david o. freedman, md - moema
TRANSCRIPT
Global Travel Health Risks 2015
David O. Freedman, MD • Professor of Medicine and Epidemiology
• University of Alabama at Birmingham
• Medical Director, Shoreland Travax
MOEMA 2015 Conference
East Lansing, Michigan, USA
September 18, 2015
Ebola Situation
• Sierra Leone: 13,600 cases (3,950 deaths)
– Current case incidence: approx. 1 case per week
• Guinea: 3,790 cases (2,520 deaths)
– Current case incidence: fewer than 3 cases per
week
• Previously EVD-Affected Countries Currently EVD-
Free
– Liberia, Mali, Nigeria, Senegal, Italy, Spain, the
U.K., and the U.S.
The Semen Debate
• Survivor infected a female (who died), 6 months later
• Duration of infectivity after recovery now unclear
(seems rare)
• Can a survivor “seed” another country and introduce
disease

Initial High-Level Assumptions
• Any hospital can care for an Ebola patient even when dedicated
containment units exist in the US
• Basic personal protective measures, even if effective, are simple to
implement with 0% error rate
• Patient confidentiality overrides public health
• Contacts can reliably self-isolate at home or follow voluntary
restrictions
• Certain subsets of direct caregivers (Africa or US) can be classified
as low-risk
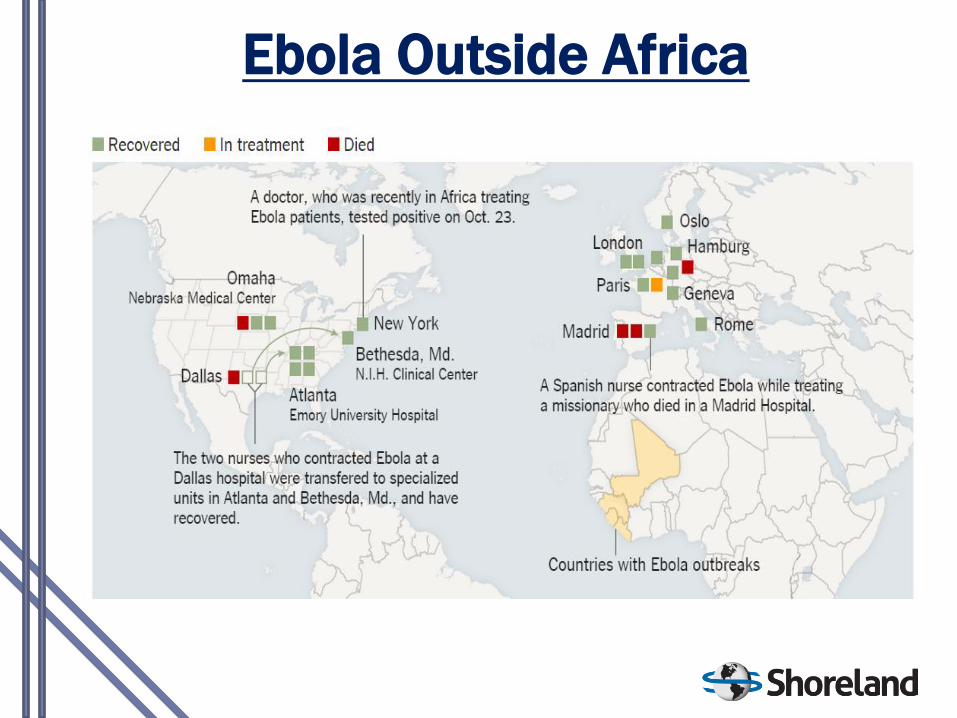
Ebola Outside Africa


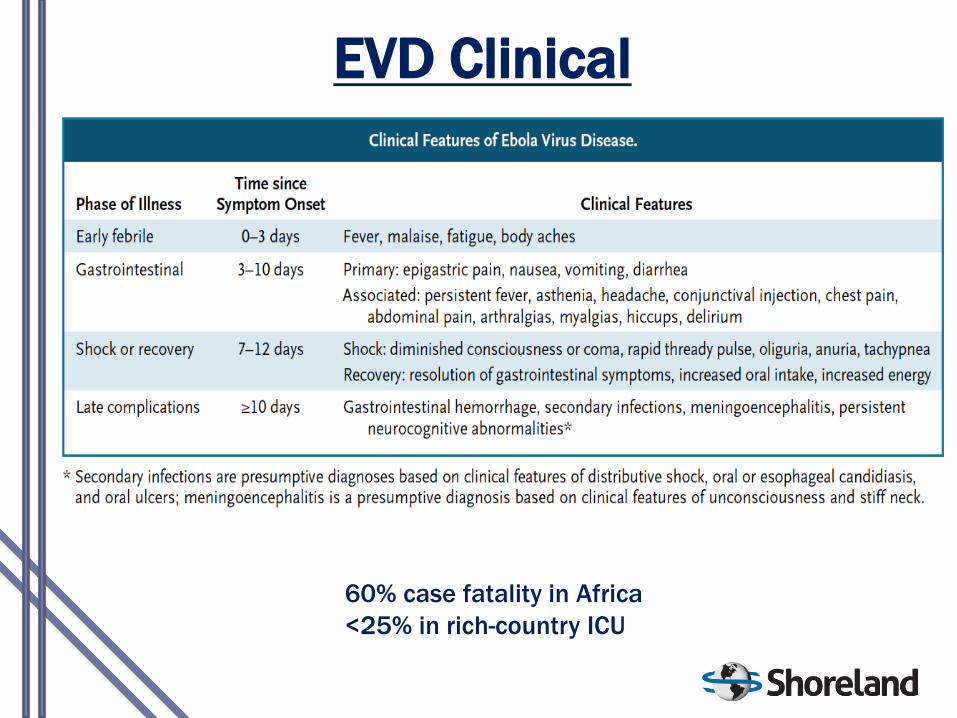
EVD Clinical
60% case fatality in Africa
<25% in rich-country ICU
Treatment is Supportive
• Early use of anti-emetics and anti-diarrheals
• Correcting often profound hypovolemia due to diarrhea and
vomiting, which may exceed 5 L/day; uncorrected hypovolemia
results in irreversible and fatal shock during the third phase of
illness
• Close monitoring and correction of profound hypokalemia,
hypocalcemia, and hyponatremia using both oral and
intravenous routes
• Maintaining blood pressure and oxygenation
• Treatment for any complicating infections
Mode of Transmission
• Human to human
– Minor contamination may be sufficient but direct contact
with human fluids in care settings
– Blood, body fluids including diarrhea, vomit, saliva, sweat,
urine, semen, breast milk
– Risk proportional to amount of virus in blood/fluid
• Mention doffing issue
– Mounting experience of no transmission early in clinical
course
• No airborne transmission
– Animal studies flawed
• No patient discharged until virus-free
• Bats, bushmeat, primates, no role in 2014
Environmental Survival
& Decontamination
• Experimental studies have yielded conflicting
results
– Most recent data indicate that virus survives
longer in a controlled hospital environ (up to 8-
13 days) than in a tropical environ
– In artificial studies introducing large amounts of
virus onto surfaces, virus can survive for several
days
• Normal hospital cleaning eliminates virus from
fomites and surfaces
• Very sensitive to all disinfectants
– Alcohol, Clorox, etc.
– Moderately sensitive even to UV light

Household & Public Transmission
• 16% household transmission rate
– Restricted to those with direct contact with EVD
infected person
– No transmission in Dallas, New York
• No aircraft related cases to date
– HEPA filtration in airliners
• No proven cases in HCWs in Africa without direct
patient contact
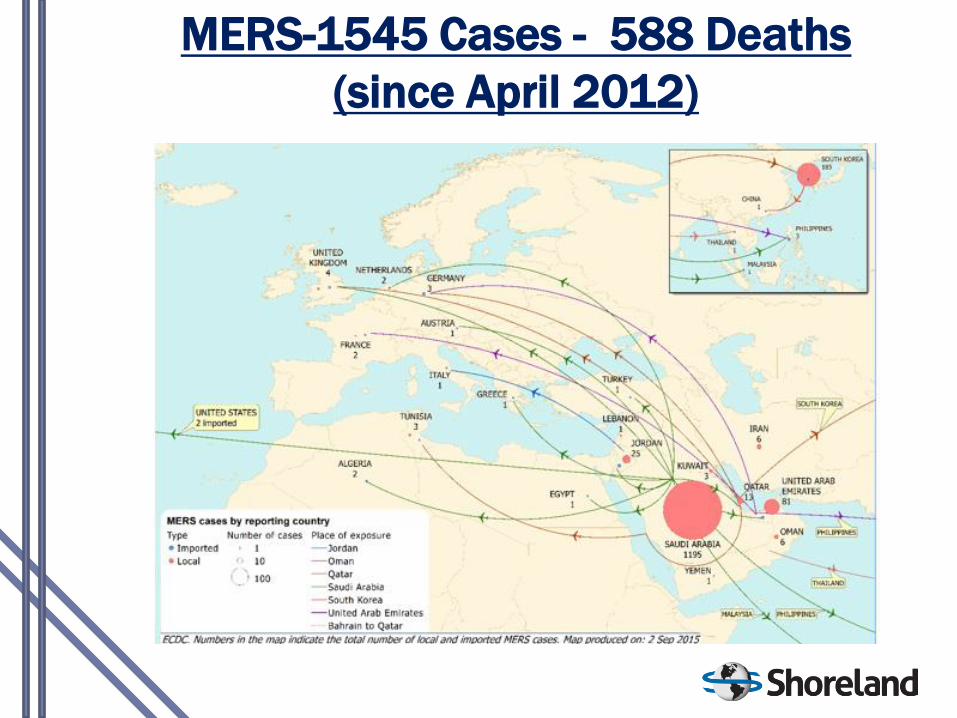
MERS-1545 Cases - 588 Deaths
(since April 2012)
MERS - Current Situation
• 1195/1545 cases from KSA
• Currently about 30 cases/week in KSA
– Cluster in Riyadh linked to King Abdulaziz Medical City
• Hajj?
– Cases during or after are anticipated due to recent case surge
• Current outbreak in Amman, Jordan
– 8 cases; index case traveled from Jeddah, KSA
• 29 exported cases total
– Last one June to Philippines
• Low risk to non-Mideast countries
• Still no known effective treatment
• Basic virus parameters still poorly studied

Summary of MERS Advice
• Usual handwashing/hygiene messages
• Good food hygiene including camel products and any undercooked meat.
• No contact with animals especially camels
• Avoid contact with ill-people in KSA
– avoid medical facilities in KSA including Riyadh
• Ill returned travelers to inform of travel history
• Contact, droplet +/-airborne precautions
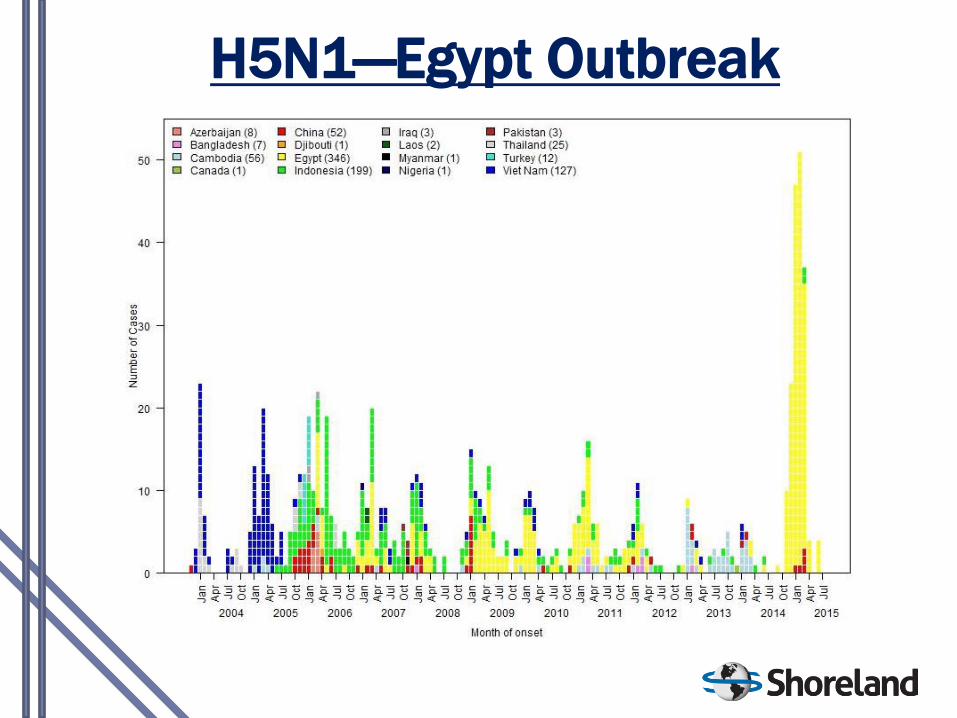
H5N1—Egypt Outbreak
H5N1
• Egypt-~130 cases in 2015
– Highest numbers of cases in 4-month period ever (Jan-Apr= 132
cases)
– Sudden silence from the Egyptian government until late June with
4 additional cases reported
• New phylotype (sub-clade) now dominant in poultry and likely humans
– Implications for increased transmission unclear
– No clusters or human chains
• 21 different Governorates, 17 recently
– Mostly Cairo, Assyut, Al Minya
• Move to new 2.2.1 vaccine candidate strains
Respiratory Threats - LPAI
• 3rd wave: 217 H7N9 cases in China since 10/14
– Guangdong, Fujian, Jiangsu, and Zhejiang
– 677 cases, 275 deaths since 2/2013
– 17 cases since June 1 (as a result of warmer
weather)
• Cases exported to HK, Taiwan, Malaysia, Canada
• Reassortment of avian strains
– Bird to human almost exclusively; birds not ill
• Nothing clinically distinct
– Tamiflu sensitive

Threats - Other H5, H9
• Birds: H5N2, H5N3, H5N6, H5N8
– Increasing detection in birds in US, Canada,
Europe, Asia, West Africa
– No human cases so far
• H5N6—4 human cases from China
• H9N2
– 3 cases Egypt, China
– Mild human disease

• December 2014 to June 2015
o No human cases and negligible risk
• Poultry, captive birds, wild birds
o H5N2, H5N3, H5N6, H5N8
• 21 states
o 15 states with domestic poultry
affected
• Losses in the billions in Iowa alone
o 30 million hens, 1.5 million turkeys
lost
Avian H5NX in the USA
• Meta-analysis of individual patient data from all available randomized
placebo-controlled trials
• accelerated time to alleviation of all clinical symptoms by approximately
1 day (from 122.7h to 95.7h), halved the risk of lower respiratory tract
complications requiring antibiotics (8.7% to 4.2%), and reduced the risk
of admittance to hospital for any cause by 63% (from 1.7% to 0.6 %)
• increased the rate of nausea and of vomiting (1.60-fold and 2.43-fold,
respectively).
• Patients with influenza-like illness not due to influenza virus experienced
only the adverse effects of oseltamivir.
• data are still scanty for children and certain other groups
Kelly H, Cowling BJ.
Influenza: the rational use of oseltamivir. (Lancet Jan 29, 2015)
Risk Assessment
Advice to Reduce Exposure to Health Risks
Immunization
Chemoprophylaxis
Advice for Self-treatment
The Pre-Travel Consultation
• Perform Risk Assessment
• Educate on Basic Preventive Measures
• Provide Immunizations
• Provide Malaria Prevention (if indicated)
• Educate on Travelers Diarrhea
• Reinforce Other Health Concerns
Elements of the Patient Encounter
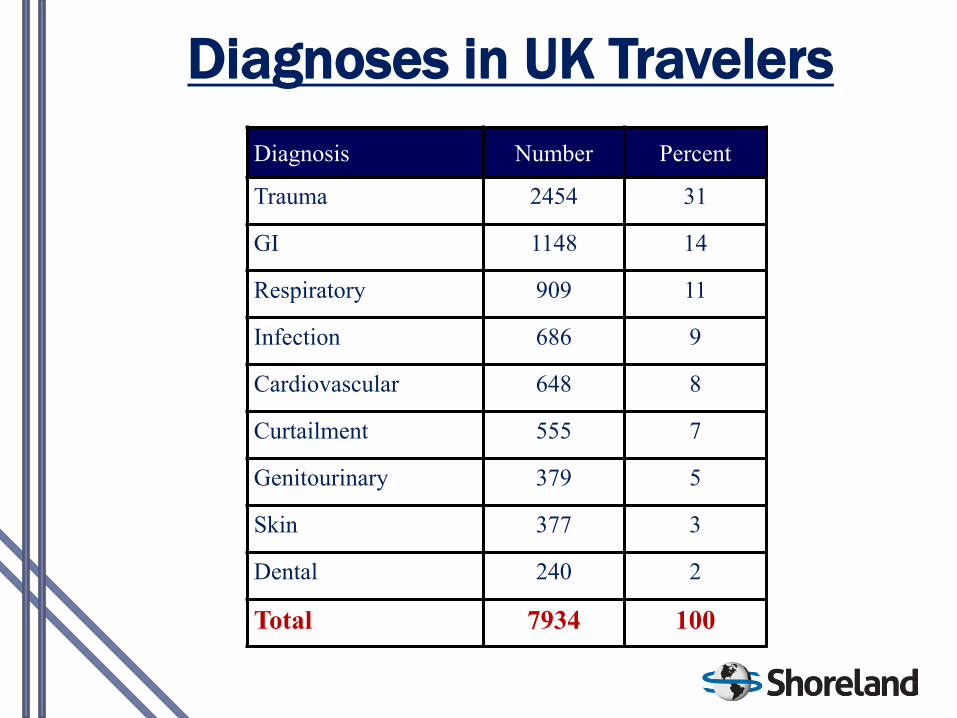
Diagnoses in UK Travelers
Diagnosis Number Percent
Trauma 2454 31
GI 1148 14
Respiratory 909 11
Infection 686 9
Cardiovascular 648 8
Curtailment 555 7
Genitourinary 379 5
Skin 377 3
Dental 240 2
Total 7934 100
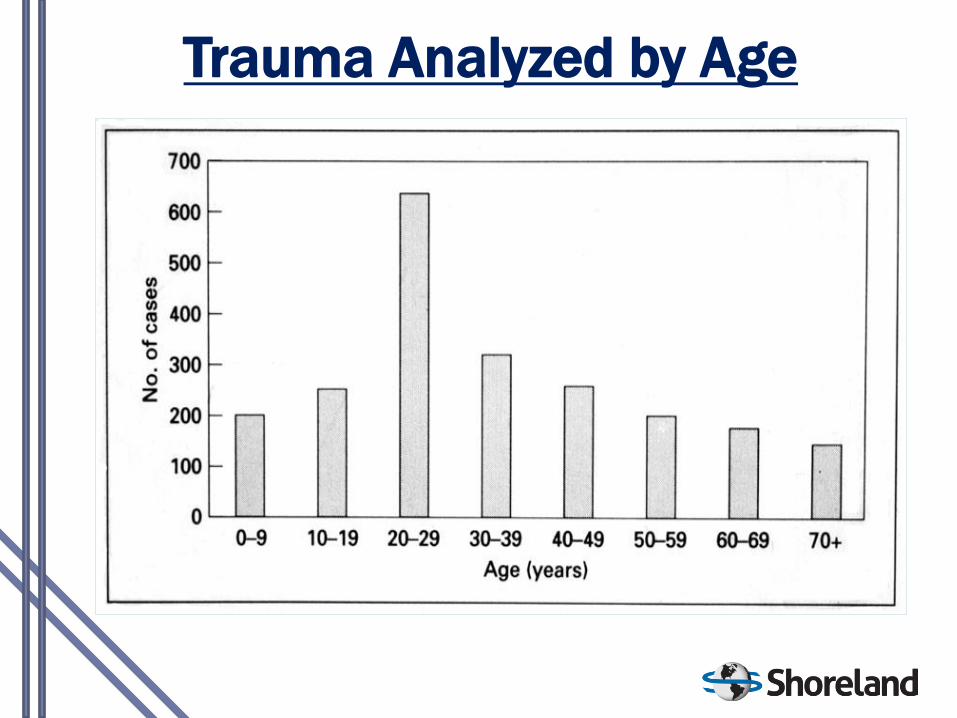
Trauma Analyzed by Age
• Malaria-free
– 2014: Sri Lanka, Argentina, Bahamas
– 2013: Georgia, Kyrgyzstan, Jamaica, and Uzbekistan
• Reminder: No chemoprophylaxis (negligible risk)
– Costa Rica, El Salvador, Paraguay, Turkey, Azerbaijan,
Tajikistan, Cape Verde, Greece
Malaria Changes

No Chloroquine Available in US
• No return date known
– Only generics made overseas were on the market
• Can use hydroxychloroquine (400 mg 1X/wk or >100 mg/day
• Atovaquone/proguanil (malarone) use is predominant anyway even in
chlorquine sensitive areas and equally effective

MRE: Unwanted
Souvenirs for Travelers
• Colonization of fecal flora with multidrug-resistant
Enterobacteriaceae (MRE) was 50% overall and 70% in Asia.
• Diarrhea during travel and taking ß-lactam antibiotics increased the risk
• Carriage brief, but, at 3 months after returning, 4.7% of travelers were still excreting MRE.
• Impact of this carriage in countries with good domestic hygiene is uncertain.
Travel Immunization
• Updates of Routine Vaccines
• Required Vaccines
– International Health Regulations
• Medically Recommended
– According to risk
• Patient tolerance of risk
• Risk may be behavior related
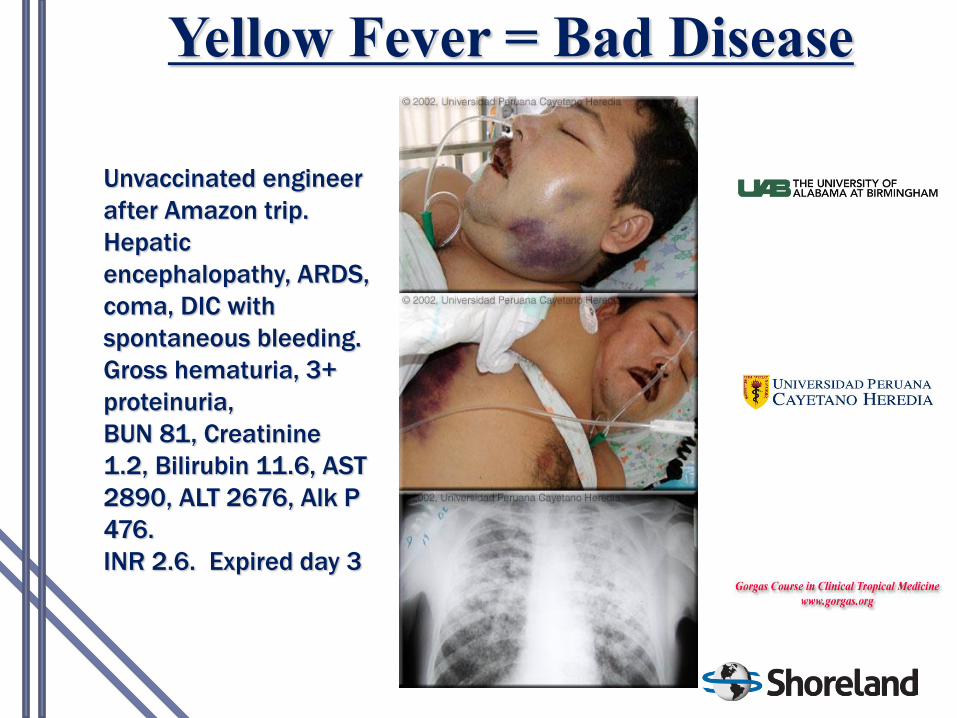
Yellow Fever = Bad Disease
Unvaccinated engineer
after Amazon trip.
Hepatic
encephalopathy, ARDS,
coma, DIC with
spontaneous bleeding.
Gross hematuria, 3+
proteinuria,
BUN 81, Creatinine
1.2, Bilirubin 11.6, AST
2890, ALT 2676, Alk P
476.
INR 2.6. Expired day 3
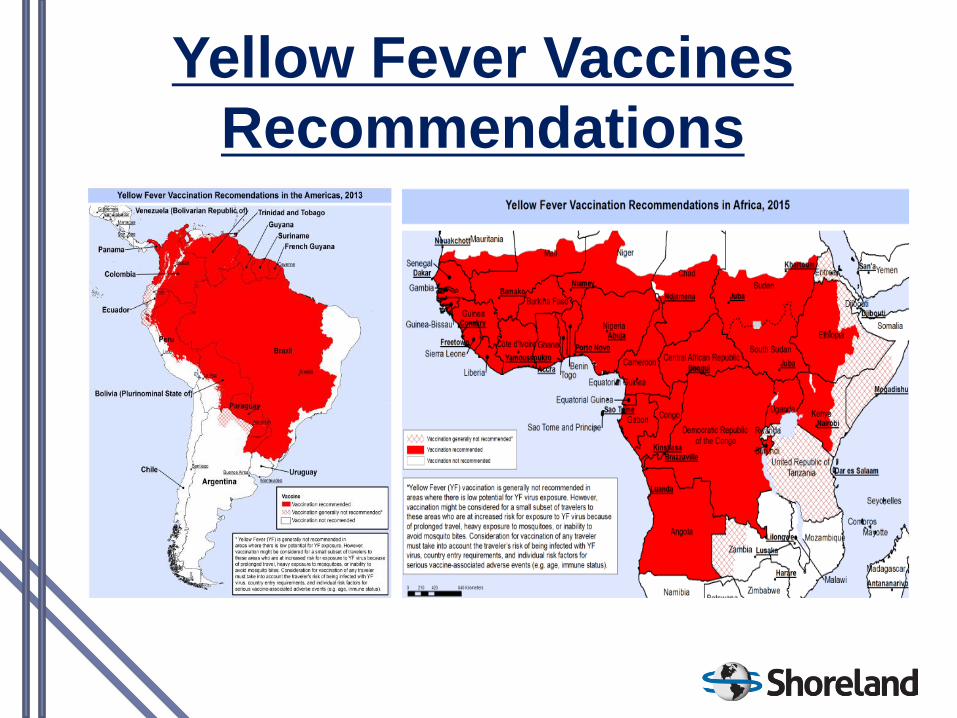
Yellow Fever Vaccines
Recommendations

Entry Requirements
International Health Regulations
(IHR):
• As of May 2014, the IHR have been amended to state an indefinite
validity of an International Certificate of Vaccination or Prophylaxis
(ICVP) for yellow fever vaccination for the purposes of an entry
requirement, no matter when issued.
• This amendment will officially take effect in June 2016.
• Until then, the current IHR-required 10-year limitation on ICVP validity
is still applicable, but countries are permitted to accept indefinite
validity if desired.

10 Years or Not?
• WHO approach is based on the rationale of no proven (2 reported) late
YF cases in previous vaccinees
• WHO concerned with vaccine sparing in endemic countries not
health of individual travelers
• Legacy 10 year rule not evidence-based
• Sero-surveys of varying methodologies indicate that up to 15% may
lose immunity after 10-15 years
• Remember: severe reactions to YF-vax don’t occur in re-vaccinees.
– Why not strive for near 100% protection in travelers?
• At the same time, the general durability of immunity is reassuring to
the immunosuppressed and others not eligible for re-vaccination
Collaborative Group for Studies on Yellow Fever Vaccines.
Duration of post-vaccination immunity
against yellow fever in adults. Vaccine. Sept. 3,
2014; 32(39): 4977-4984;
• 691 subjects, male (73%) and aged 18-83 years.
• PRNT testing in Rio de Janeiro
• 30-45 days after YF vaccination, 94% became seropositive.
• The proportion of seropositive subjects declined from 1-4 years to 5-9
years and 10-11 years post-vaccination (94%, 83%, and 76%,
respectively)
• The trend of decline was particularly striking in persons aged 18-30 years
• Immune response in different sub-populations requires further
assessment
Duration of Immunity for
Personal Protection
Due to the transition in the IHR requirements,
WHO and national recommendations on duration
of immunity for personal protection for travelers
who have true exposure to yellow fever virus risk
vary somewhat and the broad wording of
individual guidelines generally require some
individual clinician interpretation on a patient-by-
patient basis.
CDC 2015: YF Vax Boosters q10yr
• Long-stay travelers to any area at risk for yellow fever
transmission
• All travelers spending any time in high risk areas such
as West Africa
• All travelers to any area with a current outbreak
• All persons who were infected with HIV at last vaccine
• Laboratory workers who handle yellow fever virus
• Women who were pregnant at their initial dose should
receive a booster once before their next risk travel
(may be < 10 years).
• Persons who received a hematopoietic stem cell
transplant after receiving a dose of vaccine and who
are now sufficiently immunocompetent should be
revaccinated once before their next risk travel (may be
< 10 years).
CDC 2015: Considered to have
“long-term” immunity
• Short-stay travel to low-risk yellow-fever endemic areas that are outside
West Africa and other high-risk areas, in which there is no current
outbreak and where no high-risk occupational exposure will occur. (Note:
Such travelers should understand the need for repeat consultation prior
to each subsequent trip to a yellow fever risk area).
• Shoreland recommends that all frequent travelers consider boosters at
10-year intervals if there is any likelihood of meeting any of the criteria for
q10 year boosters in the future.
Measles
• Live virus vaccine
• Born before 1957 = immune
– Epidemiology varies by country, e.g., Canada=1970
• 2 countable doses needed for protection
– what is a countable dose?
• Routine now at 12-15 months & 4-6 years
• If no countable doses – 2 doses at least 1 month apart
• MMR introduced in 1970 as a 1-dose regimen
- Changed to 2 doses in 1991
- 957-1970 birth cohort most likely susceptible
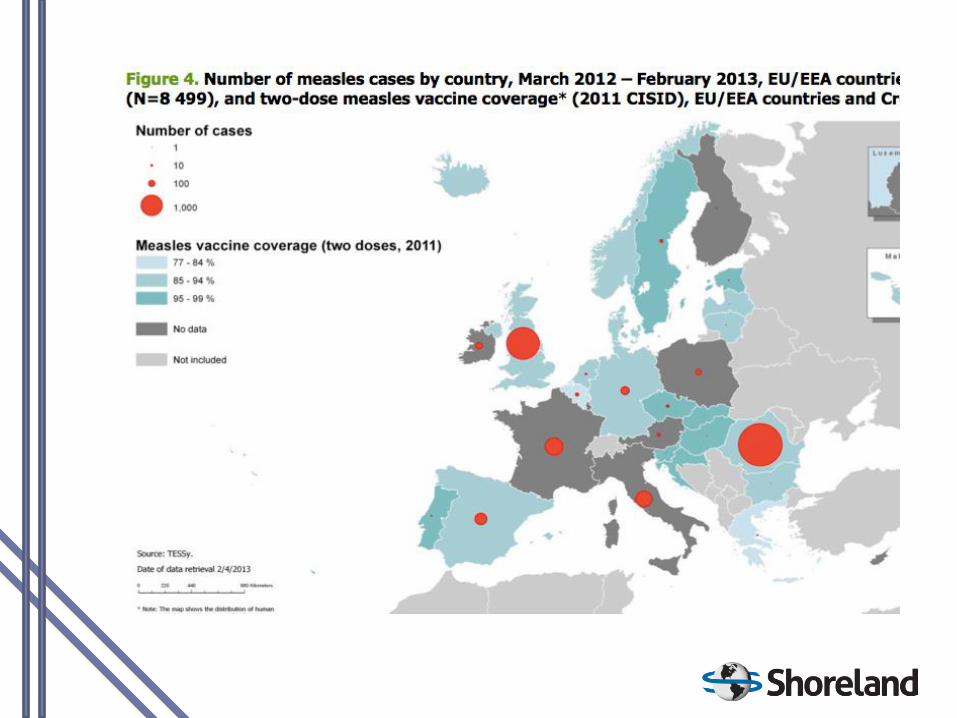

Figure 2. Distribution of measles cases by country, July 2015 (N=173),
and vaccine coverage (two doses, from 2013-2014, WHO), EU/EEA
countries

Rabies & Travelers
• Most controversial of all the travel vaccines
– Low-risk for short tourist trips on most
itineraries
– Bad outcome if acquired
– Vaccine=3 doses over 3 weeks, $$$$ ($600)
• Incubation of disease 9 days to 1 yr
• In US: HDCV, PCEC, and RVA
–Vero cell, DEV, mouse brain etc. elsewhere
• Cost/benefit of vaccine $5 billion per life saved
Rabies Vaccine
• Vaccine
–Given in 3 doses over 21 to 28 days
• ID dosing off-license in all countries
– Indicated for travel to rabies-risk countries, especially long-stay travelers, children, & those with occupational risks
–Post-exposure immunization is necessary even when pre-exposure vaccine has been administered
• Human Rabies Immunoglobulin (HRIG)
–Difficult to obtain during travel
• Newer digested Fab2 ERIG products (Favirab) may be acceptable
–Not needed following a rabies exposure if pre-exposure vaccination was completed

Rabies
• High risk: SE Asia, Africa, India/Nepal, China
• Boosters: No regular boosters recommended,
must get 2 doses post-exposure
• Post-exposure: RIG plus 4-5 vaccine doses
over 14-28 days if no pre-exposure series
Rabies Post-Exposure (ACIP July 2009)
• Post-exposure: RIG plus 4 X 1 cc IM vaccine doses over
14 days if no pre-exposure series
–Days 0, 3, 7,14
–5th dose at Day 28 eliminated for supply reasons
–5th dose retained if immunocompromised
• WHO still recommends 5 IM doses (Essen)
• WHO also recommends Zagreb regimen
–1 cc IM--2 doses on d0, 1 dose d7, 1 dose d21
• Intradermal PEP is for resource-limited settings
Vaccine Industry Shake-up
• Novartis, Baxter, Crucell Exit Vaccine Business
• All Novartis vaccines to GSK
– Except: Novartis Flu Vaccines to CSL
• Baxter Neissvac and TBE Vaccines to Pfizer
• Crucell Vivotif oral typhoid to PaxVax
• Crucell Dukoral to Valneva
• Valneva Ixiaro (?Future distribution; was with Novartis)
Overlapping Aedes
Transmitted Diseases
• Dengue: flavivirus, fever, rash, arthralgia, “break bone fever”,
uncommon progression to hemorrhagic fever, post-viral fatigue
• Zika: flavivirus, fever, rash, no severe manifestations
• Chikungunya: alphavirus, fever, rash, inflammatory arthritis, no
life-threatening manifestations, significant rheumatologic sequelae

2015 Local Chikungunya
in the Americas
Chikungunya-Current Situation
• Current hotspots
– Colombia: currently >3,800 cases/week
– Honduras: currently >2,400 cases/week
– Ecuador: currently >100 cases/week
• Imported cases
– U.S.: 3,124 cases (origin country not reported by CDC)
– France: 464 cases
– U.K.: 239 cases
• No anti-virals, vax candidates still in Phase 1
• Past peak in the majority of Caribbean islands

Chikungunya-Future
• Endemic as a zoonosis in Africa
• Every 40-50 years emerges in worldwide pandemic waves
– 1770, 1824, 1871, 1902, 1923, 1963
• 2005: Current pandemic wave Indian Ocean
• Human populations develop immunity after 2-3 years
• Theoretical risk of enzootic entrenchment in South America;
history against this
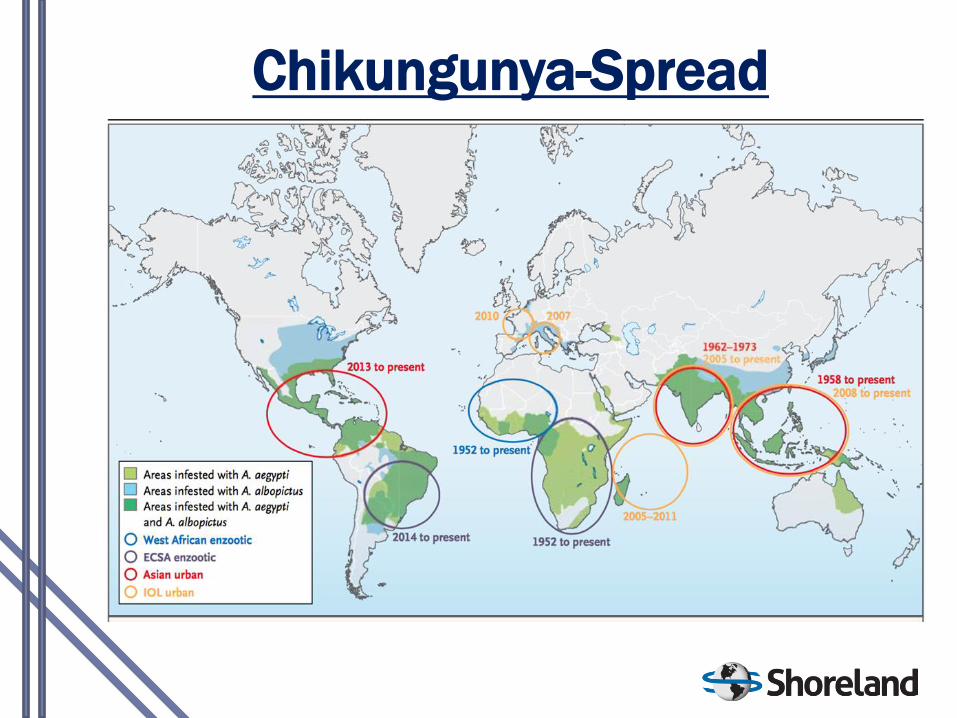
Chikungunya-Spread
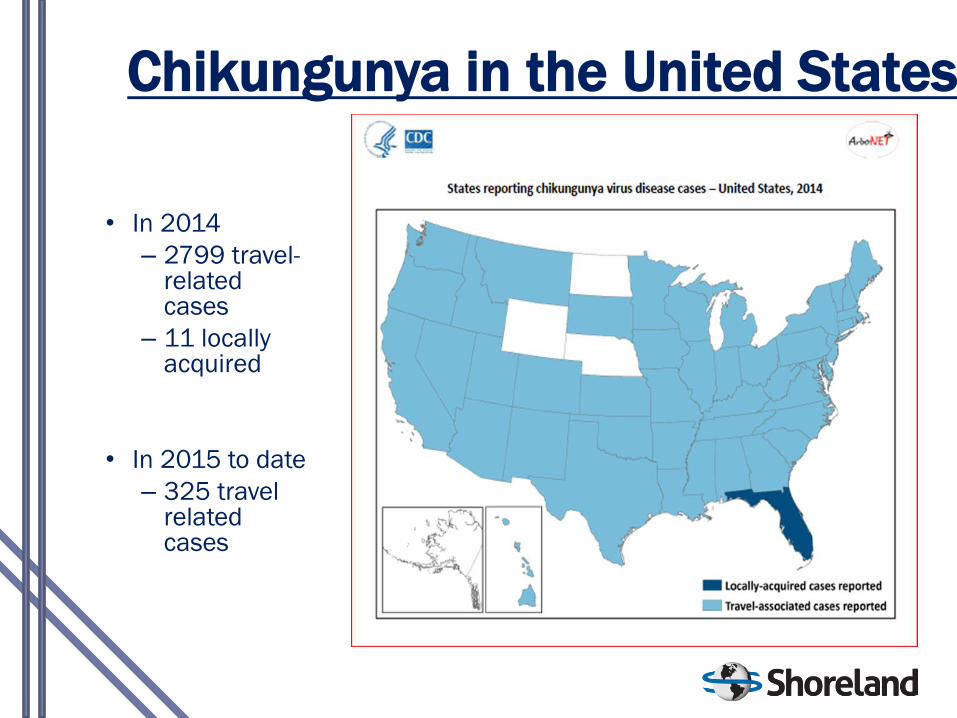
Chikungunya in the United States
• In 2014
– 2799 travel-related cases
– 11 locally acquired
• In 2015 to date
– 325 travel related cases
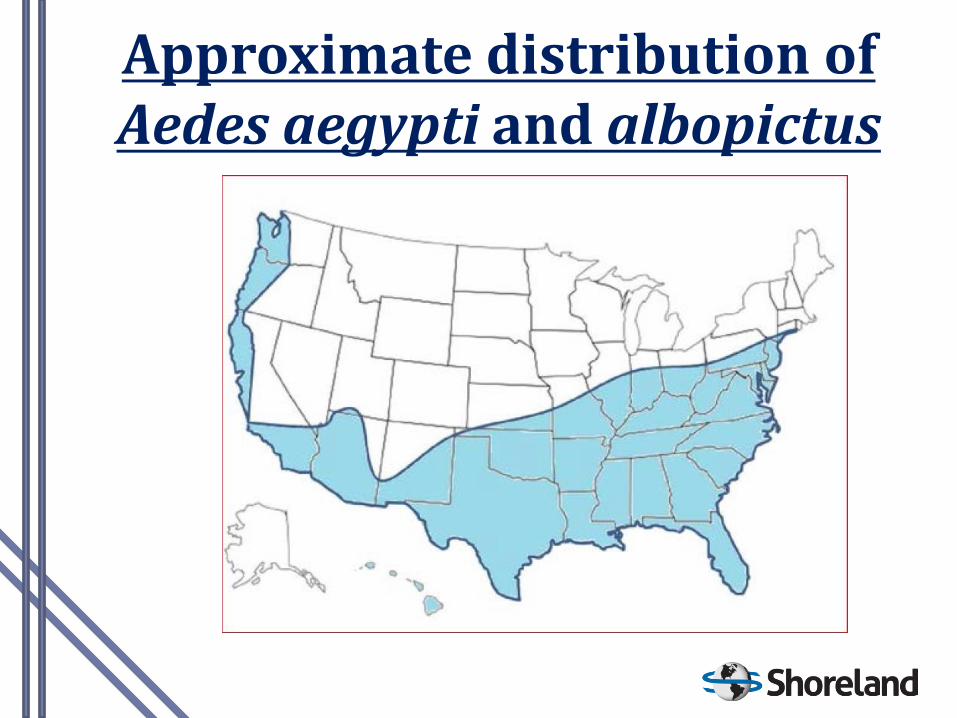
Approximate distribution of Aedes aegypti and albopictus
Enterovirus D68 (non-polio enterovirus)
• 1,153 cases in 49 states 8/14-1/15, then ceased
o Severe respiratory illness in children with
asthma
o ~100 children with acute flaccid myelitis,
association not yet definitive
• Described in 1962 in California
o Only 79 cases reported in US 2009-13
• Multiplex PCR respiratory screening panels
increasing case detection
• Ubiquitous, described in every country
investigated.
• Viral pathogenetic factors and correlates of illness
in early phases of study

What about Canada?
• West Nile
– 2015: 4 cases YTD
• Birds/Horses positive in AB, SK
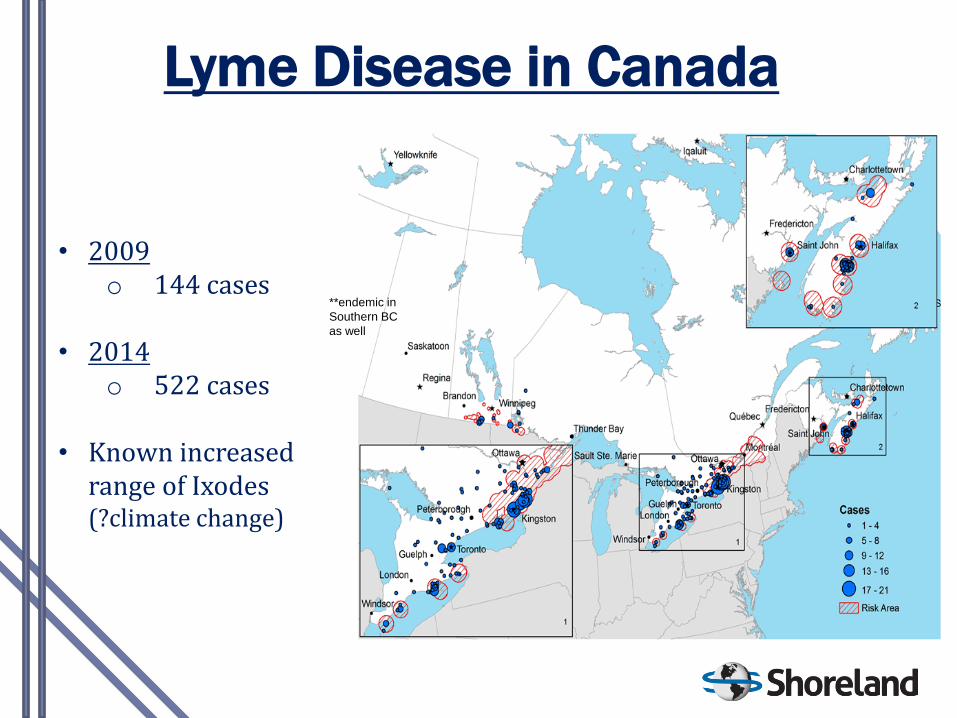
Lyme Disease in Canada
• 2009 o 144 cases
• 2014
o 522 cases
• Known increased range of Ixodes (?climate change)
**endemic in
Southern BC
as well

Summary - Lesson of Asking :
Where Have you Been?
• Where have
you been? Additional lesson from MERS – South
Korea vs Thailand

Thank You!
David O. Freedman, MD • Professor of Medicine and Epidemiology • University of Alabama at Birmingham • Medical Director, Shoreland Travax • [email protected]