dementia-friendly dentistry
TRANSCRIPT

Dementia-Friendly Dentistry
Good Practice Guidelines


iDementia-Friendly Dentistry Faculty of General Dental Practice (UK)
Dementia-Friendly Dentistry
Good Practice Guidelines
EDitor: Paul BatchelorBDS, DDPH(rCS) MCDH, MPH,
PHD, FFDGP(UK), FDS, FFPH.
FEllow anD ViCE DEan, FGDP(UK) anD Honorary SEnior lECtUrEr,
UniVErSity CollEGE lonDon (UCl).

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)ii
Published byFaculty of General Dental Practice (UK)london
Email: [email protected]: www.fgdp.org.uk
iSBn: 978-1-5272-1390-6
First edition published 2017
© Faculty of General Dental Practice (UK) 2017all rights reserved. no part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopied, recorded or otherwise, without the prior written permission of the Faculty of General Dental Practice (UK).
while every effort has been made to ensure the accuracy of the information contained in this publication, no guarantee can be given that all errors and omissions have been excluded. the Faculty of General Dental Practice (UK) can accept no responsibility for loss occasioned to any person acting or refraining from action as a result of material in this publication.
all commerical product names carry the trademark of their manufacturer.
Editorial production: amy Brewerton, Jamie woodward Design: tU ink Print management: tU ink
Dementia-FriendlyDentistry

iiiDementia-Friendly Dentistry Faculty of General Dental Practice (UK)
C o n t E n t S
ForEworD
aCKnowlEDGEMEntS
PrEFaCE
1. PRINCIPLES BEHIND CARE MANAGEMENT
1.1 introDUCtion
1.2 DiaGnoSiS oF DEMEntia
1.2.1 the importance of a diagnosis
1.2.2 the progressive development of dementia
1.2.2.1 Before dementia becomes apparent
1.2.2.2 Dementia as a progressive condition
1.2.2.3 Rate of progression
1.2.2.4 The staged development of dementia
1.2.2.4.1 Early (‘mild’) stage
1.2.2.4.2 Middle (‘moderate’) stage
1.2.2.4.3 Late (‘severe’) stage
1.3 KEy PointS in tHE DiaGnoSiS
1.3.1 Signs and symptoms of dementia
1.3.2 associative medical conditions
1.3.2.1 Cardiovascular factors
1.3.2.2 Depression
1.3.2.3 Other conditions
1.3.2.4 Lifestyle factors
1.4 SUMMary
1.5 rEFErEnCES anD rESoUrCES
vii
ix
xi
1
1
2
2
3
3
4
5
6
6
7
8
9
9
10
10
11
11
11
12
13

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)iv
2 PRINCIPLES OF CARE PROVISION
2.1 GEnEral ConSiDErationS
2.1.1 Pre-examination
2.1.1.1 Personal information
2.1.1.2 Medical history
2.1.1.3 Socio-behavioural history
2.1.1.4 Dental history
2.1.1.5 Communication
2.1.2 Early stages of dementia
2.1.3 later stages of dementia
2.2 ManaGEMEnt oF DEMEntia PatiEntS
2.3 PraCtiCE SUrGEry DESiGn
2.4 ProViSion oF CarE oUtSiDE DEntal PraCtiCES
2.4.1 Care homes
2.4.2 Domiciliary care
2.5 trEatMEnt PlanninG
2.5.1 Drugs and dental problems
2.5.2 Consent and capacity
2.6 DEMEntia anD DEntal ConDitionS
2.6.1 Bruxism
2.6.2 Chewing and swallowing
2.6.3 Denture wearing
2.6.4 Denture marking
2.7 SUMMary
2.8 rEFErEnCES anD rESoUrCES
C o n t E n t S ( C o n t i n U E D )
15
15
16
17
17
18
19
19
24
25
25
26
27
27
27
29
29
30
31
31
32
32
33
34
35

vDementia-Friendly Dentistry Faculty of General Dental Practice (UK)
3 IMPLICATIONS FOR DENTAL PROFESSIONALS
3.1 GEnEral iMPliCationS
3.2 How to raiSE ConCErnS anD aPProaCH tHE SUBJECt oF DEMEntia
3.3 PotEntial inDiCatorS oF DEntal ProBlEMS in PEoPlE
liVinG witH DEMEntia
3.4 MEDiCation
3.4.1 what are the main drugs used in the management of dementia?
3.5 tyPES oF DEntal trEatMEnt
3.5.1 Early stages of dementia
3.5.2 Middle stages of dementia
3.5.3 later stages of dementia
3.6 aDDitional iSSUES
3.7 KEy StanDarDS
3.7.1 Medical history
3.7.2 Side effects
3.7.3 Planning treatment
3.7.4 Consent and capacity
3.7.5 Safeguarding
3.8 SUMMary
3.9 rEFErEnCES anD rESoUrCES
4 SUPPORT MATERIALS AND FURTHER READING
4.1 introDUCtion
4.2 StaFF traininG anD awarEnESS
4.3 loCal SUPPort nEtworKS
4.4 PatiEnt inForMation lEaFlEtS
4.5 SElF HElP
4.6 rEFErEnCES anD rESoUrCES
39
39
40
41
42
42
44
44
45
46
47
47
48
49
49
51
54
57
57
59
59
59
60
61
61
61
C o n t E n t S ( C o n t i n U E D )

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)vi
APPENDICES
a1 SElECtED DEFinitionS
a2 aBBEy Pain SCalE
a3 CoMMUniCation ViSUal aiD
a4 aDaPtED HanDlE tootH-BrUSHinG aiDS
a5 tECHniqUE For aSSiStED BrUSHinG
a6 CliniCal DEMEntia ratinG (CDr)
C o n t E n t S ( C o n t i n U E D )
62
62
63
65
66
67
68

viiDementia-Friendly Dentistry Faculty of General Dental Practice (UK)
the core function of the Faculty of General Dental Practice (UK) is to raise the
standards of care delivered to patients. to help achieve this, the FGDP(UK) engages
with a number of bodies where a multidisciplinary approach may help in designing
care provision and where the profession and the public may benefit from guidance
on how best care can be assured. one of the tasks facing all care professionals
surrounds how best to address conditions that arise due to the evolving
epidemiology of diseases. indeed, the successes of previous care modalities can
themselves create new challenges that, when combined with other factors, mean
the management of patients may be more complex when compared to previous
cohorts of patients.
with the welcome increase in life expectancy, some conditions take on a growing
importance. Dementia is now one of the most common neurological disorders in
people aged 65 or older, although a growing number of cases are identified at earlier
ages. Estimates suggest that the prevalence in the UK population is about 5%, with an
annual incidence of 2%. over 850,000 people live with dementia in the UK presently,
a figure predicted to rise to over a million by 2021. Dementia leads to a continual
decline in all aspects of an individual’s ability to function, along with increased levels
of anxiety and depression. there is a need to improve overall care for people with
dementia, emphasised by governments in the UK and many other countries.
the aim of the present document is to provide the dental profession and their teams
with guidance on how they can help ensure the best contribution to individuals living
with dementia. oral health care for individuals with dementia is one aspect where
improvements can make a substantial difference to an individual’s quality of life. to
reach high standards of oral health, a relationship between the individual and those
F o r E w o r D

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)viii
tasked with care provision is required. Furthermore, the progressive nature of dementia
means that these responsibilities may change as the disease impacts on the ability of
individuals to contribute to the maintenance of their health through self-care.
the state of oral tissues impacts not only on an individual’s oral health but also on
their quality of life in general. negative developments in eating habits, socialising
and general wellbeing all arise through poor oral health. the dental profession can
not only play a major role in reducing morbidities associated with poor oral health,
but help ensure the achievement of such goals. However, this requires the
development of guidance to help achieve this work.
this publication, developed to help mark our 25th anniversary as the academic
home for primary dental care, is an adjunct to the current documents; it aims
specifically to help support the provision of care to patients living with dementia.
Mick Horton
Dean, Faculty of General Dental Practice (UK) – 2017

ixDementia-Friendly Dentistry Faculty of General Dental Practice (UK)
WORkING GROUP
Paul Batchelor (Editor)
Emma Bould
Blánaid Daly
richard Emms
linda Hillman
Bryan Harvey
John Milne
with special thanks to the alzheimer’s Society
ACkNOWLEDGEMENTS
the Faculty of General Dental Practice (UK) would also like to express its
thanks to the following organisations and individuals for their review,
comments and other support during the development of this document:
British Dental association
British Geriatrics Society
British Society of Gerodontology
Care England
Care quality Commission
the Dental Defence Union
Eastman Dental Hospital Special Care Dental Department
the Flintshire Dementia Dental Care Pathway Development team
Health Education England
Health Education England thames Valley and wessex
Healthwatch England
london Dementia Clinical network
a C K n o w l E D G E M E n t S

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)x
the Medical and Dental Defence Union of Scotland
nHS Cheshire and Merseyside local Dental network
nHS Cheshire and Merseyside Special Care Dentistry Managed Clinical network
nHS Education Scotland
nHS South Central Special Care and Paediatric Dentistry Managed Clinical network
oral Health Foundation
Public Health England
Society of British Dental nurses
welsh Government
David arnold
Shirley Bain
andrew Boaden
Sarah Buckingham
Dominic Carter
Hana Cho
Janet Clarke
laura Cook
aubrey Craig
ian Davies-abbott
onkar Dhanoya
Fiona Ellwood
Jonathan Farmer
Jonathan Gardam
lesley Gough
Daniel Harwood
rowan Harwood
roger Hollins
Mick Horton
lisa Howells
rachel Hutchings
Charlotte Jeavons
quentin Jones
Vicki Jones
Katy Kerr
navdeep Kumar
Stephen lambert-Humble
John l Makin
Jose Marshall
Susan nelson
rebecca owen-Evans
abhi Pal
Helen quinn
Michele Seager
rowenna Spencer
Pearse Stinson
Joe Sullivan
Patricia thomson
Devika Vadher

xiDementia-Friendly Dentistry Faculty of General Dental Practice (UK)
P r E F a C E
to help the dental practitioner ensure standards, the present document is divided
into a number of sections. For those that are dental-specific, standards of care are
described to help ensure the qualities of care can be achieved. these standards
have used published material and existing guidance that cover dementia care
provision and the guidance material has adopted the ‘aBC’ approach of existing
FGDP(UK) published guidelines.
we have categorised recommendations as A (aspirational), B (basic) and C
(conditional upon circumstances). no practitioner should be censured for failing
to meet A grade recommendations. nor does a failure to meet B or C grade
recommendations necessarily imply negligence on the part of the clinician.
a clinician must assess each patient on their merits, in the circumstances in
which they find themselves, and with the evidence available to them they must
use their clinical judgement to settle on a course of action. it is possible to fail
to adhere to our recommendations and still be acting in a patient’s best interests.
However, we would recommend that when taking a course of action other than
that recommended in these guidelines, a clinician should be able to justify their
reasoning and record it in the patient’s records.
the present document is divided into four main sections. in the first, background
material dealing with the principles of care management, the epidemiology of
dementia and its diagnosis are provided.
the second section covers important implications of dental care provision for people
who are living with dementia. it is important to remember that care plans may need
to be adapted to be appropriate to meet the needs of a patient living with dementia,

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)xii
and so may look very different when compared to the general population. this
section, therefore, provides background knowledge on dementia and management,
and the implications for dental practice.
the third section details standards in five areas, which have been identified as
specific to dementia care, to help dental care providers ensure the qualities of
care. it also provides supporting material for dental professionals and references.
three main themes are presented.
• Management: the identification of patients; issues surrounding competence
and referrals; communication with patients and/or their carers; communication
between other health personnel; and the issues of consent and capacity.
• Clinical care: history taking; treatment planning; care delivery;
and prescribing.
• Site considerations: the practice and/or surgery; care homes;
and domiciliary care.
Finally, the fourth section contains material on where to find educational
programmes, local support networks including information sharing with health
professionals and samples of patient information sheets.

1Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
1.1 IntroductIon
understanding the reality of the condition and the complex ways dementia affects
each individual is a key element to improving standards of care for people living with
dementia. As a profession that advises regular attendance for care, dental professionals
are well-placed to play a major role in monitoring and helping ensure that high
standards of care management exist.
one in three people over 65 will die with dementia, but despite its prevalence, the
condition remains under-diagnosed; fewer than half of people with dementia in
England receive a formal diagnosis.1 Improvements in rates of diagnosis have been
observed, although considerable variation exists across the uK.2 Such disparities
mean that many people are unaware of steps they can take to manage their
condition, including planning for the future and how to access support and care.
Several factors have led to this low diagnosis rate, including historical lack of
diagnosis of dementia, lack of understanding by the public and healthcare
professionals, and an attitude among some healthcare professionals that there
is little benefit to diagnosing dementia.
Alongside low diagnosis rates, there exists little public understanding of the nature,
prevalence and symptoms of dementia, which in turn leads to misconceptions that
perpetuate the stigma associated with the condition.3 People with dementia are
often isolated, or withdraw, because of stigma and fear of negative reactions from
neighbours, their families and the wider community to their behavioural and
psychological symptoms. Stigma may prevent people acknowledging the symptoms
of dementia and obtaining the help they need to live the life they want to lead.
People with dementia and their carers should be treated with dignity and receive
P r I n c I P L E S B E H I n d c A r E M A n A G E M E n t1

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)2
care and support that is based on individual need, rather than assumptions about
the condition.4
dementia is perceived differently in different cultures, faiths and communities. this
includes dementia being considered as a normal part of ageing, as a mental illness,
or being linked to supernatural or spiritual beliefs. People from black, Asian and
minority ethnic (BAME) backgrounds face significant barriers when accessing support.5
A lack of culturally-sensitive dementia services may impact families when available
support does not meet cultural or religious needs. Such shortcomings need to be
considered when supporting patients and their families.
Good oral health is important for health and wellbeing. As dementia is a progressive
condition, it is important to establish (if one is not in place already) a dental care
programme at – or soon after – diagnosis, to help establish the principle of continuity
of care. Maintaining oral health brings benefits in terms of self-esteem, dignity, social
integration and nutrition. Poor oral health can lead to pain, which the individual may
have difficulty articulating, and tooth loss. It can negatively affect self-esteem and the
ability to eat, laugh and smile. Both pain and infection can worsen the confusion
associated with dementia.
1.2 Diagnosis of Dementia
1.2.1 the importance of a diagnosis
A diagnosis enables access to treatments and support, acting as a catalyst for
discussions about how to live with dementia, including power of attorney (for finance
and health and wellbeing), maintaining health, mobility and advanced care planning
while the person can still actively participate. there are numerous barriers to a
diagnosis of dementia, which are steadily being broken down, but two that remain
persistent include the stigma attached to dementia, and the misplaced perception
that it is a natural and inevitable part of ageing. In addition, as no cure for dementia
currently exists and only a few treatments with limited effectiveness for Alzheimer’s

3Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
disease (the most common form of dementia) are available, some clinicians are led
to question the value of a diagnosis. Such opinions ignore the importance of support
and information in helping people to feel more in control.
1.2.2 the progressive development of dementia
the term dementia covers a range of neurological conditions, all of which are progressive.
the most common types of dementia are: Alzheimer’s disease, vascular dementia,
dementia with Lewy bodies, and fronto-temporal dementia.6 All types impact on a person’s
ability to remember, understand, communicate and reason, and the abilities of an
individual with dementia will gradually decline. How quickly the condition progresses
will depend on the individual; each person is unique and experiences dementia in their
own way, and indeed may demonstrate more than one type of dementia.
Common forms of dementia and their incidence
Alzheimer’s disease 62%
Vascular dementia 17%
Mixed dementia 10%
dementia with Lewy bodies 4%
Fronto-temporal dementia 2%
Parkinson’s dementia 2%
other 3%
Viewing dementia as a series of stages can be a useful way to understand the illness,
although such an approach only provides a rough guide to the progress of the condition.
1.2.2.1 Before dementia becomes apparent
there is strong evidence that, by the time most people develop any symptoms of
dementia, the underlying disease has been causing damage to the brain for a
considerable time.7 during this ‘pre-symptomatic’ period, tests that explore the brain
chemistry, function and structure have been developed and may suggest future

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)4
treatment modalities, including medication, which could slow down or prevent
progression before the disease is fully established.
over time, changes in the brain will begin to cause mild symptoms, but do not enable
a diagnosis of dementia to be made with a high level of accuracy. Subtle problems in
areas such as memory, reasoning, planning or judgement may cause difficulties with
more demanding tasks (such as preparing a meal) but do not significantly affect daily
life. A person at this stage may be given a diagnosis of mild cognitive impairment (McI).
About 10-15% of people with this diagnosis will go on to develop dementia each year.
McI may be used as a ‘flag’ to dental teams to think about starting the planning
process for treatment and prevention going forward. Medical history-taking could
include asking patients directly about any memory issues they may have, and
specifically about the McI diagnosis. While dementia is not the only cause of
memory issues, management pathways may be similar.
1.2.2.2 Dementia as a progressive condition
A common feature of all dementia lies in the structure and chemistry of the brain
becoming increasingly damaged over time. the person’s ability to remember, understand,
reason and communicate will gradually decline. As dementia worsens, the person will
need increased support with daily living. their behaviour and mood will also change.
Health professionals often use indices to measure these changes. At different times
they may assess a person’s mental ability (for example with a ‘Mini Mental State
Examination’),8 daily living skills (such as dressing or managing medication),
behaviours, overall functioning, or quality of life. Some of these scales were developed
specifically for Alzheimer’s disease and work better for that than for other types of
dementia. Assessment of the extent of an individual’s dementia should take account
of the data from such scales, but equally take a broader view of the person, including
their capabilities and needs.

5Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
1.2.2.3 Rate of progression
there is evidence that some types of dementia can progress at different rates or
more aggressively, but experts are unsure whether this is conclusive. Every person’s
experience is different and there can be a huge amount of variability in people’s
response to the disease. difficulties with diagnosis may mean that people are
diagnosed later, making their progression seem faster.8
A wide range of factors influence the progression of dementia in an individual.
People who develop symptoms before the age of 65 often have a faster rate of
progression, and evidence suggests that there may be a genetic link. overall
physical health also seems to be a factor. People with a dementia diagnosis
who also have poorly-controlled heart disease or diabetes, those who have had
several strokes, or those who have repeated infections are all likely to show a
faster rate of progression.
on the positive side, evidence shows that keeping active and involved in social
activities can help a person with dementia retain their existing abilities for longer.
regular physical exercise in particular seems to slow the rate of decline.
Some of these factors affect the underlying pathological processes of the
brain, while others simply help address symptoms. those supporting someone
with dementia should encourage the individual to stay active – physically,
mentally and socially. A person with dementia should also try to eat healthily,
get enough sleep, take medications as advised and not smoke or drink too
much alcohol. It is also important for the person to follow appropriate health
interventions such as assessments for teeth/dentures, eyes, ears and feet as
advised, and recommended seasonal vaccination programmes, e.g. influenza
and pneumonia. the advice is equally valid for a carer. Sudden changes in a
person’s abilities or behaviour could indicate a physical or psychological health
problem or an infection.

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)6
1.2.2.4 The staged development of dementia
Although by necessity somewhat artificial, it can be useful to view the course that
dementia follows as having three stages in development; early, middle and late.
Each type of dementia tends to have a particular early set of symptoms, arising from
the differing parts of the brain initially affected. over time, as damage spreads to
more areas of the brain, the symptoms of the different types tend to become similar.
Indeed, by the later stages, the individual will need a high level of care, irrespective
of the type of dementia.
Such a framework helps provide an understanding of the changes that are occurring,
albeit in very general terms. It is important to consider:
• Some symptoms may appear earlier or later than indicated here, in a different
order, or not at all.
• the stages may overlap – the person may need help with one task, but may be
able to manage another activity on their own.
• Some symptoms, such as irritability, may appear at one stage and then vanish,
while others, such as memory loss, will worsen over time.
the way a person experiences dementia will depend on many factors. these include
their physical make-up, other illnesses they may have, their emotional resilience,
the medication they take and the support they can rely on.
1.2.2.4.1 Early (‘mild’) stage
dementia usually begins with very minor changes in the person’s abilities or
behaviour. At the time, such signs can often be mistakenly attributed to stress or
bereavement or, in older people, to the normal process of ageing. It is often only later
on that it becomes apparent these signs were probably the beginnings of dementia.
Loss of memory of recent events is a common early symptom. the person will have
difficulty recalling things that happened recently, in addition to problems with

7Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
learning new information. Someone with dementia may:
• Mislay items around the house.
• Forget recent conversations or events.
• Struggle to find the right word or lose the thread of what is being
said during conversation.
• Become slower at grasping new processes or concepts and unwilling
to try out new things.
• Become confused, disorientated or lose track of the day or date.
• Show poor judgement, or find it harder to plan or make decisions.
• Have problems judging distance or seeing objects in three dimensions
(for example when navigating stairs or parking the car).
• Lose interest in other people or activities.
In the early stages of dementia, retaining usual activities where possible can help
maintain independence. It helps the individual retain their sense of identity and
self-worth if they are given the chance to do things for themselves (with support
if necessary). Focus should be on what the person can do as opposed to what
they cannot, and on exploring how things can be achieved in a different way.
the person may also become anxious, irritable or depressed. they may experience
distress over their failure to manage tasks and may need reassurance. In such cases,
talking and giving them emotional support is important. disclosure by a patient
or relative regarding their dementia status needs to be handled sensitively.
1.2.2.4.2 Middle (‘moderate’) stage
As dementia progresses, the changes become more marked. the person will need
more support to help them manage their day-to-day life. they may need frequent
reminders or help to eat, wash, dress and use the toilet. they are likely to become
increasingly forgetful – particularly with names of objects and people – and may
sometimes repeat the same question or sentence. they may also fail to recognise

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)8
people or confuse them with others. At this stage, the individual could put himself/
herself or others at risk through their forgetfulness, for example by not lighting the
gas on the cooker or forgetting to take medication.
Some people at this stage may become very easily upset, angry or aggressive –
perhaps because they are feeling frustrated at not being understood or because
they misinterpret what is happening. they may lose their confidence and need
a lot more support or reassurance. other symptoms may include:
• Becoming confused about where they are, or wandering and becoming lost.
• Muddling up time and getting up at night because they are confusing
night and day.
• Behaving in ways that may seem unusual, such as going outside in their
nightclothes, becoming very agitated or unknowingly behaving in socially
inappropriate ways.
• Experiencing difficulty with perception and, in some cases, having delusions
(strongly believing things that are not true) or, less often, hallucinations
(usually, seeing things that are not really there).
changes in behaviour tend to be most common from the middle stage of dementia
onwards, and are one of the most challenging aspects of dementia for carers.
1.2.2.4.3 Late (‘severe’) stage
At this stage, the person with dementia will need even more help and will gradually
become totally dependent on others for care. Loss of memory may become very
pronounced, with the person unable to recognise familiar objects, surroundings or
even people closest to them, although there may be sudden flashes of recognition.
the person may also become increasingly weak. they may start to shuffle or
walk unsteadily, eventually spending more time in bed or a wheelchair. other
symptoms may include:

9Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
• difficulty eating and sometimes swallowing (dysphagia).
• difficulty communicating.
• considerable weight loss, loss of muscle bulk (sarcopenia) and muscle
weakness (although some people may overeat and put on weight).
• Incontinence – losing control of their bladder and sometimes bowels.
• Gradual loss of speech, though the person may repeat a few words or
cry out from time to time.
• Fatigue at relatively low levels of activity, associated with sarcopenia, means
that the person is less likely to be able to adhere to oral hygiene frequency.
the individual may become restless, sometimes seeming to be searching for someone
or something. they may become distressed or aggressive, especially if they feel
threatened in some way. Angry outbursts may occur during close personal care,
usually because the person does not understand what is happening. those caring for
the person should try not to take this personally – the person is not being deliberately
aggressive. It is also important to consider that the person may be experiencing pain
that they cannot express verbally. Painkillers can often help in such circumstances, but
clinicians should also investigate the cause and address this appropriately if possible.
during the later stages of dementia, most people will become increasingly frail due to
the progression of the illness. they will also gradually become dependent on others for
all of their care. Knowing what to expect can help everyone to prepare. It can enable the
person with dementia to think about the kind of treatment and care they might want,
and allows them to write an informed advance decision (which could be known either as
a Living Will or an Advance directive) before they reach this stage so they can have input
into their future care. It also allows carers and family to think about these aspects too.
1.3 KeY Points in tHe Diagnosis
1.3.1 signs and symptoms of dementia
the impact of dementia on an individual is unique, with different types of dementia

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)10
affecting people differently, especially in the early stages. How others respond to the
person, and how supportive or enabling the person’s surroundings are, also greatly
affect how well someone can live with dementia.
dementia is progressive, which means the symptoms gradually get worse over time.
How quickly dementia progresses will vary greatly from person to person.
1.3.2 associative medical conditions
there are a number of associative conditions that lead to an increased risk of
dementia that the dental care provider should consider if dementia is undiagnosed.
these are covered below.
1.3.2.1 Cardiovascular factors
there is very strong evidence cardiovascular risk factors that damage the heart,
arteries or blood circulation all significantly affect a person’s chances of developing
dementia.9 the main conditions linked to dementia are:
• type 2 diabetes – in mid – or later life.
• High blood pressure – in mid-life.
• High total blood cholesterol levels – in mid-life.
• obesity – in mid-life.
these conditions are avoidable risk factors for dementia but also for cardiovascular
diseases (stroke and heart disease, such as abnormal heart rhythm). Having cardiovascular
disease or type 2 diabetes can double an individual’s risk of developing dementia.
these cardiovascular conditions are most strongly linked to vascular dementia. this
is because vascular dementia is caused by problems with blood supply to the brain.
research10 suggests that many people with dementia have mixed dementia, or
Alzheimer’s disease with some vascular damage in the brain. the cardiovascular risk
factors and diseases should be considered as risk factors for mixed dementia and not

11Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
just vascular dementia. In some cases (such as in diabetes or high mid-life
cholesterol) they are known risk factors for Alzheimer’s disease as well.
1.3.2.2 Depression
People who have had periods of depression – whether in mid-life or later life – also
seem to have increased rates of dementia.9 Whether depression is a risk factor that in
part causes dementia is not clear, and the answer probably differs with age. there is
some evidence that depression in middle age does lead to a higher dementia risk in
older age. In contrast, depression in later life (when a person is in their 60s or older)
may be an early symptom of dementia rather than a risk factor for it.
1.3.2.3 Other conditions
other medical conditions that can increase a person’s chances of developing dementia
include Parkinson’s disease and HIV. down’s syndrome and other learning disabilities
also increase a person’s risk of dementia. Patients who suffer from multiple sclerosis
can experience cognitive impairment or cognitive dysfunction similar to dementias.
A number of further conditions have been linked to dementia in some studies, but
evidence is currently weak. these conditions include chronic kidney disease, hearing loss,
anxiety and sleep apnoea. there is also growing evidence that loneliness and social
isolation may increase someone’s risk of dementia. In many of these cases, more research
is needed to show the strength and ‘direction’ of this link (i.e. what causes what).9
1.3.2.4 Lifestyle factors
there is overwhelming evidence that lifestyle factors influence the risk of developing
dementia, but public awareness of this is low.11 Studies of large groups show that
dementia risk is lowest in people who have several healthy behaviours in mid-life.
these behaviours include regular physical exercise, not smoking, drinking alcohol only
in moderation (if at all), and maintaining a healthy diet and weight. the dementia risk
is lowest in people who adopt three or more of these behaviours, not just one or two.

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)12
1.4 sUmmaRY
the term dementia refers to a number of conditions with similar clinical
manifestations. the epidemiology of dementia suggests that about 5% of the
population live with dementia, and that this figure will grow as the age profile
of the population changes with increases in life expectancy.
dementia impacts on a person’s ability to remember, understand, communicate
and reason, and an individual’s ability will gradually decline. How quickly the
condition progresses will depend on the individual. A wide range of factors
influence the progression rate of dementia – including age – with those
developing symptoms before the age of 65 experiencing a more rapid decline.
Evidence also exists of a genetic link. overall physical health is another factor;
people with poorly-controlled heart conditions or diabetes, those who have had
several strokes or those who have repeated infections are all likely to show faster
deterioration. the dental team may be the first healthcare professionals (HcPs)
to notice a change in a person’s abilities and behaviours.
Good oral health is important for health and wellbeing. As dementia is a
progressive condition, it is important to establish or reinforce a dental care
programme as soon as possible upon diagnosis to assist with continuity of care.
Maintaining oral health brings benefits in terms of self-esteem, dignity, social
integration and nutrition.
A useful guide for the dental team to help understand the issues surrounding
the dementias and their impact is available on the Guy’s and St thomas’ nHS
Foundation trust website entitled ‘Barbara’s story.’12

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK) 13
1.5 RefeRenCes anD ResoURCes1. mcnamara g, millwood J, Rooney Ym & Bennett K. forget me not – the role of the general dental
practitioner in dementia awareness. BDJ 2014;217:245–248.
2. nHs Digital Recorded dementia diagnoses. april 2017. available at: www.content.digital.nhs.uk/
catalogue/PUB24036.
3. Cahill s, Pierce m, Werner P, Darley a, Bobersky a. a systematic review of the public’s
knowledge and understanding of alzheimer’s disease and dementia. alzheimer Dis assoc Disord
2015;29(3):255-75.
4. alzheimer’s society. Right to Know campaign – diagnosis and support. available at: www.
alzheimers.org.uk/info/20016/campaigns/204/right_to_know_campaign_-_diagnosis_and_support.
5. moriarty J, sharif n, Robinson J. sCie Research briefing 35: Black and minority ethnic People with
Dementia and their access to support and services. sCie; 2011. available at: www.scie.org.uk/
publications/briefings/briefing35.
6. alzheimer’s society. exercise and Physical activity. available at: www.alzheimers.org.uk/info/20029/
daily_living/15/exercise_and_physical_activity/2.
7. Reiman em, et al. Brain imaging and fluid biomarker analysis in young adults at genetic risk for
autosomal dominant alzheimer’s disease in the presenilin 1 e280a kindred: a case-control study.
the Lancet neurology 2012;11(12):1048-1056.
8. alzheimer’s society. the mmse test: mini mental state examination. available at: www.alzheimers.
org.uk/info/20071/diagnosis/97/the_mmse_test.
9. alzheimer’s society. Risk factors for dementia: factsheet 450. 2016. available at: www.alzheimers.
org.uk/download/downloads/id/1770/factsheet_risk_factors_for_dementia.pdf.
10. Bennett D. Public health importance of vascular dementia and alzheimer’s disease with
cerebrovascular disease. international Journal of Clinical Practice supp 2001(120):41–48.
11. Public Health england. Public unaware of the factors that increase the risk of dementia. 2016.
available at: www.gov.uk/government/news/public-unaware-of-the-factors-that-increase-the-risk-
of-dementia.
12. guy’s and st thomas’ nHs foundation trust. Barbara’s story. available at: www.guysandstthomas.
nhs.uk/education-and-training/staff-training/Barbaras-story.aspx.
Resources and further reading
alzheimer’s society. Dementia 2013: the hidden voice of loneliness. available at: www.alzheimers.
org.uk/download/downloads/id/1677/dementia_2013_the_hidden_voice_of_loneliness.pdf.
alzheimer’s society. Building dementia-friendly communities – a priority for everyone. 2014.
available at: www.alzheimers.org.uk/download/downloads/id/1918/building_dementia_friendly_
communities_a_priority_for_eveyone_-_executive_summary.pdf.

Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)14
Chen J-H, Kun-Pei L, Chen Y-C. Risk factors for Dementia. J formosan medical association
2009;108:10:754-764.
Clarke n, Clarke f, edwards D. (eds). Diagnosing Dementia in general Practice, in How to manage
Dementia in general Practice. oxford: John Wiley & sons; 2013.
Dementia. a niCe–sCie guideline on supporting people with dementia and their carers in
health and social care. national Clinical Practice guideline number 42 national Collaborating
Centre for mental Health. available at: www.scie.org.uk/publications/misc/dementia/dementia-
fullguideline.pdf.
social Care institute for excellence. Dementia. available at: www.scie.org.uk/dementia.
sosa-ortiz Ls, acosta-Castillo i, Prince mJ. epidemiology of Dementias and alzheimer’s Disease.
archives of medical Research 2012;43(8):600–608.
Walls a. Developing pathways for oral care in elders: challenges in care for the dentate the
subject? gerodontology 2014;31(suppl 1):25–30.

15Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
2.1 General considerations
Management of an individual’s oral health is dependent not only on what happens in
a dental surgery but how that individual self-manages their mouth. There are a number
of general considerations to take into account when treating people with dementia.
First, the recognition that the impact of dementia on an individual will vary; some
people have ‘good’ and ‘bad’ days. Where possible, dental appointments may be better
postponed to a ‘good’ day, and scheduled to fit in with the individual’s ‘best’ time of day.
Some people with dementia may have reduced attention spans, meaning that their
ability to co-operate may be decreased. Dental appointments should be kept within the
individual’s capacity to cope and their preferred timings. As with all patients, the use
of appointment reminders can help ensure that people remember to attend for their
appointment. While common practice, flexibility in the arrangements for sending the
reminder – for example the use of text messages, emails or printed diary stickers –
should be considered. Patients may appreciate a telephone call the day before their
appointment. This will reduce anxiety for the person living with dementia and help
ensure that appointments are not missed.
If attending with a family member who is also due for a check-up, it may help to conduct
their check-up first so the patient can acclimatise and watch so they are more prepared
for what will happen in their own examination.
Carers (either formal, or informal such as family members) play a vital role in supporting
people living with dementia to access health and social care.1 Their close relationship
and proximity to the patient means carers are well-placed to help a person to give a pain
history, describe symptoms, and attend the dentist.2 In later stages of the disease, carers
P R I N C I P L E S O F C A R E P R O V I S I O N2

16 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
will usually play a key role in initiating help and seeking treatment2 and in supporting
individuals to have choice and control over decisions affecting them.1 It is hugely
important that the dental team develop close working relationships with carers in order
to facilitate access to dental care, such as identifying the most suitable times to attend.
In later stages of the disease this will include supporting decisions and choices about
the dental treatment.
Access to a surgery where the examination will take place should, if possible, be step-
free. The requirement to climb stairs in general has been identified as a barrier to
various activities in the elderly and can be exacerbated for those living with dementia.3
The overall approach to managing the care of individuals who have been diagnosed
with dementia should be consistent, where possible, with those outlined in Clinical
Examination & Record Keeping – Good Practice Guidelines.4 The dentist should be aware,
however, that some variation may be necessary in the format and depth of enquiry
to ensure that treatment can be provided in a safe and appropriate manner.
The clinician must consider not only the patient’s current dementia status when
formulating treatment plans, but its likely rate of development. This covered in more
detail in section 2.5.
As with all history-taking, it is essential to update and record at each patient visit, as the
nature of the condition means that progression is continuous, protracted and often erratic.5 B
2.1.1 Pre-examination
The incorporation of this element in the care process ensures that adequate information
is collected and can assist in establishing whether the patient is attending with a
particular problem. If there is a carer involved in supporting the patient, their help
with gathering this vital pre-examination information can be invaluable.

17Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
The information in this ‘pre-exam’ comprises:
• Personal information.
• Medical history.
• Socio-behavioural history.
This can be collected prior to attendance at the practice using a pro-forma.
2.1.1.1 Personal information
• For existing patients, a change in details or manner of the patient’s responses and
behaviour may alert the dental team to a change in a person’s cognitive abilities. The
dental team might be the first healthcare professionals to notice symptoms indicating
early onset of disease. This may lead to a sensitive discussion as to whether the
patient should contact their own GP in relation to (either the patient’s or dentist’s)
concern over a noticeable change in memory. It is important that advice to seek
further medical assessment is given in a neutral way, avoiding alarming or worrying
the patient unnecessarily. The process should be the same as if there were concerns
about a patient’s physical health, such as a persistent cough (see also section 3.2).
• Should the dentist and patient agree to contact the GP, the dentist should be aware
of General Dental Council (GDC) standards of disclosing information and seek the
patient’s consent (see 3.2 for further information). C
• As dementia advances, updating history may become more difficult and time-
consuming, even if the carer is present. A preliminary phonecall requesting this
information before the dental visit may be helpful. Many people living with
dementia may have a ‘patient passport’ which can provide helpful details about
medical history, medications and how the person likes to be treated, including
conditions which enable treatment (e.g. familiar music and interests).
2.1.1.2 Medical history
Understanding a patient’s medical history and being aware of the patient’s medical
condition while providing care is essential, as it may influence the type and extent
of treatment provided.6 B

18 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
• Patients may not always disclose that they have dementia, but dentists should
be aware of the common drugs used to help patients with the condition.
This will aid the dental team in patient management (see section 3.4.1). B
• The frequency of administration (e.g. daily, twice daily, morning, evening)
and whether tablet – or syrup-based should be particularly noted. B
• Nutritional supplements may be also prescribed and these too should be
noted. A
• For all patients, drug regimes should be recorded. For computerised systems,
an updated entry may suffice. B
• The medical history should be signed and dated for the current course of
treatment by the patient, carer or relative as appropriate, and the clinician. A
• There may be issues with swallowing and dysphagia, particularly if there has
been a history of stroke or Parkinson’s disease. It is important to identify if there
is speech and language support for the patient, and whether patients have been
prescribed thickened fluids, and/or given advice regarding their posture during
eating and drinking. A
2.1.1.3 Socio-behavioural history
In addition to information gathered as part of the medical history, there is additional
material that may be of value that should be discussed for patients living with dementia.
• There may be a preferred time of day for the patient to attend and this should
be borne in mind when arranging appointments. A
• Their preferred type of communication for both appointment reminders and
overviewing agreed treatments. A
• There may be carer involvement and the extent of this should be noted. Their
role is of vital importance to supporting people living with dementia to attend
the dentist. A
• Who that carer is and what their relationship is to the patient should be noted
in the records. A

19Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
• How the patient should be contacted; either directly or via a carer. This is of
importance to avoid ethical or confidentiality issues. A
• In some circumstances, where mental capacity has been lost, a lasting power
of attorney may be in place for health and care issues, as well as financial matters.
If one is not in place, there may be a carer or family member who supports the
person living with dementia to make decisions and choices about care and support,
including dental care and their details recorded. C
2.1.1.4 Dental history
Condition-specific information should be discussed and recorded, including:
• The ability to chew foods comfortably. A
• Swallowing difficulties. A
• Previous difficulties with treatment. A
• Oral hygiene regimen – particularly whether assistance is required. B
• Dry mouth. B
• Dentures previously provided but not worn. A
In certain circumstances, particularly where communication is poor, there may be
difficulty in discerning the cause of a problem. General malaise may prove to be of
dental origin, particularly dental pain. Asking patients and carers to complete a pain
diary for a planned appointment can be very useful. One example of recording pain
for individuals living with dementia is the Abbey Pain Scale, which is an instrument
designed to assist in the assessment of pain in patients who are unable to clearly
articulate their needs (see Appendix A2).7
2.1.1.5 Communication
It is important that all healthcare professionals (HCPs) develop specific communication
skills for working with people living with dementia. All members of the dental team
should maintain key standards of good communication, but where necessary adjust
communication strategies to meet the needs of those living with dementia. A

20 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
First, at every clinical encounter the clinician/nurse/receptions should introduce
themselves by name and state their role, for example, “Good morning Mrs Black, my
name is Mary Brown, I am a dentist.” Always address the patient by their preferred name
(check beforehand what that might be) and if unsure, it is wise to start more formally.
Approach the patient from the front (avoid coming in from behind as it can be frightening
and startling) and get to a comfortable level where it is possible to maintain eye contact.
Standing over people can feel intimidating; likewise, crouching in front of people can
seem patronising. It is important to retain a high level of understanding and keep the
conversation simple. Give time for your patient to process information using familiar
words and terms. Refer to people and things by their name (for example, “…your
daughter Jan,” or “your doctor, Dr Shah”). Ask one question at a time, giving the patient
time to process and respond, and repeat the answer back to the patient to check that
they have been understood. Give the person your full attention while they are speaking.
Keep information requests simple; where possible ask for one decision at a time, for
example “Do your prefer to attend in the morning or afternoon?” It is important to give
people choice but not to overwhelm. The same approach applies to taking the medical
history; ask about one aspect at a time. Try not to interrupt, and when there is a gap
in conversation or digression, steer the patient back to the point of interest.
Sometimes the clinician may ask a question that generates a response unrelated to the
question. Try and rephrase the question. Rather than correcting the patient overtly, gently
distract them and draw them back to the area of interest. Avoid using too many direct
questions; rather than “Do you know who I am?” or “Do you know where you are?” try
“Good morning Mrs Smith, I am Joan Evans the dental hygienist and we are in my dental
surgery.” Physical touch, such as a pat on the shoulder or hand, can be reassuring; but it is
important to be aware of any socio-cultural issues around touching a non-family member.
Ensure that conditions are optimal for effective communication. Make sure the patient (if
21Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
required) has his/her reading glasses, hearing aid (switched on with batteries working) and
if possible have effective pain control. Avoid background noises such as a beeping from
equipment, staff entering and leaving the surgery, moving instruments, or playing a radio/
music system too loudly. For some people, music can be relaxing and comforting, so it
may be a good idea to check with the patient for a favourite performer or piece of music.
In the later stages, when dementia is more advanced, the person’s verbal skills can
deteriorate and therefore they can become more sensitive to body language. Assume a
calm reassuring presence, do not make sudden movements, and ensure body language
reflects what is being said. Ensure that facial expressions and tone of voice correspond;
nod and show active listening. Even if the clinical encounter is frustrating for the dental
team, a calm and reassuring voice can reduce anxiety, even if the conversation is not
understood by the patient. In middle and later stages, family members and carers can
often advise on what might work best; how people react to different stimuli and how
communication should be approached. It is useful to ask family and carers about
collateral information – what is ‘typical’ for this patient, any particular habits or fidgets,
conversational habits or reactions to pain and discomfort. Family members/carers can
be very useful in helping the dental team manage an individual’s behaviour, identify
what coping mechanisms and reassurances work, and advise on what triggers to avoid.
Challenging behaviour is often as a consequence of a need not being met; the person
is thirsty, hungry, or needs to use the toilet. Such needs being unmet can manifest in
behaviour such as agitation, wandering and preservation (repeating the same word).
Try not to keep the patient waiting, and ensure he/she has eaten and drunk recently, and
used the toilet. Avoid triggers by using distraction; for example, instead of saying to the
patient “Don’t leave the waiting room” or “Don’t fiddle with the chair,” perhaps try “Let’s
look at these pictures”, or “Let’s go in to meet the dentist.” A visual prompt for facilitating
successful communication in the practice environment is provided in Appendix A3.
A useful mnemonic to assist in managing communication with patients living with

22 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
dementia is VERA.8 This is particularly helpful when it is unclear what the person is
trying to express, or when the patient says something that is known to be untrue.
V: Validation. This acknowledges that the person is trying to express and communicate,
even if it is unclear (including relevance) about what is being communicated. A 90-year-
old man might say he wants to see his mother. Accept the communication. (“You want
to see your Mum, Jim?”) Do not dismiss the behaviour as simply a symptom of dementia.
E: Emotional context. Understand that there is an emotional context to the behaviour.
Pay attention to the emotion, even if the verbal communication is not clear (e.g. “You
sound worried, Jim.”) Do not dismiss the emotion as a symptom of dementia.
R: Reassurance. This can involve any verbal or non-verbal communication. A calm
voice and demeanour can reassure and alleviate anxiety. This might be supplemented
with a reassuring pat on the hand or arm, but be aware of socio-cultural issues around
physical touch. (“Its OK Jim, you are safe here,” perhaps followed by a reassuring pat
on the hand).
A: Activity. Institute an activity by assessing what the unmet need might be and find
a way of addressing it (e.g. offer a drink or a trip to the toilet).
SUMMARY OF RECOMMENDATIONS
KEY: A – ASpIRATIONAl B – BASIC C – CONDITIONAl
Medical history
Understand patient’s medical history B
Update and record history at each patient visit B
Seek patient consent to inform GP of potential symptoms C
Be aware of common drugs used to help dementia patients B
Note frequency of medicine administration B

23Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
Record use of nutritional supplements, if appropriate A
Record changes to drug regimens B
History of medication changes noted for new patients B
Medical history signed and dated by patient/carer/relative and clinician
for each course of treatment A
Identify support and interventions received in relation to dysphagia A
socio-behavioural history
Establish and accommodate preferred
time of day for appointments A
Establish and accommodate preferred method of communication
for appointment and treatment information A
Note presence and/or extent of carer involvement A
Note details of carer and their relationship to the patient A
Establish whether the patient should be contacted directly
or via a carer, keeping patient confidentiality in mind A
Where mental capacity has been lost, establish whether there is power of
attorney in place, or a person whose role it is to make decisions for the patient C
dental history
Record the ability to chew foods comfortably A
Record swallowing difficulties A
Record previous difficulties with treatment A
Note the patient’s oral hygiene regimen and whether assistance is required B
Record whether the patient has dry mouth B
Record where dentures were previously provided but not worn A
coMMunication
Adjust communication methods to meet the needs of patients with dementia A

24 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
2.1.2 early stages of dementia
In the early stages, it is important to undertake an oral health risk assessment and base
any preventive strategies on mitigating future risk; for example review the oral hygiene,
assess risk of adverse effects from medications, the impact of a dry mouth and
effectiveness of the care plan.9 Someone in the early stages of dementia should be
encouraged to carry out their own mouth care for as long as possible, but they may
need to be reminded or supervised. This might involve a carer prompting oral hygiene
by providing a brush and toothpaste and reminding or showing them what to do.
The person with dementia may find it easier to use an electric toothbrush or a
toothbrush with an adapted handle to improve their grip (see Appendix A4).
The dentist or dental hygienist should advise both the person and their carer on the best
methods for preventing tooth decay and gum disease in their particular circumstances
and signposting them to the relevant National Institute for Health and Care Excellence
(NICE) guidance.10,11 It is very important to establish a daily care routine in the early
stages of dementia. These daily care routines need to be reviewed on a regular basis to
ensure they are effective. Good mouth care is essential, but achieving this can be highly
problematic. There is a need to be pragmatic, and as Walls12 suggests, to accept that
there may be two approaches to establishing an oral hygiene regime: social cleanliness
and disease prevention. In the case of disease prevention, effective and thorough
cleaning is required every 48 hours. An oral hygiene strategy might therefore include a
targeted approach, where the teeth are cleaned twice daily for social cleanliness, but at
each session only one quadrant is cleaned to ensure maximal plaque removal. This way,
over a 48-hour period, all four quadrants are fully cleaned, but the patient’s attention
is maximised and their functional reserve is conserved.
Oral hygiene may include a high-concentration fluoride toothpaste (5000ppm) and
regular application of fluoride varnish for people with natural teeth. This routine may
need to be adapted based on the individual challenges the person with dementia has,
such as forgetting to brush teeth daily. This could be addressed by advising a visible

25Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
reminder to prompt the individual (such as on a bathroom mirror) or brushing the
teeth at the same time as another family member.
As the condition progresses, families and carers may need signposting to resources
offering advice and support for the more dependent patient. For example ‘Looking after
the mouth – A training guide for carers’ has been produced by the British Society of
Gerodontology (BSG) and British Society for Disability and Oral Health (BSDH), and gives
excellent guidance on how to support oral hygiene for a dependent adult. There is
detailed guidance available on how to support mouth care, with excellent video guidance,
from BSG/BSDH,13 and for further information.14,15 Research among carers suggests that
they are very keen to receive training around oral hygiene and behaviour management.2
2.1.3 later stages of dementia
As dementia progresses, the person may lose the ability to clean their teeth, stop
understanding that their teeth need to be kept clean, or lose interest in doing so.
Carers may need to take over this task. The dental professionals responsible can provide
guidance and support on how to assist in cleaning another person’s teeth. The technique
will vary depending on the individual concerned. Again, a targeted approach is
warranted, aiming for social cleanliness and effective full quadrant cleaning in every
48 hours. Generally, the easiest way is for the person with dementia to sit on a straight-
backed chair with the carer standing behind. The carer supports the person against their
body, cradling their head with one arm (see Appendix A5). They can then brush the
person’s teeth using a dry toothbrush and a pea-sized amount of toothpaste. Detailed
helpful guidance and a video demonstration is available on the web link listed as the
BSG/BSDH resource.13
2.2 ManaGeMent of deMentia Patients
Patients who are in the early stages of dementia are best cared for through a stable
and on-going relationship; the central principle being one of continuity of care, with
flexibility. Seeing the same clinician, where possible, provides a degree of stability and

26 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
allows the opportunity for parties to build up trust, and the clinician to note changes
in the overall status of the patient. There is a growing literature to support the need
for continuity of care to improve outcomes. Adair et al16 highlighted the positive
relationships between continuity of care and health outcomes, and Marrsingh et al17
found that poor continuity of care in general practice was associated with a higher risk
of mortality. A number of other reviews of continuity of care, including those by Hsiao
et al18 and Saultz et al19 all highlight its importance. Where a person with dementia
already has a dentist they know and trust, this relationship should continue if possible.
2.3 Practice surGery desiGn
In general, the issues surrounding surgery design for patients with dementia are very similar
to those for all patients. Research on long-term residential homes and GP surgeries provides
some insight for practice design. The use of unobtrusive safety measures; variation in
ambience, the size and shape of spaces; maximising visual access, and controlling levels of
stimulation are all helpful. There is less agreement on the usefulness of signage, provision
for engagement in ordinary activities, or the impact of small surgery size.20
Experiences of surroundings are interpreted at a sensory level, and as an individual’s
cognitive functions deteriorate, the ability to integrate sensory experiences and
understand context declines. Thus, people with dementia are very sensitive to sensory
experiences and their environment needs to be managed carefully to make it
understandable, comfortable, and (if possible) therapeutic. Light can be used to stabilise
the circadian rhythm, which may be disturbed in dementia. Music therapy, aromatherapy,
massage and multisensory stimulation are recommended by NICE for the management of
behavioural and psychological symptoms of dementia (BPSD), although the mechanisms
behind such interventions are poorly understood and evidence is limited.21
These could be adapted throughout the practice in the following ways, using the
Dementia Friendly Physical Environments Checklist:
• Clear signage at eye level, which has contrast between text and background,
27Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
at decision points and on the doors they refer to.
• Well-lit, wheelchair-accessible entrances and walking routes, utilising natural light
as much as possible, avoiding bright light or deep shadows.
• Plain flooring – avoiding dark mats, highly reflective, slippery floor surfaces or
patterned carpets, and undistinguished changes in floor level.
• Recognisable (not abstract) seating which supports the upper back and has armrests
to allow momentum to exit the chair.
• Easy-to-locate, accessible toilets with contrasting toilet seats and a changing place
(where applicable) or unisex facilities where an opposite-sex carer can change
clothes without embarrassment.
• Relaxing music in the waiting room or practice rooms to calm patients
with dementia.
• Interesting features such as a fish tank, painting or TV to relax and distract patients.
2.4 Provision of care outside dental Practices
2.4.1 care homes
Care homes have a duty to ensure that their residents’ healthcare needs are met.
This includes dental care. Quality standards for care homes include the recommendation
to have an oral health assessment on admission, and for residents to have a named
dental provider. It is likely that the local dental practice may be asked for advice and
input into resident’s daily oral care plans, and to provide ongoing care.
The care home manager is expected be able to supply information about their
arrangements for dental care. It may be helpful to speak to care homes in the local
area and provide contact details, should you feel able or willing to provide such care.
NICE has issued guidance on Oral health in care homes.11
2.4.2 domiciliary care
As dementia progresses, it can become increasingly disruptive for patients to attend
visits outside of their normal environment. In this situation, an individual may require

28 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
domiciliary care in their own home or in their nursing or residential care home. In
Evidence-Based Dentistry, Carson and Edwards22 describe the most common barriers
to delivering oral care to older people in care homes, ranging from a lack of adequate
equipment and facilities, to poor financial reimbursement, lack of training and loss of time
from private practice. Detailed guidance on the provision of domiciliary oral health care
has been provided by British Society for Disability and Oral Health (BSDOH).23 Alternatively,
patients may be directed to the local salaried/community or special care dental service, who
usually lead on triaging the more dependent patients’ access to domiciliary dental care.
For those in later stages of the disease, a referral to a specialist in special care dentistry may
be required, particularly when the inclusion of behavioural adjuncts to help people tolerate
dental care is beneficial. Use of behavioural adjuncts, such as a combination of oral or
intranasal sedation with intravenous sedation or general anaesthesia, may be considered;
but the benefit from treatment has to be weighed up and at least balanced with the risks
and difficulties of providing it, in terms of co-operation, consent and medical status.
The British Society of Gerodontology guidelines24 are useful when considering strategic,
long-term, oral care planning for people with dementia. These include:
• Instigate appropriate preventive measures to minimise dental disease as
soon as possible.
• Undertake dental intervention in the early stages of the condition to manage
outstanding dental treatment needs.
• Ensure dentures are named, cleaned professionally on a regular basis, and
renewed using a duplication technique when replacement is necessary.
• Instigate regular review tailored to the individual’s needs, to maintain the oral
status quo, avoid pain and minimise further interventions.
• Ensure that fear, stress and embarrassment for the carer and the person with
dementia are minimised by adopting an ‘open-door’ approach, namely encouraging
open communication, feedback, and discussion about any matter the individuals
feel are of of importance.

29Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
2.5 treatMent PlanninG
The key issues when considering treatment planning lie in recognising how dementia
may impact on an individual in the future, especially how self-care and management
may alter. As the impacts arising from dementia increase, two main aspects should
be considered: how the changes influence medication for dementia and other
comorbidities, and how care should be managed. For a person with dementia,
degradation of hearing is common. The ability to understand normal conversation
is usually not affected at first, but when combined with the presence of background
noise, comprehension may be decreased. If possible, minimise meaningless background
noise and reverberation.25 Where possible, treatment planning should follow the care
arrangements outlined in other FGDP(UK) guidance documents.26
2.5.1 drugs and dental problems
People with dementia may be taking medication for a number of conditions. They may
also be prescribed antidepressants or – less often – antipsychotics and sedatives. Dry
mouth is a common side effect of these drugs. Saliva acts as a lubricant and also cleans
the mouth and teeth. Lack of saliva can lead to a build-up of plaque and increase the
risk of dental decay, gum disease and infection. Dry mouth can also cause problems with
dentures, including discomfort and looseness. Denture fixatives and artificial saliva can
help some people with denture problems. The dentist will be able to offer advice to
relieve discomfort and problems caused by lack of saliva or dry mouth. Frequent sips of
water throughout the day, especially at mealtimes, will help. Discussion with their doctor
may be useful if alternatives with a reduced xerostomia impact are available.
Some antipsychotic drugs can cause involuntary repetitive tongue and jaw movements,
making it difficult to wear dentures, particularly in the lower jaw. In some cases, these
movements will continue after the drug is stopped. If this occurs, the dentist may be
able to advise on what can help and how best to ensure that the person is comfortable.
If medication is syrup-based (e.g. Lactulose), there is an increased danger of tooth decay.
The doctor may be able to prescribe a sugar-free alternative if asked. The dentist may

30 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
also be able to apply chlorhexidine and fluoride varnishes to help prevent cervical decay.
Reduction of sugar in the diet − particularly sugary snacks − also helps to control decay.
2.5.2 consent and capacity
As with all care, treatment and care should take into account the individual’s needs
and preferences. People with dementia should have the opportunity to make informed
decisions about their care and treatment, in partnership with their healthcare
professionals. The care provider should make an assessment of the individual’s capacity.
The nature of the disease may mean that capacity to consent may vary, as consent is time
and procedure specific – consent is given for that treatment at that time. If patients do
not have the capacity to make decisions, healthcare professionals should follow the
Department of Health’s advice on consent26 and the code of practice that accompanies
the Mental Capacity Act.27
In Wales, healthcare professionals should follow advice on consent from the Welsh
Government.29 Indeed, discussions with the patient should also include if and how they
want their family or carers to be involved in their care. As dementia progresses, it is
important that such discussions take place at intervals appropriate to the changing
circumstances. The skills needed to negotiate and work with families and carers are
complex, and will involve issues relating to information sharing and confidentiality.
As with all patients, the use of written material to support the decision-making process
is good practice. This is important for people living with dementia, and families or carers
should have a written record to refer to after the appointment. A written copy of the
proposed treatment and care plan should be provided and dated.30,31 B
The critical issue is the need to identify and be aware of the contact at a local level,
including within the dental practice where care is being provided. Again, notes on actions
should be kept in the patient’s records. B

31Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
2.6 deMentia and dental conditions
Although the strength of the evidence base for linking dementia and the manifestation
of certain dental conditions is variable, there is some data linking conditions with oral
issues that people living with dementia have exhibited increased problems with. These
include bruxism, chewing and swallowing, and denture wearing.
SUMMARY OF RECOMMENDATIONS
KEY: A – ASpIRATIONAl B – BASIC C – CONDITIONAl
consent and caPacity
Follow Department of Health advice on consent
and code of practice accompanying Mental Capacity Act B
Provide a written and dated copy of the proposed treatment and care plan B
Notes on action kept in patient’s records B
2.6.1 bruxism
The link between increased risk of bruxism, whether diurnal bruxism (throughout the
day) or nocturnal bruxism (during sleep) appears not be a straightforward. However,
it may help to consider the following:
• Anti-psychotic and anti-depressant drugs have been known to cause bruxism in some
dementia patients. However it is important to mention that anti-psychotic medication
has also been used to successfully treat this symptom. It may help to discuss the
person’s current medication with their doctor to see if any changes could be made.
• Sometimes bruxism can be indicator that a person is in pain but unable to
communicate this to those taking care of them. Assessment of the teeth to ensure
no damage is occurring as a result of grinding or to establish if bruxism is arising
through dental pain should be taken into consideration. In some cases, gum shields
have been used to reduce this symptom and to protect the individual’s teeth.

32 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
2.6.2 chewing and swallowing
People with dementia can have increased difficulties with chewing. They may hold food in
their mouth, forget to chew, continuously chew or avoid harder-to-chew foods. Advice on
diet, and in particular on avoiding foods that are more difficult to chew or swallow, is good
practice. A painful mouth or ill-fitting denture can make chewing difficult and uncomfortable.
People with dementia may tire easily, which can also lead to problems chewing and
swallowing. Advising on the consumption of soft, moist food that needs little chewing –
such as soup, soft fruit (such as bananas), soft vegetables or scrambled eggs – is helpful.
Families and carers should be reminded of reduced oral clearance, and the necessity
of regular daily oral hygiene.
Difficulty swallowing (dysphagia) becomes more common as dementia progresses.
Swallowing difficulties can lead to weight loss, malnutrition and dehydration. If someone
is experiencing problems with their swallow they should be referred to a speech and
language therapist (SALT) and to the local special care dentistry service to assess oral
health, should nutritional supplementation be advised.
2.6.3 denture wearing
People with dementia should be encouraged to wear their dentures (and offered help
with putting them in) for as long as possible. Dentures are important for maintaining
dignity and self-esteem. If a person does not wear their denture(s), it may affect their
appearance, diet and ability to speak.
Denture loss is common in people with dementia, especially if they are in an unfamiliar
environment, such as a residential home for respite care. Encouraging the use of portable
carry-cases if dentures are removed to eat during the day reduces the risk of breakage,
and putting them in a secure place at night can be helpful. Replacing lost dentures can
present problems (see ‘Denture marking’). If the person is without their dentures for any
length of time they may forget how to wear them, or they may lose their ability to adapt
33Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
to a new set. The person may also be unable to co-operate with the dentist during
the visits required to make the new dentures. Sometimes interventions by the carer
(for example, hand-holding or distraction through talking) may be all that is needed.
If co-operation is limited, a realistic approach may be to provide an upper denture
only, for the sake of appearance.
It can sometimes be difficult and distressing for relatives and carers when they are told
that it will not be possible to successfully make a set of new or replacement dentures
for the person with dementia. The decision not to provide new or replacement dentures
would only be made after an individual assessment, and if it is in the person’s best
interests. Eventually, many people with dementia reach a stage where they will no
longer tolerate dentures in their mouth, even if they have worn them without problems
in the past.
2.6.4 denture marking
A person with memory problems associated with dementia is at greater risk of losing
their dentures. Marking a person’s name on dentures means that lost dentures can often
be returned. New dentures should be permanently marked during their manufacture, but
existing dentures can be easily marked by the dentist, hygienist or carer. Commercially
available dental marking kits typically contain an abrasive pad, a non-toxic pen or pencil,
and a clear sealant. Consideration should also be given to making copy dentures or
routinely providing a duplicate set.
2.7 suMMary
People with dementia may be taking medication for a number of conditions. They
may also be prescribed antidepressants or, less often, antipsychotics and sedatives.
A dry mouth is a common side effect of such drugs and can lead to a build-up of
plaque and associated increase in the risk of dental decay, gum disease and infection.
34 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
A dry mouth can also cause problems with dentures, including discomfort and
looseness. Denture fixatives and artificial saliva can help, but frequent sips of
water throughout the day, especially at mealtimes, will alleviate symptoms. Some
antipsychotic drugs can cause involuntary repetitive tongue and jaw movements,
making it difficult to wear dentures, particularly in the lower jaw. In some cases,
these movements will continue after the drug is stopped.
Dry mouth is an important risk factor for oral disease, and the need for regular daily
oral hygiene needs to be reinforced with patients, family members and carers.
The medical management of dementia can influence the rate of progression of
oral disease. For individuals taking medication, there is likely to be an increased
risk of oral disease.
Managing an individual’s oral health is dependent on two key factors; the care
provided by professionals and that provided by the individual. While this is no
different to any other patient, for individuals with dementia, the ability to undertake
their activities will become more difficult as the condition progresses. Recall
arrangements, surgery design, and the inclusion of carers to support decision-making
are all factors that can help ensure care provision is of the highest quality.

35Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
2.8 references and resources1. national institute for health and care excellence (nice). dementia independence and well being
Qs30. london; nice: 2013. available at: www.nice.org.uk/guidance/Qs30.
2. newton 2016 MissinG reference
3. innes a, Page sJ, cutler c. barriers to leisure participation for people with dementia and their
carers: an exploratory analysis of carer and people with dementia’s experiences. dementia
2015;15(6):1643-1665.
4. hadden a. clinical examination and record-keeping (3rd edition). london: faculty of General
dental Practice (uK); 2016.
5. fiske J, et al. Guidelines for the development of local standards of oral health care for people
with dementia. Gerodontology 2006;23(suppl. 1):3-32.
6. General dental council (Gdc). standards for the dental team. standard 4.1.1. Gdc; london: 2013.
available at: https://standards.gdc-uk.org/pages/principle4/principle4.aspx.
7. abbey J, Piller n, de bellis a, esterman a, Parker d, Giles l, lowcay b. the abbey pain scale:
a 1-minute numerical indicator for people with end-stage dementia. int J Palliat nurs 2004;
10(1):6-13.
8. blackhall a, hawkes d, hingley d, Wood s. vera framework: communicating with people who
have dementia. nursing standard 2011;26(10):35-39.
9. Pretty a, ellwood eP, lo e, et al. the seattle care Pathway for securing oral health in older patients.
Gerodontology 2014;31(1):77–8710.
10. national institute for health and care excellence (nice). dementia: supporting people with
dementia and their carers in health and social care (cG42). 2016. london: nice; 2016. available at:
www.nice.org.uk/guidance/cg42.
11. national institute for health and care excellence (nice). oral health in care homes. Quality
standard [Qs151]. london; nice: 2017. available at: www.nice.org.uk/guidance/qs151.
12. Walls a. developing pathways for oral care in elders: challenges in care for the dentate the subject?
Gerodontology 2014;31(suppl. 1):25–30
13. british society of Gerodontology (bsG) and british society for disability and oral health (bsdh).
looking after the mouth. 2014. available at: www.1000livesplus.wales.nhs.uk/looking-after-the-
mouth.
14. royal college of nursing (rcn), department of health (dh). Promoting older people’s oral health.
2011. available at http://journals.rcni.com/userimages/contenteditor/1373368451935/Promoting-
older-peoples-oral-health.pdf.
15. edwards M, et al. nhs health scotland. caring for smiles: Guide for care homes. better oral care
for dependent older people. nhs health scotland. 2013. available at: www.nes.scot.nhs.uk/
media/2603965/caring_for_smiles_guide_for_care_homes.pdf.
16. adair ce, Mcdougall GM, Mitton cr, et al. continuity of care and health outcomes among Persons
With severe Mental illness. Psychiatric services 2005;56:1061–1069.
17. Maarsingh or, henry y, van de ven PM, deeg dJh. continuity of care in primary care and
association with survival in older people: a 17-year prospective cohort study. br J Gen Pract
2016;66(649): e531-e539.

36 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
18. hsiao cJ, boult c. effects of quality on outcomes in primary care: a review of the literature.
am J Med Qual 2008;23:302-10.
19. saultz JW, lochner J. interpersonal continuity of care and care outcomes: a critical review.
ann fam Med 2005;3:159-66.
20. fleming r, Purandare n. long-term care for people with dementia: environmental design
guidelines. international Psychogeriatrics 2010;22(7):1084–1096.
21. behrman s, chouliaras l, ebmeier KP. considering the senses in the diagnosis and management
of dementia. Maturitas 2014;77(4):305-310.
22. carson sJ, edwards M. barriers to providing dental care for older people. evidence-based dentistry
2014;15:14-15.
23. british society for disability and oral health (bsdoh). Guidelines for the delivery of a domicillary
oral healthcare service. august 2009. available at: www.wales.nhs.uk/documents/bsdh_
domiciliary_Guidelines_august_2009.pdf
24. british society of Gerodontology. oral health resources. available at: www.gerodontology.com/
resources/oral-health.
25. hayne MJ, fleming r. acoustic design guidelines for dementia care facilities. Proceedings of 43rd
international congress on noise control engineering: internoise 2014;1-10. australia: australian
acoustical society.
26. faculty of General dental Practice (fGdP)(uK). Guidance and standards. available at: www.fgdp.org.
uk/guidance-standards.
27. department of health (dh). reference guide to consent for examination or treatment (second
edition). london: dh; 2009. available at: www.gov.uk/government/publications/reference-guide-to-
consent-for-examination-or-treatment-second-edition.
28. office of the Public Guardian. Mental capacity act: making decisions. 2014. available at:
www.gov.uk/government/collections/mental-capacity-act-making-decisions.
29. nhs Wales. Governance e-manual: Patient consent. available at: www.wales.nhs.uk/governance-
emanual/patient-consent.
30. royal college of surgeons (rcs). consent: supported decision-Making. a Guide to Good Practice
available at: www.rcseng.ac.uk/library-and-publications/college-publications/docs/consent-good-
practice-guide.
31. General dental council (Gdc). standards for the dental team. Principle 3. Gdc; london: 2013.
available at: http://standards.gdc-uk.org/pages/principle3/principle3.aspx.

37Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
Resources and further reading
alzheimer’s society. daily living aids. available at: https://shop.alzheimers.org.uk/daily-living-aids.
birtles a. the patient with dementia: communication tips. available at https://geekymedics.com/
patient-dementia-communication-tip.
dementia action alliance. dementia friendly Physical environments checklist. available at:
www.dementiaaction.org.uk/assets/0000/4334/dementia_friendly_environments_checklist.pdf.
leigh e. how to communicate with patients with dementia. available at www.kevinmd.com/
blog/2014/10/communicate-patients-dementia.html.
hazel M, edwards P, brooker d. enriched care planning for people with dementia: a Good Practice
Guide to delivering Person-centred care. london: Jessica Kingsley publishers; 2009.
nhs choices. dementia guide: communicating with someone with dementia. 2017. available at:
www.nhs.uk/conditions/dementia-guide/Pages/dementia-and-communication.aspx.
national institute for health and care excellence (nice). dementia: supporting people with
dementia and their carers in health and social care (cG42). 2016. london: nice; 2016. available
at: www.nice.org.uk/guidance/cg42.

38 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)

39Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
I M P L I C A T I O N S F O R D E N T A L P R O F E S S I O N A L S3
3.1 General implications
Many dentists have a personal relationship with their patients; they may treat
the whole family and are able to build up a comprehensive picture of their
patients as individuals. As such, they may be more likely to notice changes
in behaviour over time, or instances where the patient doesn’t quite seem
themselves. As highlighted in the previous section, the stage at which an
individual presents is important. Indeed, in the early stages of disease it may
be rather difficult to identify whether an individual has any problems. However,
the first step lies in approaching the subject, and any concerns that a dental
professional may have as to whether the individual has (or considered whether
they might have) dementia.
As with all patients there are some general considerations to take into account
when discussing care. People with dementia want information that is clear, easy
to understand and presented in a positive way. The importance of written material
cannot be overstated. Remove unnecessary words and keep to one subject in each
sentence. Avoid jargon, and explain all terms and concepts clearly or through a
glossary. Keep language simple, but aimed at an adult audience.
Colour can be used to distinguish between different sections of information. Set
out text in one column. Use bullet points, bold text, titles and headings to separate
information in manageable chunks or boxes. Bigger type, clear font without serifs
with a font size of at least 12-14pt. Present information logically, one piece at a
time. Diagrams and pictures alongside text are helpful. These should be relevant
and not used simply for decoration. Include contact information, so that if further
clarification is needed, it is clear how to get in contact.

40 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
The ability to comply with oral hygiene procedures and dental care is often influenced
by past dental behaviour and experiences. Some people with dementia who have
had regular dental treatment throughout their lives seem to remember what they
are expected to do in the dental surgery. They have little difficulty co-operating with
simple procedures until the late stage of the disease. Familiar surroundings, routines
and people may be reassuring and aid co-operation.
In certain circumstances a home visit may be helpful. This can be less stressful and
confusing for the person, and may increase co-operation. As mentioned previously,
have a carer present and remain in the person’s sight while they are having treatment
and, where appropriate, offer reassurance by holding the person’s hand. However,
in general it is recommended that wherever possible a patient is seen in a practice
setting where the clinician has access to the full range of facilities and equipment
necessary to provide high quality care.
3.2 How to raise concerns and approacH tHe subject of dementia
The individual personality of a dentist and their relationship with the patient dictates
the communication style used in approaching this subject. For many it may be a
sensitive and tactful approach, with gentle probing and leading questions to investigate
difficulty with memory or changes in behaviour, either with the patient, carer or family
member. This can be termed ‘softer questioning’ and examples include:
• “What did you have for breakfast this morning?”.
• “Did you have a good journey? How did you travel here today?”
For others it may be a direct, clinical approach with a frank, objective question such as:
• “Have you had any change in your health recently?”
• “Have you noticed any change in your memory?”
• “Do you struggle to recall things you have heard, seen or read?”
• “Do you ever forget names of people or everyday objects?”
• “Do you have any difficulty following conversations?”

41Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
Confidentiality is central to trust-based relationships between clinicians and patients,
and appropriate information sharing is vital for the provision of safe and effective
care. The General Dental Council (GDC) publication Standards for the Dental Team1
stipulates that dentists should explain to the patient the circumstances in which
they may share information, that they seek the patient’s consent to do so wherever
possible, and that in information sharing they are prepared to justify those decisions
and any action taken.
If a dentist feels there may be some evidence of memory difficulty or deterioration,
they can mention to the patient that they wish to write to the GP suggesting the
need for a more thorough check-up or review. The dentist can write briefly to the GP,
describing their observation and the reason for concern, requesting that the patient
be reviewed. If there is concern regarding the patient’s mental capacity, advice or
confirmation can be requested. Once a diagnosis has been made, it is essential that
the dental team are fully involved in the multi-disciplinary care resulting from that
diagnosis (for further information, refer to 2.1).
3.3 potential indicators of dental problems in people livinG witH dementia
There may come a time when the person with dementia is unable to voice that
they are experiencing pain or discomfort from their mouth or teeth. They will
need to rely on other people to notice and interpret their behaviour and to
arrange a dental appointment. There are however several behavioural changes
that may indicate that someone with dementia is experiencing dental problems.
These include:
• Refusal to eat or drink (particularly hard or cold foods).
• Frequent pulling at the face or mouth.
• Leaving previously worn dentures out of their mouth.
• Increased restlessness, moaning or shouting.
• Disturbed sleep.
• Refusal to take part in daily activities.

42 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
• Aggressive behaviour.
• Bruxism.
Physical signs that may also indicate a problem exists include drooling saliva, redness,
and or swelling. These signs should be taken in context with the clinical findings, previous
behaviours and knowledge. A pain diary collated by the carer may also be helpful.
If there is no explanation for the change in behaviour, arrangements should be made
to identify the cause, which may involve contacting the patient’s GP.
3.4 medication
There are no drug treatments that can cure Alzheimer’s disease or any other common
type of dementia. However, medicines have been developed for Alzheimer’s disease
that can temporarily alleviate symptoms or slow down their progression.
3.4.1 what are the main drugs used in the management of dementia?
There are two types of medication used to treat Alzheimer’s disease:
acetylcholinesterase inhibitors (often shortened to just ‘cholinesterase inhibitors’)
and N-methyl-D-aspartate (NMDA) receptor antagonists. The generic names for the
cholinesterase inhibitors are donepezil, rivastigmine and galantamine. Donepezil
was originally patented as the brand name Aricept, but is more widely available
now as just generic donepezil. Rivastigmine was patented as Exelon and is now also
available as other brands, as well as generic rivastigmine. Galantamine was patented
as Reminyl and is now also available as generic galantamine and the brands Reminyl
XL, Acumor XL, Galsya XL and Gatalin XL (see Table 3.4.1).
The NMDA receptor antagonist is memantine. It was originally patented as Ebixa and
is now also available as generic memantine. Other UK brand names for memantine
include Maruxa and Nemdatine.

43Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
table 3.4.1: the generic and brand names of the main drugs used in the
management of alzheimer’s disease.
Antipsychotic drugs (also known as neuroleptics or major tranquillisers) are a group
of medications that are usually used to treat people with mental health conditions
such as schizophrenia. They are also commonly prescribed for behavioural and
psychological symptoms in dementia. This is because in some cases they can
eliminate or reduce the intensity of psychotic symptoms, such as delusions and
hallucinations, and can have a calming and sedative effect.
Antipsychotic drugs benefit less than half of the people with dementia who take
them2 but can be an important part of their treatment. However, they can cause
serious side effects, especially when used for longer than 12 weeks. Possible side
effects include:
• Sedation (drowsiness).
• Parkinsonism (shaking and unsteadiness).
• Increased risk of infections.
• Increased risk of falls.
• Increased risk of blood clots.
CHOLINESTERASE INHIBITORS NMDA ANTAGONISTS
Generic Name Brand Name Generic Name Brand Name
Donepezil Aricept Memantine Ebixa, Maruxa,
Memdatine,
Nemdatine
Rivastigmine Exelon
Galantamine Reminyl, Reminyl XL,
Acumor XL, Galsya XL,
Gatalin XL

44 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
• Increased risk of stroke.
• Worsening of other dementia symptoms.
• Increased risk of death.
It is important to consider that antipsychotic drugs may help reduce behavioural and
psychological symptoms, but because of these side effects, this may be at the expense
of the person’s quality of life.
3.5 types of dental treatment
3.5.1 early stages of dementia
In the early stages of dementia, most types of dental care are still possible. The dentist
should plan treatment keeping in mind that the person with dementia will eventually
be unable to look after their own teeth. It is important at this stage that there is
strategic long-term oral care planning which avoids end-stage crisis management.
Care planning should be based on a detailed oral health risk asse ssment. Factors to
consider in the pre-dependent early stages oral health risk assessment are:
• Caries risk: number of exposed root surfaces; patient’s perception that their
mouth is dry (xerostomia); reduced saliva flow (salivary hypofunction);
medications; diet and nutrition; oral hygiene.
• Periodontal disease risk: presence of active disease; diabetes; smoking.
• Manual dexterity: the ability to maintain oral hygiene; level of fatigue when
an individual is undertaking oral hygiene themselves.
• Dependency: extent of dependence on carer/family member or residential care.
• Drugs and other co-morbidities: cardiovascular factors; Parkinson’s; diabetes.
Preventing further gum disease or decay is very important at this stage. Rigorous
preventive measures (both home and surgery-based) should be put in place so that
they become routine for both the individual and their carer. Prescription of high
fluoride toothpaste (5000ppm) may be considered, and professional application
of high fluoride varnish twice yearly may be beneficial.

45Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
Restorative treatment should be high quality and low maintenance. Where possible,
treatment should be simple, serviceable and (ideally) easily cleansable. Key teeth
should be identified and restored, such as canines, molars and occluding pairs.
Crowns, bridges and implants should only be considered if someone is prepared to
carry out daily brushing for the person living with dementia, should the person reach
a stage where they cannot do this for themselves.
At this stage, when the person is able to participate in discussions about their
treatment, some consideration should be given to long-term outcomes, such as a
shortened dental arch with the aim of securing adequate function and nutrition. In
cases where the patient may need to be rendered edentulous, consideration might be
given to two-implant retained overdentures, as per the McGill consensus statement.3
As dementia is a progressive condition, it is important for the individual and their
carer to receive continuing advice on prevention from the dentist and the dental team.
They may need to be reminded to carry out the task, or they may need to be
supervised. If they need help, the carer can try offering them the brush and
toothpaste and showing them what to do. As manual dexterity decreases, an electric
toothbrush, or toothbrush with an adapted handle to improve grip, may help maintain
independence (see 2.1.2 for useful information and guidance from BSG and BSDH).
3.5.2 middle stages of dementia
During this stage of dementia, the person may be relatively physically healthy
but have lost some cognitive abilities. The focus of treatment is likely to be on
prevention of further dental disease, from restoration and rehabilitation to
maintenance and prevention. During this stage, the person is often relatively
physically healthy, but increasingly cognitively impaired. Patients with support
may still be able to receive dental care with little or no difficulty. For some,
however, changes in behaviour – including agitation or aggression – may occur

46 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
when a person feels threatened, intimidated or agitated. With reduced powers
of logic and reason and heightened emotional responses, people may lash out
where they previously might have behaved in a very different way. The decision
will be based on the individual’s ability to co-operate, their dental treatment
needs, general health and social support. Rigorous prevention should be continued,
adapted visit procedures considered and more frequent recall visits and support
for carers arranged as appropriate.
At this point it may be decided that the patient no longer has the capacity to
consent to their dental treatment. It is during the middle stages that issues
around consent to treatment may start to arise (see section 3.7.4). This is where
the Mental Capacity Act4 states that we must assess capacity, act in the patient’s
best interest and choose the least restrictive treatment option. Having been involved
in treatment decisions the patient may have made previously, this is where the GDP
is truly valuable, especially as they are already aware of who may wish to be involved
in communication about the patient’s care. At this stage, the GDP may also choose
to refer to a special care dental service for specialist advice and continuing care,
which may include sedation or general anaesthesia for their dental treatment.
3.5.3 later stages of dementia
In the later stages of dementia, the person is likely to have severe problems with
thinking, reasoning and memory and will often be physically frail or disabled with
complex medical conditions. Treatment at this stage focuses on prevention of dental
disease, maintaining oral comfort and provision of emergency treatment. Dental
interventions should be as non-invasive as possible, for example using Carisolv® for
caries removal, atraumatic restorative techniques (ART) such as glass ionomer cement
restorations, and regular application of high fluoride varnish to control root caries.
Changes in an individual’s ability or desire to maintain oral health are likely. They
may lose the ability to clean their teeth, or an interest in doing so, and carers may

47Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
need to take over this task. Even people with very advanced dementia can retain the
capability of tooth brushing if handed a toothbrush. A dentist or hygienist can provide
guidance and support on how to clean another person’s teeth. The technique will vary
depending on the individual concerned (for further information, refer to section 2.1.3).
3.6 additional issues
The dental professional can help support good practice in managing dementia by
being aware of other conditions that have a bearing on the its impact. For example,
dehydration can have a negative effect on people with dementia, causing a worsening
of symptoms and leading to medical problems. A person with dementia should drink
at least 1.2 litres of fluids a day. Dehydration can lead to:
• Headaches.
• Increased confusion.
• Urinary tract infections.
• Constipation.
These can all worsen the symptoms of dementia. As people get older, the sensation
of thirst changes, which can lead to people being unaware that they are dehydrated.
A person with dementia may have similar difficulties. They may also be less able to
provide drinks for themselves.
The person should be encouraged to drink throughout the day, but placing a drink
in front of someone does not mean they will drink it. An empty cup does not mean
the contents have been drunk; it may have been spilled, drunk by someone else or
poured away. Daily living aids such anti-spill mugs, beakers or protective drink lids
should be considered.
3.7 Key standards
In this section, five key standards have been identified that relate to the previous
discussions. These cover:

48 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
• Ensuring the medical history is up-to-date and the practitioner is aware of
the drug regime being used.
• An appreciation of the potential side effects of the drug regimes and their
influence on oral conditions.
• Treatment planning that recognises the possible impact that dementia may
have on the individual.
• Consent and capacity.
• Safeguarding against physical or financial abuse.
3.7.1 medical History
The medical history form should conform, where possible, to the principles outlined
in section 3.1 on written material. The initial assessment of a new patient and their
drug regime may give an indication that the individual has been diagnosed with
dementia. Quite often people with dementia have a list of all the drugs they are
currently taking, as frequently they are requested to provide it, and subsequently
the list is either created themselves or provided by the GP or pharmacist. The dental
professional should explore with the patient and/or carer/relative what drugs the
patient is taking and seek clarification as required.
The basic standard is for the medical history to be completed (new patient)
or updated (subsequent visits) including details of any drug regimes. B
The aspirational standard is for the original medical history to be signed and
dated by the patient, carer/relative as appropriate, and the clinician. For new
patients, a history of relevant past medication regimens should be sought. A
For computerised systems, electronic entries and updates may suffice.

49Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
3.7.2 side effects
As with the majority of medications, those used in the management of the dementia have
side-effects. As highlighted above, these include some general impacts as well as those
specific to the oral environment. In particular, the medications can give rise to xerostomia
which in turn has implications for care modalities and subsequent management.
The aspirational standard will include a discussion with the patient/carer/relative on the
side effects of the drug regime the individual is on and how best the potential problems
arising can be managed. This should include discussions with the patient/carer/relative
on maintaining their fluid intake, dietary advice (especially concerning achieving a
low intake of sugars) and appropriate fluoride exposure. The preventive approach, as
outlined in Delivering Better Oral Health,5 should be followed where possible. Discussions
should also cover the potential problems arising in chewing and swallowing. A
Basic standard would cover discussions with the patient/carer/relative on the impact
on reduced salivary flow and basic oral hygiene advice. B
3.7.3 planning treatment
Once a person has a dementia diagnosis, it is important to establish an individual,
long-term dental care plan. The long-term objective is to eliminate pain, control
infection and prevent new disease. This is facilitated by a timely dementia diagnosis,
as a person in the early stages of the condition is more likely to be receptive to
treatment and be able to take an active role in decision-making.
Treatment planning must take account of the stage of the illness and the level of
cognitive impairment. Ideally, a dentist should form part of a multidisciplinary
care team. There may be an integrated care pathway for people diagnosed with
progressive neurogenic disorder. Members of the dental team are important in this
pathway approach to ensure that oral care can be planned throughout the disease
process, and does not become crisis management in the later stages of dementia.

50 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
From the outset, it is important to work in partnership with the carer and/or
family to obtain an accurate assessment of cognitive impairment. They should also
be able to advise how well the person is maintaining a dental hygiene routine,
whether they remain physically able to brush their teeth and whether they may
benefit from an electric toothbrush, or modified toothbrush with an adapted handle
or specialised head.
The dental care plan must take into account that as dementia progresses, the person
affected may become less able to:
• Express their needs or wishes and to explain what they want.
• Understand and explain dental symptoms, such as pain.
• Take part in the decision-making process about treatment.
• Give informed consent.
• Tolerate dental interventions.
• Perform daily living activities such as oral hygiene.
• Understand that oral hygiene needs to be carried out.
For people with or without dementia, the recommended interval between check-
ups at the dentist should be determined specifically for the individual and tailored
to meet their needs, based on assessment and risk of dental disease. For adults, the
shortest interval that is recommended is three months, and the longest is two years.
If treatment becomes necessary for a person with dementia, the dentist (together
with the person and their family or carers) will discuss treatment needs and agree
on the best treatment plan. They should take into consideration:
• The level of independence, co-operation, cognitive abilities, mental state,
and physical impairment of the person with dementia.
• What (if any) dental symptoms or problems the person is experiencing.
• Whether the person is able to give informed consent.
• A Clinical Dementia Rating may be available. This is a five-point scale used to
characterise six domains of cognitive and functional performance applicable

51Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
to Alzheimer’s disease and related dementias and allows a care professional
to understand and follow the disease progression (see Appendix A6).6
Once these questions have been answered, the dentist will be able to decide on
the most appropriate treatment. They will also decide how regularly they need
to see the person.
The aspirational standard for treatment planning should include a detailed proposal
for the long-term management of the individual. This should be broken down into
immediate care proposals and longer-term management and cover both clinical need
and the self-care management programme, including advice on the use of fluorides,
and dietary sugars.
This should be patient and condition specific, should also include recommended
recall intervals, and a written copy that follows the guidance above should be given
to the patient and/or carer/relative. A
For a basic standard, the clinician should provide a treatment plan that covers
proposals for managing the current oral problems and generic advice on self-care.
Details of a recall interval should be provided. B
Conditional standard provides details of the current treatment plan being proposed
and offers no generic advice on self-care. C
3.7.4 consent and capacity
Consent to treatment must be confirmed, ideally in writing, and certainly recorded
in patient’s notes. If treatment is being carried out over several visits, then consent
must be sought and given at every visit. For consent to be valid, it must be:
• Given by a person with the capacity to make the decision in question.
• Given voluntarily.

52 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
• Based on appropriate information.
• Understood.
The nature of the disease may mean that capacity to consent may vary, as consent
is time and procedure specific – consent is given for that treatment at that time. If
any of the above criteria are missing, the patient is not considered to have given
permission to proceed to treatment.
For patients with late stage dementia, assent needs to be sought from the family
member/carer who accompanies the patient at the time of the dental visit. It is
essential to be aware of any lasting power of attorney (LPA) (see 2.1.1.3), as the
person attending with the patient may not be the person who holds that power, and
consequently not be in a position to sign, should written consent be required.
The capacity of an individual to understand is currently defined in Section 1 (2) of the
Mental Capacity Act 2005.4 It states that “a person must be assumed to have capacity
unless it is established that he lacks capacity.” When assessing an individual’s capacity
there are two elements to consider:
1. Does the person have an impairment of the mind or brain, or is there some sort
of disturbance affecting the way their mind or brain works? (It does not matter
whether the impairment or disturbance is temporary or permanent).
2. If so, does that impairment or disturbance mean that the person is unable to
make the decision in question at the time it needs to be made?7
In emergency situations, the ‘best interests’ principle may be used. This principle in
the Mental Capacity Act 2005 states that any act done or decision made on behalf
of an adult lacking capacity must be in their best interests.4 This can cover financial,
health and social care decisions. The person making the decision is the ‘decision-
maker’ and is likely to be the person caring for the patient on a day-to-day basis;
the doctor or other member of the healthcare staff responsible for carrying out the

53Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
particular treatment or procedure; or an LPA or Court of Protection deputy.
The Act sets out what to consider when deciding what is in the best interests
of the patient. The following should be taken into account:
• Past and present wishes and feelings.
• Beliefs and values that may have influenced the decision being made,
had the person had capacity.
• Other factors that the patient would be likely to consider if they had capacity.
If the patient has been attending the practice for some time, it may aid your decision-
making if you are aware of previous treatment choices, but you must have objective
reasons for any decision you make. You must also be able to show that you considered
all circumstances relevant to the decision in question. All options and decisions taken
should be noted in records.
To reach the basic standard the dentist should have:
• Explained the diagnoses made. B
• Explained the treatment options. B
• Explained the consent and decision-making process to the patient. B
• Taken into account the level of dementia the patient is living with. B
This should include issues associated with self-care and longer-term
control of oral diseases. B
The risks and benefits of the differing options should be explained and discussed with
the patient and or carer/relative, including costs, as well as the impact, recovery time
and subsequent importance of maintenance of any treatment. B
A signed copy of the agreed proposal should be given to the patient and/or carer/
relative, and a copy kept in the patient’s notes. An assessment of the patient’s
capacity should be included along with details of the diagnosis and treatment

54 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
options. Risks and benefits and costs should be prepared and discussed with the
patient/carer or relative. A
3.7.5 safeguarding
Safeguarding means protecting people’s health, wellbeing and human rights, and
enabling them to live free from harm, abuse and neglect. Achieving this requires
individual care providers and organisations to work together to mitigate the risk
of abuse or neglect, and to stop harm from occurring.
Abuse and improper treatment includes care or treatment that is degrading,
and care or treatment that significantly disregards their needs or that involves
inappropriate recourse to restraint. For these purposes, ‘restraint’ includes the
use or threat of force, as well as physical, chemical or mechanical methods of
restricting liberty to overcome a person’s resistance to the treatment in question.
Where any form of abuse is suspected, occurs, is discovered, or reported by a
third party, the provider must take appropriate action without delay. The action
they must take includes investigation and/or referral to the appropriate body.
This applies whether the third party reporting an occurrence is internal or external
to the provider. Potential sexual, emotional and financial abuse should also
be considered.
The basic standard for safeguarding should include that the dental provider is aware of
what to do if there are concerns about maltreatment, be aware of any safeguarding lead
with the practice or organisation including local policies and procedures around who to
contact, where to obtain further advice and support, and have awareness of the referral
process. Details should be kept in the patient notes of all actions undertaken. B

55Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
SuMMARy Of RECOMMENDATIONS
KEY: A – ASpIRATIONAL B – BASIC C – CONDITIONAL
MediCal history
For new patients, medical history completed including
details of any drug regimes B
For existing patients, medical history updated including
details of any drug regimes B
Original medical history signed and dated by patient,
carer/relative if appropriate, and clinician. For new patients,
history of relevant past medication regimens sought A
side effeCts of MediCations
Discussion with patient/carer/relative about side effects
of drug regime and management of potential issues A
Discussion with patient/carer/relative about fluid intake,
dietary advice and fluoride exposure A
Discussion with patient/carer/relative about potential
problems relating to chewing and swallowing A
Discussion with patient/carer/relative about impact
of reduced salivary flow and basic oral hygeine advice B
treatMent planning
Proposals for immediate care addressing current problems B
Generic advice on self-care B
Proposals for longer-term management of the individual A
Individual self-care management programme
(use of fluorides, dietary sugars, etc) A

56 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
Recommended recall intervals B
Written copy given to patient and/or carer/relative A
Details of treatment being proposed C
Consent and CapaCity
Valid consent obtained B
Explain diagnosis/diagnoses made B
Explain the treatment options B
Explain consent and decision-making process to the patient B
Take into account the level of dementia
(including self-care and longer-term control) B
Risks and benefits of differing options explained
(including costs, impact, recovery and maintenance) B
Signed copy of agreed proposals given to patient and/or
carer/relative and kept in notes, including capacity assessment A
safeguarding
Be aware of process for concerns about maltreatment B
Be aware of safeguarding lead for practice or organisation B
Be aware of local policies and procedures B
Be aware of who to contact, where to access advice and referral process B
Keep notes on all actions undertaken B

57Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
3.9 references and resources1. General dental council (Gdc). standards for the dental team. Gdc; london: 2013. available
at: http://standards.gdc-uk.org.
2. banerjee s. the use of antipsychotic medication for people with dementia: time for action.
2009. available at: www.rcpsych.ac.uk/pdf/antipsychotic%20bannerjee%20report.pdf
3. feine js, carlsson Ge, awad ma, chehade a, duncan wj, et al. the mcGill consensus statement
on overdentures. mandibular two-implant overdentures as first choice standard of care for
edentulous patients. int j oral maxillofac implants 2002;17(4):601-2.
4. office of the public Guardian. mental capacity act: making decisions. 2014. available at:
www.gov.uk/government/collections/mental-capacity-act-making-decisions.
5. public Health england (pHe). delivering better oral Health: an evidence-based toolkit for
3.8 summary
The general approach to managing individuals who may have dementia is the
same as that for the population as a whole. However, certain factors have to be
modified in light of the likely impact that dementia will have on the individual,
namely their ability to manage their oral tissues and the impact that medications
can have on them.
Five areas have been identified in which standards for dementia care provision
will contribute to ensuring the qualities of care to patients. These include:
• Ensuring the medical history is valid and using it as a tool to quantify
the rate of progression of the condition (covered in 2.1).
• The side-effects of the drugs most commonly used in the management
of the condition, and their impact (covered in 3.4).
• Issues when planning treatment (covered in 3.7.3).
• Issues surrounding consent and capacity (covered in 3.7.4).
• Safeguarding (covered in 3.7.5).
Reaching the aspirational standards in these areas, as well as following the
guidance for dental care in general, will help ensure high standards of dental
care for people living with dementia.

58 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
prevention. 2017. available at: www.gov.uk/government/publications/delivering-better-oral-
health-an-evidence-based-toolkit-for-prevention.
6. washington university in st louis (wusl). clinical dementia rating worksheet. available at:
http://alzheimer.wustl.edu/cdr/cdr.htm
7. royal college of surgeons (rcs). consent: supported decision-making. a Guide to Good practice
available at: www.rcseng.ac.uk/library-and-publications/college-publications/docs/consent-good-
practice-guide.
Resources and further reading
alzheimer’s society, mistreatment and abuse of people with dementia. available at: www.
alzheimers.org.uk/info/20091/position_statements/205/mistreatment_and_abuse_of_people_
with_dementia.
british society for Gerontology and bristish society for disablity and oral Health (2014). looking
after the mouth. available at: www.1000livesplus.wales.nhs.uk/looking-after-the-mouth
dougall a. special care dentistry: caring for frail older people. 2016. ageing & oral Health joint
seminar series from the faculty of General dental practice (ireland) and the dublin dental
university Hospital, trinity college dublin.
fiske j, frenkel H, Griffiths j, jones v. Guidelines for the development of local standards of oral
health care for people with dementia. Gerodontology 2006;23(suppl 1):5-32.
Hee thames valley & wessex dental school. the appointment. available at: www.oxforddeanery.
nhs.uk/dental_school_home.aspx.
monaghan dt, jane de. pharmacology of nmda receptors. in: van dongen am, editor. biology
of the nmda receptor. boca raton (fl): crc press/taylor & francis; 2009. (available at: https://
www.ncbi.nlm.nih.gov/books/nbK5282/)
royal college of paediatrics and child Health (rcpcH). safeguarding children and young people:
roles and competences for health care staff intercollegiate document 3rd edition: march 2014.
available at: www.rcpch.ac.uk/sites/default/files/page/safeguarding%20children%20-%20roles%20
and%20competences%20for%20Healthcare%20staff%20%2002%200%20%20%20%20(3).pdf.
social care institute for excellence (scie). safeguarding people with dementia. 2017. available
at: www.scie.org.uk/dementia/after-diagnosis/support/safeguarding.asp.

59Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
4.1 IntroductIon
There is a wealth of material available to help all health providers address the
challenges that dementia creates. This final section is divided into four sub-sections,
dealing with staff training and awareness, local support networks, patient information
leaflets, and self-help. In addition, there is a section covering further reading and
sources of information that may be helpful.
4.2 Staff traInIng and awareneSS
Each and every member of the dental team plays an important role in the patient
journey through their dental visit. Being aware of the difficulties some patients face in
booking and keeping their appointments, accessing the dental surgery and even getting
as far as the dental chair is the first step to addressing the barriers they face. Positively
welcoming patients and offering the opportunity to ask questions can help set a
positive tone for the appointment. It is also worth remembering that a patient with
dementia will have the same anxieties about dental care as the rest of the population.
Continuity of care is a valuable aspect of general dental practice. Often patients and
their family members attend over a long period of time, and a beneficial rapport
can be established. Even with patients who are anxious or reluctant, the dentist
can build a professional relationship and understanding. As well as the clinical and
technical aspects of dental care, the dental team play a vital role in presenting a
patient-centred approach to each dental appointment. The practice receptionist and
dental nurse may establish a good relationship with the patient and family members,
observing any subtle dynamics or support given. A holistically-minded general dental
practitioner and dental team are well positioned to spot any changes in memory,
behaviour and ability to communicate, which may be indicative of the early stages of
S U P P O R T M A T E R I A L S A N D F U R T H E R R E A D I N G4

60 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
dementia. While not suggesting that a diagnosis can (or should be) made in the dental
chair, having a regular and open dialogue with a patient and, where appropriate,
their family could provide the context for discussion concerns about their memory.
The dentist can signpost a patient to their GP or resources such as Alzheimer’s Society
Worried about your memory?1
All members of the dental team could consider becoming a Dementia Friend,2 a
national initiative run by Alzheimer’s Society to change the way the nation thinks,
talks and acts when it comes to dementia. The campaign aims to create a more
dementia-friendly society by encouraging four million people to become Dementia
Friends by 2020. Dementia Friends learn more about what it is like to live with
dementia and how to turn that understanding into action – anyone of any age can
become a Dementia Friend by attending a 45-minute face-to-face awareness session
run by a Dementia Friends Champion. It is easy to find a local session or organise one
in your practice via the Dementia Friends website.2
Further training, qualifications and continuing professional development (CPD)
accredited courses for health professionals are available through Alzheimer’s Society3
and Skills for Care.4 This will enable further understanding of the challenges people
living with dementia might face, and equip with skills and practical knowledge to
support patients affected by dementia. Training should be available not just on
dementia in isolation but how this impacts specifically on treatment planning and
delivering dental treatments to patients affected by dementia.
4.3 LocaL Support networkS
Practices can become part of their local Dementia Friendly Community5 or
Dementia Action Alliance6 to get support and advice on how to become dementia-
friendly. This can be done by contacting your local Alzheimer’s Society office or
emailing [email protected] who will put you in touch
with your local community.

61Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
Alzheimer’s Society facilitates user engagement through Living with dementia and
Service User Review Panels. These groups across the country are made of people with
dementia. You might be interested in either visiting one of these groups to hear about
the challenges people living with dementia face when visiting the dentist, or seeing
if a group could conduct an audit of your practice to recommend any changes.
Additional support may be found by contacting the following groups in your area
should they exist: Local Dental Networks, Managed Clinical Networks for Special Care
Dentistry, NHS England local dental commissioning team, Health Education England,
the Local Authority Public Health and Adult & Social Care Services.
4.4 patIent InformatIon LeafLetS
Alzheimer’s Society has worksheets on different topics related to this standard. These
are available for downloading at the Society’s web page: www.alzheimers.org.uk.
4.5 SeLf heLp
The later stages of dementia can be a distressing time for carers and relatives.
There is support available if patients need it. Alzheimer’s Society’s National
Dementia Helpline (0300 222 1122, national call rates apply) provides information,
support, guidance and signposting to other organisations. Admiral Nursing
Direct dementia helpline (0800 888 6678, freephone) can provide specialist
practical and emotional support.
4.6 referenceS and reSourceS1. alzheimer’s Society. worried about your memory? available at: www.alzheimers.org.uk/downloads/
file/339/worried_about_your_memory_english_version.
2. dementia friends – an alzheimer’s Society initiative. available at: www.dementiafriends.org.uk.
3. alzheimer’s Society. training and consultancy. available at: www.alzheimers.org.uk/info/20050/
training_and_consultancy.
4. Skills for care. Support for our dementia workforce. available at: www.skillsforcare.org.uk/topics/
dementia/dementia.aspx.

62 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
5. alzheimer’s Society. dementia friendly communities. available at: www.alzheimers.org.uk/
info/20079/dementia_friendly_communities.
6. dementia action alliance. available at: www.dementiaaction.org.uk.
Resources and further reading
there are a considerable number of additional readings and interactive material available to help
support care providers. In particular, the web addresses listed below provide a sample of useful
learning materials on how to support those living with dementia and their carers.
the authors Journal compilation. Blackwell munksgaard Ltd, gerodontology 2006;23(Suppl.
1):3–32. available at: http://onlinelibrary.wiley.com/store/10.1111/j.1741-2358.2006.00140.x/
asset/j.1741-2358.2006.00140.x.pdf;jsessionid=846940275a6d67348d1c095d36656339.f03t04?v=
1&t=izemd9y3&s=b5b5f17672584715cce3a3468fc4f018b0cb09ad
alzheimer’s Society. types of dementia. 2017. available at: www.alzheimers.org.uk/info/20007/
types_of_dementia.
admiral nursing direct dementia helpline, open monday to Sunday: 0800 888 6678.
alzheimer’s Society helpline, open monday to Sunday: 0300 222 11 22.
Bentler Se, morgan ro, Virnig Ba, et al. evaluation of a patient-reported continuity of care model
for older adults. Qual Life res 2014;23:185. doi:10.1007/s11136-013-0472-z
ettinger rL. dental management of patients with alzheimer’s disease and other dementias.
gerodontology 2000;17:8–16.
fiske J, frenkel h, griffiths J, Jones V, British Society of gerodontology; British Society for disability
and oral health. 2006. guidelines for the development of local standards of oral health care for
people with dementia
hill a, freeman g. promoting continuity of care in general practice. London: royal college of
general practitioners; 2011.
health education england. dementia guide for carers and care providers. available at: https://hee.
nhs.uk/our-work/person-centred-care/dementia/dementia-guide-carers-care-providers.
hoben m, kent a, kobagi n, et al. effective strategies to motivate nursing home residents in oral
healthcare and to prevent or reduce responsive behaviours to oral healthcare: a systematic review
protocol. BmJ open 2016;6:e011159. doi:10.1136/bmjopen-2016- 011159.

63Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
kurrle S. oral disease. In: kurrle, S., hogarth, r. and Brodaty, h. ed. physical comorbidities of
dementia. cambridge; cambridge university press: 2012;99-110.
nhS england cheshire and merseyside dementia friendly dentistry advice and guidance
for the primary dental care team. available at: http://healthwatchwirral.co.uk/wp-content/
uploads/2016/07/dementia-friendly-dentistry-Book-may-SoV.pdf.
preston a. the oral health of individuals with dementia in nursing homes. gerodontology
2006;23(2):99–105.
prince m, Bryce r, albanese e, wimo e, ribeiro w and ferri cp. (2013) the global prevalence of
dementia: a systematic review and metaanalysis
Skills for health (2015) dementia core Skills education and training framework (available at:
http://www.skillsforhealth.org.uk/services/item/176-dementia-core-skills-education-and-training-
framework) accessed: July 2017
Social care policy, dh. (2011) Safeguarding adults: the role of health service practitioners
turner d, tarrant c, windridge k, Bryan S, Boulton m, freeman g, et al. do patients value
continuity of care in general practice? an investigation using stated preference discrete choice
experiments. J health Serv res policy 2007;12:132-7.
64 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
Glossary of abbreviations and acronyms
ART Atraumatic restorative techniques
BPSD Behavioural and psychosocial symptoms of dementia
BSDH British Society for Disability and Oral Health
BSG British Society of Gerodontology
CPD Continuing professional development
FGDP(UK) Faculty of General Dental Practice (UK)
GDC General Dental Council
GDP General dental practitioner
HCP Healthcare professional
LPA Lasting power of attorney
MCI Mild cognitive impairment
NICE National Institute for Health and Care Excellence
NMDA N-methyl-D-aspartate (receptor antagonist)
SALT Speech and language therapist
VERA Validation, emotional context, reassurance, activity
S E L E C T E D D E F I N I T I O N Sa1

65Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
A B B E y P A I N S C A L Ea2
for measurement of pain in people with dementia who cannot verbalise
how to use scale: while observing the resident, score questions 1 to 6.
name of resident
name and designation of person completing the scale:
date time
last pain relief given was at hrs
Q1. Vocalisation (eg. whimpering, groaning, crying)
absent 0 mild 1 moderate 2 severe 3 Q1
Q2. Facial expression (eg. looking tense, frowning, grimacing, looking frightened)
absent 0 mild 1 moderate 2 severe 3 Q2
Q3. Change in body language (eg. fidgeting, rocking, guarding part of body, withdrawn)
absent 0 mild 1 moderate 2 severe 3 Q3
Q4. Behavioural change (eg. increased confusion, refusing to eat,
alteration in usual patterns)
absent 0 mild 1 moderate 2 severe 3 Q4
Q5. Physiological change (eg. temperatire, pulse or blood pressure
outside normal limits, perspiring, flushing or pallor)
absent 0 mild 1 moderate 2 severe 3 Q5
continued overleaf
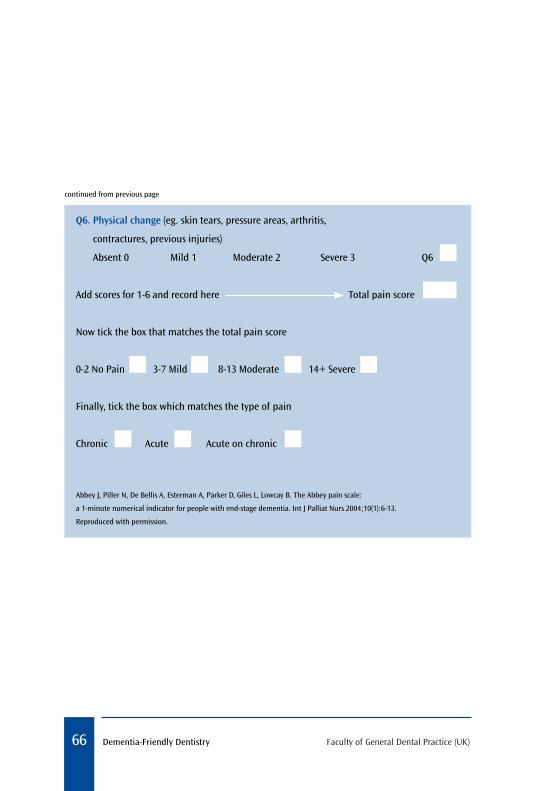
66 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
Q6. Physical change (eg. skin tears, pressure areas, arthritis,
contractures, previous injuries)
absent 0 mild 1 moderate 2 severe 3 Q6
add scores for 1-6 and record here total pain score
now tick the box that matches the total pain score
0-2 no pain 3-7 mild 8-13 moderate 14+ severe
finally, tick the box which matches the type of pain
chronic acute acute on chronic
abbey J, piller n, de bellis a, esterman a, parker d, Giles l, lowcay b. the abbey pain scale:
a 1-minute numerical indicator for people with end-stage dementia. int J palliat nurs 2004;10(1):6-13.
reproduced with permission.
continued from previous page

67Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
C O M M U N I C A T I O N V I S U A L A I Da3
communicatinG with patients with dementia
Introduce by name and role
Verbal
approach patient from front and maintain eye contact
address patient by preferred name – if unsure, start formally
refer to people and things by their name, eg. “your daughter Jan”
Give time for your patient to process information, using familiar words and terms
ask one question at a time, giving time to understand and respond
Keep requests simple and specific
Do not interrupt the patient while they are speaking
repeat answer back to patient to check understanding
Avoid keeping the patient
waiting
enVIronment
Avoid back-ground noises (equipment,
talking, music, etc)
Make sure patient has
reading glasses, hearing aids
and pain control in place
Ensure basic needs are
met (hunger, thirst, need for
the toilet)Use a calm and reassuring tone
Use calm and reassuring body
language
non-Verbal
Physical touch can be
reassuring but be aware of
cultural norms
Try not to overwhelm with too many direct
questions
Be patient and divert back to conversation if
it veers off-topic

68 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
A D A P T E D H A N D L E T O O T H - B R U S H I N G A I D Sa4
images a-d from national institute of dental and craniofacial research. dental care every day: a caregiver’s Guide. february 2012. reproduced with permission. available at: www.nidcr.nih.gov/oralhealth/topics/developmentaldisabilities/dentalcareeveryday.htm
image e used with kind permission from tepe oral hygeine products ltd.
a a velcro strap, often used to hold eating utensils, can be attached to the toothbrush
b a wide elastic band can be looped over the toothbrush to attach it to the hand
c tubing (such as a bicycle handle grip) slipped over the handle of the toothbrush may provide additional control
d an electric toothbrush may be easier to hold
e specially designed aids are available to improve manual toothbrush grip
a b
c
d
e

69Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
T E C H N I q U E F O R A S S I S T E D B R U S H I N Ga5
national institute of dental and craniofacial research. dental care every day: a caregiver’s
Guide. february 2012. reproduced with permission. available at: www.nidcr.nih.gov/oralhealth/topics/
developmentaldisabilities/dentalcareeveryday.htm

70 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
subject initials: Impairment
none0
QuestIonable0.5
mIlD1
moDerate2
seVere3
memory no memory loss or slight inconsistent forgetfulness
consistent slight forgetfulness; partial recollection of events; “benign” forgetfulness
moderate memory loss; more marked for recent events; defect interferes with everyday activities
severe memory loss; only highly learned material retained; new material rapidly lost
severe memory loss; only fragments remain
orientation fully orientated fully orientated except for slight difficulty with time relationships
moderate difficulty with time relationships; orientated for place at examination; may have geographic disorientation elsewhere
severe difficulty with time relationships; usually disoriented to time, often to place
orientated to person only
Judgement & Problem solving
solves everyday problems and handles business and financial affairs well; judgement good in relation to past performance
slight impairment in solving problems, similarities, and differences
moderate difficulty in handling problems, similarities, and differences; social judgement usually maintained
severely impaired in handling problems, similarities, and differences; social judgement usually impaired
unable to make judgements or solve problems
Community affairs independent function at usual level in job, shopping, volunteer and social groups
slight impairment in these activities
unable to function independently at these activities although may still be engaged in some; appears normal to casual inspection
no pretence of independent function outside home
appears well enough to be taken to functions outside a family home
appears too ill to be taken to functions outside a family home
Home & Hobbies life at home, hobbies, and intellectual interests well maintained
life at home, hobbies, and intellectual interests slightly impaired
mild but definite impairment of function at home; more difficult chores abandoned; more complicated hobbies and interests abandoned
only simple chores preserved; very restricted interests, poorly maintained
no significant function in home
Personal Care fully capable of self-care needs prompting requires assistance in dressing, hygiene, keeping of personal effects
requires much help with personal care; frequent incontinence
C L I N I C A L D E M E N T I A R A T I N G ( C D R )a6clinical dementia
ratinG (cdr): 0 0.5 1 2 3

71Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
subject initials: Impairment
none0
QuestIonable0.5
mIlD1
moDerate2
seVere3
memory no memory loss or slight inconsistent forgetfulness
consistent slight forgetfulness; partial recollection of events; “benign” forgetfulness
moderate memory loss; more marked for recent events; defect interferes with everyday activities
severe memory loss; only highly learned material retained; new material rapidly lost
severe memory loss; only fragments remain
orientation fully orientated fully orientated except for slight difficulty with time relationships
moderate difficulty with time relationships; orientated for place at examination; may have geographic disorientation elsewhere
severe difficulty with time relationships; usually disoriented to time, often to place
orientated to person only
Judgement & Problem solving
solves everyday problems and handles business and financial affairs well; judgement good in relation to past performance
slight impairment in solving problems, similarities, and differences
moderate difficulty in handling problems, similarities, and differences; social judgement usually maintained
severely impaired in handling problems, similarities, and differences; social judgement usually impaired
unable to make judgements or solve problems
Community affairs independent function at usual level in job, shopping, volunteer and social groups
slight impairment in these activities
unable to function independently at these activities although may still be engaged in some; appears normal to casual inspection
no pretence of independent function outside home
appears well enough to be taken to functions outside a family home
appears too ill to be taken to functions outside a family home
Home & Hobbies life at home, hobbies, and intellectual interests well maintained
life at home, hobbies, and intellectual interests slightly impaired
mild but definite impairment of function at home; more difficult chores abandoned; more complicated hobbies and interests abandoned
only simple chores preserved; very restricted interests, poorly maintained
no significant function in home
Personal Care fully capable of self-care needs prompting requires assistance in dressing, hygiene, keeping of personal effects
requires much help with personal care; frequent incontinence
score only as decline from previous usual level due to cognitive loss, not impairment due to other factors.
morris Jc. the clinical dementia rating (cdr): current version and scoring rules. neurology 1993;43:2412-2414. reproduced with permission.

72 Dementia-Friendly Dentistry Faculty of General Dental Practice (UK)
antImICrobIal PresCrIbInG for General Dental PraCtItIonersAntimicrobial Prescribing for General Dental Practitioners provides guidance on the prescribing of antimicrobials to adults and children in primary dental care. It gives clear, simple and practical advice on when to prescribe, what to prescribe, for how long and at what dosage. An invaluable asset in any dentist’s library, the current edition reflects changes to recommendations since the previous (2006) update, and includes dosage recommendations for children for the first time.• Available in hard copy format, e-book format, and free-of-charge online.
ClInICal examInatIon anD reCorD-KeePInG: GooD PraCtICe GuIDelInesCovering dental records, history-taking, full examination, recall visits, consent, confidentiality, data protection, referrals, electronic records, special situations and more, this third edition of Clinical Examination and Record-Keeping has been fully updated and expanded to reflect technological and regulatory developments, and introduces a simple ‘ABC’ system for grading its recommendations. The hard copy also includes scenarios to put the guidance into context, as well as a series of extensive appendices, diagrams, charting notes and template forms which dental professionals may adopt for use in their practice.• Available in hard copy format and free-of-charge online.
seleCtIon CrIterIa for Dental raDIoGraPHySelection Criteria for Dental Radiography is the leading text on indications for radiographic investigation. Based on a comprehensive review of all of the available data and guidance, and wide consultation with relevant professional bodies and specialist groups to provide consensus on best practice, it gives clear, simple and practical advice on the safe and effective use of radiography in practice.• Available in hard copy format, e-book format, and free-of-charge online.
stanDarDs In DentIstryStandards in Dentistry brings together all previous standards and guidelines in oral healthcare, including material published by the FGDP(UK), BDA, GDC, ISO, and the Department of Health, among others. The comprehensive manual includes tables of clinical outcomes, based on the FGDP(UK)’s previous publication Self-Assessment Manual and Standards (SAMS), covering 17 treatment areas in both primary and secondary care dentistry. This ambitious package is an indispensable compendium for the conscientious oral healthcare professional in helping to guide personal or practice-based quality assessment.• Available in hard copy format with accompanying online access for purchasers.
O T H E R S T A N D A R D S A N D G U I D A N C E P U B L I C A T I O N S F R O M T H E F G D P ( U K )
all available at www.fgdp.org.uk


Faculty of General Dental Practice (UK)
Email: [email protected] Website: www.fgdp.org.uk
Dementia-Friendly
Dentistry
Good Practice Guidelines