disparity impact statement (dis)
TRANSCRIPT
DISPARITY IMPACT STATEMENT (DIS)PREPARATION and REPORTING
WEBINAR
DSP: Tonia Gray and Tonia SchafferCAPT: Molly Lowe and Jessica GoldbergPEP–C: Phillip W. Graham and Janelle Armstrong-Brown
November 10, 2016
Agenda
• Describe connections between behavioral health disparities, health equity, and cultural competency
• Provide examples of training and technical assistance (T/TA) available to grantees from SAMHSA’s CAPT and Program Evaluation for Prevention Contract (PEP-C)
• Present components of a comprehensive Disparity Impact Statement
• Provide overview of the current status of PEP-C’s health disparities data collection instruments
3
The What of Addressing Behavioral Health Disparities:
Understanding the Language
4
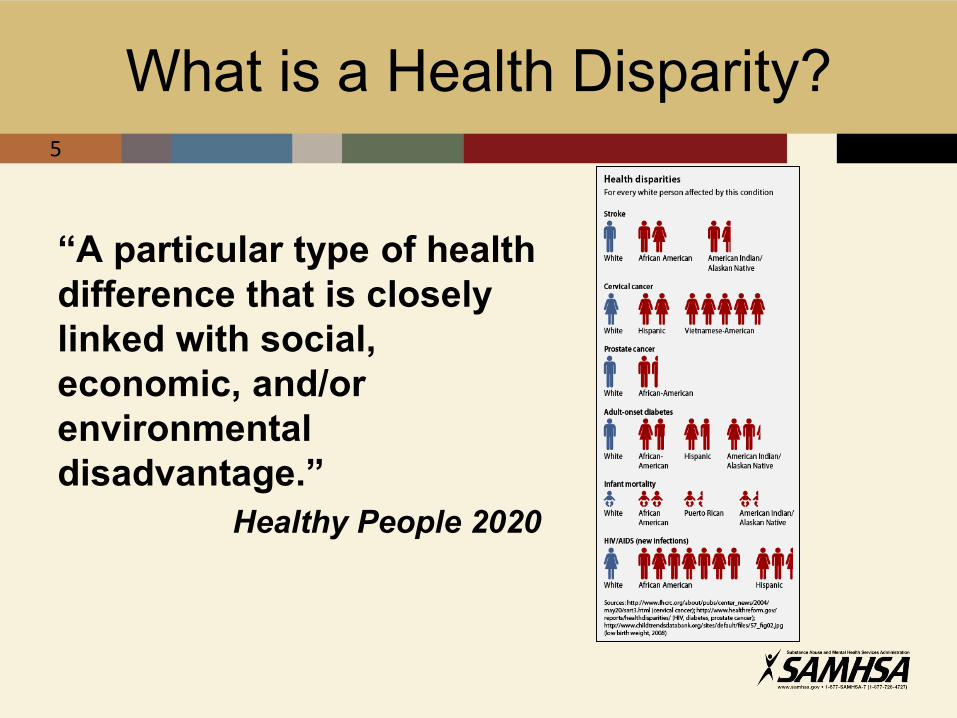
What is a Health Disparity?
“A particular type of health difference that is closely linked with social, economic, and/or environmental disadvantage.”
Healthy People 2020
5
Why Now? – Unfolding OpportunitiesKey Policy and Data Drivers
Healthy People 2020
Affordable Care Act
2010
National CLAS
Standards
6
HHS Action Plan to Reduce Racial and Ethnic Health Disparities
7
1. Assess and heighten the impact of all HHS policies, programs, processes, and resource decisions to reduce health disparities. HHS leadership will assure that:
(c) Program grantees, as applicable, will be required to submit health disparity impact statements as part of their grant applications. Such statements can inform future HHS investments and policy goals, in some instances, could be used to score grant applications if underlying program authority permits
7
Behavioral Health Disparities and the Road to Health Equity2
Reduction of Behavioral
Health Disparities
Increased Behavioral
Health Equity
8
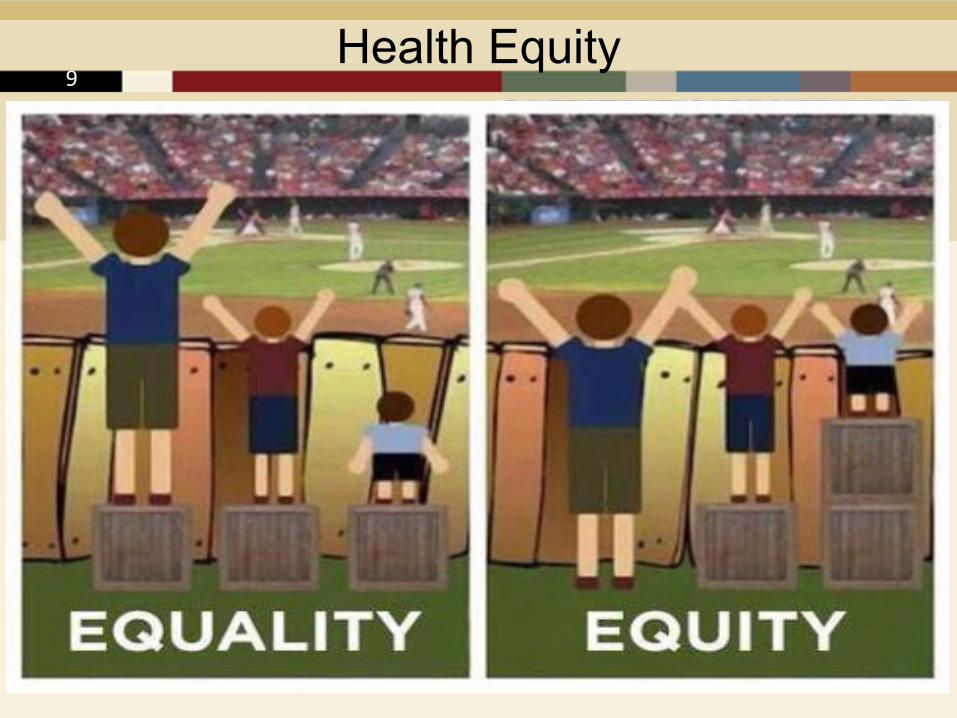
Health Equity9
The Connection Between Disparities and Health Equity
Identify Behavioral
Health Disparities
Implement Approaches to Reducing Behavioral
Health Disparities
Reduction of Behavioral
Health Disparities
Increased Behavioral
Health Equity
10
Role of Cultural Competency in Reducing Behavioral Health Disparities
Example of an Approach to Reducing Behavioral
Health Disparities
11

Enhanced National Culturally & Linguistically Appropriate Services (CLAS) Standards3
• Intended to advance health equity, improve quality, and help eliminate health care disparities
• Includes: Principal Standard (Standard 1) Governance, Leadership, and Workforce
(Standards 2-4) Communication and Language Assistance
(Standards 5-8) Engagement, Continuous Improvement, and
Accountability (Standards 9-15)
12
How Can the CAPT and PEP-C Help?
• CAPT: Focuses on general evaluation training and technical assistance
• PEP-C: Focuses on the national cross-site evaluations*
*For the PDO grant, the evaluation will be conducted in partnership with CDC
13
CAPT: Examples of T/TA
• Training for grantees and sub-recipients on approaches to understanding, identifying, and addressing disparities
• TA on developing a process for evaluating impact of CLAS standards on disparities
• Facilitating Evaluators’ Roundtables, Tribal Talking Circles, and other peer-sharing opportunities with grantees
• CAPT tips and tools on approaches to addressing disparities
14

Increasing Cultural
Competence to Reduce Health
Disparities
http://www.samhsa.gov/capt/
Tools from the CAPT15
PEP-C: Examples of T/TA
• PFS and SPF-Rx grantee and community outcomes reporting (including help selecting appropriate measures)
• PFS Quarterly progress reporting (e.g., health disparities-related SPF step activities)
• PFS Grantee-Level Instrument – Revised and Community-Level Instrument – Revised (e.g., intervention implementation, sub-recipient capacity needs, numbers reached)
16
Documenting Your Approach to Addressing Behavioral Health Disparities:
The Disparity Impact Statement
17
Three (3) Components of the Disparity Impact Statement (DIS):
1. Identification of subpopulations vulnerable to disparities (e.g. racial, ethnic, gender, age, sexual minority groups) to be engaged in grant activities
2. Proposed quality improvement plan (QIP) to decrease the differences in access, service use and outcomes among those subpopulations
3. Incorporation of the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care (National CLAS Standards) in the Quality Improvement Plan (QIP).
18
Purpose of the Disparity Impact Statement
• Track disparities in access, use and outcomes for racial, ethnic or sexual/gender minority subpopulations
• Use program performance data to implement a quality improvement (QI) process
• Implement new strategies, procedures, and organizational policies, building on the National CLAS Standards, as a means of improving the overall quality of program services and to ensure better access to, use of, and outcomes from those services for the identified disparate population(s)
19
Components of the DIS: Data
• Data to describe the prevention priority (identified in FOA)
• Select and describe the high need and low capacity communities
• Determine and describe which sub-populations are experiencing behavioral health disparities. Describe the “referent” population or comparison population.
20
Components of the DIS: Data (cont.)
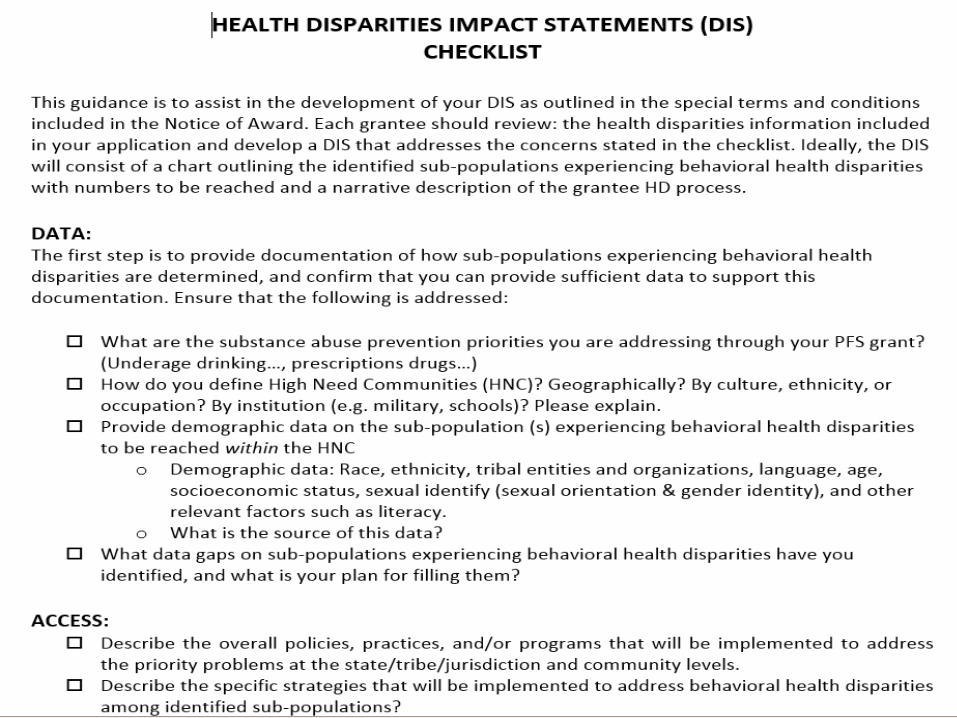
• What substance abuse prevention priorities are you addressing through your grant (e.g., prescription drug misuse and abuse among 12- to 25-year-olds)?
• How do you define high-need communities (HNC)? Geographically? By culture, ethnicity, or occupation? By institution (e.g., military, schools)?
21
• Provide demographic data, including data sources, on the sub-population(s) experiencing behavioral health disparities you will reach withinthe HNC : include race/ethnicity, age, gender, sexual orientation, (other data)
• What data gaps for these sub-populations have you identified, and what is your plan for filling them? Describe how program will address and improve access, use and outcomes of vulnerable population.
22
Components of the DIS: Data (cont.)
Health Disparities Data Sources
• National sources• National surveys (e.g. NSDUH, MTF, BRFSS, YRBSS)• Archival data systems (e.g. TEDS, CDC Wonder) • Census data
• Local sources• State and community surveys• State and community hospitals, poison control centers, ER• Focus groups, key informant interviews
• Agency and program level data• Prescription Drug Monitoring Program (PDMP)
data
23
Health Disparities Data Sources
CAPT Substance Abuse and Prevention Planning and Epidemiology Tool (SAPPET) compiles data from various national sources
• National surveys (NSDUH, BRFSS, YRBSS)• National archival data systems (TEDS, CDC
Wonder, FARS)• Special population data
• Tribal data from national sources
Website: https://sappet-epi.com/(password: sappet)
24
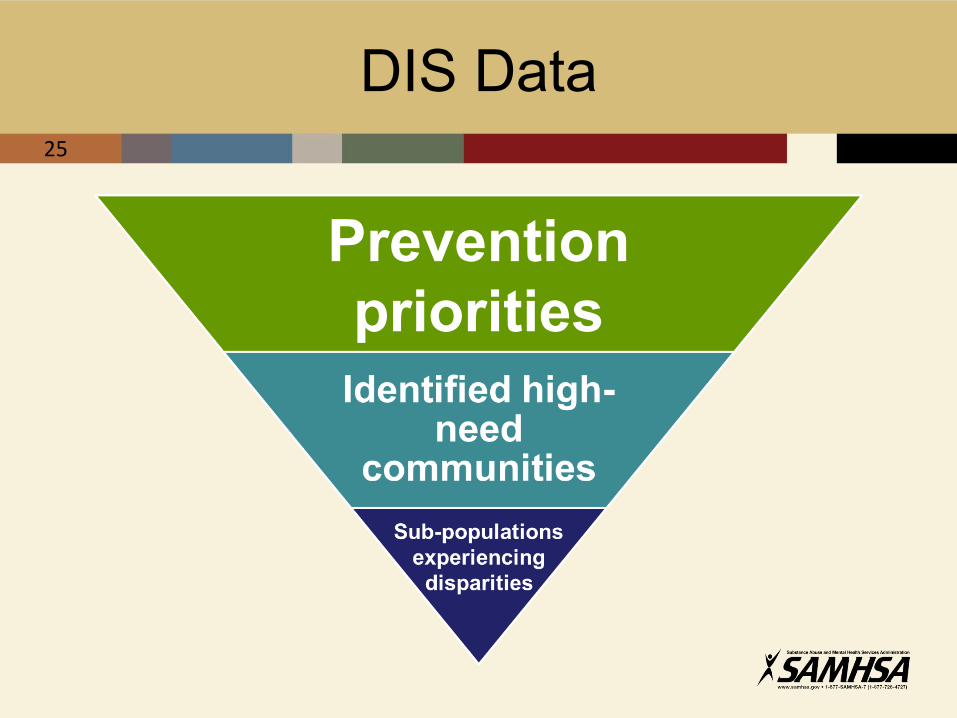
DIS Data25
Prevention priorities
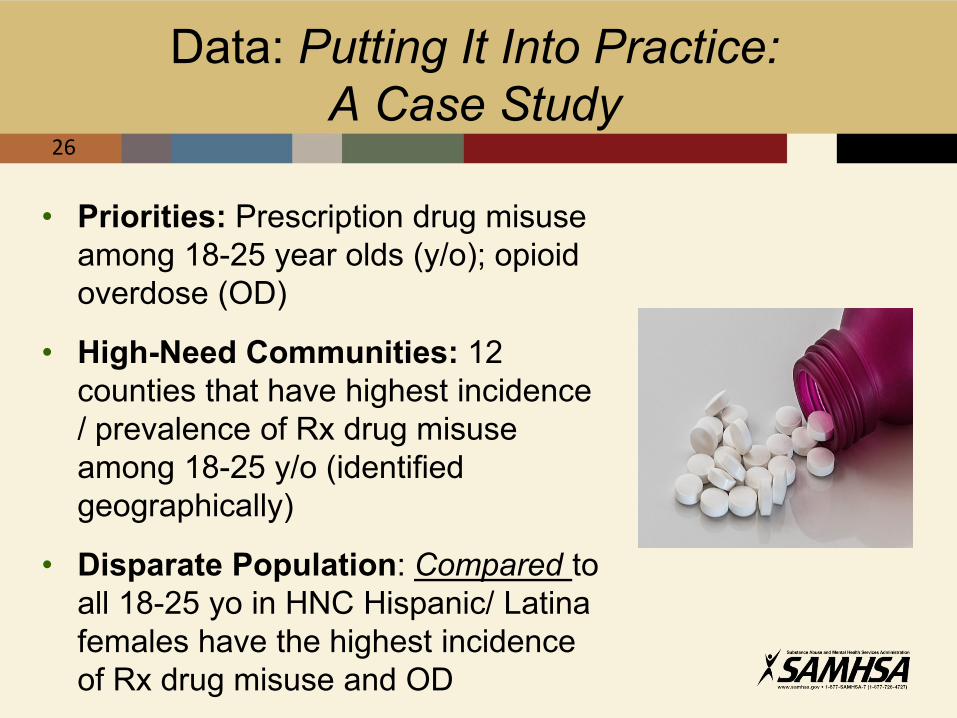
Data: Putting It Into Practice: A Case Study
• Priorities: Prescription drug misuse among 18-25 year olds (y/o); opioid overdose (OD)
• High-Need Communities: 12 counties that have highest incidence / prevalence of Rx drug misuse among 18-25 y/o (identified geographically)
• Disparate Population: Compared to all 18-25 yo in HNC Hispanic/ Latina females have the highest incidence of Rx drug misuse and OD
26
Components of the DIS: Quality Improvement Plan (QIP)
• Describes how you will use your program (GPRA) data on access, use, and outcomes to reduce disparities. Includes:
strategies for how adjustments will support efforts to reduce disparities for the identified sub-populations
methods for developing and implementing policies and procedures to ensure adherence to the CLAS Standards and provide effective services
27
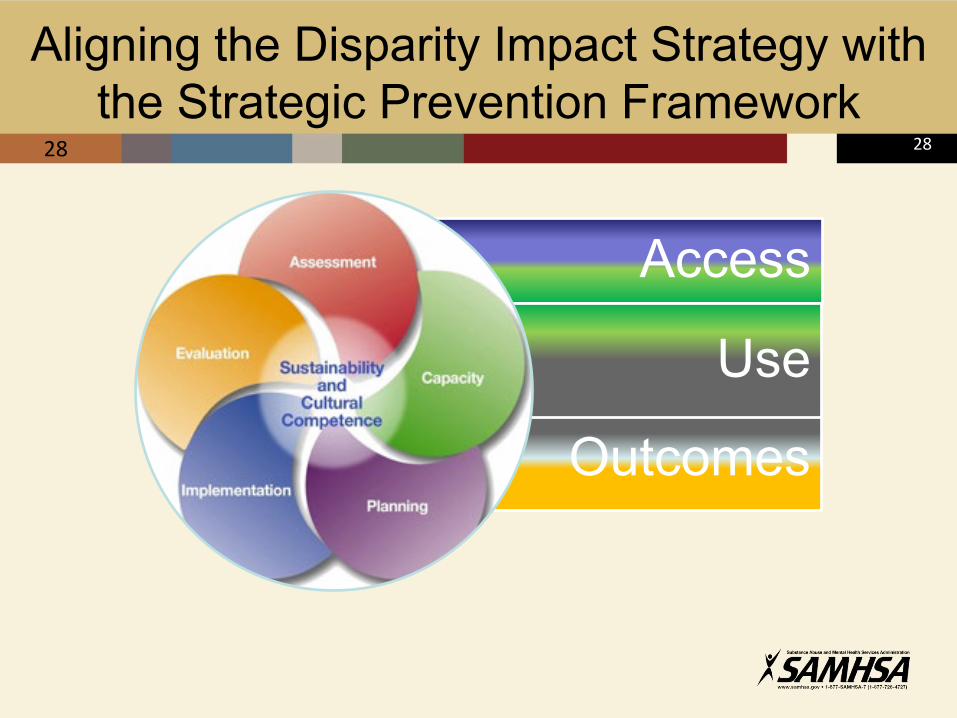
Aligning the Disparity Impact Strategy with the Strategic Prevention Framework
28
Outcomes
Access
Use
28
QIP Component
• What are the prevention needs of your identified sub-population(s)?
• What strategies are you implementing to address identified priorities, and which ones will you implement to address disparities among identified sub-populations?
• How will you integrate your approach to addressing disparities at each step of the SPF?
• How will you develop and implement policies/ procedures to ensure adherence to the CLAS standards?
30

Putting It Into Practice:A Case Study
Need: • Hispanic females experience higher rates of
Rx drug misuse/abuse than their peers
• Opioid overdose incidents have increased among Hispanic females
• Hispanic females are significantly less likely to access prevention services than their peers
31
Putting It Into Practice:A Case Study
Strategy: Statewide media campaign for 18-25 year olds to increase perception of harm and readiness to address the issues; tailor campaign to ensure representation of and reach to Hispanic females (CLAS Standard 5-8)
Specific strategy for sub-population of focus:Provide training in opioid overdose prevention education (including the use of naloxone) to first responders, healthcare providers and staff working at organizations with access to Hispanic females
32
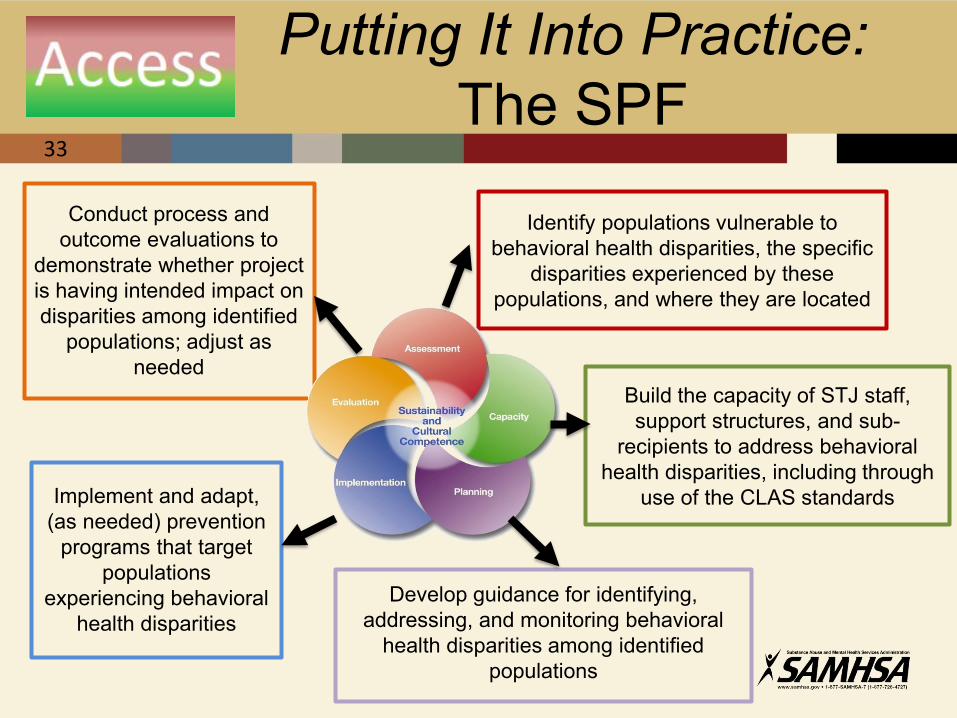
Identify populations vulnerable to behavioral health disparities, the specific
disparities experienced by these populations, and where they are located
Build the capacity of STJ staff, support structures, and sub-
recipients to address behavioral health disparities, including through
use of the CLAS standards
Develop guidance for identifying, addressing, and monitoring behavioral
health disparities among identified populations
Implement and adapt, (as needed) prevention
programs that target populations
experiencing behavioral health disparities
Conduct process and outcome evaluations to
demonstrate whether project is having intended impact on disparities among identified
populations; adjust as needed
Putting It Into Practice: The SPF
33
Putting It Into Practice: CLAS Standards
Governance, Leadership, and Workforce (Standards 2-4):
• Identify, engage, and track collaborations with “non-traditional” community partners (e.g. people who use drugs, substance use treatment providers)
Communication and Language Assistance (Standards 5-8):
• Customize and track customizations made to prevention materials to be inclusive of Hispanic females
• Advertise campaign where the sub-population spends time
34
Putting It Into Practice: CLAS Standards (cont.)
Engagement, Continuous Improvement, and Accountability (Standards 9-15):
• Collect data on impact of your approaches and share results with Hispanic females (e.g. in college, out of college, workplace)
• Partner with community members to design, implement, and evaluate policies, practices, and services to ensure cultural and linguistic appropriateness.
35
QIP Component
• What is your process for collecting data on sub-populations reached, including the sources of data you will use and the frequency of data collection?
• How will you monitor implementation of the grant and the use/reach of your policies, practices, and/or programs?
36
Putting It Into Practice:A Case Study
• Number of Hispanic females you propose to serve
• Data sources you propose to use to document reach (quantitative and qualitative)
• Tracking and monitoring of approaches to involve Hispanic female adults in prevention efforts
• T/TA provided to sub-recipients on engaging the population
37
QIP Component
• How will you use data to evaluate processes and/or make programmatic adjustments to address disparities experienced by identified sub-populations?
• How else do you intend to use programmatic data to demonstrate the impact of your efforts (e.g., tracking and monitoring impact of Enhanced CLAS standards)?
38
Putting It Into Practice:A Case Study
Document how you will :• Track adaptations made to strategies, including use
of CLAS standards, for Hispanic females
• Demonstrate the impact of the media campaign and other strategies (e.g., numbers reached, dosage and frequency of environmental strategies)
• Report all required data to PEP-C
• Report the programmatic progress in MRT
39
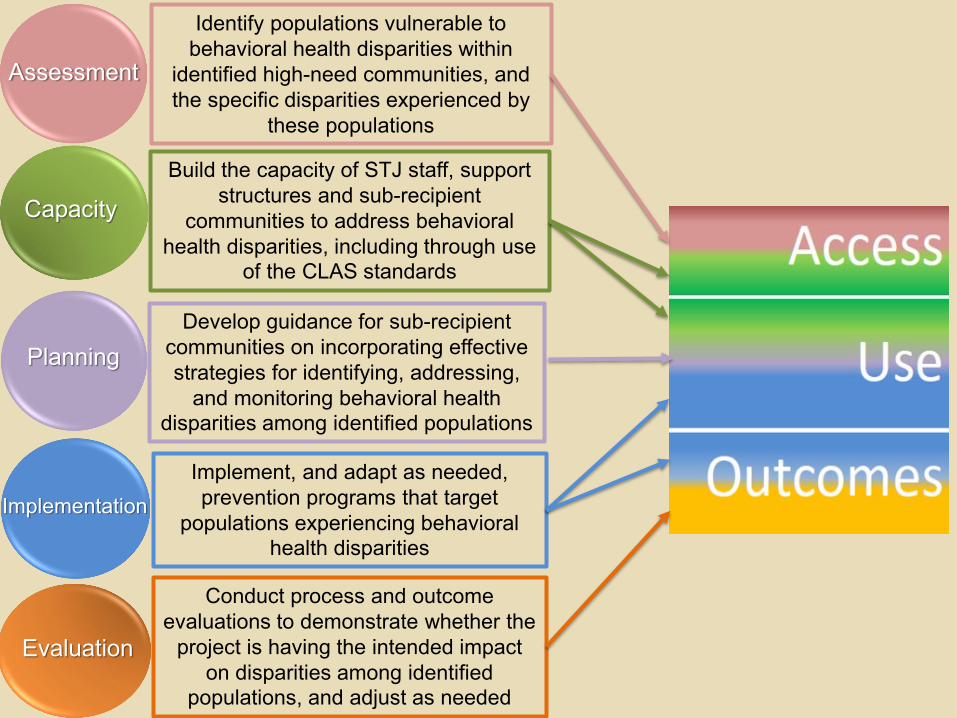
Identify populations vulnerable to behavioral health disparities within
identified high-need communities, and the specific disparities experienced by
these populations
Build the capacity of STJ staff, support structures and sub-recipient
communities to address behavioral health disparities, including through use
of the CLAS standards
Develop guidance for sub-recipient communities on incorporating effective strategies for identifying, addressing,
and monitoring behavioral health disparities among identified populations
Implement, and adapt as needed, prevention programs that target
populations experiencing behavioral health disparities
Conduct process and outcome evaluations to demonstrate whether the
project is having the intended impact on disparities among identified
populations, and adjust as needed
Assessment
Capacity
Planning
Implementation
Evaluation
Questions?41
Reporting on Health Disparities: SAMHSA’s Cross-Site Evaluations
42

Cross-Site Evaluation Data Collection
PFS Grantees• PFS 2016 Grantees will
complete data collection protocols and instruments from the current PFS cross-site evaluation.
SPF-Rx & PDO/Naloxone Distribution Grantees • Instrumentation for SPF
Rx and PDO is currently under development.
• PEP-C will provide more information on health disparities measures and data collection during the March/April new grantees meeting.
The following slides focus on data collection for Partnerships for Success.
General Evaluation Measures
• Improvements in outcomes in behavioral health disparities as a result of intervention efforts
• Use of prevention efforts by populations experiencing behavioral health disparities
• Strategies to increase access to populations experiencing behavioral health disparities
45
General Evaluation Measures for Health Disparities
PFS• What strategies/activities have
you undertaken to increase the access of your Health Disparities populations to your interventions?
• How did you apply each of the CLAS standards?
SPF-Rx & PDO• Describe the overall policies,
practices, and/or programs that will be implemented to address the priority problems at the state/tribe/jurisdiction and community levels.
• Describe a plan to develop and implement policies/procedures to ensure adherence to the (CLAS) Standards
46
General Evaluation Measures for Health Disparities (cont.)
Partnerships for Success• What are the demographics of the
individuals/population you served/ reached with your interventions?
• How many individuals from your target health disparities population did you serve/reach?
SPF-Rx & PDO• Describe your process for
collecting data (demographic data) on sub-populations reached? Include data sources and the frequency of data collection (annual, bi-annual, etc.)
• How will you monitor the implementation of the grant and the use/reach of your policies, practices, and/or programs to identified sub-populations in the grant program?
46
General Evaluation Measures for Health Disparities (cont.)
PFS• Has your target health disparities
population improved on your target outcomes (relative to some reference group)?
• What data sources do you have to provide information on alcohol use or prescription drug misuse; related risk and protective factors; and related consequences (substance use related overdoses, arrests, ER visits, school suspensions/expulsions)? Is that data broken out for your target health disparities group?
SPF-Rx & PDO• Has your target health disparities
population improved on your target outcomes (relative to some reference group)?
• Describe how you will use data on outcomes regarding sub-populations experiencing behavioral health disparities (race, ethnicity, LBGT status, etc.) to evaluate processes and/or make programmatic adjustments to address identified priorities and issues (high need, underage drinking, prescription drug abuse)
47
PEP-C PFS Data Collection Instruments – Health Disparities
Grantees and sub-recipients provide data related to their health disparities-focused activities through:• Quarterly Progress Reports: Grantee accomplishments and
barriers related to health disparities
• Community Outcomes (possibly)
• Grantee-Level Instrument – Revised (GLI-R): Target populations, cultural competence
• Project Director (PD) Interview: Health disparities target populations and plans/processes
• Community-Level Instrument – Revised (CLI-R): Population targets, demographics on intervention use, health disparities accomplishments
48
PFS Quarterly Progress Reports
Accomplishments for Health Disparities at Each SPF Step • Assessment: Defining and identifying health disparities, obtaining
data to capture health disparities
• Capacity: Creating partnerships, delivering training
• Planning: Consider health disparities
• Implementation: Serving vulnerable populations, adapting services and increasing access and availability
• Evaluation: Assessing changes in # served and outcomes
• Cultural Competence: Including health disparity populations in planning, integrating CLAS standards
• Sustainability: Planning for sustainability in addressing health disparities
46
PFS Quarterly Progress Reports (cont.)
Barriers for Health Disparities at Each SPF Step • Assessment: Difficulty defining and identifying health
disparities, or obtaining data to capture health disparities
• Capacity: Difficulty creating partnerships, low sub-recipient capacity, difficulty providing/finding relevant training
• Planning: Difficulty considering health disparities in planning
• Implementation: Lack of interventions for target populations, difficulty adapting interventions
• Evaluation: Lack of data on target population
• Cultural Competence: Difficulty engaging health disparity populations in SPF steps, applying CLAS standards
47
PFS Grantee- and Community-Level Instruments
• Grantee-Level Instrument – Revised (GLI-R)• Q19: Demographic and cultural categories targeted (overall) • Q20: Enforcement of cultural competence standards• Q21: Assessment of cultural appropriateness of prevention
materials• Q22: Barriers to improving cultural competence
• Community-Level Instrument – Revised (CLI-R)• Q7: Health disparity-related accomplishments• Q17: Demographic and cultural categories targeted (overall) • Q19: Community density (urban/rural)• Q23: Training needed/received (cultural competence and health
disparities)• Q191, 200, 201: Intervention adaptations
49
PFS Project Director Interview
• What health disparities are you addressing?
• What is your plan for addressing health disparities at the grantee level? How will you ensure that strategies reach populations affected by health disparities?
• How are you planning to support sub-recipients in addressing health disparities?
51
Limitations of PEP-C PFS Reporting Relative to Health Disparities
• SELF-REPORT: Dependent on information provided by grantees and community sub-recipients
• ACCESS: Only general information on where (zip code) and to whom interventions are targeted
• USE: Numbers reached/served for only some sub-population demographics—others not asked (e.g., LGBTQ); sub-recipients’ limited knowledge of demographic breakdown of intervention participants (especially environmental)
• OUTCOMES: Dependent on grantee reporting of community outcomes for targeted health disparities groups (and some comparison sub-populations); limited data availability by relevant sub-populations
53

Questions?49
Next Steps
DIS STATEMENTS DUENovember 30, 2016
50
References
1. U.S. Department of Health and Human Services, Healthy People 2020 (n.d.). Disparities. Retrieved from http://www.healthypeople.gov/2020/about/disparitiesAbout.aspx.
2. U.S. Department of Health and Human Services (2012). HHS action plan to reduce racial and ethnic health disparities. Retrieved from http://www.minorityhealth.hhs.gov/npa/files/Plans/HHS/HHS_Plan_complete.pdf
3. SAMHSA’s Center for the Application of Prevention Technologies (2012). Cultural Competence. Retrieved from http://captus.samhsa.gov/access-resources/about-strategic-prevention-framework-spf#cultural.
51