diane a. tennies, ph.d., ladc lead teap regional health specialist august 5 & 7, 2014
TRANSCRIPT

TEAP and TUPP: How to Thrive During a ROCA
Diane A. Tennies, Ph.D., LADCLead TEAP Regional Health SpecialistAugust 5 & 7, 2014

Summary and Goals
Assist TEAP specialists to: Learn strategies to prepare for a
ROCA Be ready to “show their work” to
demonstrate the PRH requirements Use this process to improve the
quality of program

ROCA Basics
Happen about every two years, depending on region
Conducted as part of center-wide review by regional office
Compliance review Opportunity for technical assistance
Wellness Documents Reviewed
List of best practices (3-5) Bloodborne Pathogen Plan CLIA certification (if applicable) Credentials for wellness staff Certifications Liability insurance Licenses Sub-contracts Waivers, if applicable HEALs Program Evaluation
Making the Grade Health Care Guidelines (HCGs) Health-related Standard Operating
Procedures Logs/Spreadsheets CA-1/injury log Dental productivity HIPAA disclosures MSWR phone contact Narcotics log Refrigerator temperature monitoring Sharps exposure Spore testing log SHR
Meeting minutes HEALs meeting minutes Monthly meeting with Center Director, Center
Physician, CMHC Quarterly SART meeting Schedule of meeting times SGA wellness committee Wellness staff meetings
Memoranda of Understanding MSWRs (past year) Materials Safety Data Sheet (MSDS) Personal authorizations Quality assurance
Student Surveys CQI studies
Reports/Surveys Annual H&W Program Description Assessments (most recent corporate and self review) H&W quality assurance surveys/results HMIS reports (past year) Student Satisfaction Survey Quarterly Alcohol Summary (past year)
SIRs (including nonmedical, past year) Staff roster (all center staff, positions included) Staff training hours (from HR including CPR/First Aid,
Bloodborne Pathogens, HCGs) percent of total staff trained, and of those not trained who are essential staff


Guidance

Preparing for ROCA
To Organize and Thrive: Complete Pre-ROCA form(s) ahead of
time!! Best practices Conduct own QA review Compile list of questions for assistance Call Regional TEAP Health Specialist

First Page:

What is Reviewed:
Basics: credentials, and operating under waiver? Hours meet/exceed PRH? Working hours that balance availability and documentation On monthly calls?
Generally: Role on center; collaboration with others; grasp of concepts; visibility; does SHR “tell the story”
Process: Generally arrive around 8 to 8:30; Brief-In; Meet staff; Review SHR; Meet with Staff; Focus Group
Prevention and Education CPP, CDP & CTP occurring? Using templates? How many events per year? What were they? Efforts to collaborate and consult?

Examples: Prevention and Education “in action”

Thanks to George in South Bronx

Thanks to Greg at Fort Simcoe

What is Reviewed?
Assessment of Risk Understand why assessment of risk critical? Review SIF within a week? (score it properly?) Look at SHR record (6-53 and Health Hx form)? Use formalized assessment measures when needed? Put all data together to understand risk and how to
intervene? Offer intervention services and/or referrals Document process in SHR
Intervention Services Documentation in SHR** Intervention Contract? Follow through and tracking

What is Reviewed?
Applicant Review Process Involved? Know how to use Appendix 610?

What is Reviewed?
Drug Testing Review urine collection procedures – chain of custody
Supervised versus observed process? Who collects? Have they been trained? How control for adulteration/contamination?
Input and 2nd test – review parameters 37 to 40 days (flexible)
What is suspicious screen process? Behaviorally based? Is staff trained? What is process for alcohol testing? If breathalyzer, are staff
trained and is it calibrated (log)? Are results filed in SHR? Quarterly Alcohol Report completed? Are students told their results (is it documented?) What is the center’s general policy for managing alcohol use?


What is Reviewed?
Relapse Prevention – it is more than just self-help groups. Should be integrated into all of work and not separate program
Individual treatment plans to include RP Yes - Self-Help groups – on versus off-center
access Speakers at assemblies (e.g. employers who
hire) Ongoing RP groups CTP groups Emphasize in individual meetings Newsletters/electronic communication

What is Reviewed?
MSWRs Understand reason for the process? Review the AODA MSWR – do they
return? How facilitate? Collaborate with CMHC? What are the community connections? Quality of referrals?

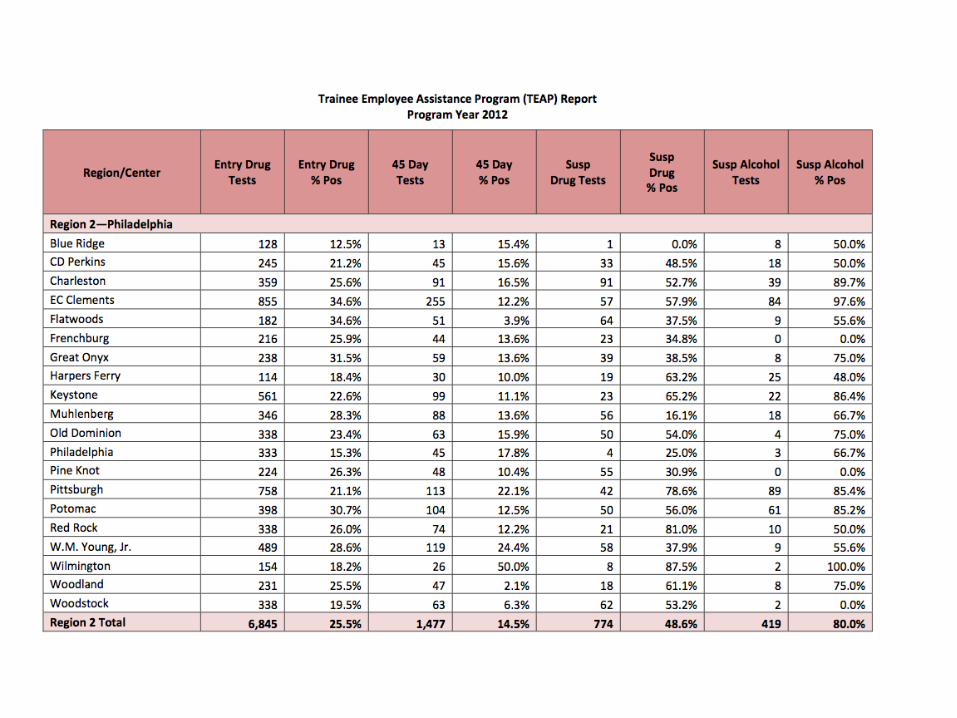
Other Data Reviewed
Use data from PY2012/2013: % + on entry % + at 45 days Both regional and national
Only use other data points if necessary to make a point about the program
Keeping own statistics? Continuous Quality Improvement
Understand why this data is a barometer of efficacy

TUPP: What is Reviewed? Who coordinates? How much time allocated? Educational materials available? Use an efficacy based tobacco cessation program? (Not
on Tobacco for instance) Policy for e-cigarettes and other tobacco products? Are minors kept out of tobacco use areas? Badges? Tobacco use areas? Will do ‘walk-about’ Are all tobacco-using minors referred to TEAP for
mandatory services? Separate out those mandated for services from those
wanting to stop using? Minors should not be getting NRP Services all documented in SHR Staff do not use tobacco around students

Documentation
“You are only as good as your documentation” = Professional Licensing requirements Standards of Care – what do we know? Basics
Pen, original signature (with credential and role), no white out or sticky notes
Document process of event Especially with MSWR; ZT termination; Counts; if unusual
Contents DOS Content (can be standardized) Individualized for each student
Shortcuts Labels; stamps; one sheet Other ideas?

Scoring
Job Corps uses a Program Rating System (PRS) as a qualitative measure of performance for center/OA/CTS operations (PAG, pg 4, Aug 2008).

ROCA Scoring
Satisfactory (4/5)Requirements and quality indicators are generally evident in applicable program areas with minor exceptions. A quality assurance plan is in place that demonstrates adequate controls to ensure integrity and accountability of program assets and data.

Unsatisfactory (0/1)Critical requirements are missing or minimally evident. Quality indicators are not achieved. The program lacks procedures and controls necessary to ensure compliance, quality, and data integrity.
ROCA Scoring

Marginal (2/3)Requirements and/or quality indicators are missing or minimally evident in applicable program areas. Quality assurance is minimal, resulting in inconsistencies in accountability and integrity of program assets and data.
ROCA Scoring

Very Good (6/7)Programs, procedures, and systems are consistently in place to ensure delivery of requirements and achievement of quality indicators. Some innovative approaches are employed to promote continuous improvement. A viable quality assurance plan ensures integrity and accountability of program assets and data.
ROCA Scoring

Exceptional (8/9)Programs, procedures, and systems are well organized, clearly communicated, and administered to ensure quality delivery of all requirements and achievement of quality indicators. Innovative approaches result in program enhancements and improved outcomes. Through rigorous self-assessments and quality assurance, the operator safeguards program assets and maintains the integrity of program data.
ROCA Scoring
Capturing Strengths
Tell the assessors what you do well – what goes “above and beyond”. What is a best practice.
Examples: The TEAP specialist has created a Comprehensive Summary
Sheet that provides him quickly with information on each student and consists of: CRAFFT, SASSI, TEAP participation, suspicious reports and drug test collection, interventions, and TUPP participation sections.
The TEAP specialist hosts Recovery Meetings with students where certificates of completion are provided to students that complete the TEAP intervention with a negative second drug test.
Additional drug counseling for five to six sessions are provided at Pennyroyal Clinic at no cost to students that need more intense services.

More Examples
There is a thriving TEAP mentoring program that is highly visible and active on center.
“Harvey’s Hacienda” represents a powerful and unique component of this TEAP. Due to the confidentiality and nonjudgmental nature of the program, students identify it as the ‘safest room on center’. There are visual representations of students’ success, which are highly motivating to participating students.
The very low retest rate on the second test and the lack of student separations before the 45-day test provide evidence that the intervention services are highly effective.
The TEAP specialist typically accompanies students to their treatment program and then picks them up when the treatment is completed, which likely contributes to the high MSWR return rate.

Questions