dermatology & plastic surgery institute - cleveland clinic · 1 dermatology & plastic...
TRANSCRIPT

Outcomes | 2007
Dermatology &Plastic Surgery
Institute

Patients First
282972A.indd 2 6/19/08 3:33:51 PM

Dermatology & Plastic Surgery Institute1
Outcomes 2007
Patients First
Quality counts when referring patients to hospitals and physicians, so Cleveland Clinic has created a series of Outcomes
books similar to this one for many of its institutes. Designed for a healthcare provider audience, the Outcomes books
contain a summary of our surgical and medical trends and approaches, data on patient volume and outcomes, and a
review of new technologies and innovations.
Although we are unable to report all outcomes for all treatments provided at Cleveland Clinic — omission of outcomes
for a particular treatment does not mean we necessarily do not offer that treatment — our goal is to increase outcomes
reporting each year. When outcomes for a specific treatment are unavailable, we often report process measures that
have documented relationships with improved outcomes. When process measures are unavailable, we report volume
measures; a volume/outcome relationship has been demonstrated for many treatments, particularly those involving surgical
technique.
Cleveland Clinic also supports transparent public reporting of healthcare quality data and participates in the following
public reporting initiatives:
• Joint Commission Performance Measurement Initiative (www.qualitycheck.org)
• Centers for Medicare and Medicaid (CMS) Hospital Compare (www.hospitalcompare.hhs.gov)
• Leapfrog Group (www.leapfroggroup.org)
• Ohio Department of Health Service Reporting (www.odh.state.oh.us)
Our commitment to providing accurate, timely information about patient care is designed to help patients and referring
physicians make informed healthcare decisions. We hope you find these data valuable. To view all our Outcomes books,
visit Cleveland Clinic’s Quality and Patient Safety website at clevelandclinic.org/quality/outcomes.
282972A.indd 1 6/19/08 3:33:51 PM
22
Dear Colleague:
I am proud to present the 2007 Cleveland Clinic Outcomes books. These books provide information on results, volumes and innovations
related to Cleveland Clinic care. The books are designed to help you and your patients make informed decisions about treatments and
referrals.
Over the past year, we enhanced our ability to measure outcomes by reorganizing our clinical services into patient-centered institutes. Each
institute combines all the specialties and support services associated with a specific disease or organ system under a single leadership at a
single site. Institutes promote collaboration, encourage innovation and improve patient experience. They make it easier to benchmark and
collect outcomes, as well as implement data-driven changes.
Measuring and reporting outcomes reinforces our commitment to enhancing care and achieving excellence for our patients and referring
physicians. With the institutes model in place, we anticipate greater transparency and more comprehensive outcomes reporting.
Thank you for your interest in Cleveland Clinic’s Outcomes books. I hope you will continue to find them useful.
Sincerely,
Delos M. Cosgrove, MD
CEO and President
282972A.indd 2 6/19/08 3:33:53 PM

what’s insideChairman’s Letter 04
Institute Overview 05
Quality and Outcomes Measures
Dermatology 07
Plastic Surgery 08
Reconstructive Surgery 13
Surgical Quality Improvement 22
Patient Experience 25
Innovations 28
New Knowledge 30
Staff Listing 33
Contact Information 35
Institute Locations 36
Cleveland Clinic Overview 37
Online Services 37 eCleveland Clinic DrConnect MyConsult
282972A.indd 3 6/19/08 3:33:54 PM

Outcomes 2007 44
On behalf of Cleveland Clinic’s Dermatology and Plastic Surgery Institute,
we are pleased to share our 2007 Outcomes book. Our physicians
and staff are dedicated to continuously improving both the quality of
our medical, surgical and aesthetic services, and to adding value to
the patient care experiences in our practices.
Major advances in the prevention and treatment of skin cancers,
aging skin and restorative and rejuvenating plastic surgery have
created an exciting environment in dermatology and plastic surgery.
Our Institute’s refinement of microvascular surgical advances in
breast reconstruction and research in composite tissue allograft
transplants will lead the future breakthroughs in plastic and
reconstructive surgery.
We hope that the information in this Outcomes book will serve as a valuable
tool and reinforce your confidence in the quality of care our Institute
offers. We consider you a partner in the care of your patients and
will continue to improve our communications with you regarding
your patient’s diagnosis, treatment options and outcomes. Please
contact us about your experiences and let us know how we can
better serve you.
Frank A. Papay, MD, FACS
Chairman, Cleveland Clinic Dermatology and Plastic Surgery Institute
Chairman’s Letter

5 Dermatology & Plastic Surgery Institute5
Institute OverviewThe establishment of the Dermatology and Plastic Surgery Institute
provides new opportunities for innovation in clinical research, physician
education and healthcare management. Both specialties offer avenues
for cross fertilization to create new standards in state-of-the-art care
of patients requiring dermatological, plastic surgical and aesthetic
services. The integration of dermatology and plastic surgery into an
Institute will enhance the residency and fellowship programs by revealing
new discoveries from both fields. Residents and fellows will have the
opportunity to become future leaders in their fields, thanks to the institute’s
interdisciplinary approach to education, research and patient care.
The Cleveland Clinic Dermatology and Plastic Surgery Institute offers
services in several specialty areas, including clinical and cosmetic
dermatology; dermatopathology, dermatologic surgery and cutaneous
oncology; Mohs micrographic surgery and reconstruction; pediatric
dermatology; industrial and environmental dermatology; facial cosmetic
surgery; cosmetic breast surgery and breast reconstruction; body
contouring, including liposuction and plastic surgery after massive weight
loss; pediatric plastic surgery; hand surgery; microsurgery; complex wound
repair and reconstruction after cancer.
Dermatologists and/or plastic surgeons are located in 11 sites throughout
Northeast Ohio: Cleveland, Beachwood, Chagrin Falls, Independence,
Lorain, Strongsville, Solon, Westlake, Willoughby Hills, Wooster and
Lutheran Hospital.
The Department of Dermatology provides expertise in the diagnosis and
management of the full spectrum of dermatologic conditions. One of
the fastest-growing services is also one of the oldest: Mohs micrographic
surgery. Mohs micrographic surgery provides the highest cure rate
for high-risk nonmelanoma skin cancers, while sparing the maximum
amount of normal skin. Cleveland Clinic dermatologists performed
approximately 2,100 Mohs procedures in 2007 and now offer the surgery
in Independence and Beachwood, in addition to the main campus. Access
at more locations affords patients more timely treatment of skin cancer.
The department continues to meet community responsibilities by
participating actively in the Skin Cancer Screening Day and in other
activities related to National Skin Cancer Week. In addition to several
health talks and other community events, the department participated in
six free skin cancer screenings, all staffed by Cleveland Clinic Dermatology
staff, residents and physicians’ assistants.
The move to the institute model of care has created an ideal opportunity
to build synergies between Dermatology and Plastic Surgery in the
areas of aesthetic facial plastic surgery and cosmetic dermatology. This
collaboration will enable patients to obtain the best from both specialties.
For the past several years, the Department of Plastic Surgery has focused
on minimally invasive techniques in facial cosmetic surgery. This includes
alternatives to face and necklift surgery, short-scar facelifts and minimally
invasive facelift techniques. Surgeons continue to collect and objectively
measure data on these procedures, and to publish results in peer-reviewed
plastic surgery journals.
282972A.indd 5 6/19/08 3:34:04 PM

Outcomes 2007 6
The department has made significant progress in objectifying surgical
results in other areas, including cosmetic breast surgery and reconstructive
surgery for breast cancer. Cleveland Clinic plastic surgeons offer numerous
methods of breast reconstruction that can be performed either at the time
of mastectomy or as a secondary procedure. These techniques include
breast implants and expanders; pedicled transverse rectus abdominis
myocutaneous (TRAM) flaps (abdominal skin and muscle); and free-tissue
transfers, such as the deep inferior epigastric perforator (DIEP) flap. The
DIEP flap minimizes injury to the abdominal wall while providing an ideal
breast reconstruction using the patient’s own tissue. This procedure is
performed in large numbers at only a few centers in the United States.
In addition to standard body contouring techniques, including
abdominoplasty and a wide variety of liposuction techniques, the
Department of Plastic Surgery is particularly interested in plastic surgery
after significant weight loss.
The department also includes three staff surgeons with Certificates of
Added Qualifications in hand surgery and four plastic surgeons with
extensive microsurgery experience. This provides a team adept at handling
all types of traumatic, congenital and work-related hand, peripheral nerve
and other upper-extremity problems.
Finally, pediatric surgery and craniofacial surgery are especially strong
specialties in this department. The head of the Section of Pediatric Plastic
Surgery and Craniofacial Surgery has more than 15 years of experience
with these rare problems.
The Dermatology and Plastic Surgery Institute is poised for the challenges
of 2008 and beyond, with planned growth on both the main campus and
in our suburban locations.
282972A.indd 6 6/19/08 3:34:04 PM

7 Dermatology & Plastic Surgery Institute
Number of ProceduresNumber of Procedures
0
500
1000
1500
2000
2500
2003 2004 2005 2006 2007
DermatologyOne of our fastest-growing services is also one of our oldest: Mohs micrographic surgery for skin cancer. By streamlining our Mohs laboratory processes, extending surgical hours and adding the availability of Mohs surgery at our Beachwood and Independence offices, we have achieved a significant increase in the number of cases performed over the previous year. This has provided faster access to treatment for patients with skin cancer.
Taking advantage of the latest technology in UVA1 phototherapy, such as light boxes and the excimer laser, the Light Therapy Unit saw a significant increase in the number of patients served.
Yearly Number of Mohs procedures
Yearly Number of Phototherapy / Ultraviolet Light Treatments
2Number of TreatmentsNumber of Treatments
0
3000
4000
5000
6000
7000
2000
1000
2003 2004 2005 2006 2007
The Department of Dermatology continues to upgrade and improve our laser program services in order to provide one of the most comprehensive lines of laser services in Northeast Ohio. Services include treatment with the Smoothbeam laser for acne and skin contouring, the Vbeam laser for vascular lesions, the erbium and carbon dioxide lasers for skin resurfacing and lesion removal, the VersaPulse laser for the treatment of pigmented lesions, tattoos and blood vessels of the face and legs, the alexandrite and YAG lasers for hair removal and the Affirm laser for fractional nonablative skin contouring. Varicose veins and spider veins are treated with laser and/or sclerotherapy treatments.
Yearly Number of Laser Treatments
0
2000
4000
6000
8000
10000
Number of TreatmentsNumber of Treatments
2003 2004 2005 2006 2007
282972A.indd 7 6/19/08 3:34:05 PM

Outcomes 2007 8
Plastic SurgeryYearly Number and Type of Facial Cosmetic Surgeries
Yearly Number of Primary and Secondary Rhinoplasties
Yearly Number and Type of Cosmetic Breast Surgeries
20030
150
50
100
200
Number of SurgeriesNumber of Surgeries
2004 2005 2006 2007
Brow lift BlepharoplastyFacelift/Neck
Number of ProceduresNumber of Procedures
0
20
40
60
80
100
2003 2004 2005 2006 2007
SecondaryPrimary
Number of SurgeriesNumber of Surgeries
0
50
100
150
200
250Breast Augmentation MastopexyBreast Reduction
2003 2004 2005 2006 2007
282972A.indd 8 6/19/08 3:34:08 PM

9 Dermatology & Plastic Surgery Institute
Yearly Number and Type of Body Contouring Procedures
Yearly Number and Type of Breast Reconstruction Procedures
Number of ProceduresNumber of Procedures
0
50
100
150
200Lipo Trunk/Extremities Lipo Head/NeckAbdominoplasty
2003 2004 2005 2006 2007
Number of ProceduresNumber of Procedures
0
50
100
150
200
300
250
2003 2004 2005 2006 2007
Breast Recon w/ProsthesisBreast Recon w/Latissimus Dorsi FlapOncoplasty
Breast Recon w/TRAM Flap
282972A.indd 9 6/19/08 3:34:08 PM
Outcomes 2007 10
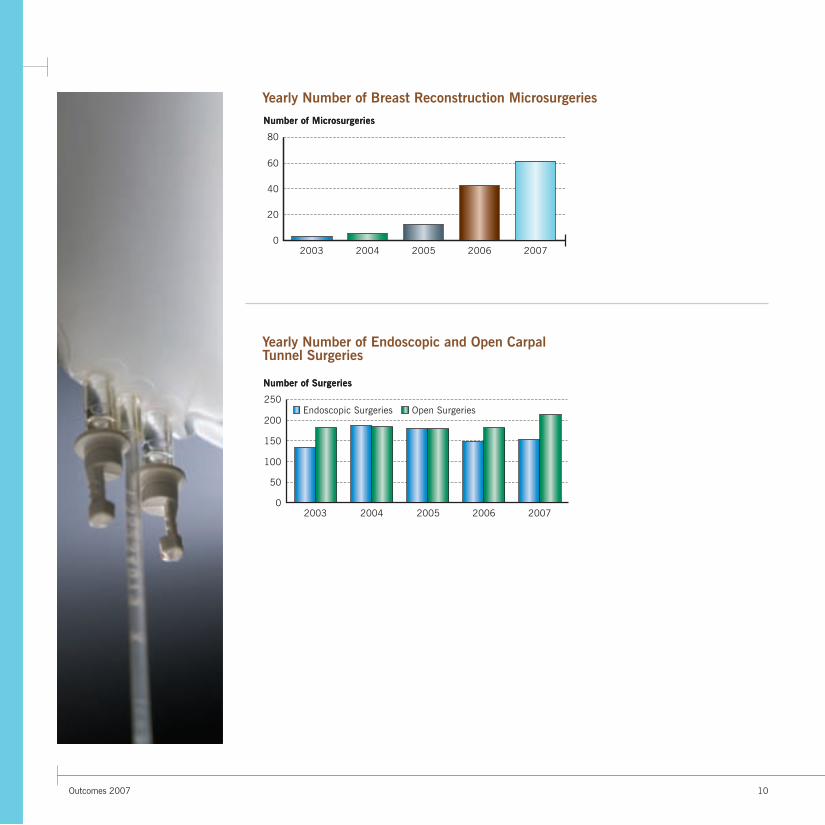
Yearly Number of Breast Reconstruction Microsurgeries
Yearly Number of Endoscopic and Open Carpal Tunnel Surgeries
Number of MicrosurgeriesNumber of Microsurgeries
0
20
40
60
80
2003 2004 2005 2006 2007
Number of SurgeriesNumber of Surgeries
0
50
100
150
200
250
2003 2004 2005 2006 2007
Open SurgeriesEndoscopic Surgeries
282972A.indd 10 6/19/08 3:34:14 PM

11 Dermatology & Plastic Surgery Institute
Percentages of Nondiabetic and Diabetic Patients Who Underwent Surgical Nerve Decompression in 2007 (N = 62)
Number and Types of Nerves Decompressed in 2007
Surgical Treatment for Peripheral NeuropathySurgical decompression of peripheral nerves has been performed on patients with both lower and upper-extremity peripheral neuropathy and in diabetic as well as nondiabetic patients. Treated nerves in the lower extremities included the common peroneal nerve, the deep peroneal nerve, the superficial peroneal nerve and the posterior tibial nerve. In the upper extremities, treated nerves included the ulnar and median nerves. Clinical evaluation and preoperative quantitative sensory testing were used to identify patients who would benefit from surgery.
Most patients in the nondiabetic group had lower-extremity neuropathy of undetermined etiology or secondary to injury.
A total of 224 nerves were surgically decompressed in the 62 patients.
11
N = 62
48% Diabetic48% Diabetic52% Nondiabetic52% Nondiabetic
Number of NervesNumber of Nerves
0
20
40
60
80
SuperficialPeroneal
Nerve
PosteriorTibial Nerve
UlnarNerve
MedianNerve
DeepPeroneal
Nerve
CommonPeroneal
Nerve
282972A.indd 11 6/19/08 3:34:14 PM

Outcomes 2007 12
Improvements in Muscle Strength
Clinical Outcomes (N = 62)
The clinical outcome was satisfactory in 86% of patients over a mean duration of 8.3 months. Clinical outcome was determined on the basis of the level of postoperative pain, the use of neuropathic and narcotic pain medications, the time to return of sensation, improvement in walking distance and the time to return to work.
Mean Muscle Power
1Time (months)
0
4
2
3
5
1
6
2
Extensor Hallucis Longus
Extensor Hallucis Brevis
N = 62
14% Fair14% Fair
34% Good34% Good
52% Excellent52% Excellent
Following surgical decompression of the common peroneal nerve at the neck of the fibula, improvements were seen in the muscle power of the extensor hallucis longus and the extensor hallucis brevis.
282972A.indd 12 6/19/08 3:34:16 PM

13 Dermatology & Plastic Surgery Institute
Reconstructive Surgery
Success/Failure Rates for DIEP
Yearly Number of DIEP Flap Reconstruction Surgeries
Microsurgical Breast Reconstruction: The Deep Inferior Epigastric Perforator FlapBreast cancer patients who need mastectomy as part of their treatment have several options for reconstruction of their missing breast tissue. The two most common and widely known methods are (1) placement of implants and (2) reconstruction with a TRAM flap. The TRAM flap, which makes use of the patient’s own tissue, requires the use of abdominal fat tissue and muscle.
Recent advances in breast reconstruction include a variation of the TRAM operation that allows for preservation of the rectus abdominis muscle. This technique is called DIEP (for deep inferior epigastric perforator) free-flap reconstruction. It involves meticulous dissection of the vessels within the rectus abdominis muscle from their distal perforation through the rectus fascia and all the way down to their proximal pedicle off the external iliac artery and vein. Once these vessels are identified and isolated, they are transected and re-anastomosed to the internal mammary or thoracodorsal vessels. This anastomosis requires a microsurgical operation to re-establish perfusion to the flap. To complete the reconstruction, the flap is secured and tailored to form a new reconstructed breast. Since this procedure is dedicated to the preservation of muscle, most patients experience less discomfort than do patients who undergo procedures that involve taking the rectus muscle.
0
40
20
60
80
100
Success Failure
PercentPercent
Number of ReconstructionsNumber of Reconstructions
0
20
40
60
80
100
2005 2006 2007
282972A.indd 13 6/19/08 3:34:17 PM

Outcomes 2007 14
Figure 1:
A. Preoperative DIEP flaps, left and right breasts, left breast side view.
B. Postoperative bilateral mastectomies immediately reconstructed with DIEP free flaps on both sides, left breast side view.
C. Preoperative DIEP flap, left breast, and preoperative mastopexy, right breast, front view.
D. Postoperative DIEP flap, left breast with nipple reconstruction, and postoperative mastopexy, right breast, front view.
E. Preoperative DIEP flap, front view, torso.
F. Postoperative DIEP flap, front view, torso.
A B
D
FE
C
282972A.indd 14 6/19/08 3:34:19 PM

15 Dermatology & Plastic Surgery Institute
Figure 2:
A. Preoperative bilateral mastectomies, right breast side view with short scar from a lumpectomy.
B. Postoperative nipple-sparing mastectomies reconstructed with implants, right breast side view.
C. Preoperative bilateral mastectomies, front view.
D. Postoperative nipple-sparing mastectomies reconstructed with implants, front view.
Breast Reconstruction in Nipple-Sparing Mastectomy During the past decade, the traditional modified radical mastectomy has evolved to become skin-sparing mastectomy. In radical modified mastectomy, the surgeon removes the cancerous tissue in the breast along with the remainder of the breast tissue and nipple areola complex through an incision around the nipple. This procedure has been further refined to become what is known as skin-sparing mastectomy.
In general, there are two major options for breast reconstruction following a mastectomy: autologous tissue reconstruction and nonautologous reconstruction. In autologous reconstruction, the breast mount is reconstructed by using the patient’s own tissue. The most common tissue used for this purpose is adipose (fat) tissue taken from the abdomen. In the nonautologous procedure, the reconstruction is accomplished by using a tissue expander and implant material. In the current technique, the plastic surgery team at Cleveland Clinic has employed two-stage reconstruction by using tissue expander placement immediately after the mastectomy followed by exchange of the expander to an implant material of choice. At times, a single-stage reconstruction after a mastectomy can be attempted by direct placement of the implant.
The Department of Plastic Surgery at Cleveland Clinic, in conjunction with the Breast Center, is conducting a review of results based on our seven-year experience in performing breast reconstruction via nipple-sparing mastectomy in 137 patients. For this institutional review board–approved study, charts were reviewed and patients were contacted by letter and asked to complete mail-in questionnaires. Of the 65 patients who responded, 32 said that they would definitely undergo the procedure again if indicated.
A B
C D
282972A.indd 15 6/19/08 3:34:21 PM

Outcomes 2007 16
Neck Correction ProceduresCultural shifts during the past decade have changed some paradigms in plastic surgery. Emerging trends show that patients want shorter recovery times, less morbidity and more immediate results. It’s about looking younger faster by targeting specific areas. Based on our experience, the neck has become a new area of concern. A number of alternative procedures to traditional facelift surgery are available, including minimally invasive facelifts and neck lifts without incisions in the front or back of the ear. More and more patients are willing to accept more subtle changes rather than undergoing invasive procedures. In elderly patients, neck correction is providing significant neckline improvement when it is performed in the appropriate surgical candidates. Neck correction is associated with less morbidity than is traditional facelift surgery.
Types of Neck Correction Procedures, 1997-2007 (N = 42)Number of ProceduresNumber of Procedures
0
10
30
20
Anterior Lipectomyand Platysmaplasty
Direct Excision SubmentalLiposuction
282972A.indd 16 6/19/08 3:34:21 PM

17 Dermatology & Plastic Surgery Institute
Submental Liposuction The ideal candidate for submental liposuction is a patient younger than 40 years who has good skin elasticity, mild skin excess and a mild to moderate amount of fat in the submental and submandibular areas. A blunt cannula is generally inserted through a very small and well-concealed submental incision. Superficial fat is then suctioned, and the skin is allowed to re-drape over the new and improved neck contour.
Figure 3:
A. Preoperative front view of a 35- year-old woman with a moderate amount of fat in the submental area and a weak chin.
B. Postoperative front view.
C. Preoperative profile view before submental liposuction and chin augmentation.
D. Postoperative profile view.
A B
DC
282972A.indd 17 6/19/08 3:34:25 PM
Outcomes 2007 18
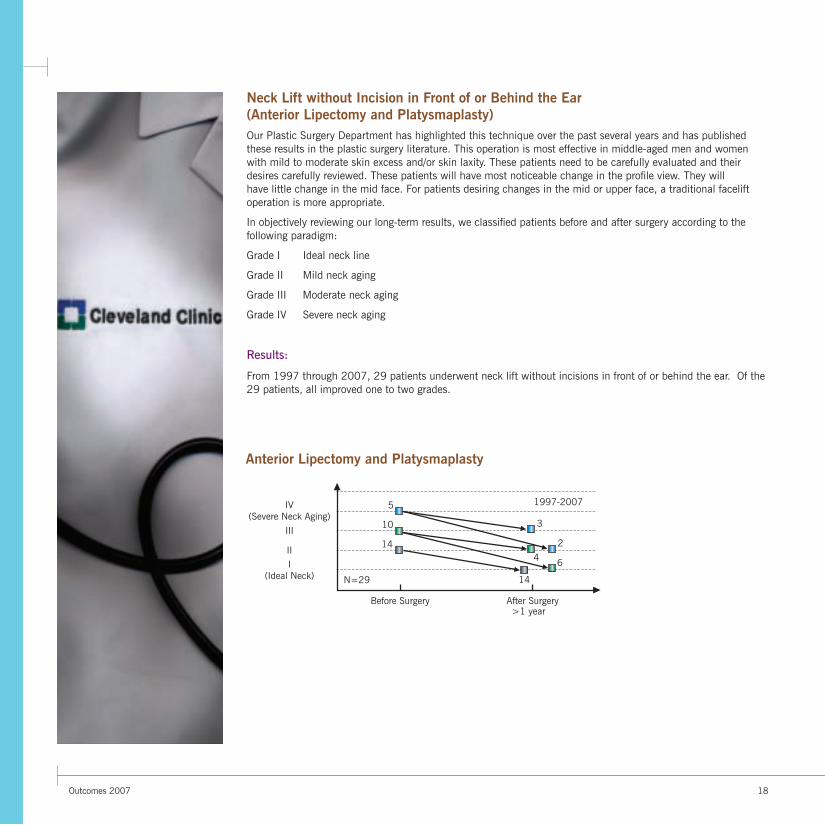
Neck Lift without Incision in Front of or Behind the Ear (Anterior Lipectomy and Platysmaplasty)Our Plastic Surgery Department has highlighted this technique over the past several years and has published these results in the plastic surgery literature. This operation is most effective in middle-aged men and women with mild to moderate skin excess and/or skin laxity. These patients need to be carefully evaluated and their desires carefully reviewed. These patients will have most noticeable change in the profile view. They will have little change in the mid face. For patients desiring changes in the mid or upper face, a traditional facelift operation is more appropriate.
In objectively reviewing our long-term results, we classified patients before and after surgery according to the following paradigm:
Grade I Ideal neck line
Grade II Mild neck aging
Grade III Moderate neck aging
Grade IV Severe neck aging
Results:
From 1997 through 2007, 29 patients underwent neck lift without incisions in front of or behind the ear. Of the 29 patients, all improved one to two grades.
5
10
14
3
24 6
14N=29
I(Ideal Neck)
IV(Severe Neck Aging)
II
III
Before Surgery After Surgery
1997-2007
Anterior Lipectomy & Platysmaplasty
Anterior Lipectomy and Platysmaplasty
>1 year

19 Dermatology & Plastic Surgery Institute
Figure 4:
A. Preoperative front view of a 45-year-old woman with a grade II neck deformity.
B. Postoperative front view.
C. Preoperative profile view before anterior lipectomy and platysmaplasty.
D. Postoperative profile view.
A B
C D
282972A.indd 19 6/19/08 3:34:33 PM

Outcomes 2007 20
Figure 5:
A. Preoperative front view of a 73-year-old woman with a grade III neck deformity.
B. Postoperative front view.
C. Preoperative profile view before anterior lipectomy and platysmaplasty.
D. Postoperative profile view.
Complications:
Complications following neck lift without preauricular incision have been minor. They have included occasional neck irregularities that resolve with time. One patient ultimately underwent traditional facelift surgery.
A B
C D
282972A.indd 20 6/19/08 3:34:37 PM

21 Dermatology & Plastic Surgery Institute
Figure 5:
A. Preoperative front view of a 73-year-old woman with a grade III neck deformity.
B. Postoperative front view.
C. Preoperative profile view before anterior lipectomy and platysmaplasty.
D. Postoperative profile view.
A B
C D
Direct Excision with Z-plastyIn elderly men and women, the direct excision of neck skin and Z-plasty significantly improves the neck contour, especially in the profile, with significantly less downtime and surgical risk when compared to traditional facelift surgery. In addition, those patients with a significant amount of skin excess will obtain an even better neck contour than those patients undergoing traditional facelift surgery because the skin excision will be in the area where laxity is the greatest.
The tradeoff is a scar in the neck area. While the scar generally heals well, its permanence must be fully discussed with the patient before surgery. It is most helpful to show these patients before-and-after photographs, including images of the neck scar itself.
This operation generally is performed in men and women who are 70 or older. It is also an operation used in patients following massive weight loss.
Figure 6:
A. Preoperative front view of a 74-year-old man with marked skin excess in the submental region.
B. Postoperative front view.
C. Preoperative profile view before neck lift surgery with neck skin excision.
D. Postoperative profile view.
282972A.indd 21 6/19/08 3:34:41 PM

Outcomes 2007 22
Surgical Quality ImprovementSurgical Care Improvement Program (SCIP)SCIP is a national campaign aimed at reducing surgical complications by 25 percent by the year 2010. SCIP is sponsored by the Centers for Medicare and Medicaid Services (CMS) in collaboration with a number of other national partners serving on the steering committee, including the American Hospital Association (AHA), Centers for Disease Control and Prevention (CDC), Institute for Healthcare Improvement (IHI), The Joint Commission and others. Cleveland Clinic is committed to improving the care of surgical patients and participates in SCIP. A multidisciplinary team including the Surgery Institute, Anesthesiology Institute, Infectious Disease Department, Nursing Institute, and Quality and Patient Safety Institute works together to ensure that our surgical patients receive appropriate care.
Cleveland ClinicNational Average*Top Hospitals*
Percent
0
20
100
40
60
80
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Appropriate Prophylactic Antibiotic Selection 2007
* Source: United States Department of Health and Human Services, Hospital Compare Most current reported discharges July 2006 to June 2007. “Top Hospitals” represent the top 10 percent of reporting hospitals nationwide. National average of all reporting hospitals in the United States.
Percent
0
20
100
40
60
80
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Cleveland ClinicNational Average*Top Hospitals*
Appropriate Preoperative Prophylactic Antibiotic Timing 2007
* Source: United States Department of Health and Human Services, Hospital Compare Most current reported discharges July 2006 to June 2007. “Top Hospitals” represent the top 10 percent of reporting hospitals nationwide. National average of all reporting hospitals in the United States.
282972A.indd 22 6/19/08 3:34:42 PM

Dermatology & Plastic Surgery Institute23
Cleveland ClinicNational Average*Top Hospitals*
Percent
0
20
100
40
60
80
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Recommended Venous Thromboembolism Prophylaxis Received by Patient 2007
Cleveland ClinicNational Average*Top Hospitals*
Percent
0
20
100
40
60
80
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Prophylactic Antibiotics Discontinued within 24 Hours After Surgery 2007
* Source: United States Department of Health and Human Services, Hospital Compare Most current reported discharges July 2006 to June 2007. “Top Hospitals” represent the top 10 percent of reporting hospitals nationwide. National average of all reporting hospitals in the United States.
* Source: United States Department of Health and Human Services, Hospital Compare Most current reported discharges January 2007 to June 2007. “Top Hospitals” represent the top 10 percent of reporting hospitals nationwide. National average of all reporting hospitals in the United States.
282972A.indd 23 6/19/08 3:34:43 PM
Outcomes 2007 24
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Percent
0
20
100
40
60
80
Cleveland Clinic*
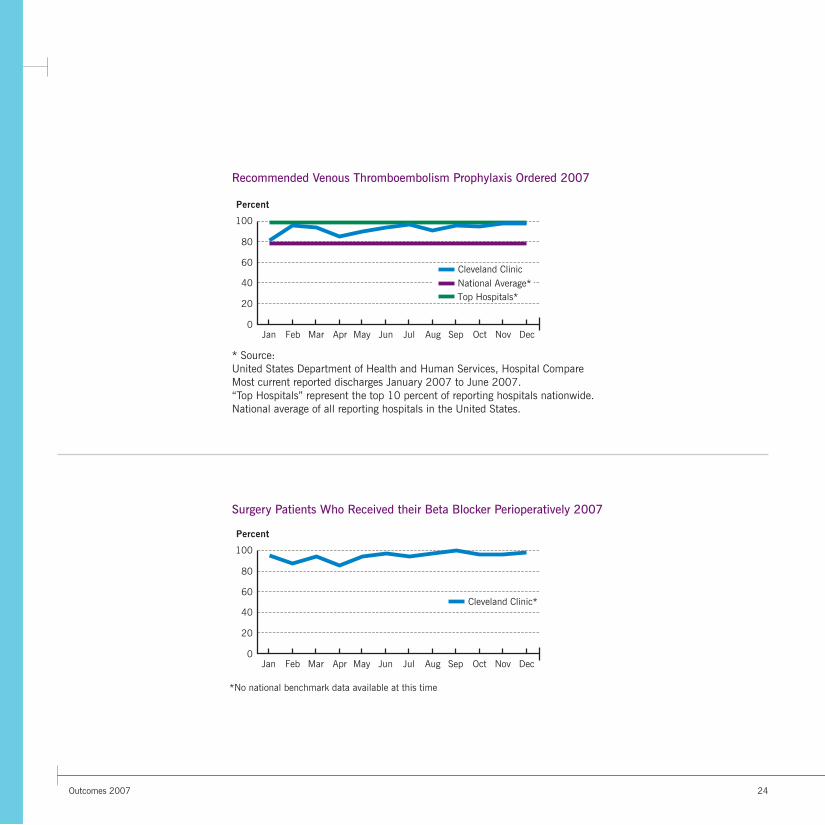
Recommended Venous Thromboembolism Prophylaxis Ordered 2007
Surgery Patients Who Received their Beta Blocker Perioperatively 2007
* Source: United States Department of Health and Human Services, Hospital Compare Most current reported discharges January 2007 to June 2007. “Top Hospitals” represent the top 10 percent of reporting hospitals nationwide. National average of all reporting hospitals in the United States.
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Cleveland ClinicNational Average*Top Hospitals*
Percent
0
20
100
40
60
80
*No national benchmark data available at this time
282972A.indd 24 6/19/08 3:34:43 PM

25 Dermatology & Plastic Surgery Institute
Overall Rating of Care 2007
Overall Rating of Provider Care 2007
Outpatient - Dermatology and Plastic Surgery InstituteWe ask our patients about their experiences and satisfaction with the services provided by our staff. Although our patients are already indicating we provide excellent care, we are committed to continuous improvement.
Patient Experience
Excellent
PercentPercent
0
100
80
60
40
20
Very Good Good Fair Poor
N=1616
Excellent
PercentPercent
0
100
80
60
40
20
Very Good Good Fair Poor
N=1616
282972A.indd 25 6/19/08 3:34:43 PM

Outcomes 2007 26
Would Recommend Provider 2007
ExtremelyLikely
PercentPercent
0
100
80
60
40
20
VeryLikely
SomewhatLikely
SomewhatUnlikely
VeryUnlikely
N=1583
282972A.indd 26 6/19/08 3:34:44 PM

27 Dermatology & Plastic Surgery Institute
Face Forward If it weren’t for baby pictures, 3-year-old Grace Lesnak would never know she was born with a large hemangioma that marred her otherwise perfect face. Thanks to laser treatments at Cleveland Clinic, the red strawberry was gone before she took her first step.
A dermatologist in her hometown of Ravenna, Ohio, referred Grace, then just 4 months old, to Allison Vidimos, RPh, MD, chair of the Der-matology Department. Dr. Vidimos immediately began a series of treatments, scheduled one month apart, in Cleveland Clinic’s state-of-the-art laser unit, which rendered the large birthmark a faint shadow.
Grace’s parents couldn’t be happier, referring to Dr. Vidimos as an angel. “Being a kid is tough enough. We didn’t want a birthmark to make it even harder,” her mother says.
282972A.indd 27 6/19/08 3:34:49 PM

Outcomes 2007 28
InnovationsDermatologyPhotodynamic therapy (PDT) using the Bluelight for treatment of precancerous actinic keratoses, acne and skin rejuvenation is available at main campus and the Independence Family Health Center. Studies are under way to investigate PDT for the treatment of psoriasis and cutaneous T cell lymphoma.
The laser unit offers state-of-the-art care with a dozen ablative and nonablative lasers for treatment of scars and wrinkles, tattoo removal, treatment of vascular lesions (e.g., port wine stain birthmarks and hemangiomas), hair removal and treatment of telangiectasias of the face and legs and pigmented lesion removal. The Affirm Laser provides the newest fractionated laser technology to treat skin contour irregularities.
The Dermatopathology Reading Room was completed by July 2007. The 18-headed microscope, computer access to Epic and the Internet and two projection screens have dramatically improved the rapidity and quality of slide interpretations, as well as the education of the fellows and residents. The dermatopathologist has the opportunity to examine lesions or rashes on the patient prior to receiving the specimen the following day.
Additionally, some new clinical studies that are occurring in Dermatology include:
• a pilot study exploring the rejuvenation of the lower eyelid using a combination of two hyaluronic acid fillers
• determination of ideal aminolevulinic acid exposure time for photodynamic therapy of actinic keratoses
• uveal melanoma and atypical nevus syndrome
• efficacy of subcutaneous phosphatidylcholine and deoxycholate injections for localized fat removal
Plastic SurgeryIn 2006 the Department of Plastic Surgery significantly increased its microsurgical expertise by recruiting two additional microsurgeons to the team. With these additions, the department has rapidly increased the numbers of microsurgical reconstructive procedures for breast cancer using the deep inferior gastric perforator (DIEP) flap. More than 70 patients underwent this procedure in 2007.
The DIEP flap minimizes the damage to the abdominal wall caused by other autogenous (the patient’s own skin and subcutaneous tissue) breast reconstruction techniques. In the more widely used and traditional transverse rectus abdominis myocutaneous (TRAM) operation, one and occasionally two muscles of the abdomen are used to reconstruct the breast. While this can be done consistently and effectively, it can result in hernias, bulges and, especially when two muscles are used, significant weakness of the abdomen. These patients are then unable to perform sit-ups and other vigorous activities. The DIEP flap may prove to minimize these adverse effects while affording excellent and natural autogenous reconstruction.
In concert with the Department of General Surgery, the Department of Plastic Surgery has established an ongoing protocol for multidisciplinary treatment of breast defects following conservative resections for breast cancer (partial mastectomy defects). These procedures are done at the time of the general surgeon’s excision of the breast tumor when the general surgeon feels that a more complex reconstruction would be advisable to minimize deformity resulting from partial mastectomy resection.
The facelift operation is the mainstay for the correction of facial aging. However, there is clearly a subset of patients who would benefit from a lesser procedure. Anterior lipectomy and platysmaplasty is an operation that has been popularized by our plastic surgery staff. This procedure has recently been published by our team in the plastic surgery literature. The operation results in improvement predominantly in the profile with little change in the mid face. A variety of minimally invasive facelifts have been added to our plastic surgery armamentarium. These techniques are currently undergoing rigorous outcomes analyses to assess their duration of efficacy, complications and patient satisfaction.
282972A.indd 28 6/19/08 3:34:49 PM

Dermatology & Plastic Surgery Institute29
Ongoing protocols are in place in a variety of aesthetic surgery procedures including brow lift, abdominoplasty, facelift, breast augmentation and breast reduction surgery to minimize postoperative pain, nausea and vomiting. This involves the use of a self-administering, continuous infusion catheter placed at the time of surgery. Through this continuous infusion catheter a long-acting, local anesthetic is used to minimize postoperative pain. As numbers of patients entered into our outcomes study increase, significant reduction in pain has been seen in breast reduction and abdominoplasty patients.
Dermatology and Plastic Surgery AnesthesiologyAnesthesiologists of the Section of Ambulatory Anesthesia improved patient safety by introducing the new “glide scope” technique to supplement conventional fiberoptic methods for difficult intubations. They also innovated their practice by employing new ultrasound-guidance technology for nerve block placement in upper extremity and other plastic surgery procedures.
In a critically important research endeavor, this section’s anesthesiologists are conducting a clinical trial to determine if adding regional anesthesia to traditional general anesthesia techniques can decrease breast cancer recurrence after mastectomy.
With this two-year laboratory and cadaver dissection behind us, we are now approaching the time when we feel that the team is ready and thoroughly trained for this highly controversial transplant to become a reality.
1) Optimizing nerve conduit scaffolds for the repair of segmental nerve defects
2) Composite tissue allograft transplantation without lifelong immunosuppression
282972A.indd 29 6/19/08 3:34:49 PM
In 2006, the Department of Plastic Surgery in collaboration with Synthes Maxillofacial completed a large animal study investigating the long-term results (1 year), the histology and the biomechanical evaluation of the use of Norian and Norian Fast-Set Putty (Synthes Maxillofacial) as an alternative to bone grafts in a full-thickness skull defect. These bone substitutes were compared with autogenous (the animal’s own) bone graft that was grafted to the opposite side of the skull. This long-term biomechanical analysis is the first of its kind in the surgical literature. This paper has been accepted for publication in the Journal of Plastic and Reconstructive Surgery. Ongoing cadaver biomechanical tests of a variety of bone substitutes were proceeding in 2007, again supported by a grant from Synthes Maxillofacial.
Our face transplant project led by Maria Siemionow, MD began in our plastic surgery laboratory where a variety of transplants were performed on small animals. This included total hind limb transplantation and ultimately transplantation of the skin and soft tissue of the face from one unrelated animal to another. A variety of immunosuppressive techniques also developed in our laboratory were used for long-term maintenance of the flap. With these improvements in immunotherapy and surgical transplantation techniques, cadaver dissection was the second phase of this project. A large number of cadaver dissections were done to prove the feasibility of this technique. This included vascular injections using barium and similar materials.
Additionally, Dr. Siemionow has been awarded a grant from the Armed Forces Institute for Regenerative Medicine (AFIRM) for the following studies:
,

Outcomes 2007 30
New KnowledgeJournal ArticlesAjani G, Sato N, Mack JA, Maytin EV. Cellular responses to disruption of the permeability barrier in a three-dimensional organotypic epidermal model. Exp Cell Res. 2007 Aug 15;313(14):3005-3015.
Amado A, Jacob SE. Dermatitis de contacto por alimentos [Contact dermatitis to foods] [Spanish]. Actas Dermosifiliogr. 2007 Sep;98(7): 452-458.
Amado A, Sood A, Taylor JS. Contact allergy to lidocaine: a report of sixteen cases. Dermatitis. 2007 Dec;18(4):215-220.
Amado A, Jacob SE. Letter: benzyl alcohol preserved saline used to dilute injectables poses a risk of contact dermatitis in fragrance-sensitive patients. Dermatol Surg. 2007 Nov;33(11):1396-1397.
Arslan E, Klimczak A, Siemionow M. Chimerism induction in vascularized bone marrow transplants augmented with bone marrow cells. Microsurgery. 2007;27(3):190-199.
Ausmus GG, Piliang MP, Bergfeld WF, Goldblum JR. Soft-tissue perineurioma in a 20-year-old patient with neurofibromatosis type 1 (NF1): report of a case and review of the literature. J Cutan Pathol. 2007 Sep;34(9):726-730.
Cevasco NC, Bergfeld WF, Remzi BK, Ramirez de Knott H. A case-series of 29 patients with lichen planopilaris: the Cleveland Clinic Foundation experience on evaluation, diagnosis, and treatment. J Am Acad Dermatol. 2007 Jul;57(1):47-53.
Chandrasekharan UM, Siemionow M, Unsal M, Yang L, Poptic E, Bohn J, Ozer K, Zhou Z, Howe PH, Penn M, DiCorleto PE. Tumor necrosis factor alpha (TNF-alpha) receptor-II is required for TNF-alpha-induced leukocyte-endothelial interaction in vivo. Blood. 2007 Mar 1;109(5):1938-1944.
Fernandez-Faith E, McDonnell J. Cutaneous sarcoidosis: differential diagnosis. Clin Dermatol. 2007 May;25(3):276-287.
Gonzalez AM, Yazici I, Kusza K, Siemionow M. Effects of fresh versus banked blood transfusions on microcirculatory hemodynamics and tissue oxygenation in the rat cremaster model. Surgery. 2007 May;141(5):630-639.
Helfrich YR, Yu L, Ofori A, Hamilton TA, Lambert J, King A, Voorhees JJ, Kang S. Effect of smoking on aging of photoprotected skin: evidence gathered using a new photonumeric scale. Arch Dermatol. 2007 Mar;143(3):397-402.
Imanguli MM, Karai LJ, Shanti RM, Stewart DM, Brahim JS. Myofibroblastic tumor of the lower lip in a patient with X-linked hypogammaglobulinemia and isolated growth hormone deficiency: a case report. J Oral Maxillofac Surg. 2007 Jun;65(6):1219-1222.
Jones S, Kress D. Treatment of molluscum contagiosum and herpes simplex virus cutaneous infections. Cutis. 2007 Apr;79(4 Suppl):11-17.
Kaplan JL, Hammert WE, Zins JE. Lawsuits against plastic surgeons: Does locale affect incidence of claims? Can J Plast Surg. 2007 Autumn;15(3):155-157.
Klimczak A, Unal S, Jankowska A, Coburn C, Siemionow M. Donor-origin cell engraftment after intraosseous or intravenous bone marrow transplantation in a rat model. Bone Marrow Transplant. 2007 Aug;40(4):373-380.
Knott PD, Zins JE, Banbury J, Djohan R, Yetman RJ, Papay F. A comparison of dermabond tissue adhesive and sutures in the primary repair of the congenital cleft lip. Ann Plast Surg. 2007 Feb;58(2):121-125.
Laungani AG, McDonnell J, Bergfeld WF, McMahon JT. What is your diagnosis? Uncombable hair syndrome (pili trianguli et canaliculi). Cutis. 2007 Apr;79(4):272, 291-292.
Meneghetti SC, Morgan MM, Fritz J, Borkowski RG, Djohan R, Zins JE. Operating room fires: optimizing safety. Plast Reconstr Surg. 2007 Nov;120(6):1701-1708.
Morrison C, Zins J. An alternative approach to brow lift fixation: temporoparietal fascia, galeal, and periosteal imbrication. Plast Reconstr Surg. 2007 Oct;120(5):1433-1434.
Olsen EA, Whiting D, Bergfeld W, Miller J, Hordinsky M, Wanser R, Zhang P, Kohut B. A multicenter, randomized, placebo-controlled, double-blind clinical trial of a novel formulation of 5% minoxidil topical foam versus placebo in the treatment of androgenetic alopecia in men. J Am Acad Dermatol. 2007 Nov;57(5):767-774.
Rietschel RL, Warshaw EM, Sasseville D, Fowler JF Jr, DeLeo VA, Belsito DV, Taylor JS, Storrs FJ, Mathias CG, Maibach HI, Marks JG Jr, Zug KA, Pratt M. Sensitivity of petrolatum and aqueous vehicles for detecting allergy to imidazolidinylurea, diazolidinylurea, and DMDM hydantoin: a retrospective analysis from the North American Contact Dermatitis Group. Dermatitis. 2007 Sep;18(3):155-162.
Rietschel RL, Warshaw EM, Sasseville D, Fowler JF, DeLeo VA, Belsito DV, Taylor JS, Storrs FJ, Mathias CGT, Maibach HI, Marks JG, Zug KA, Pratt M. Common contact allergens associated with eyelid dermatitis: data from the North American Contact Dermatitis Group 2003-2004 study period. Dermatitis. 2007 Jun;18(2):78-81.
Sato N, Moore BW, Keevey S, Drazba JA, Hasan T, Maytin EV. Vitamin D enhances ALA-induced protoporphyrin IX production and photodynamic cell death in 3-D organotypic cultures of keratinocytes. J Invest Dermatol. 2007 Apr;127(4):925-934.
282972A.indd 30 6/19/08 3:34:49 PM

Dermatology & Plastic Surgery Institute31
Sellheyer K, Krahl D. Response to letter to the editor regarding Hidradenitis suppurativa is acne inversa. Int J Dermatol. 2007 Mar;46(3):330-332.
Sellheyer K. Mechanisms of laser hair removal: could persistent photoepilation induce vitiligo or defects in wound repair? Dermatol Surg. 2007 Sep;33(9):1055-1065.
Siemionow M, Nasir S. Chimerism and bone marrow based therapies in transplantation. Microsurgery. 2007;27(5):510-521.
Siemionow M, Composite tissue allograft transplants and nonhuman primates. Transplantation. 2007 Jan 27;83(2):242.
Siemionow M, Agaoglu G. Tissue transplantation in plastic surgery. Clin Plast Surg. 2007 Apr;34(2):251-269.
Siemionow M, Bramstedt KA, Kodish E. Ethical issues in face transplantation. Current Opinion in Organ Transplantation. 2007 Apr;12(2):193-197.
Siemionow M, Sari A, Demir Y. Effect of early nerve release on the progression of neuropathy in diabetic rats. Ann Plast Surg. 2007 Jul;59(1):102-108.
Siemionow M, Agaoglu G, Hoffmann R. Anatomic characteristics of a fascia and its bands overlying the ulnar nerve in the proximal forearm: a cadaver study. J Hand Surg [Am]. 2007 Jun;32(3):302-307.
Siemionow M, Bozkurt M, Kulahci Y. Current status of composite tissue allotransplantation. Handchir Mikrochir Plast Chir. 2007 Jun;39(3):145-155.
Somani N, Martinka M, Crawford RI, Dutz JP, Rivers JK. Treatment of atypical nevi with imiquimod 5% cream. Arch Dermatol. 2007 Mar;143(3):379-385.
Stoller JK, Berkowitz E, Bailin PL. Physician management and leadership education at the Cleveland Clinic Foundation: program impact and experience over 14 years. J Med Pract Manage. 2007 Jan;22(4):237-242.
Trost LB, Bergfeld WF. Reply [Iron and hair loss in women; what is deficiency? This is the real question!]. J Am Acad Dermatol. 2007 Mar;56(3):519.
Warshaw EM, Ahmed RL, Belsito DV, DeLeo VA, Fowler JF Jr, Maibach HI, Marks JG Jr, Mathias CGT, Pratt MD, Rietschel RL, Sasseville D, Storrs FJ, Taylor JS, Zug KA. Contact dermatitis of the hands: cross-sectional analyses of North American Contact Dermatitis Group Data, 1994-2004. J Am Acad Dermatol. 2007 Aug;57(2):301-314.
Warshaw EM, Schram SE, Belsito DV, DeLeo VA, Fowler JF Jr, Maibach HI, Marks JG Jr, Mathias CGT, Pratt MD, Rietschel RL, Sasseville D, Storrs FJ, Taylor JS, Zug KA. Shoe allergens: retrospective analysis of cross-sectional data from the North American Contact Dermatitis group, 2001-2004. Dermatitis. 2007 Dec;18(4):191-202.
Yazici I, Carnevale K, Klimczak A, Siemionow M. A new rat model of maxilla allotransplantation. Ann Plast Surg. 2007 Mar;58(3):338-344.
Zins JE, Moreira-Gonzalez A, Papay FA. Use of calcium-based bone cements in the repair of large, full-thickness cranial defects: a caution. Plast Reconstr Surg. 2007 Oct;120(5):1332-1342.
Zins JE. Intraosseous “hemangiomas” are malformations and not tumors: Reply. Plast Reconstr Surg. 2007;119(6):1950.
Book ChaptersBergfeld WF, Elston DM. Cicatricial alopecia diagnosis and therapeutic options. In: Roenigk RK, Ratz JL, Roenigk HH Jr, eds. Roenigk’s dermatologic surgery: current techniques in procedural dermatology. 3rd ed. New York, NY: Informa Healthcare; 2007:451-462.
Galloway T, Thornton S, Ratz JL, Wheeland RG, Bailin P. Mohs micrographic surgery. In: Roenigk RK, Ratz JL, Roenigk HH Jr, eds. Roenigk’s dermatologic surgery: current techniques in procedural dermatology. 3rd ed. New York, NY: Informa Healthcare; 2007: 385-393.
Meine JG, Moosally AJ. The face (forehead, cheeks, and chin). In: Roenigk RK, Ratz JL, Roenigk HH Jr, eds. Roenigk’s dermatologic surgery: current techniques in procedural dermatology. 3rd ed. New York, NY: Informa Healthcare; 2007:239-246.
Moosally AJ, McGillis T. The neck. In: Roenigk RK, Ratz JL, Roenigk HH Jr, eds. Roenigk’s dermatologic surgery: current techniques in procedural dermatology. 3rd ed. New York, NY: Informa Healthcare; 2007:247-253.
Poblete-Lopez C, Vidimos AT. The foot. In: Roenigk RK, Ratz JL, Roenigk HH Jr, eds. Roenigk’s dermatologic surgery: current techniques in procedural dermatology. 3rd ed. New York, NY: Informa Healthcare; 2007:271-279.
Ratz JL, Kaye JJ, Yetman RJ. The hand. In: Roenigk RK, Ratz JL, Roenigk HH Jr, eds. Roenigk’s dermatologic surgery: current techniques in procedural dermatology. 3rd ed. New York, NY: Informa Healthcare; 2007:261-269.
282972A.indd 31 6/19/08 3:34:50 PM

Outcomes 2007 32
Dermatology and Plastic Surgery AnesthesiologyGan TJ, Meyer TA, Apfel CC, Chung F, Davis PJ, Habib AS, Hooper VD, Kovac AL, Kranke P, Myles P, Philip BK, Samsa G, Sessler DI, Temo J, Tramer MR, Vander Kolk C, Watcha M. Society for Ambulatory Anesthesia guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2007 Dec;105(6):1615-1628.
Maurer WG. Ambulatory anesthesia: whither thou goest. Anesth Analg. 2007 May;104(5):1299-1300.
Roizen MF, Ellis J, Mantha S, Foss J. Perioperative anesthetic considerations in noncardiac surgery for those at high risk of cardiovascular disease. In: Topol EJ, ed. Textbook of cardiovascular medicine. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:721-735.
Siemionow M, Kulahci Y. Experimental approaches to composite tissue allograft transplants. In: Lanzetta M, Dubernard JM, Petruzzo P, eds. Hand transplantation. New York, NY: Springer; 2007:61-77.
Siemionow M, Kulahci Y, Agaoglu G. Diabetic neuropathy: Pathogenesis and treatment. In: Qureshi GA, Parvez SH, eds. Oxidative stress and neurodegenerative disorders. Boston, MA: Elsevier; 2007:543-579.
Taylor JS. Contact dermatitis and related disorders. In: Dale DC, Federman DD, eds. ACP medicine. 3rd ed. New York, NY: WebMD; 2007:481-494.
Thornton S, Galloway T, Bailin P. Laser treatment of vascular lesions. In: Roenigk RK, Ratz JL, Roenigk HH Jr, eds. Roenigk’sRoenigk’s dermatologic surgery: current techniques in procedural dermatology. 3rd ed. New York, NY: Informa Healthcare; 2007:671-676.
282972A.indd 32 6/19/08 3:34:50 PM

Dermatology & Plastic Surgery Institute33
Staff ListingDermatology and Plastic Surgery Institute Frank A. Papay, MD, FACS, FAAP, Chairman
Department of Dermatology Allison T. Vidimos, RPh, MD, Chair
Quality Review Officer Jon G. Meine, MD
Section of Clinical Dermatology Kenneth J. Tomecki, MD, Vice Chair Wilma F. Bergfeld, MD, FACP Jacob W. Dijkstra, MD David Hamrock, MD Edward V. Maytin, MD, PhD Jonelle McDonnell, MD Melissa Piliang, MD Apra Sood, MD James S. Taylor, MD
Section of Dermatologic Surgery and Cutaneous Oncology Philip L. Bailin, MD, MBA, FACP, Head Christine Poblete-Lopez, MD Jon Meine, MD Rebecca Tung, MD Allison T. Vidimos, RPh, MD
Section of Dermatopathology Wilma F. Bergfeld, MD, FACP, Co-Director Melissa Piliang, MD, Co-Director
Section of Industrial Dermatology James S. Taylor, MD, Head Section of Clinical Research Jonelle McDonnell, MD
Cutaneous Care Center Jonelle McDonnell, MD
Molecular Dermatology Edward V. Maytin, MD, PhD, Head
Family Health and Surgery Center Physicians Beachwood Ann Kooken, MD Jon G. Meine, MD Arlene Ruiz de Luzuriaga, MD Rebecca Tung, MD
Chagrin Falls Rosemary S. Keskinen, MD Amy M. Polster, MD
Independence Beverly K. Lehman Cameron, MD Pamela Ng, MD Christine Poblete-Lopez, MD Carol Slover, MD
Lorain John Secrist, MD
Strongsville Irene C. Lalak, MD
Westlake John Krebs, MD
Willoughby Hills Ursula Stanton-Hicks, MD Abena Ofori, MD
Wooster George H. Kuffner, MD
282972A.indd 33 6/19/08 3:34:50 PM

Outcomes 2007 34
Department of Plastic Surgery James E. Zins, MD, Chairman
Quality Review Officer Mark F. Hendrickson, MD
Steven L. Bernard, MD Risal S. Djohan, MD Mark F. Hendrickson, MD Raymond Isakov, MD Robert Lohman, MD Armand R. Lucas, MD Frank A. Papay, MD Silvia C. Rotemberg, MD Maria Siemionow, MD, PhD Randall J. Yetman, MD James E. Zins, MD
Family Health and Surgery Center PhysiciansBeachwood Armand R. Lucas, MD Frank A. Papay, MD Silvia C. Rotemberg, MD Randall J. Yetman, MD Independence Shashidhar Kusuma, MD Lorain Steven L. Bernard, MD Lutheran Hospital Mark F. Hendrickson, MD Solon Mark F. Hendrickson, MD Raymond Isakov, MD Strongsville Risal S. Djohan, MD Shashidhar Kusuma, MD Westlake Steven L. Bernard, MD John Krebs, M.D.
Dermatology and Plastic Surgery Anesthesiology Armin Schubert, MD, MBA, Chairman, General Anesthesiology Walter Maurer, MD, Section Head Harendra Arora, MD Charanjit Bahniwal, MD Raymond Borkowski, MD Thomas Bralliar, MD J. Michael DeUngria, MD Joseph Foss, MD Ursula Galway, MD Brock Gretter, MD Robert Helfand, MD Maria Inton-Santos, MD Tatiana Kopyeva, MD Priya Kumar, MD R. Michael Ritchey, MD Stacy Ritzman, MD Peter Schoenwald, MD Sara Spagnuolo, MD Karen Steckner, MD
Some physicians may practice in multiple locations. For a detailed list including staff photos, please visit clevelandclinic.org/staff.
282972A.indd 34 6/19/08 3:34:50 PM
Dermatology & Plastic Surgery Institute35
Contact InformationAdditional Contact InformationGeneral Information
216.444.2200
Hospital Patient Information
216.444.2000
Patient Appointments
216.444.2273 or 800.223.2273
Special Assistance for Out-of-State Patients
Complimentary assistance for out-of-state patients and families
800.223.2273, ext. 55580, or email [email protected]
International Center
Complimentary assistance for international patients and families
800.884.9551 or 001.631.439.1578 or visit clevelandclinic.org/ic
Cleveland Clinic in Florida
866.293.7866
For address corrections or changes, please call 800.890.2467
General Patient Referral
24/7 hospital transfers or physician consults 800.553.5056
General Dermatology Appointments/Referrals
216.444.5725 or 800.223.2273 ext. 45725
Surgical Dermatology Appointments/Referrals
216.444.5724 or 800.223.2273, ext. 45724
Cutaneous Care Center
216.444.2649 or 800.223.2273, ext. 42649
Dermatology Clinical Research
216.445.8454 800.223.2273, ext. 58454
Dermatology Financial Counselor
216.445.8662 or 800.223.2273, ext. 58662
Plastic Surgery Appointments/Referrals
216.444.6900 or 800.223.2273 ext. 46900
Plastic Surgery Financial Counselor
216.445.1331 or 800.223.2273, ext. 51331
On the Web at:
clevelandclinic.org/dermatology and clevelandclinic.org/plastics
282972A.indd 35 6/19/08 3:34:50 PM

Outcomes 2007 36
Institute LocationsStrongsville Family Health and Surgery Center
16761 SouthPark Center Strongsville, OH 44136 Dermatology and Plastic Surgery: 440.878.2500
Westlake Family Health Center
30033 Clemens Road Westlake, OH 44145 Dermatology and Plastic Surgery: 440.899.5555
Willoughby Hills Family Health Center
2570 SOM Center Road Willoughby Hills, OH 44094 Dermatology: 440.943.2500
Cleveland Clinic Wooster
1739 Cleveland Road Wooster, OH 44691 Dermatology: 330.287.4500
Main Campus
9500 Euclid Avenue Cleveland, OH 44195
Beachwood Family Health and Surgery Center
26900 Cedar Road Beachwood, OH 44122 Dermatology and Plastic Surgery: 216.839.3000
Chagrin Falls Family Health Center
551 E. Washington St. Chagrin Falls, OH 44022 Dermatology: 440.893.9393
Independence Family Health Center
5001 Rockside Road Crown Center II Independence, OH 44131 Dermatology and Plastic Surgery: 216.986.4000
Lorain Family Health and Surgery Center
5700 Cooper Foster Park Road Lorain, OH 44053 Dermatology and Plastic Surgery: 440.204.7400
Lutheran Hospital
1730 West 25th St. Cleveland, OH 44113 Plastic Surgery: 216.363.2311
Solon Family Health Center
29800 Bainbridge Road Solon, OH 44139 Plastic Surgery: 440.519.6800
282972A.indd 36 6/19/08 3:34:51 PM

Dermatology & Plastic Surgery Institute37
Cleveland Clinic Overview Online Services
Cleveland Clinic, founded in 1921, is a nonprofit multispecialty academic medical center that integrates clinical and hospital care with research and education. Today, 1,800 Cleveland Clinic physicians and scientists practice in 120 medical specialties and subspecialties, annually recording more than 3 million patient visits and more than 70,000 surgeries.
In 2007, Cleveland Clinic restructured its practice, bundling all clinical specialties into integrated practice units called institutes. An institute combines all the specialties surrounding a specific organ or disease system under a single roof. Each institute has a single leader and focuses the energies of multiple professionals onto the patient. From access and communication to point-of-care service, institutes will improve the patient experience at Cleveland Clinic.
Cleveland Clinic’s main campus, with 37 buildings on 140 acres in Cleveland, Ohio, includes a 1,000-bed hospital, outpatient clinic, specialty institutes and supporting labs and facilities. Cleveland Clinic also operates 14 family health centers; eight community hospitals; two affiliate hospitals; a 150-bed hospital and clinic in Weston, Fla.; and health and wellness centers in Palm Beach, Fla., and Toronto, Canada. Cleveland Clinic Abu Dhabi (United Arab Emirates), a multispecialty care hospital and clinic, is scheduled to open in 2011.
At the Cleveland Clinic Lerner Research Institute, hundreds of principal investigators, project scientists, research associates and postdoctoral fellows are involved in laboratory-based research. Total annual research expenditures exceed $150 million from federal agencies, non-federal societies and associations, and endowment funds. In an effort to bring research from bench to bedside, Cleveland Clinic physicians are involved in more than 2,400 clinical studies at any given time.
In September 2004, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University opened and will graduate its first 32 students as physician-scientists in 2009.
Cleveland Clinic is consistently ranked among the top hospitals in America by U.S.News & World Report, and our heart and heart surgery program has been ranked No. 1 since 1995.
For more information about Cleveland Clinic, visit clevelandclinic.org.
eCleveland CliniceCleveland Clinic uses state-of-the-art digital information systems to offer several services, including remote second medical opinions to patients around the world; personalized medical record access for patients; patient treatment progress for referring physicians (see below); and imaging interpretations by our subspecialty trained radiologists. For more information, please visit eclevelandclinic.org.
DrConnectOnline Access to Your Patient’s Treatment Progress
Whether you are referring from near or far, DrConnect can streamline communication from Cleveland Clinic physicians to your office. This online tool offers you secure access to your patient’s treatment progress at Cleveland Clinic. With one-click convenience, you can track your patient’s care using the secure DrConnect website. To establish a DrConnect account, visit eclevelandclinic.org or email [email protected].
MyConsultMyConsult Remote Second Medical Opinion is a secure online service providing specialist consultations and remote second opinions for more than 600 life-threatening and life-altering diagnoses. The MyConsult service is particularly valuable for people who wish to avoid the time and expense of travel. For more information, visit eclevelandclinic.org/myconsult, email [email protected] or call 800.223.2273, ext 43223.
282972A.indd 37 6/19/08 3:34:51 PM
9500 Euclid Avenue, Cleveland, OH, 44195
© The Cleveland Clinic Foundation 2008
Cleveland Clinic is a nonprofit multispecialty academic medical center. Founded in 1921, it is dedicated to providing quality specialized care and includes an outpatient clinic, a hospital with more than 1,000 staffed beds, an education institute and a research institute.
pantone black 7pantone 3005
pantone 348
pantone 151
Secondary colors
pantone 260 pantone 220 pantone 7406
pantone 665
Supporting colors
Brights
pantone 393 pantone 380 pantone 150 pantone 305 pantone 204
pantone 5807
Neutrals
pantone 705 pantone 5175 pantone 351 pantone 7513 pantone 649 pantonecool gray 9
pantone 7546 pantone 497 pantone 7533
10%
Please visit us on the Web at clevelandclinic.org.
282972A.indd 38 6/19/08 3:34:51 PM