damage control resuscitation
TRANSCRIPT


Sunday, October 26, 2014 2
Damage Control ResuscitationBy
DR. Mahmoud Abdulkareem
M.S {Cairo} , FRCS {Glasgow}
Consultant Surgeon,
King Fahad Specialist Hospital

Sunday, October 26, 2014 3
History of Trauma Resuscitation
About fifty years ago; there was Little or no systematic resuscitation after a civilian injury.

Sunday, October 26, 2014 4
“the neglected disease of modern society.”
THE NEED FOR TRAUMA SYSTEMS—HISTORY …. cont.
National Research Council: Accidental Death and Disability: The Neglected Disease of Modern
Society. Washington, DC: U.S. Government Printing Office, 1966.
Sunday, October 26, 2014 5
MODERN TRAUMA SYSTEM
DEVELOPMENT …. cont.
By 1975, Germany had established a nationwide trauma system, so that no patient was more than 15–20 minutes from one of these regional canters.

Sunday, October 26, 2014 6
Injury prevention
has become an essential focus for all trauma systems
prevention

4/21/14 7

Sunday, October 26, 2014 8
Trauma system
The true value of a trauma system is derived from the seamless transition between each phase of care

Sunday, October 26, 2014 9
Trauma Management: Golden Hour
Golden HourTime to reach operating room (or other definitive treatment)Patients in their Golden Hour must Be recognized quickly Have only immediate life threats managedBe transported to an appropriate facilitySurvival depends on assessment skillsGood assessment results fromAn organized approachClearly defined prioritiesUnderstanding available resources

Sunday, October 26, 2014 10
Prehospital Care ….con. The goal is to get the right patient to the
right hospital at the
right time for definitive care

Sunday, October 26, 2014 11
Advanced life support is provided[by an organized trauma team]
Early hospital phase:

Sunday, October 26, 2014 12
Trauma TeamDefinition
The trauma team is an organized group of professionals who perform initial assessment and resuscitation of critically injured patients. Team composition, level of response, and responsibilities of each member are institution-specific. Personnel are outlined as follows:
1. Trauma surgeon—a general surgeon with demonstrated training and interest in trauma care. In designated trauma centers, the trauma surgeon typically functions as the trauma team leader.
2. Emergency medicine physician—in many hospitals, the emergency medicine physician functions as the trauma team leader depending on the perceived severity of injuries. Ideally, these physicians have Advanced Trauma Life Support (ATLS) certification.
3. Anesthesiologist—a physician with special skills in airway management, sedation, and analgesia. In many trauma centers, this role may be fulfilled by a certified registered nurse anesthetist
4. Trauma nurses—emergency department nurses with specialized training and demonstrated interest in trauma care.
5. Resident physicians—residents in emergency medicine or surgery and trauma fellows may assume active roles in the trauma team. In Level I and II trauma centers, senior surgical residents and trauma fellows may function as trauma team leaders.
6. Respiratory therapist—therapist available to assist in the evaluation and management of the patient's respiratory status.
7. Radiology technicians—technicians available to obtain x-rays as indicated by the initial assessment and secondary survey.
8. Surgical subspecialists—although not typically involved in the initial assessment, surgical consultants (e.g., orthopedic surgeons, neurosurgeons) are vital members of the trauma team.
9. Other personnel—the trauma team may also include OR nurses, laboratory technicians, ECG technicians, chaplains, social workers, transport personnel, and case managers.

Sunday, October 26, 2014 13

Sunday, October 26, 2014 14
Original article
Impact of a multifunctional image-guided therapy suiteon emergency multiple trauma care
T. Gross1, P. Messmer1,7, F. Amsler5, I. Fu¨ glistaler-Montali1, M. Zu¨ rcher2, R. W. Hu¨ gli1,6,P. Regazzoni1,3 and A. L. Jacob1,4
British Journal of Surgery 2010; 97: 118–127Conclusion: Implementation of a MIGTS in the emergency treatment of multiple trauma significantly
accelerated the procedure and reduced the number of in-hospital transports.

Sunday, October 26, 2014 15

Sunday, October 26, 2014 16

4/21/14 17

Posttraumatic hemorrhage is responsible for one of the leading causes of preventable
human deaths worldwide.

4/21/14 19
Sunday, October 26, 2014 20
INTRODUCTIONDuring the last two decades, advances in pre-hospital care and the adoption of the “scoop and run” philosophy has resulted in the arrival of more severely injured patients who typically might have died in the field or en route to the hospital.

Sunday, October 26, 2014 21
Standard surgical practice
Standard surgical practice (early total care. The best operation for a patient is one, definitive procedure
The first chance of any surgical intervention is the best chance for any definitive repair or reconstruction
ER
ER→OR→ICU
OR ICU

What has been going on??
The conventional sequence of the management of trauma surgery was to bring the patient to the operating room after initial resuscitation and then to operate for complete repair of the injuries. Subsequently, these patients were sent to the intensive care unit where a good number of them succumbed due to metabolic derangement of the body.

4/21/14 23
The outcome…..
“The operation was a success but the
patient died anyway”–
Anonymous

DCS 2
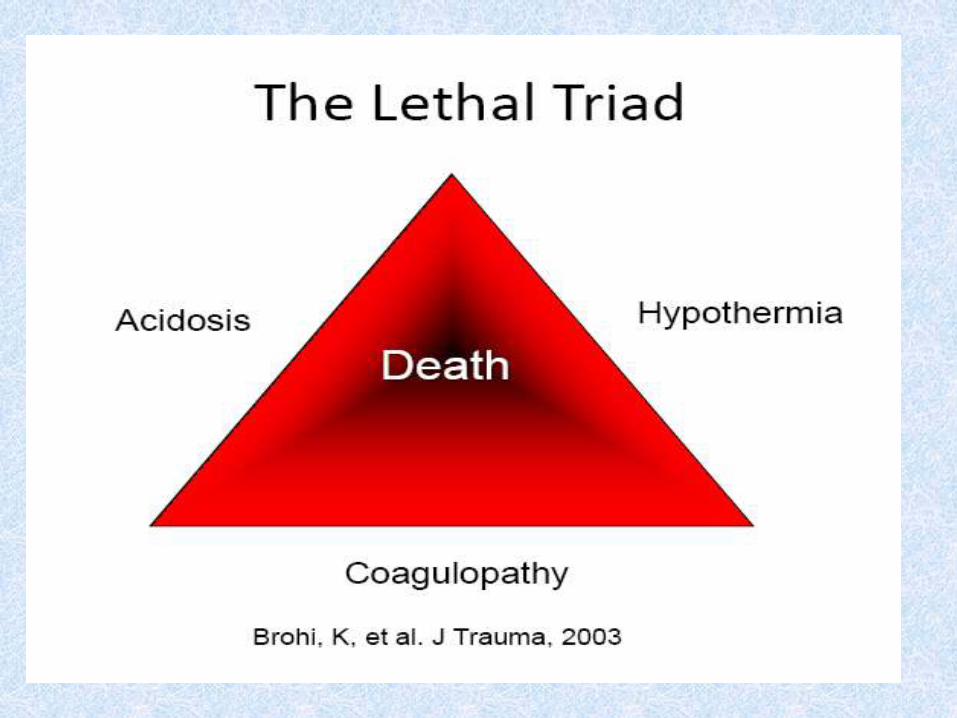
In severe trauma patients a triad of
hypothermia, metabolic acidosis, and
coagulopathy rapidly established. This so
called " vicious cycle of metabolic failure " is
irreversible as long as patient is in the
operating room with the abdomen open
during a prolonged procedure.
But,…… why?!

" vicious cycle of metabolic failure "

Damage control is a naval term first used during World War II to describe emergency measures for control of flooding that threatens to sink a ship. A range of simple procedures may be used, but the central goal is to ensure survival of the ship until it reaches a port where definitive repairs can be safely performed.
Damage control

Sunday, October 26, 2014 28
Damage Control !

Damage Control – Philosophy
Damage control is based on the principal that outcome after major trauma is determined by the physiological limits of the patient , rather than by the effort of anatomical restoration by the surgeon.

Applying the same philosophy
To save the patients in extremis, surgery should be abbreviated . only immediately life threatening injuries should be attended and repaired, while other injuries should be temporized and repaired definitively when the patient is more stable. The best place for a severely and multiply injured patient is in the intensive care unit.

Damage Control – Philosophy
The damage control concept places surgery as an integral part of the resuscitative process, rather than an end in itself.

The term “Damage control”
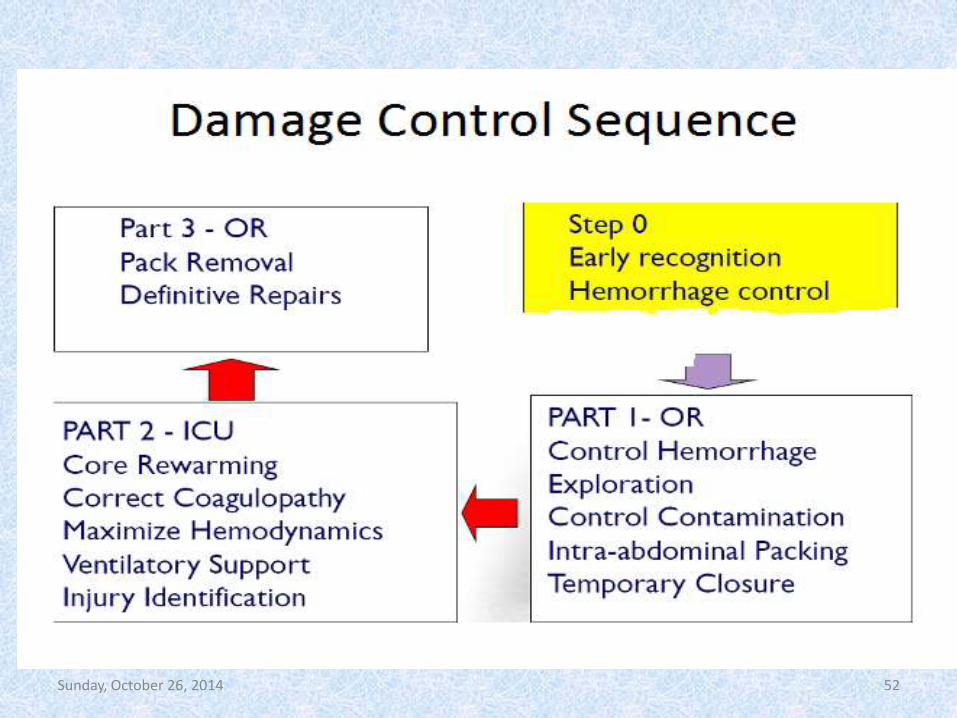
Rotondo and Schwab in 1992 coined the term “damage control” and outlined a three phased approach:
Part one (DC I) consists of immediate exploratory laparotomywith control of bleeding and contamination, abdominal packing and abbreviated wound closure.
Part two (DC II) consists of the ICU resuscitation; immediate endpoints include physiological and biochemical stabilization. A tertiary exam should be performed at this time to identify all injuries.
Part three (DC III) consists of re-exploration and definitive repair of all injuries.

Sunday, October 26, 2014 33

Damage Control Surgery
The later damage control is applied, the less successful the outcome.

When to employ damage controlο Use damage control in patients who are present with or at risk for developing:♦ Multiple life-threatening injuries.♦ Acidosis (pH < 7.2).♦ Hypothermia (temp < 34°C).♦ Hypotension and shock on presentation.♦ Combined hollow viscus and vascular or vascularized organ injury.♦ Coagulopathy (PT > 19 sec and/or PTT > 60 sec).
♦ Mass casualty situation.ο

When to employ damage control

When to employ damage control

Sunday, October 26, 2014 38



REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta), together with a pelvic binder, for control of hemorrhage in ER

REBOA (Resuscitative EndovascularBalloon Occlusion of the Aorta)

Sunday, October 26, 2014 43

4/21/14 44
Phase 1 of damage control includes 5 distinct steps:1. Control of hemorrhage.

4/21/14 45
intra-arterial shunt in left common iliac artery
Phase 1 of damage control includes 5 distinct steps:1. Control of hemorrhage

4/21/14 46
In this case, especially with colonic injuries, or multiple small bowel lesions, it is wiser to resect non-viable bowel and close the ends, leaving them in the abdomen for anastomosis at the second procedure. The linear stapler is useful to achieve this, but bowel ends may be closed with running suture or even umbilical tapes. Ileostomies or colostomies should preferably not be performed in a damage control setting, especially if the abdomen is to be left open, as control of spillage is almost impossible.
Phase 1 of damage control includes 5 distinct steps:
2. Control of contamination.

Phase 1 of damage control includes 5 distinct steps:3- EXPLORATION TO R/O SIGNIFICANT INJURY
4/21/14 48
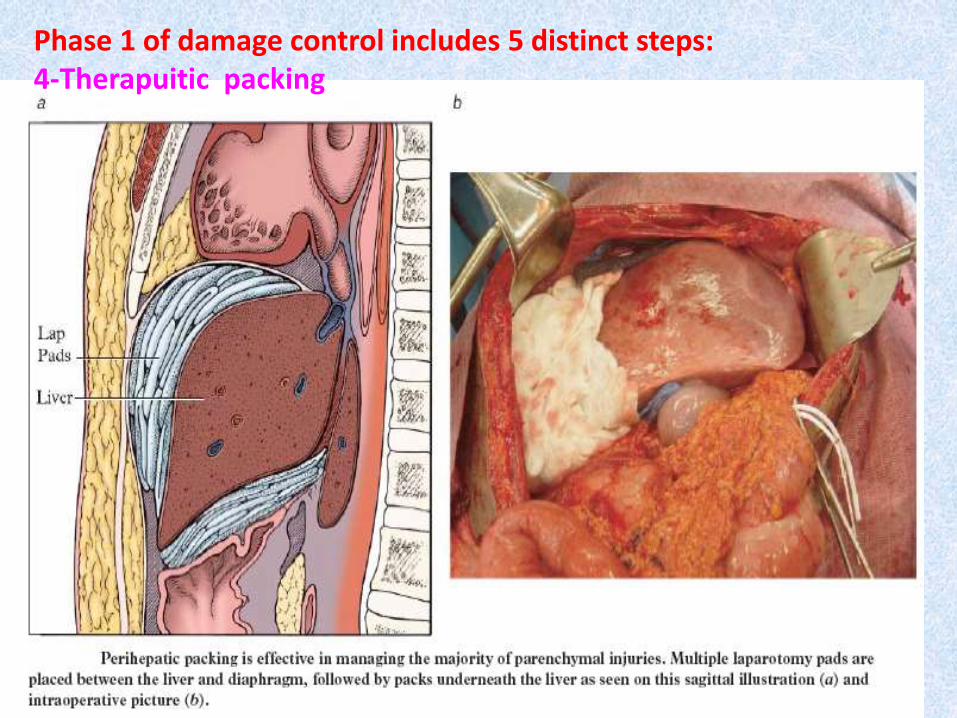
Phase 1 of damage control includes 5 distinct steps:4-Therapuitic packing

Directly to the IS- jointPacking of the fractured areaLaparotomy pads into the true pelvis
Extraperitoneal Packing

Sunday, October 26, 2014 50
Phase 1 of damage control includes 5 distinct steps:5- Temporary abdominal closure .
Left lateral thoracotomy with towel clip closure of damage-control celiotomy. Courtesy of Pedro Gustavo R. Teixeira, Trauma Surgeon, Brazil, The Trauma Imagebank.

Methods of Temporary abdominal closure
Bogota bag
Sunday, October 26, 2014 52

4/21/14 53

Sunday, October 26, 2014 54
Approach :
1. Permissive Hypotension
2. Limited Crystalloid
3. Transfuse Blood Components in Equal Ratios
PRBC’s / FFP / Platelets
Source Control of Bleeding
Damage Control Resuscitation in Combination With Damage
Control Laparotomy : A Survival Advantage
J Trauma. 2010;69: 46–52

Sunday, October 26, 2014 55
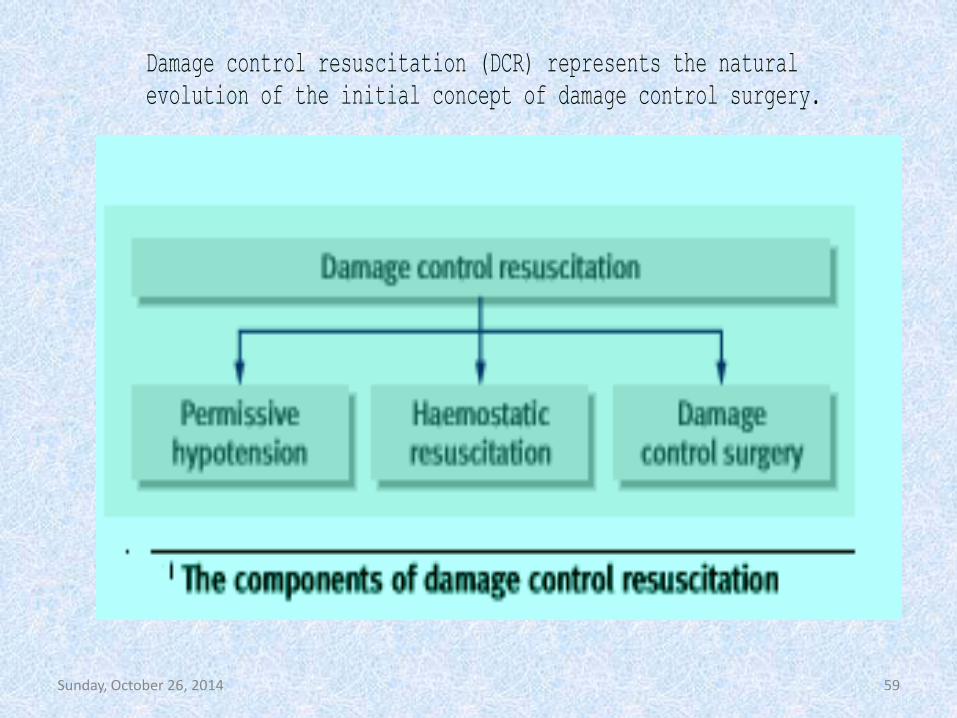
Damage control resuscitation (DCR) represents the natural
evolution of the initial concept of damage control surgery.

Permissive Hypotension in Trauma Resus.
IV fluids in hypovolemic shock:
• No survival, some mortality
Theories on IVF in trauma:
1. BP dislodges clots
2. BP = bleeding
3.IVF hemodilutes clotting factors
Duchesne JC et al. Damage Control Resuscitation: From Emergency Department to the Operating Room. The Amer Surgeon. 2011; 77: 201-206.

Permissive Hypotension Limits• SBP 90 (MAP 50 – 60 mmHg):
• Ideal permissive hypotension < 90 min.
• Severe damage when > 120 min.
• It is important to remember that permissive hypotension is a temporizing measure to improve outcomes until the source of bleeding is controlled.
Li T, et al. Ideal Permissive Hypotension to Resuscitate Uncontrolled Hemorrhagic Shock and the Tolerance Time in Rats. Anesthesiology. 2011; 114 (1): 111-119.

Contraindication of Permissive Hypotension
• traumatic brain injuries, because adequate perfusion pressure is crucial to ensure tissue oxygenation of the central nervous system.
• Preexisting conditions such as hypertension, angina pectoris, coronary disease, and carotid stenosis may also lead to severe cardiovascular dysfunction when trauma patients are hypotensive. These conditions are common mainly in the elderly (>65 years old), but also occur in other age groups because of occult disease.
Sunday, October 26, 2014 59
Damage control resuscitation (DCR) represents the natural
evolution of the initial concept of damage control surgery.

The concept of giving plasma and platelets early along with red cells in an attempt to closely approximate whole blood makes a lot of sense. In fact, when we reviewed blood usage at the Shock Trauma Center in the year 2000, massively transfused patients ultimately received a unit of plasma for every unit of blood that was transfused. It made a lot of sense that giving FFP earlier would be beneficial.
Hemostatic Resuscitation

Hemostatic resuscitation, which promotes balancedblood product transfusion ratios while minimizing crystalloid infusion, improves outcome in critically injured, coagulopathic adults.
Hemostatic Resuscitation
Hemostatic resuscitation is a transfusion strategy that targets coagulopathy with early blood product administration.

The new resuscitative paradigm has become to allow a systolic blood pressure to be around 80 mmHg, to limit crystalloid resuscitation, and use blood, FFP and platelets in a one to one to one ratio.
Hemostatic Resuscitation

Sunday, October 26, 2014 63
Damage control resuscitation (DCR) represents the natural
evolution of the initial concept of damage control surgery.

DCR, which in part aims to reproduce whole blood resuscitation via the use of approximately 1:1:1 ratios of red blood cells (RBCs), plasma, and platelets, has become the standard of care for the transfusion management of patients with severe hemorrhage. This approach, however, comes with a potential cost: the use of a greater quantities of plasma and platelets.
Disclaiming and Criticizing Hemostatic Resuscitation with 1:1:1 ratios

CAGS AND ACS EVIDENCE BASED REVIEWS IN SURGERY. 50Is early transfusion of plasma and platelets in higher ratios associated with decreased in-hospital mortality in bleeding patients?
J can chir, Vol. 57, No 5, octobre 2014 © 2014 Association médicale canadienne
While the PROMMTT study adds further evidence to support transfusions with higher plasma :RBC transfusions, further studies are needed, especially regarding how to efficiently identify the patients who will benefit from early administration of the therapy.



Sunday, October 26, 2014 68

Sunday, October 26, 2014 69
Recent studies have shown that nearly 25% of trauma patients
present with a clinically significant coagulopathy upon arrival
in the emergency department which affects their overall
outcome.4 Interestingly, this early coagulopathy occurred
before any significant consumption or fluid administration and
in the absence of a relevant acidaemia or hypothermia.
Br. J. Anaesth. (2010) 105 (2): 103-105.
Acute Traumatic Coagulopathy

Sunday, October 26, 2014 70

Sunday, October 26, 2014 71
Acute Traumatic Coagulopathy
Recognized in patients with significant tissue injury and hypotension
Distinct from iatrogenic coagulopathy after trauma
Dilutional coagulopathy
Present prior to resuscitation in rapidly evacuated severe trauma
Mortality rate increased 4x
Modulated through protein C activation

Sunday, October 26, 2014 72

Sunday, October 26, 2014 73

Sunday, October 26, 2014 74


Sunday, October 26, 2014 76

Sunday, October 26, 2014 77

Sunday, October 26, 2014 78
The anticoagulant thrombomodulin protein C pathway is overtly
activated, resulting in reduced pro-coagulatory potential and
increased fibrinolytic activity. Once protein C is activated through a
thrombin–thrombotic-dependent reaction, activated protein C
(aPC) exerts its profound anticoagulant effects by irreversibly
inactivating factors Va and VIIIa. In addition to its direct inhibition
of fibrin formation, aPC causes resolution of formed clots by
stopping the inhibition of fibrinolysis by direct inhibition of
plasminogen activator inhibitor .
Acute Traumatic Coagulopathy

Sunday, October 26, 2014 79

Hemostasis is a complex physiologic process involving many constituents that act in symphony to form a clot. Conventional coagulation tests, such as prothrombin time (PT), international normalized ratio (INR), activated partial thromboplastin time (aPTT), fibrinogen concentration, and platelet count, measure only a fraction of this process. Moreover, these tests sometimes lack accuracy in trauma settings.
Hemostasis


Sunday, October 26, 2014 83

Sunday, October 26, 2014 84

Sunday, October 26, 2014 85

Sunday, October 26, 2014 86
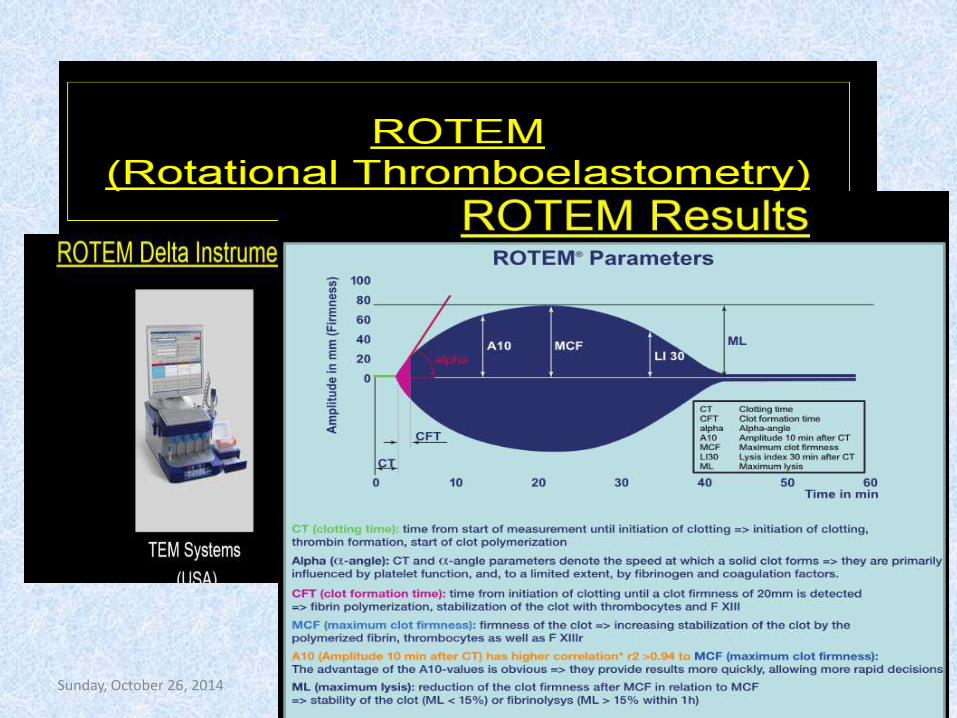
In recent years, viscoelastic hemostatic assays (VHA), including thrombelastography (TEG) and thrombelastometry, have been demonstrated to be ideal methods of monitoring coagulation function in trauma patients . Furthermore, several studies have suggested the potential of VHA tests to guide component blood transfusion in a variety of patient groups . In particular, a recent study by Kashuk et al. showed that goal-directed transfusion based on rapid TEG was useful in managing trauma-induced coagulopathy, with the potential to reduce blood product administration in trauma patients.
Viscoelastic Hemostatic Assays (VHA),

Specifically, TEG depicts the following four stages of clot formation: (1) initiation, (2) amplification, (3) propagation, and (4) termination through fibrinolysis. This is accomplished by placing a 0.36 mL aliquot of citrated whole blood sample into a Kaolin coated (“standard”) TEG cup that has been pre-warmed to 37°C. A pin, attached by a wire to a transducer, is then suspended into the sample. The cup rotates around the pin within the TEG autoanalyzer at an angle of 4.45 degrees every 10 seconds. As the clot forms, the pin and the cup are ultimately joined by the formation of the fibrin and platelet clot. This causes the pin and the cup to rotate together, with the resultant change in tension detected by the transducer. A graphical output is then plotted as a change in tension (measured in millimeters on the y axis) versus time (measured in minutes on the x-axis).The four key parameters of the TEG tracing are the: (1) r value (reaction time to clot formation), (2) α (alpha) angle – rate of clot formation, (3) MA (maximum amplitude – maximum strength of clot), and (4) LY30 (percent clot lysis 30 minutes after the MA).
Viscoelastic Hemostatic Assays (VHA),

Sunday, October 26, 2014 88
Sunday, October 26, 2014 89

Sunday, October 26, 2014 90

Normal TEG tracing (in black) resembles a wide flat (non-functional) shovel with a short handle. The superimposed “shovel” (in red) demonstrates a tracing with a prolonged r, flat α angle, small MA, and increased LY 30, indicative of a systemic coagulopathy with fibrinolysis.


Abnormal TEM Tracings, Interventions

Sunday, October 26, 2014 94

Sunday, October 26, 2014 95

Sunday, October 26, 2014 96
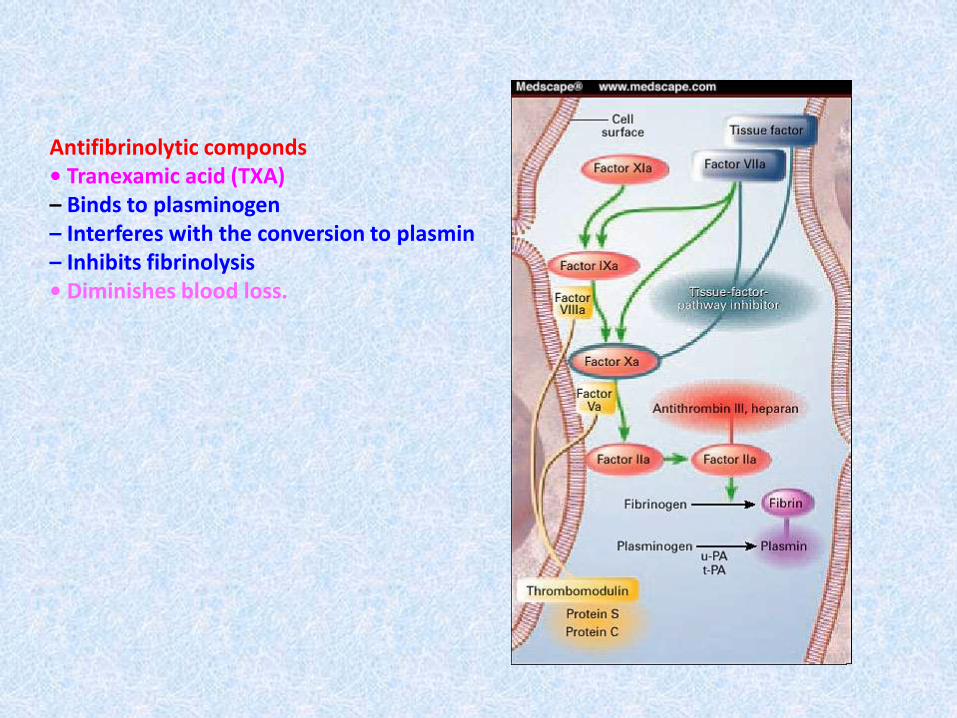
Antifibrinolytic componds• Tranexamic acid (TXA)– Binds to plasminogen– Interferes with the conversion to plasmin– Inhibits fibrinolysis• Diminishes blood loss.

How and When to Use TXA for Trauma PatientsIndications:
Adults with acute traumatic injury leading to significant hemorrhage and requiring blood transfusion.May be beneficial in trauma patients with significant hemorrhage and evidence of hyperfibrinolysis on rotational electrothromboelastometry (ROTEM).Should only be given less than 3 hours from the time of injury.
Dosing: 1 gram IV bolus over 10 minutes, followed by 1 gram continuous IV infusion over 8 hours.


Sunday, October 26, 2014 100

Sunday, October 26, 2014 101
Sunday, October 26, 2014 102

Sunday, October 26, 2014 103

Sunday, October 26, 2014 104

Sunday, October 26, 2014 105
Damage control resuscitation (DCR) represents the natural
evolution of the initial concept of damage control surgery.

.وآخر دعوانا أن الحمد هلل رب العالمين
10/26/2014