developmental disturbances of teeth dr. saleem shaikh
TRANSCRIPT

DEVELOPMENTAL DISTURBANCES OF TEETH
Dr. Saleem Shaikh

DEVELOPMENTAL DISTURBANCES IN STRUCTURE OF TEETH Enamel hypoplasia Dentinogenesis imperfecta Dentin dysplasia Regional odontogenic dysplasia

ENAMEL HYPOPLASIA ENAMEL HYPOPLASIA
Defect of enamel due to disturbance during its formative process
Ameloblasts are among the most sensitive cells in the body
During the formative stages of enamel the ameloblast cells are susceptible to various factors which can disturb the process and the effect of which are reflected on the surface enamel after the eruption of tooth

Types
Based on causative factors:
Enamel hypoplasia Enamel hypoplasia
Hereditary (Amelogenesis Imperfecta)
Environmental
Focal(Turners hypoplasia)
Generalized

Differences between hereditary & environmental enamel hypoplasiaDifferences between hereditary & environmental enamel hypoplasia
Hereditary 1. Both dentition
affected
2. Only enamel is affected
3. Affected tooth shows diffuse or vertical orientation of defects
Environmental1. Either one
dentition affected
2. Affects enamel and other calcified structures
3. Affected tooth shows defect which is horizontally arranged

Hereditary enamel hypoplasia Amelogenesis imperfecta Hereditary enamel hypoplasia Amelogenesis imperfecta
Hereditary enamel dysplasia; Hereditary brown enamel; Hereditary brown opalescent tooth
It is a heterogenous group of hereditary disorders of enamel formation Entirely an ectodermal disturbance. The condition involves only the enamel while dentin, cementum & pulp remain normal
3 types 1. Hypoplastic type - Defective matrix deposition 2. Hypocalcification type – Defective calcification3. Hypomaturation type- Defective maturation
Classification
1. Hypoplastic type Generalized Pitted, autosomal dominantLocalized Pitted, autosomal dominant Localized Pitted, autosomal recessiveDiffuse Smooth, autosomal dominantDiffuse Smooth, X-linked dominantDiffuse Rough, autosomal dominantEnamel agenesis autosomal recessive 2. Hypomaturation type
Diffuse pigmented, autosomal recessive
Diffuse, X-linked recessiveSnow capped, X-linkedSnow capped, autosomal dominant
3. Hypocalcification type Diffuse,Autosomal dominantDiffuse,Autosomal recessive

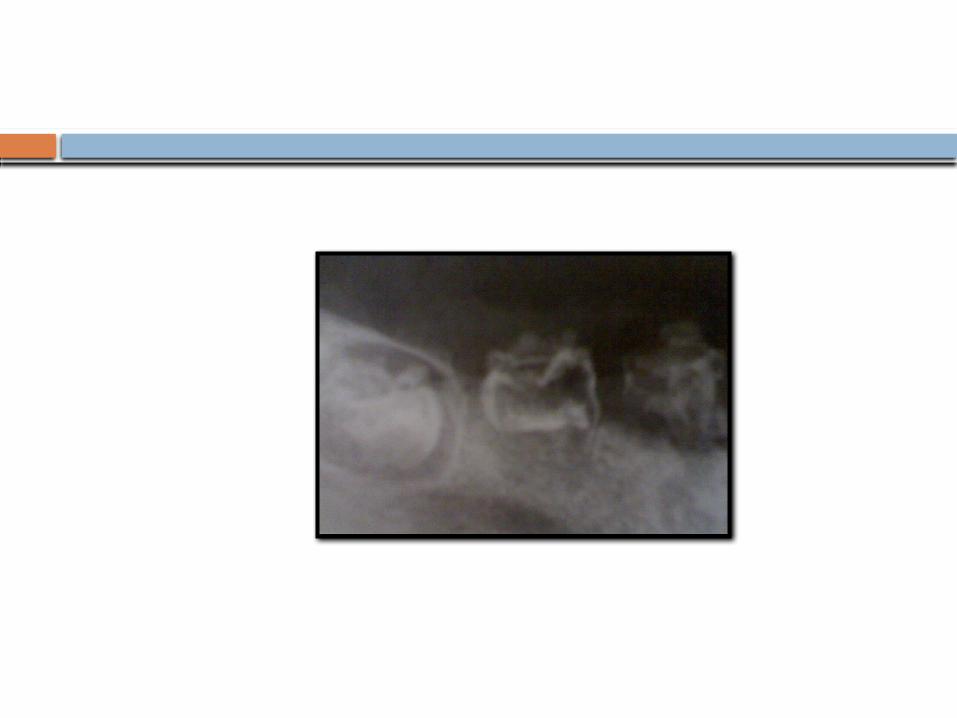
Hypoplastic type Hypoplastic type
The disease affects the stage of matrix formation Teeth exhibit complete absence of enamel or there may be
presence of enamel on some focal areas Enamel thickness is usually below normal Quantity is affected, but quality of formed enamel is normal Tooth appears as though prepared for receiving a prosthetic
crownRadiographic features -
Enamel may appear totally absent or as a thin lineRadiodensity of affected enamel is similar to that of normal enamel (greater than dentin)

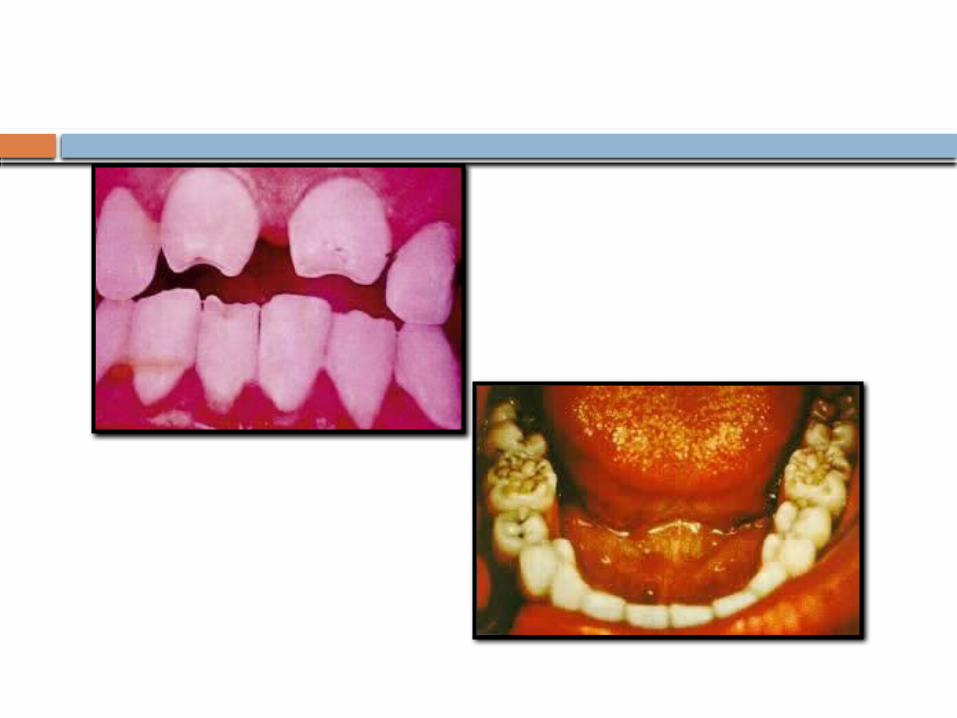
Hypocalcification type Hypocalcification type
The disease affects the stage of early mineralization Enamel is of normal thickness(quantity not affected) Tooth is normal in shape on eruption, but the enamel is lost
very easily Enamel is soft & can be easily removed with a blunt
instrument Enamel is yellowish brown on eruption
Radiodensity of affected enamel is lesser than that of normal enamel and is equivalent to normal dentin

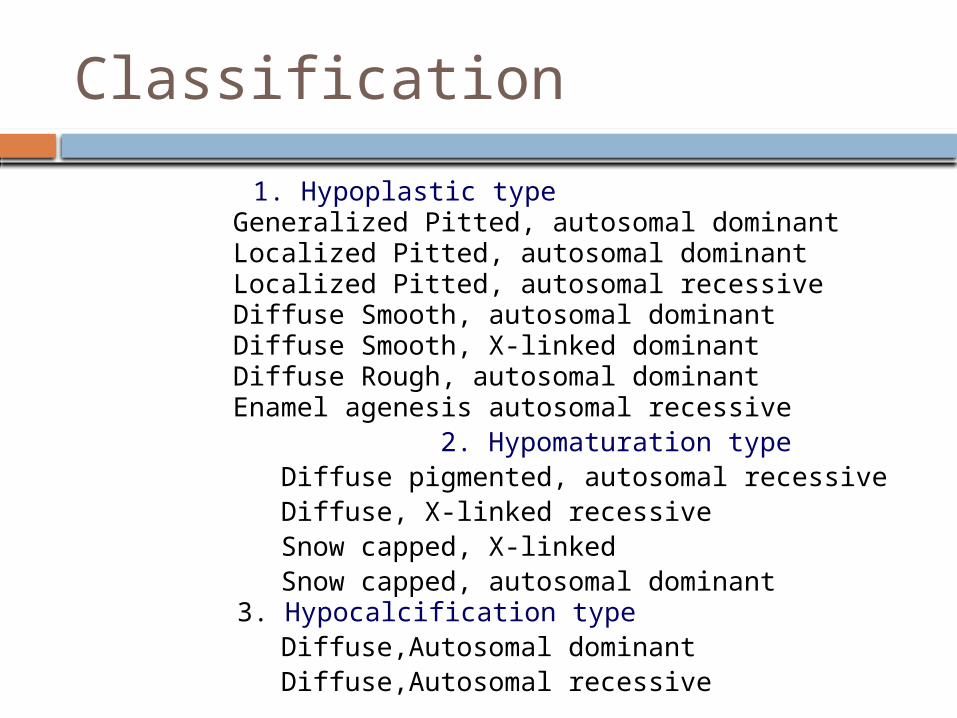
Hypomaturation type Hypomaturation type
The disease affects the stage of maturation Enamel is of normal thickness (quantity not affected) Teeth are normal in shape but enamel is opaque white or
brownish in colour Enamel does not have normal hardness & translucency and
tend to chip off easily It Can be pierced with an explorer tip with firm pressure Snow capped teeth - It is the mildest form of
hypomaturation type of amelogenesis imperfecta. The enamel is of near normal hardness & has a zone of
white opaque enamel on the incisal or occlusal one quarter to one third of crown.
Demonstrates an anterior to posterior distribution and have been compared to a denture dipped in white paint
Radiodensity of affected enamel is much lesser than that of normal enamel



Environmental enamel hypoplasiaEnvironmental enamel hypoplasia
FOCAL ENAMEL HYPOPLASIA; Also known as Turner’s hypoplasia;
Most common form of enamel hypoplasia
Occurs due to trauma or infection to deciduous teeth
Usually affects single tooth & is called as Turners tooth
Hypoplasia ranges from a mild, brownish discolouration to a severe pitting of enamel surface on the labial aspect
Frequently involved teeth are permanent maxillary/mandibular bicuspids & maxillary incisors
Severity of hypoplasia depends on severity of infection,
degree of tissue involvement and stage of tooth formation

Pathogenesis Pathogenesis
Deciduous teeth
Trauma Periapical Infection
Affect the ameloblastic layer of permanent tooth
Disturb the enamel formation
Enamel defects


Generalized Enamel Hypoplasia Generalized Enamel Hypoplasia
The ameloblasts in the developing tooth germ are sensitive to external stimuli
Any systemic or environmental disturbance can result in abnormalities in enamel formation which manifests as defects on the surface of tooth
It affects numerous teeth which are being formed at the time of disturbance
Clinically the defects can manifests as
1. Hypoplasia
2. Diffuse opacities
3. Demarcated opacities Most often it manifests as a horizontal line of enamel
hypoplasia with pits & grooves CHRONOLOGIC HYPOPLASIA -

The line on the tooth surface indicates the zone of enamel hypoplasia
The location of the line corresponds with the developmental stage of affected tooth & width indicates the duration of the disturbances

Causes Causes
PrenatalInfections (Rubella, Syphilis)Malnutrition, Metabolic & Neurological disorders during
pregnancy Chromosomal abnormalities Excess chemical intake (Tetracycline, Fluoride)
Neonatal Birth injury Premature delivery Prolonged laborLow birth weight
Postnatal Severe childhood infections (Viral exanthematous fever)Congenital heart diseases Nutritional deficiencies (Vit-B, Vit-D)Endocrinal disorders

Enamel hypoplasia due to nutritional deficiency and exanthematous fevers
Enamel hypoplasia due to nutritional deficiency and exanthematous fevers
Serious nutritional deficiency is potentially capable of producing enamel hypoplasiaThe teeth that form within the first year after birth are affected.Teeth most frequently affected are central & lateral incisors, cuspids and first molars.Premolars, 2nd & 3rd molars are rarely affected, since their formation does not begin until the age of 3 or laterPresents as pitting of the tooth surface

Enamel hypoplasia due to congenital syphilisEnamel hypoplasia due to congenital syphilis
Hypoplasia is not of pitted variety Involves the permanent maxillary & mandibular incisors and 1st
molars Anterior teeth are referred to as Hutchinson’s incisors and
posterior teeth are referred to as mulberry molars. Characteristically, the upper central is screw driver shaped,
the mesial and distal surfaces tapering and converging towards the incisal edge.
Incisal edge is usually notched. Middle lobe of tooth is affected The crowns of first molars are irregular & constricted, and the
enamel of the occlusal surface and occlusal third of tooth appears to be arranged in an agglomerate mass of globules rather that well formed cusps.
Resembles a mulberry, hence the name mulberry molars

Enamel hypoplasia due to fluorideEnamel hypoplasia due to fluoride
Excess amounts of fluoride can result in enamel defect known as dental fluorosis./ mottled enamel
The severity increases with an increase in amount of fluoride in the water.
The optimum range of fluoride in drinking water is 0.7 -1.2 ppm
Increased levels of fluoride interferes with calcification process of the enamel matrix leading to the formation of hypomineralized enamel
These alterations results in an increased surface and subsurface porosity of the enamel which alters the light reflection and creates the appearance of white chalky areas which later gets stained


Clinical featuresClinical features
Affected teeth are caries resistant Wide range of manifestations depending on fluoride levels Grading
Questionable changes White flecking or spotting of enamel
Mild changes White opaque areas involving more of tooth surface
areas Moderate and severe changes
Pitting and brownish staining of surface Corroded appearance
Mild cases- Bleaching of teeth Severe cases- Prosthetic crowns

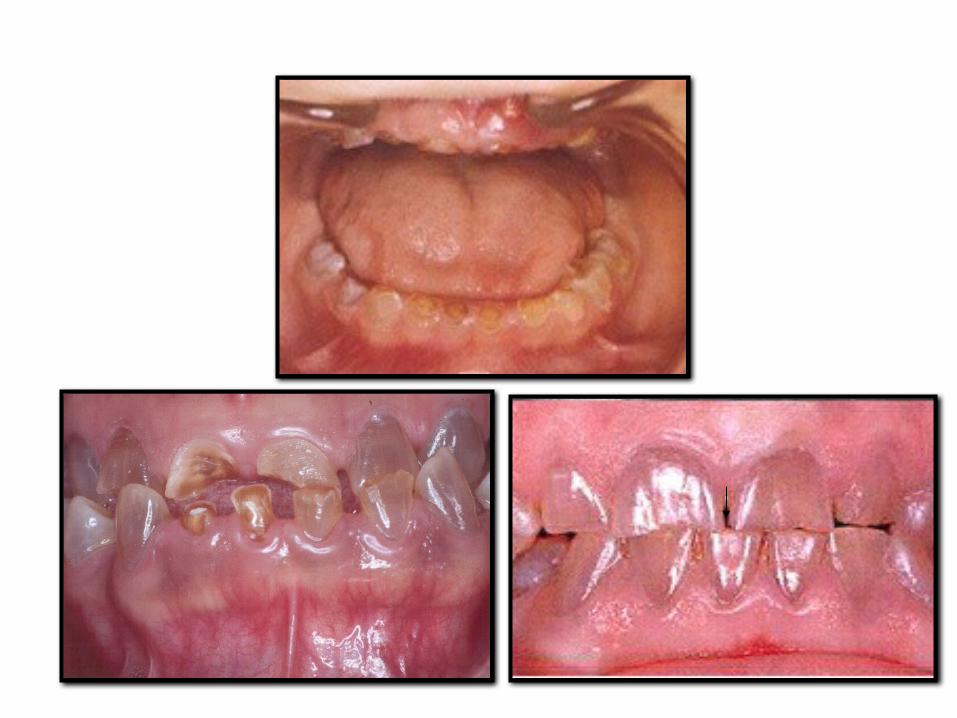
Dentinogenesis Imperfecta Dentinogenesis Imperfecta
A hereditary defect of dentin in the absence of any systemic disorder, consisting of opalescent teeth composed of irregularly formed and undermineralized dentin that obliterates the coronal and root pulpal chambers.
Also known as “Hereditary opalescent dentin”, “Capdepont’s teeth”
Severely affects the deciduous teeth than permanent teeth (Incisors & 1st molars; Least involved teeth- 2nd & 3rd molars)
Teeth exhibits a gray to brownish violet or yellowish brown appearance
Involved teeth exhibits a characteristic unusual translucent or opalescent hue.
Enamel is normal but fractures and chips away easily leads to exposed dentin and functional attrition presumably because of defective DEJ
Teeth are not particularly sensitive & are not caries prone

Type I Associated with osteogenesis imperfecta, blue
sclera Type II
Not associated with osteogenesis imperfecta unless by
chance This type is most frequently referred to as
Hereditary opalescent dentin
Most common type Type III
Brandywine type, racial isolate in Maryland state Same clinical presentation of Type I or II with
multiple pulpal exposures in deciduous dentition

Classification (Shafer)
DENTINOGENESIS IMPERFECTA 1: Dentinogenesis imperfecta without osteogenesis imperfecta (opalescent dentin), this corresponds to dentinogenesis imperfecta type II of Shields classification.
DENTINOGENESIS IMPERFECTA 2: Brandywine type dentinogenesis imperfecta: this corresponds to dentinogenesis imperfecta type III of Shields classification.
There is no substitute in the present classification for the
category designated as DI Type I of the previous classification (Shield’s ).

Radiological features Radiological features
Exhibit bulb-shaped or bell shaped crowns with constricted CEJ (tulip shaped)
Thin & blunted roots Early obliteration of root canals and pulp chamber Cementum, PDL & bone appears normal Type II exhibits great variability in deciduous teeth, ranging
from normal to those changes of type I Shell teeth
Apparently normal enamel
Extremely thin dentin (may involve entire tooth or isolated to the root)
Enormous pulp chambers (not as a result of resorption, but due to insufficient dentin)
Appear as shells of enamel & dentin surrounding enormous pulp chambers and root canals.


Histopathological features Histopathological features
Enamel & mantle dentin are normal Remaining dentin is severely dysplastic & exhibits vast
areas of inter-globular dentin Dentinal tubules are short, disoriented, irregular & widely
spaced Scanty odontoblasts line the pulp and they can be seen in
the defective dentin Smooth DEJ
Treatment is aimed at preventing excessive tooth attrition & improving esthetics
Metal / Ceramic crowns & over dentures can be given

Dentin dysplasia Dentin dysplasia A hereditary defect characterized by defective dentin
formation & abnormal pulpal morphology Autosomal dominant disorder Type I – Radicular dentin dysplasia
Also known as “Rootless teeth” Type II – Coronal dentin dysplasia
MildSevere

Clinical features Clinical features
Type I Type II
Disturbance in development of radicular dentin
Disturbance in development of coronal dentin
Normal crowns both structurally & morphologically
Semi-transparent opalescent primary
teeth Normal appearance in the permanent teeth
Color of teeth normal with slight bluish translucency in cervical region
Amber – grey color
Early loss of dentin organization results in extremely short rootsLater disorganization results in minimal root changesAffected teeth exhibits short roots, delayed eruption , severe mobility & premature exfoliation


Radiological features Radiological features Type I Type II
Permanent teeth: Features vary on the proportion of organized versus disorganized dentin Early disorganization - extremely short roots with little or no pulpSomewhat Later disorganization - crescent or chevron shaped pulp chambers overlying shortened roots that exhibit no pulp canals Late disorganization – normal pulp chamber with large pup stone
Permanent teeth: Exhibits abnormally large pulp chambers and apical extension described as flame shaped or thistle-tube in shape. Pulp stones present
Deciduous teeth affected severely with little or no detectable pulp
Deciduous teeth shows bulbous crowns, cervical constriction and early obliteration of pulp (Resembles DI)
Periapical radiolucencies around the defective roots
Absence of periapical radiolucencies


Histopathological features Histopathological features
Type I Type II
Normal enamel Normal enamel and radicular dentin with partial obliteration of root canals
Portion of coronal dentin is usually normal and may show tubular dentin apical to itPulp is obliterated by calcified tubular dentin, osteodentin & fused denticles
Near normal coronal dentin with numerous areas of interglobular dentin near the pulp
Normal dentinal tubule formation appears to be blocked so that new dentin forms around obstacles and takes on characteristic appearance described as lava / stream flowing around boulders
Abnormally large pulp chambers with pulp stones


Regional Odontodysplasia Regional Odontodysplasia
It is a uncommon non-hereditary developmental disturbances of tooth characterized by defective formation of enamel & dentin with abnormal calcifications of pulp & follicle
Also known as “Ghost teeth”
Cause - Local ischemic change during odontogenesis Clinical features: More common in permanent dentition More common in maxilla Affects several teeth in a single quadrant Maxillary anterior teeth affected more Failure of eruption or delayed eruption of affected teeth Teeth are deformed, yellowish – brown in color with a soft leathery
surface

Radiological features Radiological features
Marked decrease in radio density of teeth Enamel & dentin are very thin & radiological
distinction not possible Extremely large & open pulp chamber with pulp stones Ghostly appearance of affected teeth
Abnormal enamel & dentin Large pulp chamber with pulp stones Calcification in follicular connective