david morgan
TRANSCRIPT

Tackling wasteful spending on health:
A pathway to improving health system performance of
OECD countries
David MorganHealth EconomistThe Organisation for Economic Co-operation and Development (OECD)

Tackling wasteful spending on health
Why do we need to talk about waste?
• Adverse events occur in 1 out of 10 hospitalisations and add 13-
17% to hospital costs when up to 70% of these events can
actually be avoided
• Geographic variations in rates of cardiac procedures (threefold)
and knee replacements (fivefold) are largely unwarranted
• Up to 50% of antimicrobial prescriptions are unnecessary
• 12-56% of ER visits are unnecessary
• Administrative expenditure varies more than six-fold
geographically, with no obvious correlation with performance
• Loss to fraud and error may average 6% of payments
for health care services
What exactly is wasteful spending?
• A pragmatic definition
– Services and processes which are either harmful or do not
deliver benefits;
– Excess costs which could be avoided by replacing them with
cheaper alternatives with identical or better benefits.
• Up to a fifth of health spending in OECD countries is at
best ineffective and at worst, wasteful
Tackling wasteful spending on health

Understanding wasteful spending
Waste
occurs
when …
Patients do not receive the right
care
Duplication of tests and services
Avoidable adverse events
Low-value care: Ineffective, inappropriate, not cost-effective
Benefits could be obtained with
fewer resources
Discarded inputs e.g. purchased drugs
Overpriced input(e.g. generic vs brand)
High cost inputs used unnecessarily (HR, hospital care)
Resources are unnecessarily
taken away from patient care
Administrative waste
Fraud, abuse and corruption
Tackling wasteful spending on health

What are the causes?
Tackling wasteful spending on health
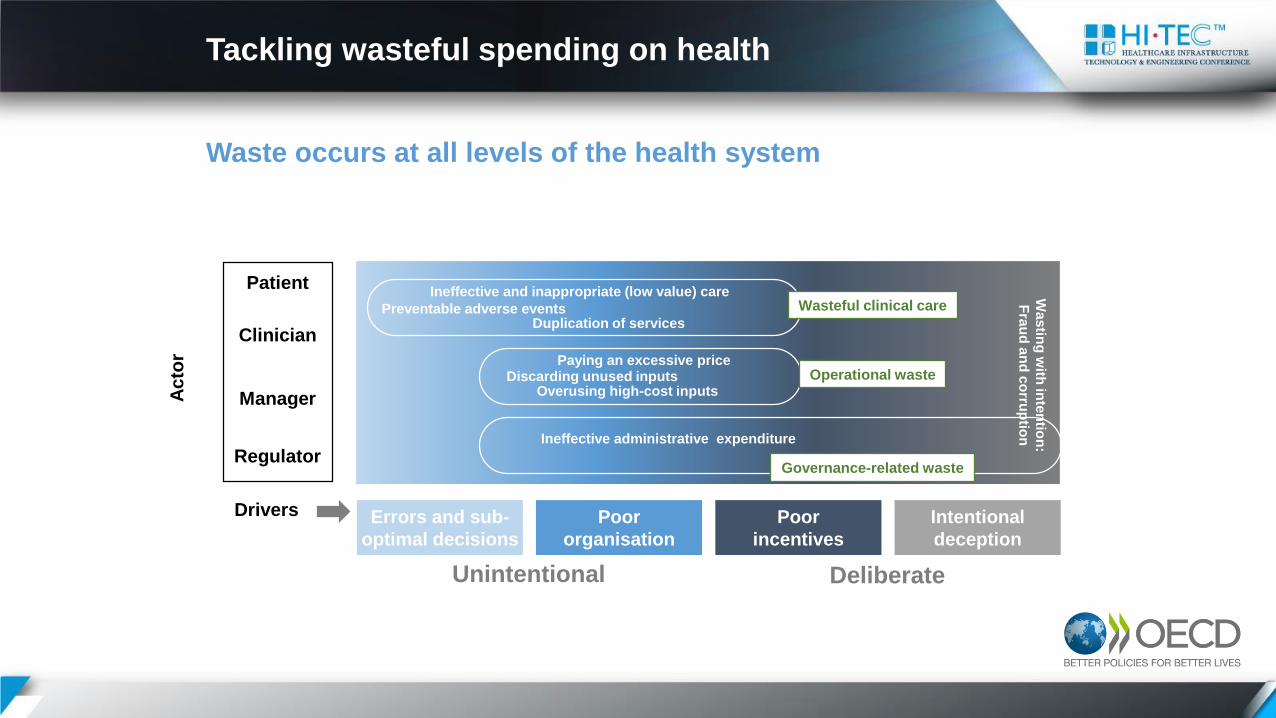
Waste occurs at all levels of the health system
Patient
Manager
Regulator
Ac
tor
Clinician
Poor
incentives
Drivers
Unintentional Deliberate
Errors and sub-
optimal decisions
Poor
organisation
Intentional
deception
Preventable adverse eventsDuplication of services
Ineffective and inappropriate (low value) careWasteful clinical care
Overusing high-cost inputs
Paying an excessive priceDiscarding unused inputs
Ineffective administrative expenditure
Wa
stin
g w
ith in
ten
tion
:
Fra
ud
an
d c
orru
ptio
n
Operational waste
Governance-related waste
Tackling wasteful spending on health

Wasteful clinical care Mounting evidence of overuse
C-section rates, 2015
53
.1
46
.8
46
.0
38
.0
37
.2
36
.2
35
.3
34
.0
32
.9
32
.3
32
.2
30
.2
30
.2
30
.1
28
.7
27
.9
27
.8
26
.3
26
.2
26
.0
25
.4
24
.5
21
.1
21
.0
20
.8
20
.8
20
.8
18
.7
17
.3
16
.2
16
.1
16
.0
15
.9
15
.5
0
10
20
30
40
50
60
Per 100 live births
Chronic benzodiazepine use, 2015
Number of patients per 1000, aged 65 years and over who have prescriptions for benzodiazepine for more than 365 days in 2015 (or nearest year)
67
54 5244
3427 25
18 18 18 18 1711 10
5 3 00
10
20
30
40
50
60
70
80
Per 1000 persons aged 65 years and over
Tackling wasteful spending on health
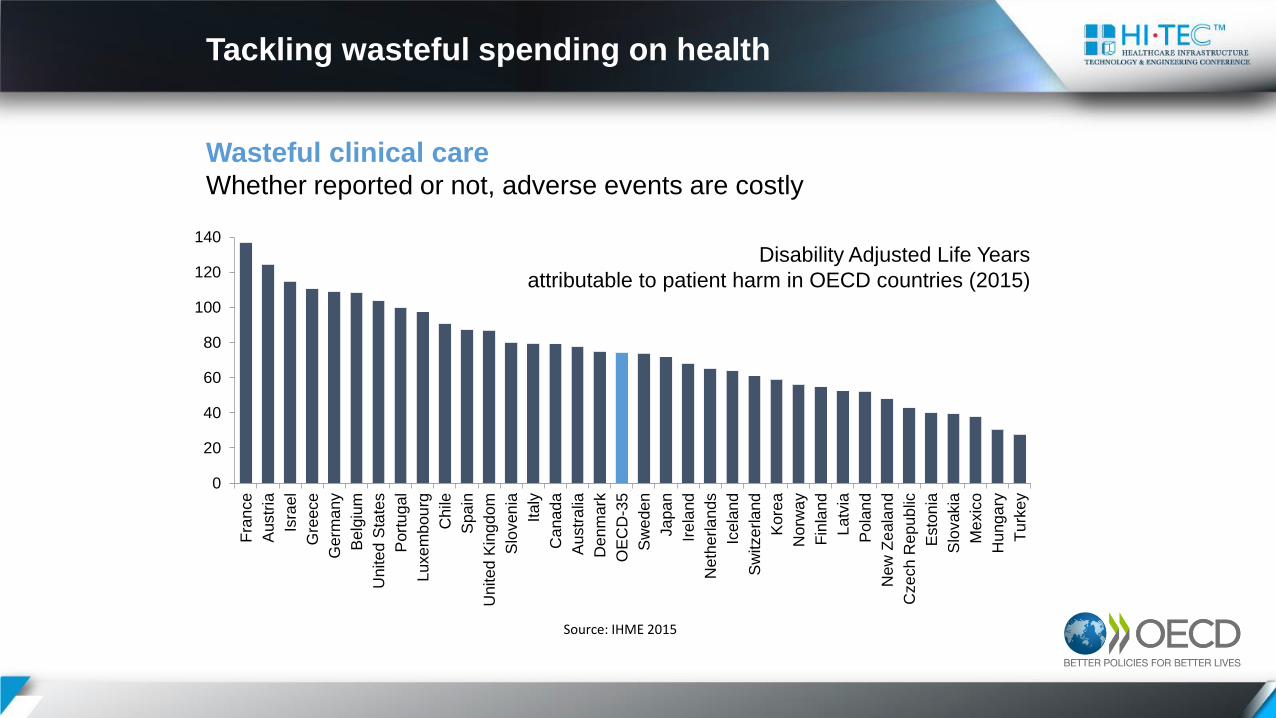
Wasteful clinical care Whether reported or not, adverse events are costly
0
20
40
60
80
100
120
140F
ran
ce
Austr
ia
Isra
el
Gre
ece
Germ
any
Belg
ium
United
Sta
tes
Port
ug
al
Luxe
mb
ou
rg
Chile
Spa
in
United
Kin
gd
om
Slo
ven
ia
Italy
Cana
da
Austr
alia
Denm
ark
OE
CD
-35
Sw
ede
n
Ja
pa
n
Ire
land
Neth
erla
nds
Icela
nd
Sw
itze
rla
nd
Kore
a
Norw
ay
Fin
land
Latv
ia
Pola
nd
New
Ze
ala
nd
Czech R
ep
ub
lic
Esto
nia
Slo
vakia
Me
xic
o
Hung
ary
Tu
rkey
Source: IHME 2015
Disability Adjusted Life Years
attributable to patient harm in OECD countries (2015)
Tackling wasteful spending on health

Wasteful clinical careInformation systems need strengthening
• Robust information systems to identify low-value care
– At least 10 OECD countries have atlases
– Limitations of many administrative data systems
• Reporting and learning systems of adverse events
– New Zealand: System covers most non-hospital providers
• Patient-reported measures
– Value and safety from the perspective of care recipient
– England: A leader among OECD countries
– PaRIS agenda
Tackling wasteful spending on health

Wasteful clinical careCombination of policy levers to tackle wasteful care
• Adherence to clinical guidelines and protocols can be
encouraged by audits and feedback
• Behaviour change campaigns
– Choosing Wisely® campaign in a third of OECD countries
– Kaiser Permanente’s antimicrobial stewardship programme
resulted in a 45% drop in prescriptions
– Safety campaigns: “SAVE LIVES: Clean Your Hands” initiative
active in 174 countries
• Financial incentives and nudges
– Australia’s Queensland withholds payment to hospitals for
“never events”
– 19 countries use the Health Technology Assessment (HTA)
disinvestment: Australia’s on-going benefit schedule review
Tackling wasteful spending on health
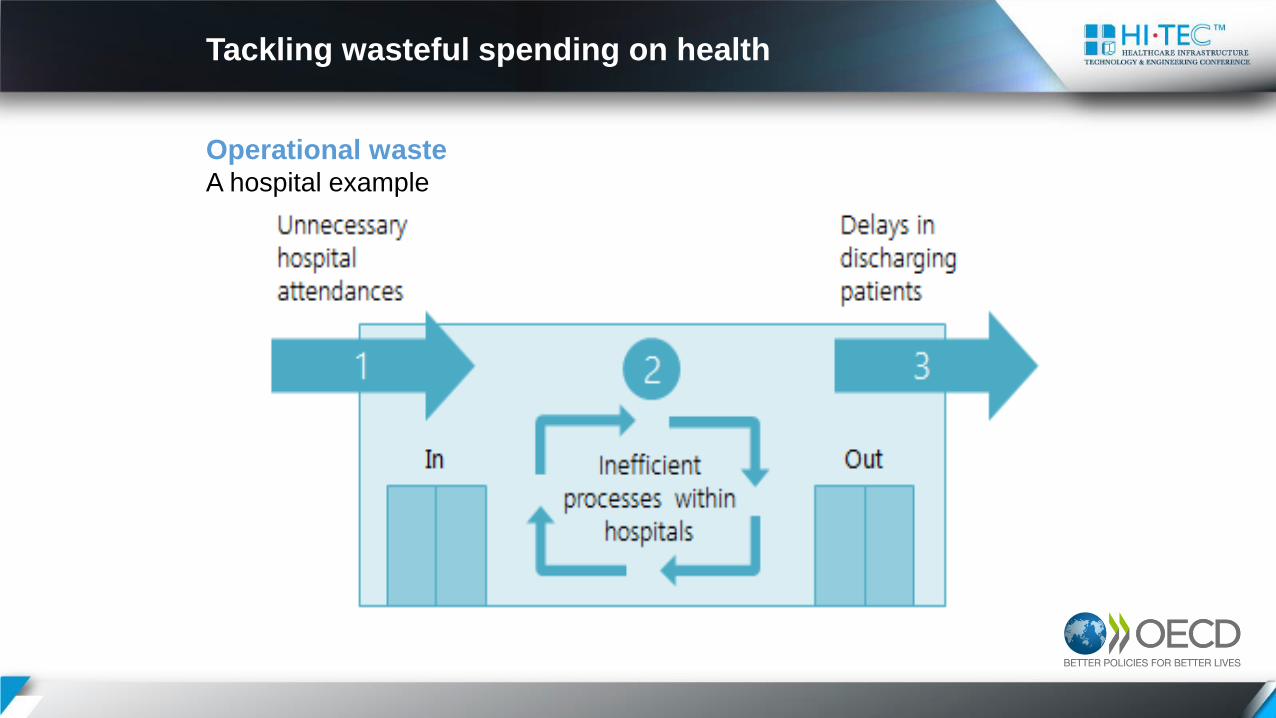
Operational wasteA hospital example
Tackling wasteful spending on health

40 41
48 53 6
6 69 70 73 73 74 9
2 94 96
10
1
11
0
11
3 13
0
13
3
13
6
13
7
14
1
14
1
14
3
14
8
15
1
15
1
17
1
18
7
19
2
19
7
20
4 21
8
22
2
22
5
26
6 28
1
29
2
0
50
100
150
200
250
300
350
4002010 2015
Age-sex standardised rates per 100 000 population
191
Operational waste Hospital admissions for chronic conditions are often avoidable
Diabetes hospital admission in adults, 2010 and 2015 (or nearest year)
Tackling wasteful spending on health

Operational waste Ambulatory surgery is developing at an uneven pace
86.3
73.6
73.5
70.8
67.9
63.3
55.6
53.0
49.8
47.8
42.8
37.9
34.1
30.6
30.4
24.2
21.0
18.3
10.7
8.8
6.6
5.9
3.7
3.7
0.1
0.0
0.0
0
20
40
60
80
100
2000 2015
%
Share of tonsillectomy carried out as ambulatory cases, 2000 and 2015 (or nearest year)
Tackling wasteful spending on health

Operational waste The share of generic continues to be low
28
71
3631
39
45
28
17
40
19
29
48
25 23
16
2320
17 18 16 1712
15 16
2318
86
86 8481
79 7875
73 7270
61
5553 52 50 49 48 47
42 4239
3634
32 30
24 2219
11
0
30
60
90Value Volume
%
Share of generics in the total pharmaceutical market, 2015 (or nearest year)
Tackling wasteful spending on health
Operational wastePolicy levers to better target hospital use
• Payments and financial incentives:
– To promote day-surgery
– Bundled or population-based payments to incentivise delivery in the
right setting (Best Practice Tariffs in England, Sweden)
• Behavioural change for providers and patients:
– Clinical guidelines, disease management
– Self-management by patients, education campaigns
• Strengthening of alternative services:
– Out-of-hours services can be provided by on-call physicians,
dedicated fleets (SOS médecins France), larger Primary Health Care
facilities (Norway) or community services (US rapid access clinics)
– Hospital at Home model (France)
Tackling wasteful spending on health

Governance-related wasteA low-hanging fruit?
• Only represents 3% of health spending on average
• Differences in level of administrative costs are largely
driven by institutional features:
– Multiple-payer systems cost more than single-payer ones
(whether SHI or a government entity)
– Private insurance schemes have higher administrative costs
• Still, functional (Australia) and multi-stakeholder reviews of
processes (Germany, the Netherlands) help identify
administrative processes and structures that add little value
Tackling wasteful spending on health

Governance-related wasteA third of OECD citizens believe the health sector is corrupt
Tackling wasteful spending on health

Governance-related wasteTackling various forms of fraud and corruption
• Detection, prevention and response to fraud in the delivery
and financing of care:
– Dedicated and specialised departments
– Proactively seek to identify problem areas (data mining,
campaigns targeted at types of care susceptible to abuse)
– Organise and phase responses (from information campaigns
targeting outliers to investigations of abusive practices)
• Combat inappropriate business practices
– Mostly rely on self-regulation (code of conducts, conflict of
interest policies)
– Increasingly, some practices are being regulated (Sunshine-
type of regulations mandating disclosure of financial ties:
US, France)
Tackling wasteful spending on health

Where to start: A chicken and egg situation
Saturation of existing
resources partly due to misuse
Tackling unnecessary
use
Releasing resources –
physically and financially
Investment
Design for the new
reality of care
Tackling wasteful spending on health

Where to start?
• Reducing wasteful clinical care could release significant
amounts of resources
– Patients and health care providers must be on board
• Administrative waste or loss to fraud and corruption is
present in all systems and should not be tolerated
– Magnitude of potential savings is relatively modest
• Eliminating operational waste is most complex
– Little evidence on policies that work
– Can pave the way for efficiency-enhancing systemic changes,
including hospital restructuring
Tackling wasteful spending on health

Levels and solutions: Acknowledge
• All OECD countries are explicitly (or not) already engaged
in activities which aim to tackle waste
• Netherlands (2013): Created a hotline and website where
stakeholders could report anonymously instances of waste,
which this led to a series of measures in the area of drugs
and medical devices, long term and curative care
• A difficult but worthwhile conversation
Tackling wasteful spending on health
Levels and solutions: Inform
• Simple comparisons are a good starting point
– Atlas variations in the volume of services (10 countries) –
2014 OECD study
– Price variations: UK NHS Atlas (2014) wristbands for hospital
patients (twofold), needles (47% variation)
• Reporting and learning systems of adverse events
• More robust and rich information systems
– Limitations of many administrative data systems
– PROM-PREM: Value and safety from the perspective of care
recipient
• Making information public can effectively support
behavioural change (IGAS France on cases of fraud)
Tackling wasteful spending on health
Levels and solutions: Pay
• Base coverage decisions on value
– 19 countries use Health Technology Assessment (HTA)
disinvestment (SiNats in charge of HTA since 2015)
– Australia’s on-going benefit schedule review
• Payment systems
– Fee-for-service encourage volume irrespective of
appropriateness and deter coordination
– Bundled or population-based payments are increasingly used
to incentivise delivery in the right setting
• Procurement (SPMS – Portugal)
• Investing in alternatives (Primary care and FHU,
Coordinating Units for Diabetes)
Tackling wasteful spending on health

Levels and solutions: Persuade
• Importance of behavioural change
• Public campaigns
– Choosing Wisely® campaign in a third of OECD countries
• Combined with individual-level interventions: Clinical
guidelines, audit and feedback
• Importance of engaging stakeholders
– Encouraging self-management and self regulation in patients
• Supporting tools (e.g. e-prescription, decision aids)
Tackling wasteful spending on health

Thank You