danielle wilkins - cabrini health - balancing the interest of your clients and mitigating litigation...
TRANSCRIPT

Balancing the interests of your clients and mi4ga4ng li4ga4on opportuni4es
Dr Danielle Wilkins

Working with a birth plan

Declara4ons • Consultant Obstetrician in private prac5ce • 2 children, planned pregnancies, births both completely not to plan
• Trained and worked in a ter5ary ins5tu5on with a midwifery model of care for 15 years

Birth plan • WriBen birth plan introduced in the 1980’s • Communica5on tool • Encourage women to think about what is important to them
• Realis5c plan • Make informed decisions
Birth Plans:The good, the Bad, and the future. Journal of Obstetric, Gynaecologic and Neonatal Nursing. Vol 35 March 2006

Birth plan • Bubhub • “extremely important part of your pregnancy planning”
• “tremendous significance” • “you are your health care providers are in agreement on all issues regarding the birth of your child”

Issues • “cynics argue that wri5ng a birth plan is fu5le as it is hard to predict a birth”
• A detailed proposal for doing or achieving something • Conflic5ng beliefs about what cons5tutes safe, effec5ve care
• Asked to prac5ce against our training and professional judgment, “Clash of world views”, prac5ce against the best available evidence
Birth Plans Tickets to the OR? • Percep5ons of obstetricians, midwives and pregnant women regarding outcomes in women with birth plans • 65% of health care providers thought that women with a birth plan were more likely to have a caesarean sec5on
• 2.4% of pa5ents believed that women with birth plans had an overall worse obstetric outcome
White-‐Corey, Shelley. MCN, The American Journal of Maternal/Child Nursing Vol 38
Oct 2013

Dr Google • “Men5on clearly how oaen you want your cervix checks and monitoring”

Dr Google • “Do you consider aBached fetal monitors to be something invasive, uncomfortable and restric5ve to your mobility and only to be used for short periods of 5me?”
Dr Google • “If you require help to deliver your baby, what would your preference be – forceps or ventouse?”

Dr Google • “Do you prefer a rou5ne episiotomy or to avoid an episiotomy altogether?”

Dr Google • “Do you prefer to have a natural third stage without the use of drugs to speed up the delivery of the placenta?”

Some real life examples • “We want the lights dimmed. We don’t want anyone to talk unless it is an emergency. The only sound we want to hear is the music we have prepared for the birth”

Some real life examples • “We are happy to have the baby monitored with Doppler only. CTG will only be consented to if there are clear and dis5nct signs of distress in the baby or clear and dis5nct concerns for the baby”

Induc4on of labour • Reluctance = medicaliza5on • Strong belief that induc5on increases CS • Cascade of interven5on • More common with prolonged pregnancy • There is a significant increase in the risk of s5ll birth, neonatal and post-‐neonatal mortality in prolonged pregnancy
Hilder L. Prolonged pregnancy:evalua5ng gesta5on-‐specific risks of fetal and infant mortality. Br J Obstet Gynaecol 1998

Induc4on of labour • A policy of induc5on compared with expectant management is associated with fewer perinatal deaths and fewer caesarean sec5ons
• Expectant management monitoring
Gulmezoglu AM. Induc5on of labour for improving birth outcomes for women at or beyond term. Cochrane Database Syst Rev
2012

Monitoring in labour • IntermiBent doppler ausculta5on vs CTG monitoring
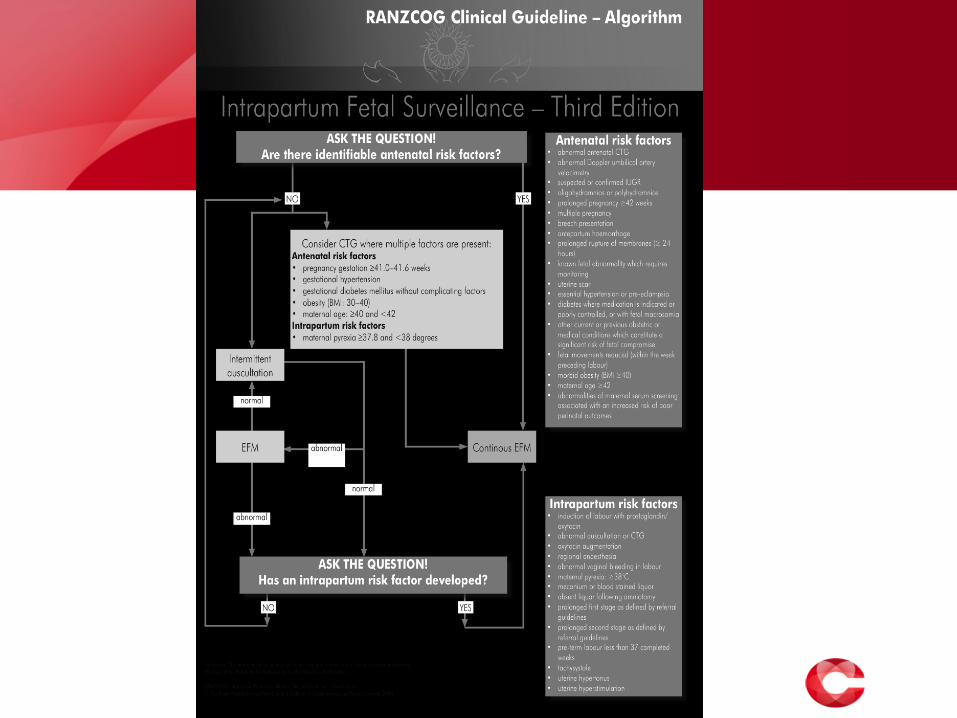

Monitoring in labour -‐ CTG • Intrapartum risk factors
• Induc5on of labour with prostaglandin or oxytocin
• Abnormal ausculta5on or CTG
• Oxytocin augmenta5on • Regional anaesthesia • Abnormal vaginal bleeding • Maternal pyrexia >37.9 • Meconium or blood stained liquor
• Absent liquor following amniotomy
• Prolonged first stage • Prolonged second stage • Pre-‐term labour less than 37
completed weeks • Tachysystole • Uterine hypertonus • Uterine hypers5mula5on

Monitoring in labour • “clear and dis5nct signs of distress “ • Blood stained liquor • Absent liquor following amniotomy • Prolonged first or second stage • Tachysystole • Uterine hypertonus
Monitoring in labour -‐ IA • RANZCOG guidelines for intermiBent ausculta5on • Every 15-‐30 minutes during the first stage of labour • Aaer each contrac5on or at least every 5 minutes in the ac5ve stage of labour
• Each ausculta5on episode should commence toward the end of a contrac5on and be con5nued for at least 30-‐60 seconds aaer the contrac5on has finished

Rou4ne vaginal examina4ons • Uncomfortable • Invasive • Flat on bed • Risk of ascending infec5on
• Confirm presen5ng part • Assess posi5on • Assess progress • Assist with progress • Assess well-‐being

Presenta5on and posi5on can be assessed by ultrasound scan but this is less common
once labour has commenced.

Ac4ve management of labour • Kieran O’Driscoll BMJ 1973 • Main emphasis was on care and managing pain • Examina5ons for progress every 1-‐2 hours • Decreased CS rate • “Rectal examina5on has a decided advantage over vaginal examina5on in assessing progress because it can be performed at regular intervals with much less formality. An important prac5cal considera5on in a busy unit.”

NICE guidelines 2014 • When conduc5ng a VE • Necessity • Aware of distress • Explana5on before • Ensure
• Consent • Dignity • Privacy • Comfort
• Explain aaerwards
• Avoid “rou5ne” interven5ons

World Health Organisa4on • 4 hour ac5on line

I won’t have an epidural Pro’s • Most cases v effec5ve pain
relief • Relaxa5on of perineal m • Rest • High blood pressure • Less discomfort with
assisted birth • Awake for CS
Con’s • 5-‐10% patchy pain relief • Effect is too high • Limited mobility • IV, monitor, catheter • Less effec5ve labour • Less effec5ve pushing with
increased risk of forceps • Can double the odds of CS • Drop in blood pressure • Spinal headache
todaysparent.com

Storknet.com • Undesired effects on newborn • Neurobehavioural effects – irritability, inconsolability, decreased ability to track an object visually or to shut out noise

54 infants…. • Possible less efficient or less organized roo5ng • Short term decreased infant responsiveness
Denise M. Risks and Benefits of Epidural Analgesia

NICE guidelines • Only form of full pain relief • Not associated with a longer first stage of labour • Not associated with an increased risk of CS • It is associated with a longer second stage (wait) • There is an increased risk of instrumental birth • Will be accompanied by more intensive monitoring

Ventouse or forceps • “an episiotomy is cut to make space for the forceps in the vagina”

Episiotomy • Not rou5ne • Does not prevent all third degree tears • Nega5ve impact on birth sa5sfac5on

Physiological third stage • Oxytocin for third stage • Less blood loss at delivery • Less likely to have a blood transfusion • More likely to have aaerpains

Making it work • Communica5on tool
• Ask • Con5nuity of carer
• Encourage women to think about what is important to them • Nature
• Realis5c plan • No epidural/episiotomy
• Make informed decisions • Accurate informa5on

PND • Sa5sfac5on with birth experience is closely linked with postpartum depression
• Women who felt in control of their birth plans, and who had support when things didn’t go as planned, were very sa5sfied with their birth experience and experienced less postpartum depression
Benoit et al 2007