discovering the causes of otitis externa - inpractice.bmj.com · in ractice focus may 016 7...
TRANSCRIPT

7In Practice FOCUS May 2016
Discovering the causes of otitis externaSue Paterson
CAUSES OF DISEASE
Otitis externa is one of the most common reasons why dogs present to veterinary surgeons in primary care practice. It is a much less common problem in the cat. This article outlines a logical approach principally to canine otitis externa. It describes the need to identify and manage primary causes of otitis, especially allergy which is the most common of these. Emphasis is placed on the fact that the more chronic the otitis, the greater the need to investigate its underlying cause rather than treat symptomatically. Secondary infections are discussed, particularly the need to perform cytology and where appropriate culture and sensitivity, in order to select specific antimicrobial therapy. The need to identify and manage both predisposing factors, such as conformation, and perpetuating factors, such as chronic change and otitis media are outlined. However, it is emphasised that these factors contribute to disease and should never be treated without addressing both secondary infection and primary causes.
OTITIS externa is inflammation of the external ear canal. The external ear canal is similar in structure to the interfollicular epidermis of the skin. It is a stratified cornifying epithelium with adnexal organs, such as hair follicles and their associated sebaceous and ceruminous glands. Therefore, any disease that affects the skin can also affect the external ear canals. The most recent classification for the aetiology of otitis externa has been proposed by Griffin (2010). In this system the aetiology of otitis externa can be divided into primary and secondary causes which are respectively diseases or infections that directly cause inflammation in the ear and perpetuating or predisposing factors that are agents or elements that contribute to ear disease. These latter two factors do not cause ear disease in their own right but may prevent resolution of the disease and lead to recurrence if they are not dealt with adequately.
Primary causesPrimary causes of otitis externa are those responsible for initiation of the inflammatory process in the ear and are all skin problems (Table 1). Failure to identify and manage primary causes is one of the most common reasons why ear disease recurs and why acute disease progresses to chronic, often irreversible, disease. Although it is not essential to investigate underlying problems
Sue Paterson, Rutland House Referrals, Abbotsfield Road, St Helens, Merseyside WA9 4HU, UKe-mail: [email protected]
in patients on their first presentation to the clinic, it is important to discuss this option and offer further investigation on subsequent visits. Allergy, especially atopic dermatitis, is the most common primary trigger for otitis externa (Paterson 2002, Saridomichelakis and others 2007, Zur and others 2011). In a review of primary causes of otitis, I found that 75 per cent of all cases of otitis presenting to my referral clinic had atopic dermatitis as a primary trigger (Paterson 2002). Although this may represent a skewed population, other studies have identified similar trends (Saridomichelakis and others 2007, Zur and others 2011). In the same study (Paterson 2002), a strong breed predisposition was recognised. German shepherd dogs, labrador and golden retrievers, boxer dogs, spaniels, especially cocker spaniels, and West Highland white terriers were identified as commonly having atopic dermatitis as an underlying cause of their ear disease.
Typically, dogs with allergic otitis present with erythema of the pinnae (Fig 1), which is
often followed by the dog scratching at the ears, rubbing the side of its face or shaking its head. In the early phase of the disease the ear canal shows similar degrees of erythema with mild hyperplasia. Cytology of ear wax at this stage is usually unremarkable. Atopic otitis and cutaneous adverse food reactions (Rosser 1993) are commonly seen in young dogs. Other important primary triggers in this age of animal include ectoparasites (Otodectes cynotis, Demodex species) and keratinisation disorders.
Juvenile cellulitis is a rare but very severe peracute cause of otitis in young puppies. These dogs present with a severe exudative – in the early stages sterile – purulent otitis. The discharge usually extends onto the ear pinna; in many cases the disease starts in the ears (Figs 2 and 3).
Where otitis externa occurs for the first time in middle-aged or older dogs, allergy cannot be ruled out as a primary cause, but systemic disease, especially hypothyroidism, is generally a more common trigger. Predisposed breeds for hypothyroidism as a cause of otitis, include spaniels (cocker and springer), English bull
Fig 1: Erythema of ear pinna in an allergic dog
Fig 2: Puppy with juvenile cellulitis showing no signs of facial involvement
Fig 3: Ear of the puppy in Fig 2, showing severe exudative otitis externa
7-11 Paterson.indd 7 22/04/2016 10:54
on 26 Septem
ber 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inp.i470 on 29 April 2016. D
ownloaded from

8 In Practice FOCUS May 2016
terriers, Newfoundlands, Dogue de Bordeaux, English setters and labrador retrievers (Paterson 2002). Although dogs often show other more general signs of hypothyroidism, such as weight increase and lethargy, dogs may present only with signs of a ceruminous otitis (Fig 4). Where the underlying trigger is not identified and managed some dogs will go on to develop more severe Gram-negative bacterial infection, especially Pseudomonas species.
Neoplastic ear disease typically presents in older animals as a unilateral problem, often in dogs with no previous history of otitis. Where neoplastic lesions are present dogs will respond poorly to symptomatic therapy and relapse is usually rapid and severe. Autoimmune disease such as pemphigus foliaceus (Fig 5), and immune-mediated disease, such as sebaceous adenitis, are primary causes that may occur in any age of dog and can affect the ears only. Clinical signs in autoimmune problems often start on the ears and progress rapidly; pemphigus especially in breeds such as the Akita may only affect the ears. Foreign bodies in the ear, such as grass awns, represent one of the most common triggers for otitis in primary care practice. Typically, these cases are peracute in presentation, painful, unilateral and lead rapidly to severe self-inflicted trauma.
Secondary causesInfection with either yeast or bacteria does not occur in a normal ear. In fact, many sources would suggest that the environment inside the external canals of most dogs is sterile, especially within the horizontal canal (Grono 1970b, Dickson and Love 1983). Infection develops because of inflammation produced by primary triggers, usually in combination with perpetuating and predisposing factors. Effective therapy of infection is essential, but if treated without any regard to the other factors contributing to ear disease then recurrence will inevitably occur. Table 2 details the most common bacterial and yeast infections identified from the ears of dogs and cats with otitis externa.
Cytology should be performed in all cases of otitis to establish the presence of infection and to identify the type of bacterial flora within the ear. In acute disease, infection tends to be with Gram-positive bacteria (Staphylococcus species, Streptococcus species) (Fig 6) and yeast, usually Malassezia species (Harvey and others 2005). Where cocci and yeast are identified on cytology, initial therapy can be successfully selected on an empirical basis. The exception to this is where cocci are identified on cytology where appropriate topical therapy appears already to be in place. In these cases, the presence of meticillin-resistant Staphylococcus species or Enterococcus faecalis should be considered and culture is important.
As otitis progresses, the inflammation created by primary factors leads to changes in the ear canal leading to modification of the micro-environment and a change in the bacteria population. Inflammation leads to hyperplasia of the stratified squamous epithelial lining of the canal, resulting in narrowing of the lumen and glandular hyperplasia (Fig 7), leading in turn to an increased production of cerumen. These chronic changes, often in tandem with recurrent courses of topical antibiotics, lead to the development of a less predictable, more resistant population of bacteria, especially Gram-negative bacteria, such as Pseudomonas species. In chronic disease where rods or mixed populations are found on cytology, culture is necessary to help select an appropriate topical antibiotic. Such cases require careful management as the canal is often ulcerated and painful (Fig 8), and otitis media is a common sequel.
Predisposing factorsPredisposing factors contribute to ear disease but will not cause ear disease in their own right. The most important of the predisposing factors are listed in Table 3 and include conformation, excessive moisture in the ear, obstructive ear disease, systemic disease and treatment effects. Although these factors do need to be addressed, especially in chronic disease, treatment of these in isolation rarely leads to successful resolution of otitis. This
Table 1: Significant primary causes of otitis externa
Primary causes
Allergy Atopy, food, contact
Endocrine Hypothyroidism, hyperadrenocorticism
Autoimmune/immune-mediated
Pemphigus foliaceus, bullous pemphigoid, cutaneous (discoid) lupus erythematosus, erythema multiforme, vasculitis, drug eruption
Keratinisation disorders
Sebaceous adenitis, primary idiopathic seborrhoea
Ectoparasites Otodectes cynotis, Demodex species
Foreign bodies Grass awns, sand, ear (canker) powder
Idiopathic Juvenile cellulitis
Fig 4: Ceruminous otitis in a dog with hypothyroidism
Fig 5: Pemphigus foliaceus affecting the ear pinna
Table 2: Secondary infection in otitis externa
Secondary infection
Bacteria – acute disease
Gram-positive bacteria Staphylococcus species, Streptococcus species Corynebacterium species
Bacteria – chronic disease
Gram-positive bacteria Enterococcus species Gram-negative bacteria Pseudomonas species, Proteus species, Escherichia coli
Yeast Malassezia species (common), Candida species (uncommon)
Fig 6: Staphylococcal infection
7-11 Paterson.indd 8 22/04/2016 10:54
on 26 Septem
ber 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inp.i470 on 29 April 2016. D
ownloaded from

9In Practice FOCUS May 2016
is why surgical intervention, such as lateral wall resection, often fails to lead to prolonged periods of improvement in atopic dogs.
Conformation is one of the most common of the predisposing factors in otitis externa. This includes the shape of the pinna, the presence of hair within the canal (Fig 9) and on the concave aspect of the pinna, the lumen of canal and the amount of glandular material within it. Several studies (Fernanado 1966, Baxter and Lawler 1972, Hayes and others 1987) have shown that dogs with pendulous ears, such as the spaniel, are more likely to develop otitis externa. However, not all breeds with pendulous pinnae develop ear disease (Fig 10), confirming that it is not just conformation that leads to otitis but the underlying primary causes that produces the initial inflammation.
Similarly the presence of hair within the canal does not correlate with disease (Hayes and others 1987). Many of the breeds with hirsute canals, such as the cocker spaniel, which has compound hair follicles within its ears, and the miniature poodle, are also breeds at increased risk of developing allergy, making them more likely to develop otitis. Anecdotally, I would suggest this is also the reason why I see increasing numbers of the poodle-gundog crosses with otitis, for example, cockapoos (Fig 11), golden doodles or labradoodles. In many of these ‘designer’ breeds the ear canals are full of thick curly hair, predisposing any atopic individual to ear disease. The
external ear canal of long-haired breeds of dogs and those containing fine hair have also been shown to contain more glandular tissue than short-haired breeds (Fernanado 1966). Stout-Graham and others (1990) found that in a comparison of breed’s predisposed and non-predisposed to otitis, sebaceous gland quantity was similar between groups; however, apocrine (ceruminous) glands were increased in predisposed breeds whether or not otitis externa was present.
The environment within the ear canal predisposes to otitis (Hayes and others 1987, Grono 1970a, b) The shar pei with its typical poorly ventilated ‘letter box’ ear conformation creates moist, humid conditions within the ear canal which increases the risk of otitis. Dogs that swim fill their ears with water, creating maceration within the ear canal, which often then leads to infection with yeast – so-called ‘swimmer’s ear’. Water-based cleaners and topical aqueous antibiotic solutions may produce similar effects.
Increasing environmental temperature and humidity, in warm climates and in the summer months in temperate latitudes, lead to small but measurable changes in the ear canal (Grono 1970a, b). Hayes and others (1987) suggest this phenomenon leads to otitis two to three months later and argue this is why otitis externa is more common during the late summer and early autumn. It is also likely that allergic triggers, such as reactions to pollens, may contribute to this increased incidence of otitis.
Obstructive disease within the canal represents an overlap between a primary cause and a predisposing factor. Many dogs tolerate benign, slow-growing lesions, such as papillomas, basal cell tumours and ceruminous gland adenomas (Fig 12) without ever showing signs of ear disease. This is probably because these lesions cause minimal inflammation within the canal. It appears that it is only when these lesions reach a critical size, to partially occlude the canal and to cause changes in the micro-environment within the ear, that they predispose to infection and otitis. More aggressive neoplasms, such as adenocarcinomas and squamous cell carcinomas, tend to act as primary causes of otitis because they are capable of inducing inflammation within the ear canal even in the early stages of the disease process.
Debilitating disease, especially hepatic, renal or pancreatic disease, also predisposes to otitis. In my experience, systemic disease does not generally act as a primary cause of otitis but increases an animal’s susceptibility to infection and slows down the rate of resolution.
Treatment effects unfortunately often predispose animals to otitis. Iatrogenic damage (to what is often a sensitive allergic ear canal) through inappropriate topical treatment choices or overzealous cleaning with dry cotton wool may cause damage to the ear canal leading to infection. Although effective ear cleaning is essential before the application of any ear treatment, careful assessment of the ear canal is crucial when selecting ear cleaning solutions. Acidic, astringent and alcohol-based cleaners should be used with care in allergic ears. Ceruminolytic cleaners containing de-waxing agents such as sodium docusate, carbamide peroxide and squalene should only be used in ears with ceruminous otitis. Breeds that commonly produce large amounts of thick waxy otic discharge, such as spaniels, benefit from cleaning with these types of agents. In sensitive, ulcerated ears, especially those with Gram-negative bacterial infection, gentle water-based flushes such as those containing chlorhexidine and tris-EDTA are preferable to ceruminolytic cleaners. Repeat courses of topical antimicrobials may lead to a changes in the bacterial population
Table 3: Predisposing factors in otitis externaPredisposing factor Specific change
Conformation Hairy ear canals (poodle), pendulous pinna (basset, bloodhound), stenotic ear canals (shar pei), hairy concave pinna (spaniel), increased glandular tissue within canal (cocker spaniel)
Excessive moisture Environmental factors (heat and high humidity), water (swimmer’s ear, gundogs), water-based cleaners, water-based antibacterial solutions, off license use of antibiotics mixed in aqueous solutions
Obstructive ear disease
Neoplasia, polyps, cysts
Systemic disease Debilitation, systemic disease (renal, hepatic, pancreatic disease)
Treatment effects Inappropriate cleaning solutions (acidic, astringent, alcohol-based cleaning solutions), traumatic cleaning (especially overzealous use of dry cotton wool), overuse of topical antimicrobials
Fig 7: Narrowing of the external ear with early glandular hyperplasia
Fig 8: Ulcerated canal and ruptured tympanic membrane in a chronic case of Pseudomonas infection
Fig 9: Hairy ear canal in a cockapoo
7-11 Paterson.indd 9 22/04/2016 10:54
on 26 Septem
ber 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inp.i470 on 29 April 2016. D
ownloaded from
10 In Practice FOCUS May 2016
within the ear, leading to the development of multiple resistant infections, such as meticillin-resistant Staphylococcus species and E faecalis.
Perpetuating factorsPerpetuating factors are those factors that prevent resolution of otitis and lead to relapse, even if infection and primary causes are adequately treated. The most important of the perpetuating factors are listed in Table 4.
Pathological change in the external ear canal In order to identify chronic changes within the ear, careful assessment of the ear canal and tympanic membrane is essential. Where possible, examination of the canal and tympanum should be performed using high magnification and a good light source so that the features of the canal and the status of the tympanic membrane can be carefully assessed. Although this can be achieved using a hand-held otoscope, superior images can be achieved using video-otoscopy.
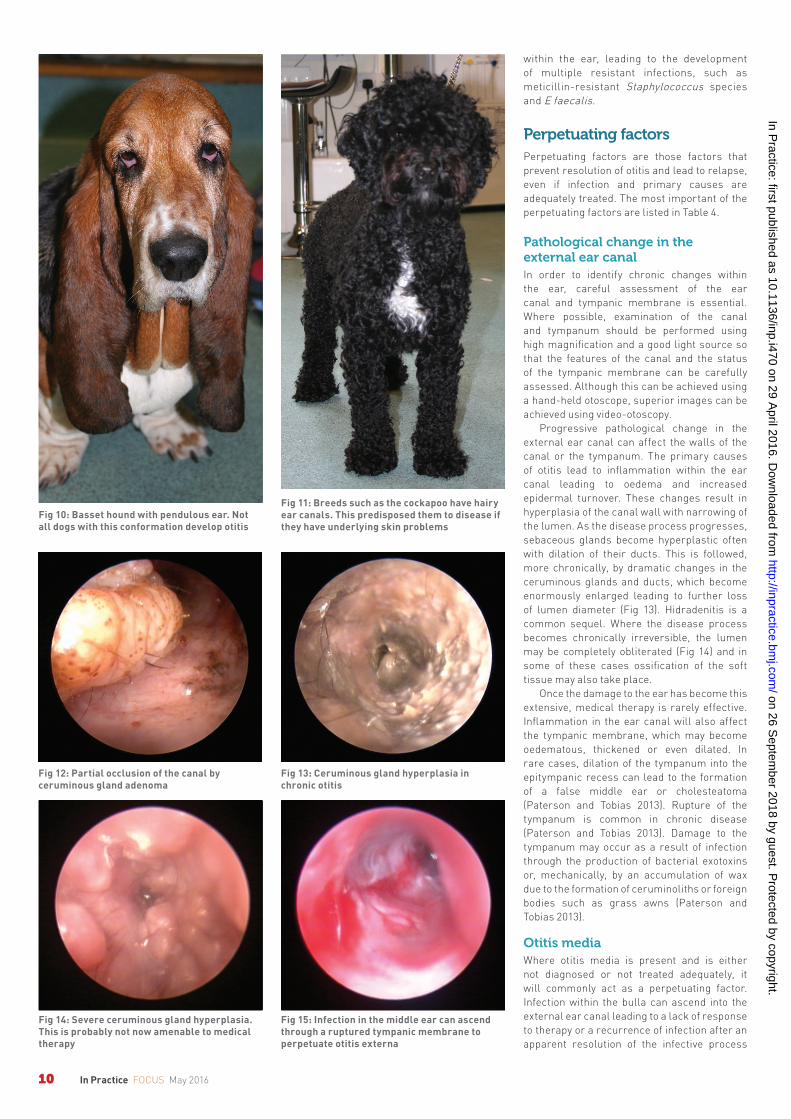
Progressive pathological change in the external ear canal can affect the walls of the canal or the tympanum. The primary causes of otitis lead to inflammation within the ear canal leading to oedema and increased epidermal turnover. These changes result in hyperplasia of the canal wall with narrowing of the lumen. As the disease process progresses, sebaceous glands become hyperplastic often with dilation of their ducts. This is followed, more chronically, by dramatic changes in the ceruminous glands and ducts, which become enormously enlarged leading to further loss of lumen diameter (Fig 13). Hidradenitis is a common sequel. Where the disease process becomes chronically irreversible, the lumen may be completely obliterated (Fig 14) and in some of these cases ossification of the soft tissue may also take place.
Once the damage to the ear has become this extensive, medical therapy is rarely effective. Inflammation in the ear canal will also affect the tympanic membrane, which may become oedematous, thickened or even dilated. In rare cases, dilation of the tympanum into the epitympanic recess can lead to the formation of a false middle ear or cholesteatoma (Paterson and Tobias 2013). Rupture of the tympanum is common in chronic disease (Paterson and Tobias 2013). Damage to the tympanum may occur as a result of infection through the production of bacterial exotoxins or, mechanically, by an accumulation of wax due to the formation of ceruminoliths or foreign bodies such as grass awns (Paterson and Tobias 2013).
Otitis mediaWhere otitis media is present and is either not diagnosed or not treated adequately, it will commonly act as a perpetuating factor. Infection within the bulla can ascend into the external ear canal leading to a lack of response to therapy or a recurrence of infection after an apparent resolution of the infective process
Fig 12: Partial occlusion of the canal by ceruminous gland adenoma
Fig 13: Ceruminous gland hyperplasia in chronic otitis
Fig 14: Severe ceruminous gland hyperplasia. This is probably not now amenable to medical therapy
Fig 15: Infection in the middle ear can ascend through a ruptured tympanic membrane to perpetuate otitis externa
Fig 10: Basset hound with pendulous ear. Not all dogs with this conformation develop otitis
Fig 11: Breeds such as the cockapoo have hairy ear canals. This predisposed them to disease if they have underlying skin problems
7-11 Paterson.indd 10 22/04/2016 10:54
on 26 Septem
ber 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inp.i470 on 29 April 2016. D
ownloaded from

11In Practice FOCUS May 2016
(Fig 15). Infection within the tympanic bulla itself leads to inflammation of the delicate mucoperiosteum lining of the bulla and the production of mucus, which traps infection within the bulla cavity, making it inaccessible to topical drugs.
Biofilms are known to develop within the middle ear of children (Bakaletz 2007) and several authors (Pye and others 2013) have suggested the same process occurs in the middle ears of dogs. A wide range of microbes are capable of forming biofilms, including many of the most common otic pathogens. Biofilms are formed when the microbes excrete an adhesive substance attracting other microbes to form a dense matrix on the wall of the tympanic bulla. This dense biofilm matrix acts as a colony rather than an isolated organism so that the outer layers of the bacteria protect those deep within the colony. Bacteria within biofilms are inherently much more resistant to antimicrobials than free-living planktonic organisms so that where biofilms are present infection can be perpetuated.
Appropriate measures to resolve infection in the middle ear include: flushing of the bulla and the instillation of appropriate drugs into the site, which may include biofilm-busting agents, anti-inflammatory drugs and antimicrobials. Where disease within the bulla is not managed, granulation tissue and bony change lead to irreversible damage that may only be successfully resolved by surgical
intervention in the form of a total ear canal ablation and bulla osteotomy.
ReferencesBAKALETZ, L. O. (2007) Bacterial biofilms in otitis media: evidence and relevance. Paediatric Infectious Disease Journal 26, 17-19BAXTER, M. & LAWLER, D. C. (1972) The incidence and microbiology of otitis externa of dogs and cats in New Zealand. New Zealand Veterinary Journal 20, 29-32 DICKSON, D. B. & LOVE, D. N. (1983) Bacteriology of the horizontal ear canal of dogs. Journal of Small Animal Practice 24, 413-421FERNANADO, S. D. A. (1966) A histological and histochemical study of the glands of the external auditory canal of the dog. Research in Veterinary Science 7, 116-119 GRIFFIN, C. E. (2010) Classifying cases of otitis externa the PPSP System. Proceedings of ESVD Workshop on Otitis. St HelensGRONO, L. R. (1970a) Studies of the microclimate of the external auditory ear canal in the dog. 1. Aural temperature. Research in Veterinary Science 11, 307-311 GRONO, L. R. (1970b) Studies of the microclimate of the external auditory ear canal in the dog. 3. Relative humidity within the external auditory meatus Research in Veterinary Science 11, 316-319 HARVEY, R. H., HARARI, J. & DELAUCHE, A. J. (2005) Microbiology of the canine external ear canal. In Ear Disease of the Dog and Cat. Manson. pp 35-38 HAYES, H. M., PICKLE, L. W. & WILSON, G. P. (1987) Effects of ear type and weather on the prevalence of
canine otitis externa. Research in Veterinary Science 42, 294-298PATERSON, S. (2002) A review of 200 cases of otitis externa in the dog. Veterinary Dermatology 14, 249 PATERSON, S. & TOBIAS, K. (2013) Conditions of the middle ear. In Atlas of Ear Disease of the Dog and Cat. Wiley-Blackwell. pp 107-123PYE, C. C., YU, A. A. & SCOTT-WEESE, J. (2013) Evaluation of the biofilm production by Pseudomonas aeruginosa from canine ears and the impact of biofilm on antimicrobial susceptibility in vitro. Veterinary Dermatology 24, 446-450 ROSSER, E. J. (1993) Diagnosis of food allergy in dogs. Journal of the American Veterinary Medical Association 203, 259-262 STOUT-GRAHAM, M., KAINER, R. A., WHALEN, L. R. & MACY, D. W. (1990) Morphologic measurement of the external ear canal of dogs. American Journal of Veterinary Research 51, 990-994 SARIDOMICHELAKIS, M. N., FARMAKI, R., LEONTIDES, L. S. & KOUTINAS, A. F. (2007) Aetiology of canine otitis externa: a retrospective study of 100 cases Veterinary Dermatology 18, 341-347 ZUR, G. L., LIFSHITZ, B. & BDOLAH-ABRAM, T. (2011) The association between the signalment, common causes of canine otitis externa and pathogens. Journal of Small Animal Practice 52, 254-258
Competing interests The author is a veterinary advisor to Dechra Animal Health, and has also accepted over the past five years hospitality or payment for work from Pfizer, Elanco, Bayer, Vetruus and CEVA.
doi: 10.1136/inp.i470
Table 4: Perpetuating factors in otitis externaPerpetuating factor Specific change
Pathological changes in the external ear canal
Changes in canal wall Inflammation causing failure of epithelial migration. Acute change: oedema, hyperplasia. Chronic change: proliferative change, canal stenosis, calcification of pericartilaginous fibrous tissue
Changes in glandular tissue Hyperplasia of ceruminous and sebaceous glands, hidradenitis
Changes in the tympanum Dilation, rupture, diverticulum (false middle ear – cholesteatoma)
Otitis media Acute Foreign material, mucopurulent exudate
Chronic Biofilm formation, granulation material, bony change in the bulla
Sue Paterson is a Cambridge university graduate. She is recognised as a RCVS and European Specialist in Veterinary Dermatology, and is currently president of the European Society of Veterinary Dermatologists (ESVD). She has lectured extensively both nationally and internationally and has written papers on a wide range of small animal and equine dermatology subjects and authored or co-authored three books on ear disease, the most recent of which, Otitis Externa, was published in 2014. She is a veterinary director at Rutland House Veterinary Hospital in St Helens where she is head of the busy dermatology department.
7-11 Paterson.indd 11 22/04/2016 10:54
on 26 Septem
ber 2018 by guest. Protected by copyright.
http://inpractice.bmj.com
/In P
ractice: first published as 10.1136/inp.i470 on 29 April 2016. D
ownloaded from