumour cells as measured by Ki-67 immuno-expression remains largely unknown. Hence, a discrimi-nating analysis of multiple parameters in the samecohort is indispensable to determine whether one orseveral of them may yield prognostic informationbeyond standard criteria.
The present study was designed with this in view. Adrawback nevertheless remains insofar as a substantialnumber of the patients (25 per cent) received adjuvantendocrine therapy. Considering that this treatment deci-sion was made on the basis of unfavourable tumourcharacteristics, a concomitant adverse clinical coursecould be expected. However, adjuvant therapy neitherwas an independent factor in the multivariate analysis,
J. Pathol. 187: 207–216 (1999)

212 P. RUDOLPH ET AL.
Copyright ?
Fig. 2—(a)–(c).
1999 John Wiley & Sons, Ltd. J. Pathol. 187: 207–216 (1999)

213PROGNOSTIC INDICATORS FOR BREAST CARCINOMA
nor did it have a sizeable influence on the results of theunivariate analysis when used as strata, which arguesagainst a significant bias due to endocrine treatment.
The prevalence of p53 expression in our series iswithin the range generally reported (reviewed in ref. 35).Its strong association with unfavourable tumour charac-teristics may well reflect a loss of the checkpoint controlfunction of p53, resulting in an accumulation of geneticdefects37 that promote an aggressive phenotype, withhigh prevalence in young patients.38 Because wild-typep53 negatively regulates the minimal promoter fortopoisomerase IIá,39 alterations of p53 would also beconsistent with an increased transcription of topoi-somerase IIá mRNA and a concomitant augmentationof its protein levels (Table II) that might entail a growthadvantage.21
In contrast to other investigators,31,40,41 we found nosignificant correlation between p53 and c-erbB-2, whichsuggests that the expression of the two proteins is causedby independent genetic mechanisms. Nevertheless, thecorrelation of c-erbB-2 with tumour grade, tumour size,aneuploidy, and low hormone receptor expression wascomparable to that described in other studies.9,42,43 Theassociation of increasing immunoreactivity levels witha proportional augmentation of topoisomerase IIáexpression (Table II) might point to a co-amplificationof the neighbouring genes encoding for the two pro-teins.15 However, because topoisomerase IIá levelswere paralleled by Ki-67 scores, the changes mayalso merely reflect a variation of the proliferativeactivity, since c-erbB-2 expression facilitates steroidhormone-independent growth in breast carcinomacells.44
Despite contradictory reports concerning its prog-nostic significance for node-negative breast carcinoma(see refs 45, 46 and refs cited therein), the DNA content
Copyright ? 1999 John Wiley & Sons, Ltd.
was of interest, because aneuploidy may be associatedwith aberrations involving chromosome 17,47 whichcontains the loci encoding for p53, c-erbB-2, andtopoisomerase IIá. These tumours also exhibited anincreased rate of c-erbB-2 amplification and p53 inacti-vation.47 Similar mechanisms might explain the signifi-cantly higher proliferative activity in our aneuploidcases.
Topoisomerase IIá scores were directly proportionalto the Ki-67 index at a ratio of approximately 0·75:1.This indicates that topoisomerase IIá expression isessentially related to the proliferative activity21,48 andthat its levels do not vary independently from those ofKi-67 within a given cell population. The lower topoi-somerase IIá labelling indices may be due to assaysensitivity, because in a major part of the G1 phase, theenzyme content may be too low49 to be detected byimmunohistochemistry. Both parameters were stronglyassociated with p53 and c-erbB-2 expression, DNAaneuploidy and standard indicators of poor prognosis,suggesting that, regardless of their nature, unfavour-able characteristics are mirrored by an increase of theproliferative activity.
The close correlations between most of the covariatesin this study further underscore the necessity of amultivariate analysis. In the Cox regression analysis,topoisomerase IIá or Ki-67 indices together with tumoursize were retained as the only independent prognosticfactors with respect to SS and DFS. Patient age §75years additionally portended a reduced OS, due to ahigh rate of disease-unrelated deaths in elderly patients.
Our results concerning the significance of p53 ex-pression are well in line with the few multivariateanalyses that included the assessment of immunohisto-chemical Ki-67 markers in archival material.31 Interest-ingly, molecular analysis of p53 mutations does not
Fig. 2—(d).
Fig. 2—Kaplan–Meier analysis of specific survival with respect to p53 (a), c-erbB-2 (b), topoisomerase IIá (c), andKi-67 expression (d). Although both p53 and c-erbB-2 are statistically significant, a better discrimination betweenlow-risk and high-risk groups is achieved by Ki-S4 and Ki-S5
J. Pathol. 187: 207–216 (1999)
214
appear to improve the prediction of prognosis.31 Bycontrast, our observations fail to support the idea thatc-erbB-2 has prognostic relevance only in node-positivebreast carcinomas10,30,50 or with regard to therapy
Copyright ? 1999 John Wiley & Sons, Ltd.
response51 (reviewed in ref. 36). It appears, however,to be of minor importance compared with standardprognostic indicators for node-negative carcinomas ofthe breast. Likewise, ploidy status appears to lose its
Table III—Significance levels of the prognostic parameters examined in the univariate analysis of overallsurvival (OS), specific survival (SS), and disease-free survival (DFS)
nOS
(% events)SS
(% events)DFS
(% events)
Age (years) p=0·00003 p=0·86 p=0·28¦49 83 (21·2) (18·8) (29·4)
50–74 191 (22·5) (14·9) (19·7)§75 82 (48·8) (11·0) (16·3)
Tumour size p=0·00009 p=0·00003 p=0·00012¦20 mm 179 (21·8) (10·1) (16·1)>20 mm 177 (38·3) (25·7) (30·3)
Oestrogen receptor p=0·01813 p=0·00329 p=0·17§10 fmol/mg 233 (24·3) (11·9) (21·3)<10 fmol/mg 123 (32·5) (22·2) (22·6)
Progesterone receptor p=0·01031 p=0·00011 p=0·01733§10 fmol/mg 175 (22·9) (9·7) (19·2)<10 fmol/mg 147 (32·0) (23·1) (26·6)
B&R grade p=0·0112 p=0·00058 p=0·009981 (low) 34 (23·5) (9·4) (10·3)2 (intermediate) 239 (27·8) (13·9) (22·4)3 (high) 83 (39·4) (32·4) (35·9)
MC p=0·0221 p=0·00005 p=0·00066<10 173 (21·2) (10·5) (14·2)
10–19 136 (34·3) (24·0) (22·8)§20 47 (40·2) (32·1) (37·4)
DNA content p=0·01579 p=0·00794 p=0·0042Diploid 168 (26·8) (11·6) (17·2)Aneuploid 188 (31·6) (19·0) (27·9)
p53 p=0·04853 p=0·00012 p=0·00396Negative 251 (27·4) (12·2) (19·4)Positive 105 (35·9) (28·6) (31·7)
c-erbB-2 p=0·00051 p=0·00061 p=0·02074Negative 225 (25·8) (13·3) (20·6)Positive 131 (37·7) (23·8) (27·5)
Topoisomerase IIá p=0·00001 p=0·000005 p=0·00004<20% 117 (23·4) (10·3) (17·5)§20% 239 (42·5) (31·9) (34·8)
Ki-67 p=0·00005 p=0·000005 p=0·000005<25% 137 (24·0) (8·9) (15·7)§25% 219 (39·6) (30·6) (34·8)
P. RUDOLPH ET AL.
Table IV—Multivariate analysis (Cox proportional-hazards regression) of prognostic covariates in three survival models (356observations). Exp(â) may be interpreted as the odds ratio for the occurrence of an event
Covariate
Overall survival Specific survival Disease-free survival
Exp(â) 95% Cl p value Exp(â) 95% Cl p value Exp(â) 95% Cl p value
Size§20 mm 2·36 1·42–3·94 0·010 3·58 1·69–5·57 0·0009 2·13 1·22–3·74 0·00812·23* 1·33–3·75* 0·0024* 3·45* 1·63–7·31* 0·0013* 2·14* 1·22–3·76* 0·0078*
Ki-S5§25% 2·34 1·39–3·93 0·0013 3·13 1·60–6·12 0·0008 2·11 1·24–3·60 0·0061Ki-S4§20% 2·58* 1·52–4·36* 0·0004* 3·21* 1·68–6·16* 0·0004* 1·95* 1·16–3·32* 0·0135*Age§75 years 2·49 1·66–3·73 <0·00005 n.s. n.s.
2·51* 1·68–3·73* <0·00005* n.s.* n.s.*
*Model including topoisomerase IIá.n.s.=Not selected.
J. Pathol. 187: 207–216 (1999)

215PROGNOSTIC INDICATORS FOR BREAST CARCINOMA
prognostic strength if proliferation parameters areincluded in the analysis. Despite the comparatively highsignificance of the mitotic count, immunohistochemicalproliferation indices appear to be a more accurate gaugeof tumour growth.
In accordance with a few earlier studies,31,52–55 mostof which examined much smaller series, our investi-gation highlights the primordial biological importanceof the proliferative activity in infiltrating carcinomas ofthe breast, regardless of whether it is measured bytopoisomerase IIá or Ki-67 immunoexpression. Itsimpact apparently remains verified irrespective of thecut-off points selected. In a series with a median Ki-67staining index comparable to ours, Pinder et al.,reported a significant correlation with survival by usingthe tertiles as cut-off points.55 We, nevertheless, pre-ferred a dichotomization by the approximated medianto avoid an intermediate risk category of questionableusefulness.
Apparently, no additional information can be gainedfrom p53 or c-erbB-2 expression. Indeed, while thenumerous factors related to the evolution of mammarycarcinomas exhibit complex interactions, genetic alter-ations as well as clinical and histological parametersappear to culminate in an increase of the proliferativeactivity, which may therefore be considered the sum ofall effects. This would explain the fact that the prolifer-ation fraction is the single most important independentprognostic factor for node-negative breast carcinoma,except for tumour size. As the latter may become lessinfluential owing to improved screening procedures,immunohistochemical proliferation markers maybecome major determinants of treatment protocols.Molecular markers, such as p53 and c-erbB-2 mightmerit reconsideration if individual genetic alterationscan be targeted by means of specific therapies.56 Untilthis is realized, immunohistochemical proliferationmeasurements appear to be the most practical andreliable means for predicting breast cancer prognosis.
REFERENCES
1. Landberg G, Roos G. The cell cycle in breast cancer. APMIS 1997; 105:575–589.
2. Caleffi M, Teague MW, Jensen RA, Vnencak-Jones CL, Dupont WD, ParlFF. p53 gene mutations and steroid receptor status in breast cancer.Clinicopathologic correlations and prognostic assessment. Cancer 1994; 73:2147–2156.
3. Lizard-Nacol S, Riedinger JM, Lizard G, et al. Loss of heterozygosity at theTP53 gene: independent occurrence from genetic instability events innode-negative breast cancer. Int J Cancer 1997; 72: 599–603.
4. Levine AJ, Perry ME, Chang A, et al. The 1993 Walter Hubert Lecture: therole of the p53 tumour-suppressor gene in tumorigenesis. Br J Cancer 1994;69: 409–416.
5. Parwaresch R, Rudolph P. The cell cycle—theory and applications tocancer. Onkologie 1996; 19: 464–472.
6. Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL.Human breast cancer: correlation of relapse and survival with amplificationof the HER-2/neu oncogene. Science 1987; 235: 177–182.
7. Slamon DJ. Studies of the HER-2/neu proto-oncogene in human breastcancer. Cancer Invest 1990; 8: 253.
8. Inglehart JD, Kraus MH, Langton BC, Huper G, Kerns BJ, Marks JR.Increased erbB-2 gene copies and expression in multiple stages of breastcancer. Cancer Res 1990; 50: 6701–6707.
9. Kallioniemi OP, Holli K, Visakorpi T, Koivula T, Helin HH, Isola JJ.Association of c-erbB-2 protein over-expression with high rate of cellproliferation, increased risk of visceral metastasis and poor long-termsurvival in breast cancer. Int J Cancer 1991; 49: 650–655.
Copyright ? 1999 John Wiley & Sons, Ltd.
10. Toikkanen S, Helin H, Isola J, Joensuu H. Prognostic significance of HER-2oncoprotein expression in breast cancer: a 30-year follow-up. J Clin Oncol1992; 10: 1044–1048.
11. Quénel N, Wafflart J, Bonichon F, et al. The prognostic value of c-erbB2 inprimary breast carcinomas: a study of 942 cases. Breast Cancer Res Treat1995; 35: 283–291.
12. Coussens L, Yang-Feng TL, Liao YC, et al. Tyrosine kinase receptor withextensive homology to EGF receptor shares chromosomal location with neuoncogene. Science 1985; 230: 1132–1139.
13. Schechter AL, Hung MC, Vaidyanathan L, et al. The neu gene: anerbB-homologous gene distinct from and unlinked to the gene encoding theEGF receptor. Science 1985; 229: 976–978.
14. Tsai Pflugfelder M, Liu LF, Liu AA, et al. Cloning and sequencing ofcDNA encoding human DNA topoisomerase II and localization of the geneto chromosome region 17q21–22. Proc Natl Acad Sci USA 1988; 85:7177–7181.
15. Smith K, Houlbrook S, Greenall M, Carmichael J, Harris AL.Topoisomerase II alpha co-amplification with erbB2 in human primarybreast cancer and breast cancer cell lines: relationship to m-AMSA andmitoxanthrone sensitivity. Oncogene 1993; 8: 933–938.
16. Hellemans P, van Dam PA, Geyskens M, van Oosterom AT, Buytaert P,Van Marck E. Immunohistochemical study of topoisomerase II-alphaexpression in primary ductal carcinoma of the breast. J Clin Pathol 1995; 48:147–150.
17. Isaacs RJ, Davies SL, Wells NJ, Harris AL. Topoisomerases II alpha andbeta as therapy targets in breast cancer. Anticancer Drugs 1995; 6: 195–211.
18. Houlbrook S, Addison CM, Davies SL, et al. Relationship betweenexpression of topoisomerase II isoforms and intrinsic sensitivity totopoisomerase II inhibitors in breast cancer cell lines. Br J Cancer 1995; 72:1454–1461 (published erratum appears in Br J Cancer 1996; 74: 1154).
19. Haupt Y, Maya R, Kazaz A, Oren M. Mdm2 promotes the rapiddegradation of p53. Nature 1997; 387: 296–299.
20. Bacus SS, Zelnick CR, Plowman G, Yarden Y. Expression of the erbB-2family of growth factor receptors and their ligands in breast cancers.Implication for tumor biology and clinical behavior. Am J Clin Pathol 1994;102: S13–S24.
21. Kellner U, Heidelbrecht HJ, Rudolph P, et al. Detection of topoisomeraseII alpha in cell lines and tissues—characterization of five novel monoclonalantibodies. J Histochem Cytochem 1997; 45: 251–263.
22. Rudolph P, Lappe T, Schubert C, Schmidt D, Parwaresch RM,Christophers E. Diagnostic assessment of two novel proliferation-specificantigens in benign and malignant melanocytic lesions. Am J Pathol 1995;147: 1615–1625.
23. Heidebrecht HJ, Buck F, Haas K, Wacker HH, Parwaresch R. Monoclonalantibodies Ki-S3 and Ki-S5 yield new data on the ‘Ki-67’ proteins. CellProlif 1996; 29: 413–425.
24. McGuire WL, Clark GM. Prognostic factors and treatment decisions inaxillary-node-negative breast cancer. N Engl J Med 1992; 326: 1756–1761.
25. Elston CW, Ellis IO. Pathological prognostic factors in breast cancer. I. Thevalue of histological grade in breast cancer: experience from a large studywith long-term follow-up. Histopathology 1991; 19: 403–410.
26. van Diest PJ, Baak JP, Matze Cok P, et al. Reproducibility of mitosiscounting in 2469 breast cancer specimens: results from the MulticenterMorphometric Mammary Carcinoma Project. Hum Pathol 1992; 23:603–607.
27. Norgren A, Borg A, Ferno M, Johansson U, Lindahl B, Tsiobanelis K.Improved method for assay of estradiol and progesterone receptors withspecial reference to breast cancer. Anticancer Res 1982; 2: 315–320.
28. Thornthwaite JT, Sugarbaker EV, Temple WJ. Preparation of tissues forDNA flow cytometric analysis. Cytometry 1980; 1: 229–237.
29. Lee GM, Thornthwaite JT, Rasch EM. Pictogram per cell determination ofDNA by flow cytofluorometry. Anal Biochem 1984; 137: 221–226.
30. Tetu B, Brisson J. Prognostic significance of HER-2/neu oncoproteinexpression in node-positive breast cancer. The influence of the pattern ofimmunostaining and adjuvant therapy. Cancer 1994; 73: 2359–2365.
31. Seshadri R, Leong AS, McCaul K, Firgaira FA, Setlur V, HorsfallDJ. Relationship between p53 gene abnormalities and other tumourcharacteristics in breast-cancer prognosis. Int J Cancer 1996; 69: 135–141.
32. Host H, Lund E. Age as a prognostic factor in breast cancer. Cancer 1986;57: 2217–2221.
33. Sigurdsson H, Baldetorp B, Borg A, et al. Indicators of prognosis innode-negative breast cancer. N Engl J Med 1990; 322: 1045–1053.
34. Osborne CK. Prognostic factors for breast cancer: have they met theirpromise? J Clin Oncol 1992; 10: 679–682.
35. Rosen PP, Lesser ML, Arroyo CD, Cranor M, Borgen P, Norton L. p53 innode-negative breast carcinoma: an immunohistochemical study of epi-demiologic risk factors, histologic features, and prognosis. J Clin Oncol1995; 13: 821–830.
36. Ravdin PM, Chamness GC. The c-erbB-2 proto-oncogene as a prognosticand predictive marker in breast cancer: a paradigm for the development ofother macromolecular markers—a review. Gene 1995; 159: 19–27.
37. Lane DP. Cancer: p53, guardian of the genome. Nature 1992; 358: 15–16.38. Walker RA, Lees E, Webb MB, Dearing SJ. Breast carcinomas occurring in
young women (<35 years) are different. Br J Cancer 1996; 74: 1796–1800.
J. Pathol. 187: 207–216 (1999)

216 P. RUDOLPH ET AL.
39. Sandri MI, Isaacs RJ, Ongkeko WM, et al. p53 regulates the minimalpromoter of the human topoisomerase II alpha gene. Nucleic Acids Res1996; 24: 4464–4470.
40. Barbareschi M, Leonardi E, Mauri FA, Serio G, Palma PD. p53 andc-erbB-2 protein expression in breast carcinomas. An immunohistochemicalstudy including correlations with receptor status, proliferation markers, andclinical stage in human breast cancer. Am J Clin Pathol 1992; 98: 408–418.
41. Sirvent JJ, Salvado MT, Santafe M, et al. p53 in breast cancer. Its relationto histological grade, lymph-node status, hormone receptors, cell-proliferation fraction (Ki-67) and c-erbB-2. Immunohistochemical study of153 cases. Histol Histopathol 1995; 10: 531–539.
42. Ro JS, el-Naggar A, Ro JY, et al. c-erbB-2 amplification in node-negativehuman breast cancer. Cancer Res 1989; 49: 6941–6944.
43. Allred DC, Clark GM, Molina R, et al. Overexpression of HER-2/neu andits relationship with other prognostic factors change during the progressionof in situ to invasive breast cancer. Hum Pathol 1992; 23: 974–979.
44. Pietras RJ, Arboleda J, Reese DM, et al. HER-2 tyrosine kinase pathwaytargets estrogen receptor and promotes hormone-independent growth inhuman breast cancer cells. Oncogene 1995; 10: 2435–2446.
45. O’Reilly SM, Camplejohn RS, Barnes DM, et al. DNA index, S-phasefraction, histological grade and prognosis in breast cancer. Br J Cancer1990; 61: 671–674.
46. Aubele M, Auer G, Falkmer U, et al. Identification of a low-risk group ofstage I breast cancer patients by cytometrically assessed DNA and nucleartexture parameters. J Pathol 1995; 177: 377–384.
47. Watatani M, Nagayama K, Imanishi Y, et al. Genetic alterations onchromosome 17 in human breast cancer: relationships to clinical featuresand DNA ploidy. Breast Cancer Res Treat 1993; 28: 231–239.
Copyright ? 1999 John Wiley & Sons, Ltd.
48. Lynch BJ, Guinee DG Jr, Holden JA. Human DNA topoisomeraseII-alpha: a new marker of cell proliferation in invasive breast cancer [InProcess Citation]. Hum Pathol 1997; 28: 1180–1188.
49. Woessner RD, Mattern MR, Mirabelli CK, Johnson RK, Drake FH.Proliferation- and cell cycle-dependent differences in expression of the 170kilodalton and 180 kilodalton forms of topoisomerase II in NIH-3T3 cells.Cell Growth Differ 1991; 2: 209–214.
50. Tandon AK, Clark GM, Chamness GC, Ullrich A, McGuire WL. HER-2/neu oncogene protein and prognosis in breast cancer. J Clin Oncol 1989; 7:1120–1128.
51. Muss HB, Thor AD, Berry DA, et al. c-erbB-2 expression and response toadjuvant therapy in women with node-positive early breast cancer. N Engl JMed 1994; 330: 1260–1266.
52. Gaglia P, Bernardi A, Venesio T, et al. Cell proliferation of breast cancerevaluated by anti-BrdU and anti-Ki-67 antibodies: its prognostic value onshort-term recurrences. Eur J Cancer 1993; 29A: 1509–1513.
53. Veronese SM, Gambacorta M, Gottardi O, Scanzi F, Ferrari M,Lampertico P. Proliferation index as a prognostic marker in breast cancer.Cancer 1993; 71: 3926–3931.
54. Pietilainen T, Lipponen P, Aaltomaa S, Eskelinen M, Kosma VM, SyrjanenK. The important prognostic value of Ki-67 expression as determined byimage analysis in breast cancer. J Cancer Res Clin Oncol 1996; 122: 687–692.
55. Pinder SE, Wencyk P, Sibbering DM, et al. Assessment of the newproliferation marker MIB1 in breast carcinoma using image analysis:associations with other prognostic factors and survival. Br J Cancer 1995;71: 146–149.
56. Baringa M. From bench top to bedside. Science 1997; 278: 1036–1039.
J. Pathol. 187: 207–216 (1999)