cytokine concentration in stored canine erythrocyte concentrates
TRANSCRIPT

Original Study Journal of Veterinary Emergency and Critical Care 24(3) 2014, pp 259–263doi: 10.1111/vec.12160
Cytokine concentration in stored canineerythrocyte concentratesRaffaella Corsi, DVM; Maureen A. McMichael, DVM, DACVECC; Stephanie A. Smith, DVM, MS,DACVIM; Mauria O’Brien, DVM, DACVECC; Jennifer Herring, DVM, DACVECC; Thandeka R.Ngwenyama, DVM; Alyssa Galligan, CVT; Alison N. Beloshapka, MS; Ping Deng, MS and Kelly S.Swanson, PhD
Abstract
Objective – To evaluate the effect of leukoreduction (LR) as compared to standard nonleukoreduced (NLR)units on cytokine concentrations in canine erythrocyte concentrates during regular storage time.Design – Randomized, experimental study.Setting – University teaching hospital.Animals – Ten random-source research dogs.Interventions – One unit of whole blood was collected from each dog and randomized to standard processing(NLR, n = 5) or prestorage LR (n = 5). All units were stored at 4◦C. Samples were aseptically collected fromeach unit weekly for 5 weeks. On day 35, 1 mL of blood was collected from each unit and submitted for aerobicculture.Measurement and Main Results – An ELISA assay was used to analyze the concentrations of IL-1�, IL-8, TNF-�, and IL-10. There were no significant effects of either group or storage time for IL-1�, IL-10, or TNF-�. IL-8concentration was significantly increased over the storage period in NLR units, and was significantly highercompared to LR units on days 28 and 35. Aerobic culture was negative on all units.Conclusions – This study demonstrated a marked, storage time-dependent accumulation of IL-8 in canineerythrocyte concentrates. Prestorage LR attenuated the accumulation of IL-8. This chemokine may contributeto the proinflammatory effects of transfusion of stored erythrocyte concentrates.
(J Vet Emerg Crit Care 2014; 24(3): 259–263) doi: 10.1111/vec.12160
Keywords: dogs, inflammation, storage lesion, transfusion
Introduction
Blood transfusions are an essential part of the treat-ment for critically ill human and veterinary patients. Al-though blood cells are usually evaluated for antigeniccompatibility prior to delivery, multiple studies have
From the Department of Veterinary Clinical Sciences, College of Veteri-nary Medicine (Corsi, McMichael, Obrien, Herring, Ngwenyama, Galligan,Swanson), Department of Biochemistry, College of Medicine (Smith), andDepartment of Animal Sciences, College of Agricultural, Consumer and En-vironmental Sciences (Swanson), University of Illinois at Urbana-Cham-paign, Urbana, IL 61802
The study was performed at the University of Illinois—Urbana campus.
The authors declare no conflicts of interests.
Presented in part at the European College of Veterinary Internal MedicineCongress, Seville, Spain, September 2011.
Address correspondence and reprint requests toDr. Maureen A. McMichael, Department of Veterinary Clinical Sciences, Uni-versity of Illinois at Urbana-Champaign, 1008 West Hazelwood Dr, Urbana,IL 61802. Email: [email protected] June 07, 2012; Accepted December 29, 2013.
Abbreviations
FNHTR febrile nonhemolytic transfusion reactionsNon-LR nonleukoreductionLR leukoreductionpRBC packed RBC
documented an association between transfusion and ad-verse events in the recipient.1–5 In people with majortrauma, blood transfusion has been independently as-sociated with increased risk of infection, developmentof respiratory complications, and admission into the in-tensive care unit.1 Additionally, trauma patients whoreceived blood transfusions within 24 hours of admis-sion had a higher risk of developing systemic inflam-matory response syndrome and death.2 Length of stor-age appears to be associated with a negative impact onthe safety of blood transfusions in people.6, 7 Recently,several studies have documented an increased risk of
C© Veterinary Emergency and Critical Care Society 2014 259

R. Corsi et al.
adverse effects associated with transfusion of aged RBCs> 14 days compared with fresh RBC transfusion.8, 9
Transfusion reactions may be either immunologicor nonimmunologic in nature. Immunologic reac-tions include febrile nonhemolytic transfusion reactions(FNHTRs), transfusion-related acute lung injury andacute, and delayed hemolytic reactions. Nonimmuno-logic reactions include infectious disease transmission,electrolyte disturbances, and endotoxic shock. FNHTRsare reported with a frequency of 1-6.8% in people3 and3–5% in companion animals.4 Immunologic transfusionreactions in human recipients, in particular FNHTRs andtransfusion-related acute lung injury, are thought to be inpart related to transfusion of bioactive molecules derivedfrom leukocytes and platelets,5, 10, 11 including proinflam-matory cytokines.
Cytokines are regulatory polypeptides that are essen-tial modulators of inflammatory responses. Increasedcytokine concentrations have been documented in hu-man erythrocyte concentrates12, 13 and concentrations ofbioactive molecules have been shown to increase duringstorage.9, 14, 15
Leukoreduction (LR) is the process of removing leuko-cytes (± platelets) from collected blood prior to stor-age of erythrocytes. Removal of the major cytokine pro-ducers, WBCs, at blood collection has the potential tosignificantly decrease cytokine concentrations in the de-livered product. Use of LR attenuates the inflamma-tory response to transfusion in people16–18 and normaldogs.19 LR of canine blood decreases the formation ofprocoagulant microparticles in stored erythrocyte con-centrates, a process that is likely mediated via the ef-fects of bioactive molecules from contaminating leuko-cytes and platelets.20 Moreover, LR has been shown todecrease the accumulation of cytokines in erythrocyteconcentrates during storage of human blood.11, 12, 21–23
The objective of this study was to evaluate LR and non-LR canine erythrocyte concentrates for changes in in-flammatory cytokine concentrations during storage. Ourhypotheses were: (1) proinflammatory cytokine concen-trations would be lower in LR units as compared to non-LR units; and (2) cytokine concentrations would increaseduring storage in non-LR units, but not in LR units.
Materials and Methods
Collection of supernatant samplesThe study protocol was approved by the University ofIllinois Institutional Animal Care and Use Committee.Whole blood units were collected and processed from10 random-source healthy research dogs as describedin detail previously.20 Briefly, 420 g of whole blood wasaseptically collected via standard methods into citrate-phosphate-dextrose adenine solution. Five of the units
were subjected to LR using an inline filter systema thatremoves leukocytes and platelets. Adequate cell deple-tion (>99% reduction) was confirmed for the 5 LR units.Centrifugation and plasma removal were performed viastandard methods. Sterile sampling ports were placedin each unit to allow removal of samples (35 mL each)on days 0, 7, 14, 21, 28, and 35 of storage. Erythrocyteconcentrate aliquots were then centrifuged at 1,850 g for20 min at 4◦C without braking. The upper 2/3 of eachsupernatant was carefully removed, and aliquotted forstorage at –80◦C. Following collection of the samples onday 35, a 1 mL aliquot was obtained from each unit andsubmitted for aerobic culture.
Cytokine assaysQuantitative ELISA was used to analyze cytokine con-centrations in supernatants. A commercially availableELISA kit was used as recommended for detection ofIL-1�.b Commercially available antibody sets for canineIL-8, IL-10, and TNF-�c were utilized as recommendedby the supplier. The use of plasma samples containingblood banking anticoagulants and additives was vali-dated for the commercial ELISA kit and all 3 antibodysets. Dilutional linearity, interassay, and intraassay vari-ability, cold-spike recovery, and lower limits of detectionwere determined, and are reported in table 1.
Statistical analysisDetermination of data distribution was established usingthe Kolmogorov–Smirnov test. Cytokine concentrationsin supernatants from erythrocyte units were comparedby two-way repeated measures ANOVA with evalua-tion for an effect of both group (NLR versus LR) andstorage time (0, 7, 14, 21, 28, 35 days). For post-hocanalysis where the ANOVA established statistical sig-nificance, a Tukey test was used for pairwise compar-isons. A P value of <0.05 was considered significant.Comparisons were performed using a statistical softwareprogram.d
Results
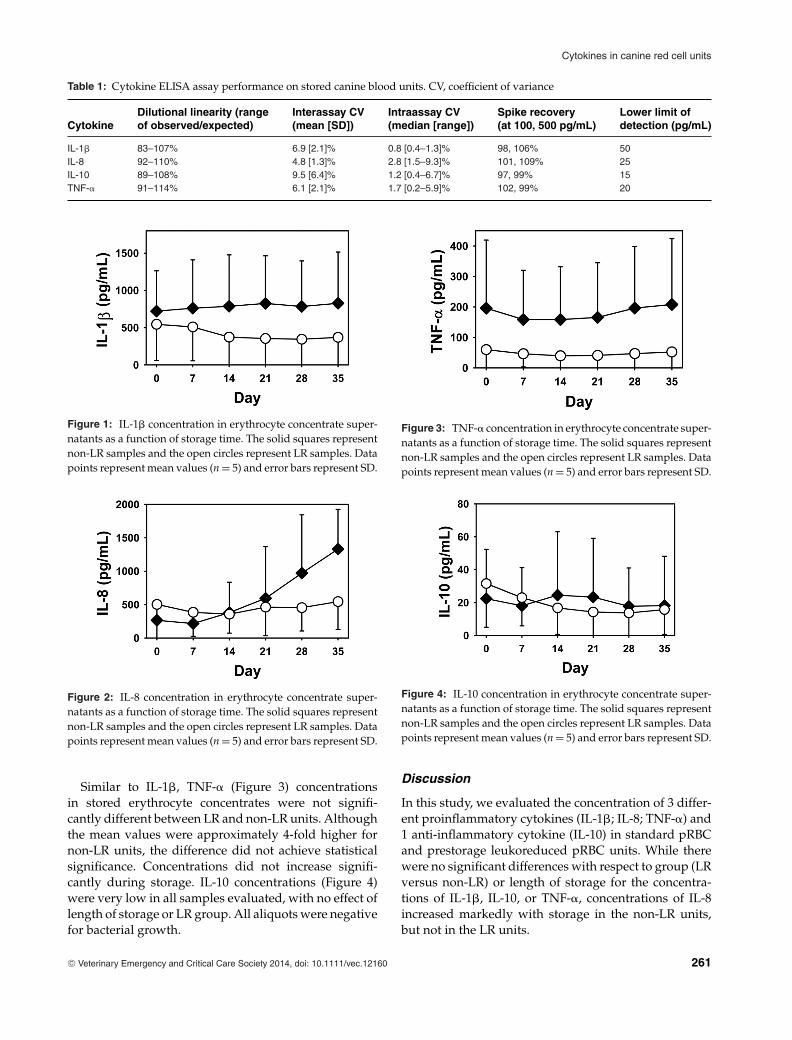
CytokinesIL-1� (Figure 1) concentrations were not significantlydifferent between LR and non-LR units. Concentrationsdid not change significantly over the storage period. IL-8 (Figure 2) concentrations in stored erythrocyte unitswere similar between non-LR and LR units on storagedays 0 thru 21, but were significantly higher in non-LRunits on days 28 and 35. IL-8 content was significantlyhigher on day 35 as compared to baseline for non-LRunits (range: 3–16-fold increase), but did not increaseover storage time in LR units.
260 C© Veterinary Emergency and Critical Care Society 2014, doi: 10.1111/vec.12160
Cytokines in canine red cell units
Table 1: Cytokine ELISA assay performance on stored canine blood units. CV, coefficient of variance
Dilutional linearity (range Interassay CV Intraassay CV Spike recovery Lower limit ofCytokine of observed/expected) (mean [SD]) (median [range]) (at 100, 500 pg/mL) detection (pg/mL)
IL-1� 83–107% 6.9 [2.1]% 0.8 [0.4–1.3]% 98, 106% 50IL-8 92–110% 4.8 [1.3]% 2.8 [1.5–9.3]% 101, 109% 25IL-10 89–108% 9.5 [6.4]% 1.2 [0.4–6.7]% 97, 99% 15TNF-� 91–114% 6.1 [2.1]% 1.7 [0.2–5.9]% 102, 99% 20
Figure 1: IL-1� concentration in erythrocyte concentrate super-natants as a function of storage time. The solid squares representnon-LR samples and the open circles represent LR samples. Datapoints represent mean values (n = 5) and error bars represent SD.
Figure 2: IL-8 concentration in erythrocyte concentrate super-natants as a function of storage time. The solid squares representnon-LR samples and the open circles represent LR samples. Datapoints represent mean values (n = 5) and error bars represent SD.
Similar to IL-1�, TNF-� (Figure 3) concentrationsin stored erythrocyte concentrates were not signifi-cantly different between LR and non-LR units. Althoughthe mean values were approximately 4-fold higher fornon-LR units, the difference did not achieve statisticalsignificance. Concentrations did not increase signifi-cantly during storage. IL-10 concentrations (Figure 4)were very low in all samples evaluated, with no effect oflength of storage or LR group. All aliquots were negativefor bacterial growth.
Figure 3: TNF-� concentration in erythrocyte concentrate super-natants as a function of storage time. The solid squares representnon-LR samples and the open circles represent LR samples. Datapoints represent mean values (n = 5) and error bars represent SD.
Figure 4: IL-10 concentration in erythrocyte concentrate super-natants as a function of storage time. The solid squares representnon-LR samples and the open circles represent LR samples. Datapoints represent mean values (n = 5) and error bars represent SD.
Discussion
In this study, we evaluated the concentration of 3 differ-ent proinflammatory cytokines (IL-1�; IL-8; TNF-�) and1 anti-inflammatory cytokine (IL-10) in standard pRBCand prestorage leukoreduced pRBC units. While therewere no significant differences with respect to group (LRversus non-LR) or length of storage for the concentra-tions of IL-1�, IL-10, or TNF-�, concentrations of IL-8increased markedly with storage in the non-LR units,but not in the LR units.
C© Veterinary Emergency and Critical Care Society 2014, doi: 10.1111/vec.12160 261

R. Corsi et al.
Several studies of cytokines in stored human erythro-cyte concentrates have indicated that IL-8 concentrationssimilarly increase throughout storage of leukocyte-containing units, and that the increase in IL-8, is attenu-ated by prestorage LR12, 14, 15 or buffy coat depletion.12
IL-8 (now referred to as CXCL8) is a chemo-attractantfor neutrophils, and causes degranulation of neutrophilsand basophils.6;14;24 IL-8 also attracts natural killer(NK) cells, T cells, and GM-CSF-primed or IL-3 primedeosinophils.25 It is produced by a variety of cells in re-sponse to stimulation with IL-1�, IL-17, TNF-�, or anti-gen binding to toll-like receptors.26 Increased plasmaconcentrations of IL-8 have been reported in inflamma-tory diseases associated with leukocyte accumulation,13
and transient granulocytopenia followed by a granulo-cytosis in nonhuman primates.27 While IL-8 does nothave direct pyrogenic effects, it primes other leukocytesfor pyrogenic responses to cytokines such as IL-1 andTNF-�. Supernatant from NLR pRBC units has been re-ported to prime polymorphonuclear cells, and inducechemotaxis and the release of additional IL-8 in vitro.28
The passive administration of IL-8 via transfusion ofstored erythrocyte concentrates may therefore mediateor exacerbate nonhemolytic transfusion reactions in illrecipients. Clinical data from humans support this con-cept, as the incidence of febrile nonhemolytic transfusionreactions decreased in concordance with the institutionof LR as standard practice (resulting in delivery of fewerleukocyte containing units).29 Furthermore, in the ab-sence of overt transfusion reactions, passive transfer ofIL-8 via transfusion may additionally trigger worseninginflammatory response in critically ill patients.
IL-1� and TNF-� are potent proinflammatorycytokines24 that are synthesized from various cell types(primarily macrophages, but also monocytes, lympho-cytes, and fibroblasts). These cytokines trigger the releaseof prostaglandin E2 in the hypothalamus30 and are pyro-genic. They also have diverse potentiating effects on cellproliferation and differentiation, and function as impor-tant mediators of the systemic inflammatory response intrauma and infection.31
We were not able to document a significant effect ofeither LR or storage time on concentrations of IL-1� orTNF-� in our study. There was however a trend towardlower concentrations of both IL-1� and TNF-� in LR ver-sus non-LR units, but due to marked interunit variation,our study was underpowered to detect a difference be-tween groups. Whether or not the concentrations of theseproinflammatory cytokines can be significantly reducedby LR will need to be addressed in future larger stud-ies. Neither IL-1� nor TNF-� concentrations changedin association with storage time in our canine blood.These findings are in contrast to those with human blood,where there is a significant time-dependent increase in
IL-1,12, 15 IL-6,12 TNF-�,15 TGF�,12 and RANTES12 in non-LR units.
IL-10 is an anti-inflammatory cytokine with impor-tant regulatory functions in several aspects of immuneresponse. It is produced mainly by monocytes, T andB cells, NK cells, macrophages, mast cells, and dendriticcells.32 It has a direct inhibitory effect on T-cells and indi-rectly downregulates the expression of many proinflam-matory cytokines, chemokines, and chemokine recep-tors. IL-10 concentrations were very low in these canineerythrocyte concentrates. The lack of IL-10 mediatedanti-inflammatory effects may be contributory to theoverall proinflammatory nature of stored blood. Al-though only performing aerobic bacterial cultures froma single aliquot from each unit was a limiting factor, bybeing performed on day 35, it ruled out massive bacte-rial contamination, as all bacterial cultures yielded nogrowth.
In conclusion, we have demonstrated that the proin-flammatory cytokine IL-8 accumulates with storage incanine erythrocyte concentrates, and that this accumula-tion can be attenuated by use of prestorage LR. Standardleukocyte containing (non-LR) units with shorter stor-age times, or alternatively LR units, may be indicatedfor patients with marked inflammatory processes. Fu-ture studies should be aimed at determining the inflam-matory effects of IL-8 in stored erythrocyte concentrateson clinical blood recipients.
Acknowledgments
The authors thank Pall Corporation for donation of theleukoreduction filter bags, Jerry Fina and Charter Medi-cal for donation of the sampling ports, and Jessica Garrettfor her assistance with blood unit centrifugation.
Footnotesa Leukotrap WB System, Pall Corporation, East Hills, NY.b Canine IL-1 beta VetSet, Kingfisher Biotech, St. Paul, MN.c Duo-sets from R&D Systems, Minneapolis, MN.d Sigma Stat 2.03, SPSS, Inc., Chicago, IL.
References
1. Duke BJ, Modin GW, Schecter WP, et al. Transfusion significantlyincreases the risk for infection after splenic injury. Arch Surg 1993;128(10):1125–1130.
2. Dunne JR, Malone DL, Tracy JK, et al. Allogenic blood transfu-sion in the first 24 hours after trauma is associated with increasedsystemic inflammatory response syndrome (SIRS) and death. SurgInfect (Larchmt) 2004; 5(4):395–404.
3. Ezidiegwu CN, Lauenstein KJ, Rosales LG, et al. Febrile non-hemolytic transfusion reactions. Management by premedicationand cost implications in adult patients. Arch Pathol Lab Med 2004;128(9):991–995.
4. Lanevschi A, Wardrop KJ. Principles of transfusion medicine insmall animals. Can Vet J 2001; 42(6):447–454.
262 C© Veterinary Emergency and Critical Care Society 2014, doi: 10.1111/vec.12160

Cytokines in canine red cell units
5. Snyder EL. The role of cytokines and adhesive molecules in febrilenon-hemolytic transfusion reactions. Immunol Invest 1995; 24(1–2):333–339.
6. Escobar GA, Cheng AM, Moore EE, et al. Stored packed red bloodcell transfusion up-regulates inflammatory gene expression in cir-culating leukocytes. Ann Surg 2007; 246(1):129–134.
7. Marik PE, Sibbald WJ. Effect of stored-blood transfusion on oxygendelivery in patients with sepsis. J Am Med Assoc 1993; 269(23):3024–3029.
8. Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and com-plications after cardiac surgery. N Engl J Med 2008; 358(12):1229–1239.
9. Weinberg JA, McGwin G, Jr., Griffin RL, et al. Age of transfusedblood: an independent predictor of mortality despite universalleukoreduction. J Trauma 2008; 65(2):279–282.
10. Heddle NM. Pathophysiology of febrile nonhemolytic transfusionreactions. Curr Opin Hematol 1999; 6(6):420–426.
11. Muylle L. The role of cytokines in blood transfusion reactions. BloodRev 1995; 9(2):77–83.
12. Wadhwa M, Seghatchian MJ, Dilger P, et al. Cytokine accumula-tion in stored red cell concentrates: effect of buffy-coat removal andleucoreduction. Transfus Sci 2000; 23(1):7–16.
13. Kristiansson M, Soop M, Saraste L, et al. Cytokines in stored redblood cell concentrates: promoters of systemic inflammation andsimulators of acute transfusion reactions? Acta Anaesthesiol Scand1996; 40(4):496–501.
14. Stack G, Baril L, Napychank P, et al. Cytokine generation in stored,white cell-reduced, and bacterially contaminated units of red cells.Transfusion 1995; 35(3):199–203.
15. Shanwell A, Kristiansson M, Remberger M, et al. Generation ofcytokines in red cell concentrates during storage is prevented byprestorage white cell reduction. Transfusion 1997; 37(7):678–684.
16. McFaul SJ, Corley JB, Mester CW, et al. Packed blood cells storedin AS-5 become proinflammatory during storage. Transfusion 2009;49(7):1451–1460.
17. Dzik S. Leukodepletion blood filters: filter design and mechanismsof leukocyte removal. Transfus Med Rev 1993; 7(2):65–77.
18. Dzik S, Aubuchon J, Jeffries L, et al. Leukocyte reduction of bloodcomponents: public policy and new technology. Transfus Med Rev2000; 14(1):34–52.
19. McMichael MA, Smith SA, Galligan A, et al. Effect of leukoreductionon transfusion-induced inflammation in dogs. J Vet Intern Med 2010;24(5):1131–1137.
20. Herring J, Smith S, McMichael M, et al. Microparticles instored canine erythrocyte concentrates. Vet Clin Path 2013; 42(2):163–169.
21. Lee TH, Donegan E, Slichter S, et al. Transient increase in circulatingdonor leukocytes after allogeneic transfusions in immunocompe-tent recipients compatible with donor cell proliferation. Blood 1995;85(5):1207–1214.
22. Bilgin YM, van de Watering LM, Versteegh MI, et al. Effects of al-logeneic leukocytes in blood transfusions during cardiac surgeryon inflammatory mediators and postoperative complications. CritCare Med 2010; 38(2):546–552.
23. Brownlee L, Wardrop KJ, Sellon RK, et al. Use of a prestorage leuko-reduction filter effectively removes leukocytes from canine wholeblood while preserving red blood cell viability. J Vet Intern Med2000; 14(4):412–417.
24. Dinarello CA. Proinflammatory cytokines. Chest 2000; 118(2):503–508.
25. Burke SM, Issekutz TB, Mohan K, et al. Human mast cell activationwith virus-associated stimuli leads to the selective chemotaxis ofnatural killer cells by a CXCL8-dependent mechanism. Blood 2008;111(12):5467–5476.
26. Coelho AL, Hogaboam CM, Kunkel SL. Chemokines providethe sustained inflammatory bridge between innate and ac-quired immunity. Cytokine Growth Factor Rev 2005; 16(6):553–560.
27. Van Zee KJ, Fischer E, Hawes AS, et al. Effects of intravenous IL-8 ad-ministration in nonhuman primates. J Immunol 1992; 148(6):1746–1752.
28. Sparrow RL, Patton KA. Supernatant from stored red blood cellprimes inflammatory cells: influence of prestorage white cell reduc-tion. Transfusion 2004; 44(5):722–730.
29. King KE, Shirey RS, Thoman SK, et al. Universal leukoreduction de-creases the incidence of febrile nonhemolytic transfusion reactionsto RBCs. Transfusion 2004; 44(1):25–29.
30. Dzik WH. Is the febrile response to transfusion due to donor orrecipient cytokine? (Letter) Transfusion 1992; 32(6):594.
31. Akdis M, Burgler S, Crameri R, et al. Interleukins, from 1 to 37,and interferon-gamma: receptors, functions, and roles in diseases. JAllergy Clin Immunol 2011; 127(3):701–721.
32. Grimbaldeston MA, Nakae S, Kalesnikoff J, et al. Mast cell-derived interleukin 10 limits skin pathology in contact dermati-tis and chronic irradiation with ultraviolet B. Nat Immunol 2007;8(10):1095–1104.
C© Veterinary Emergency and Critical Care Society 2014, doi: 10.1111/vec.12160 263