1
COMMUNITY ENGAGEMENT PROJECT: NIMHE Mental Health Programme)
REPORT OF THE COMMUNITY LED RESEARCH PROJECT FOCUSSING ON ASIAN ELDERS
AND CARERS ACCESS TO MENTAL HEALTH SERVICES
BY SUBCO TRUST LTD
COMMUNITY IN EAST LONDON
SOUCHEIN
Conducted by
Taskin Saleem - Safir Ahmed - Shabana Asif - Mohammed Ofu - Hitesh Patel
Ali Ahmed - Khatija Cadinouche - Maryam Athman - Mohammed Akhtar -
Thakorbhai Patel - Naheed Anwar - Maryam Mahmood - Dinesh Patel - Hetal Patel
DATE: MARCH 2008
Funded by the (NIMHE managed and supported by
The Centre for Ethnicity and Health, University of Central Lancashire.
Care Services Improvement Partnership

2
Project Team
Profiles of some of the researchers
Taskin Saleem - I have (BA Hons) Education & Sociology, a Diploma in Social Work, and NVQ
Level 4 in Management. I am currently the Chief Executive of SubCo and I am also working as a
personal tutor to students on the Social Work degree course at the University of East London. I am
also a Non Executive Director of the Newham Primary Care Trust, as well as a Director of the
Renewal Programme and the Chair of Newham Carers Network in Newham. I have been working
with SubCo for the last 13 years. Before working at SubCo I had a range of experiences working
with the Social Services Department as a Racial Equality Officer providing services for black
minority groups; in various voluntary organisations as a Community Advice Worker, Development
Worker, and Youth Worker. I have also undertaken voluntary work in a range of voluntary
organisations over the years.
My role was to establish the project and coordinate it, provide support and advise the community
researchers, volunteers and Steering Group and ensure good communication flows throughout the
life of the project. Another important aspect was to identify future areas of work and sustainability.
My name is Safir Ahmed, I have grown up, live and work in East London. I work in the sports,
community and leisure industry. Working on this project helped give me a better understanding of
Mental Health Issues and how they can affect people. I found it to be a valuable learning
experience. I would like to share our findings and create more awareness and try to reduce any
Mental Health related stigmas within the Asian community. This is only the beginning and I hope to
see the ripples of this project reach those who are in a position to help make a change.
My name is Shabana Asif. I have been working for SubCo for past 3 years. In the past I have been part of projects organised by SubCo relating to Mental Health Issues. This project was somehow different from the previous projects as it required research. I was happy to be part of the project as I saw this as an opportunity to learn and raise awareness of Mental Health Illnesses. Since I spoke various Asian languages and was given training my interest in this project grew more and more. This project also gave me the chance to work one-to-one with the users and get their views on what they would like and how they feel. I hope this research will continue in a form of services, rather than just remaining as findings.
My Name is Hitesh Patel, not a lot of people know that but it is, my job which not a lot of people know is finance and admin for SubCo Trust. I was born in Africa in 1960 and came to England on one very cold November day in 1969. I took part in this research by listening and recording the experiences of people who had in some way in their life been through emotional or mental distress but had to cope and are still coping. I was flabbergasted but not surprised to learn that nearly all the people surveyed had very little or no idea of the services being offered around mental health or dementia which could be easily accessed by anyone regardless their age, gender, ethnicity or mobility. Although very reluctant to help with the survey at first I was very happy that I took part in it because it showed me that what we sometimes take for granted cannot be said the same for the older less fortunate in our community and with this in mind surveys are a positive way in hearing silent voices.
I am Mohammed Ofu, 32 years of age and currently the Day Care manager for SubCo Day Care Centre. I volunteered to participate in the Souchein project and carried out interviews as well as assisting the focus groups. I am multilingual and was able to communicate with the participants in both English and Swahili. I found the Souchein project to be most interesting especially due to the fact that I have a Mental Health Nursing Background. The project helped me to better my

3
knowledge on the day to day issues concerning elderly and isolation. This was a great experience in which participants were given the chance to talk about their problems in an appropriate setting.
My name is Khatija Cadinouche and I am a 23 year old Holistic Care Support Worker for SubCo
Day Care Centre. I am currently studying an NVQ in Health & Social Care and have a previous
background in Psychology. I offered my assistance to the Souchein project via conducting several
interviews with Asian elders and carers. I found participating in this project to be an insightful
experience as I had the opportunity to interact with the individuals on a one-to-one basis
concerning mental health and isolation. In depth conversations with the group of individuals has
made me more perceptive to their thoughts and feelings concerning such issues. I hope that the
project has provided some input towards how these issues can be dealt with.
My Name is Ali Ahmed and I am a 20 year old Holistic Care Support Worker for SubCo Day Care Centre. I am also currently studying for an NVQ3 in Health & Social Care. I volunteered to take part in the Souchein project by contributing to interviews and focus groups. I was able to communicate with the individuals in Urdu, Hindi and Punjabi. The project was highly moving as it has given me an in depth insight into the regular thoughts of individuals in this group and the impact of isolation on their lives. I particularly found the focus groups of interest as it gave the individuals the chance to interact with others who experience similar feelings thus allowing them to elaborate and share their thoughts.
I am Maryam Athman, I am 32 and I am working as a Holistic Care Support Worker for SubCo Day Care Centre. I took part in the Souchein project and conducted interviews in Swahili and English. It was an enlightening experience to take part in such a project as I was given the chance to find out about how the elderly feel in terms of such mental health issues. It was good that they were given the opportunity to discuss and communicate their issues within such a setting.
My name is Mohammad Akhtar & I voluntarily participated in the Souchein Project. Several group meetings were arranged and we were well informed concerning the project. There was a wide range of questions to which the elders responded in an open manner and were positive towards the fact that we were interested in ways to reduce their isolation and loneliness. I found it to be very informative and knowledgeable after which the problems can be addressed.
I am Thakorbhai Patel and I am 61 years of age. I have escorting and day care duties for SubCo day care centre. I also run the exercise group and provide Reiki for service users. I took part in the Souchein project and helped with interviews requiring a Gujerati speaker. I found the project to be most beneficial to the elders as it gave them the chance to talk about their problems both in a group setting and in a one-to-one format. The elders had the opportunity to speak to people they have confidence in and can trust.
My name is Hasumati Patel and I am 62 years old and I volunteer at SubCo day care centre. I enjoyed helping out with the Souchein project very much. I can speak Gujerati and Hindi and helped with several interviews. It was a very good experience for me as I was able to understand the problems they go through in more depth. It has definitely opened my eyes to the effects of isolation on mental health.
I am Hetal Patel and I am 24 years old. I am doing my placement at SubCo for my NVQ2 course in Health and Social Care. I am fluent in both Hindi and Gujerati and took part in several interviews as well as focus groups. The Souchein project was very enlightening in terms of understanding isolation and its effect on this particular group of people. I was not aware of the extent of the effects within the Asian community so I found it to be an insightful experience. It was good to gain such knowledge so that these issues can be aided.

4
My name is Naheed Anwar and I have worked in the voluntary sector for over ten years. My work has included day care work with Asian elders. I previously worked with SubCo trust as a day care worker, yet have continued to work with the organisation on a voluntary basis - I am now the Vice Chair. Currently, I work as a carer’s rights officer for Newham Carers Network, which is a local organisation providing advice, information and support to carers. My involvement in the Souchein project included contacting Asian elders and their carers and interviewing them in focus groups about their knowledge of the many effects of mental health problems. This experience enabled me to understand that Asian people have many barriers preventing them from accessing mental health services. For example, cultural issues such as the stigma associated with seeking help and a lack of understanding and knowledge of mental health issues.
My name is Maryam Mehmood I work as an Asian Carers Rights/Groups Worker at Newham Carers Network, which is part of the Renewal Programme. At Newham Carers Network we provide information, advice and support for carers from all communities. As an Asian Carers Rights/ Groups worker my work involves providing Asian Carers with support, advice, outreach, advocacy and access to leisure opportunities. Therefore, improving accessibility to services and quality of life for older people in the community by supporting older people. My involvement in the Souchein project was to help with focus group interviews and one to one interviews. The purpose of the interviews was to help understand how much knowledge Asians elders have of mental health problems and services available. It was very important for me to make sure that the client understood what I was asking them. It was also important to make the client aware that all was kept confidential. I also felt that it was important for me to make sure the client felt safe and comfortable. Taking part in the Souchein project helped me understand what problems Asian Elder face in accessing mental health services.
Acknowledgements
SubCo Trust
Taskin Saleem, Safir Ahmed, Shabana Asif, Mohammed Ofu, Hitesh Patel, Ali Ahmed, Khatija Cadinouche, Maryam Athman, Mohammed Akhtar, Thakorbhai Patel, Dinesh Patel, Hetal Patel, Naheed Anwar, Maryam Mahmood.
UCLAN – Imran Mirza and the Team
Steering Group
Ian Kennedy – Group Manager: Older People & General Services, Michael McGhee –General
Manager: Older persons Services Jane Tilston – Integrated Commissioning Manager Older
People (until November 2007), Sylvia West, Commissioning Consultant (from November 2007,
Taskin Saleem – Chief Executive, SubCo Trust and coordinator of the Community engagement
Research Project, Tim Bishop, FIS, Denise Bobb, Race Equality Lead, Ghulam Hussain - Service
User, The Safir Ahmed, Community Engagement Research Worker, Shabana Asif, Community
Engagement Research Worker, Thakorbhai Patel, Community Engagement Research Worker.
Newham Carers Network, Katherine Road 50+ Men’s Group, Punjabi Women’s Group Tej Bhavan –LHA ASRA,

5
Contents
Page
Cover Page......................................................................................................................................1
Project Team – Profiles of Researchers...........................................................................................2
Acknowledgements..........................................................................................................................4
Contents...........................................................................................................................................5
List of Figures ..................................................................................................................................7
Executive summary..........................................................................................................................9
Section 1
Introduction..............................................................................................................................14
1.1 The key ingredients of the model ......................................................................................15
1.2 The UCLan Community Engagement Team......................................................................17
1.3 Programme outcomes .......................................................................................................18
1.4 Background Information about Newham ...........................................................................19
Table 1 Smiling More Often Report .........................................................................................19
Table 2 Older people in Newham by age and gender – mid 2002...........................................20
Table 3 Older people in Newham by age and gender – 2011 projections ...............................20
Table 4 Older people in Newham by age and ethnic origin .....................................................21
Section 2
The Focus of this Report..........................................................................................................23
2.1 SubCo Trust and who we are............................................................................................24
2.2 Methods.............................................................................................................................25
2.3 The Questionnaire.............................................................................................................26
2.4 The Focus Groups.............................................................................................................27
2.5 The Steering Group...........................................................................................................27
2.6 The Community Engagement Research Team .................................................................28
2.7 Ethics ................................................................................................................................29
Section 3
Questionnaire Results.............................................................................................................29
3.1 Photos...............................................................................................................................31
3.2 Quantitative Data Graphs..................................................................................................32
3.3 Quantitative Data Open Questions....................................................................................39
6
Section 4
Qualitative Data ......................................................................................................................40
4.1 Focus Groups....................................................................................................................40
4.2 Punjabi Women’s Group Focus Group..............................................................................40
4.3 Asian Carers Focus Group................................................................................................43
4.4 Asian Elders Focus Group.................................................................................................44
4.5 Katherine Road Men’s 50+ Focus Group ..........................................................................46
Section 5
Themes arising from discussions at the Focus Groups...........................................................49
5.1 Discussion and Impact......................................................................................................51
Section 6
Reflection................................................................................................................................53
Section 7
Recommendations ..................................................................................................................54
Section 8
References..............................................................................................................................55
Section 9
Appendix:
9.1 Souchein Poster and Booking Form ..................................................................................56
9.2 Souchein Questionnaire.....................................................................................................57
9.3 Souchein Focus Group Questions .....................................................................................61
9.4 Souchein Consent forms for 1:1 Questionnaires and Focus Groups .................................62
9.5 Guidelines for 1:1 interviews..............................................................................................63
9.6 Application for Ethical approval .........................................................................................64
9.7 Steering Group – Terms of Reference ..............................................................................74

7
Contents
List of Figures: Page
Fig.1 Gender..................................................................................................................................32
Fig.2 Age........................................................................................................................................32
Fig.3 Ethnicity ................................................................................................................................32
Fig.4 Where you born in the UK.....................................................................................................32
Fig.5 If no, how long have you lived here.......................................................................................32
Fig.6 Are you a (citizenship)...........................................................................................................32
Fig.7 First language spoken or signed ...........................................................................................32
Fig.8 First language written............................................................................................................32
Fig.9 Which languages are you fluent in ........................................................................................ 33
Fig.10 Which languages are you fluent in written...........................................................................33
Fig.11 Marital Status ......................................................................................................................33
Fig.12 Accommodation ..................................................................................................................33
Fig.13 What is your place of residence ..........................................................................................33
Fig.14 How many people are there living in your house ................................................................33
Fig.15 Do you speak to the people living in your home..................................................................33
Fig.16 If yes, do you manage to speak to them on a regular basis................................................33
Fig.17 How long do your conversations last...................................................................................34
Fig.18 How often do you go out in a week .....................................................................................34
Fig.19 Do you have visitors that visit you at home.........................................................................34
Fig.20 Do you feel lonely................................................................................................................34
Fig.21 If yes, how often..................................................................................................................34
Fig.22 How lonely do you feel ........................................................................................................34
Fig.23 Is there anything that you do to reduce your loneliness ......................................................34
Fig.24 When you are lonely what do you feel ................................................................................34
Fig.25 Do you know of any services that are available to you........................................................35
Fig.26 Would you like help.............................................................................................................35
Fig.27 Have you or your friends/ relatives ever suffered from mental health/ stress related issues35
Fig.28 Have you or your friends/ relatives ever suffered from the following mental health/ stress
related issues.................................................................................................................................35
Fig.29 Have you or anyone you know ever used any of the following services to help you with
these issues...................................................................................................................................35
Fig.30 Were you or anyone you know given enough time to discuss your/ their condition and
treatment........................................................................................................................................35
Fig.31 What type of treatment have you or anyone you know received.........................................35

8
Fig.32 Where you or anyone that you know provided with an advocate or interpreter...................35
Fig.33 If not, would you have wanted one......................................................................................36
Fig.34 Did you or anyone you know have trust and confidence in the service provider .................36
Fig.35 Overall how satisfied are you or anyone you know with the help that you received from
these services................................................................................................................................36
Fig.36 How do you think these services can be improved .............................................................36
Fig.37 Do you know of any mental health services that are available in Newham.........................36
Fig.38 Would you like to attend day activities if they were available to you ...................................36
Fig.39 What is your religion............................................................................................................36
Fig.40 Have you ever used any of the following alternative therapies ...........................................36
Fig.41 Sexuality .............................................................................................................................37
Fig.42 Do you have a disability ......................................................................................................37
Fig.43 Felt lonely............................................................................................................................37
Fig.44 Women who felt lonely were ...............................................................................................37
Fig.45 How often do you feel lonely ...............................................................................................37
Fig.46 When lonely they felt...........................................................................................................37
Fig.47 Second Language...............................................................................................................37
Fig.48 The people who have or know someone who has suffered from mental health/ stress
related issues but did not know about available services...............................................................37
Fig.49 Suffered from mental health/ related issues........................................................................38
Fig.50 Where you or anyone you know provided with an advocate or interpreter..........................38
Fig.51 If not would you have wanted one.......................................................................................38
Fig.52 How do you think these services can be improved .............................................................38
Fig.53 Would you attend day care activities if they were available to you......................................38
Fig.54 Have you ever used the following alternative therapies ......................................................38
Fig.55 Where do you go.................................................................................................................38
Fig.56 If yes, who...........................................................................................................................38
Fig.57 How Often ...........................................................................................................................39
Fig.58 If yes, what do you do .........................................................................................................39

9
EXECUTIVE SUMMARY
Aims and Objectives
The project seeks to identify and engage local groups that are under-represented in mental health services. The work is a collaboration between, UCLAN, DOH, CSIP and SubCo. The project ultimately aims to:
• Enhance social inclusion for these individuals • Encourage the development of social capital projects through engagement with
communities and Providers of services in Newham
Support was provided by the UCLAN Support Worker and the Steering Committee. The research
team’s weekly meetings also provided individual and team support and supervision through
SubCo Trust.
The finding of the community engagement research project has highlighted a number of areas that need to be addressed in order to deliver equal and accessible services to Asian elders, many of which coincide with the above DRE building blocks which are about:
• More appropriate and responsive services • Community engagement. • Better Information
The Community engagement project was established to ascertain the experiences of Asian elders
and their family carers when trying to access Mental Health Services, and/ or their experiences
when they have been given a service.
We were particularly interested in how loneliness and isolation affected Asian elders and family carers. We set out to find what type of services (if any) had been accessed and whether they had helped in any way. We also wanted suggestions for future improvements so that we could feed them back to the Commissioners and Providers of services in Newham
Our aim was to gather information from questionnaires: in order to build a picture of: • How current services are provided • What are the current gaps and barriers to accessing services • How current barriers can be removed in order to improve services
The focus of our work was the needs of: a) Asian Elders – over the age of 55yrs living in the community b) Asian Family Carers – ages varied – living in the community
Some of the respondents were known and were held on SubCo’s database and they were
contacted via a letter, leaflet and personal contact was made. We also contacted other
organisations, for example, Katherine Road Community Centre, LHA-ASRA Housing Association,
and Newham Carers Network, inviting them to participate. Potential respondents were invited to
participate in the project, and were offered the choice of one to one interviews or a focus group.
Prior to the actual gathering of data, 5 sessions were held to introduce the project and engage in
discussions around “Mental Health and Mental Wellbeing.” This was particularly important in
setting the scene for participation by exploring concepts and understanding of Mental Health in the
Asian Community and particular amongst elders and their family carers. These sessions were held
in discussion for a in the relevant community languages.

10
These sessions also encouraged people to come forward and participate in the community
engagement research project with SubCo.
If we had not undertaken this particular work then participation would have been very low.
Participants were invited by letter and in person via telephone conversations. Eight sessions were
available where individuals could choose which session they wanted to attend and bore in mind
linguistic and cultural preferences, for example:
• Language Specific
• Gender
• Female y Male Elders Only
• Male only Female Elders Only
• Mixed (male and female) Asian Elders
• Male Family Carer Specific
• Female Family Carer Specific
• Mixed (male and female) Family Carers
Participants also had the choice of whether they wanted to be interviewed on a one to one basis or be part of a focus group. Timings for each session were allocated accordingly for:
• One to one questionnaires • Focus Groups
• Complementary therapies
• Refreshments
• Assistance with travel
• Personal Care support
The research tools that were used include: one to one questionnaires undertaken in structured
interviews and focus groups.
50 Asian elders were interviewed and answers were noted on the questionnaire.
The Focus Groups
Four focus groups were held and the makeup of these groups varied as we were able to offer a
choice of:
• Asian Family Carer Women only group
• Asian Family Carer Men only group
• Asian elders Men only
• Asian elders Women only
• A facilitator and a co facilitator led each of the groups, plus volunteers were on hand to
provide additional support where appropriate, both in terms of the discussion and personal
care support.

11
Results and Discussion
The results of the Communality Engagement Research programme are as follows:
• There was a lack of awareness of Mental health Services in Newham • They found it difficult to describe Mental Health • They did not know how to deal with Mental Health issues • They did not know where to go for assistance, advice etc • Mental Health was seen as a “stigma” • Mental Health was seen as a contagious disease • Where Mental Health had been identified then it had to be coped with internally, in the
family, and kept hidden • Many felt that abnormal behaviour was seen as a deviation from the norm and therefore the
person was “mad” • Isolation led to “loneliness”, which then resulted in “depression,” which in turn led to a loss
of confidence. • Another strong theme was the factor of withdrawing from daily activities outside of the home
by “shutting themselves away” so as not to cause embarrassment to the family, or where the family did not let them interact with the world outside
• There were very few participants who had experience of mental health services, or a family, friend etc, who they had known. However, where one participant had experience they talked about being given “pills,” but no one really explaining to them what the cause of their illness was, only that they “would feel better if they took the “pills.”
In discussions around improvements that could be made to services and access easier, many of
the respondents said that:
• Staff who spoke appropriate languages would be very helpful. Also staff who had experience of working with people who did not have English as their first language and therefore their understanding of what was being said to them could be misinterpreted.
• Another theme was around information, where information needed to be made widely available in places where people would normally go, e.g. places of worship, support groups, GP Practices, Health Centres, and Community Centres etc. However, it was imperative that the people who ran groups were aware of what services were available so that they could pass the information on when approached by a member.
• There was also a discussion around the importance of Mental Health Services undertaking outreach work at Community Centres and places of Worship to raise awareness around services available, types of support that could be provided and how to refer people to the right services.
• The magnitude of enabling Asian communities to discuss Mental Health per se was seen as imperative in dispelling myths and tackling taboos around Mental Health in Asian communities was seen as a key piece of work that needed to be undertaken.
A prevalent theme to reducing isolation and depression was the role that faith played at an
individual and group level. Many sought solace in their religion through, prayer.
This was undertaken both at home on an individual level, and/or as a group activity.
During the course of the project a number of discussions have been stimulated in relation to the
future work that needs to be undertaken. We have undergone a very steep learning curve and at
the same time we have consolidated our current good practice in the way we have been able to
access and have dialogues with so called “hard to reach communities.”
In relation to gender over 70% of the respondents were women. It is an interesting indicator that less men were willing to participate then women, whether this is due to the fact the more men

12
know about Mental Health then women, or whether this was due to the fact that they did not want to discuss the issues needs further exploration.
In relation to ethnicity and religion we had a very mixed grouping, with participants from Bangladesh, East Africa, India, and Pakistan, with over a quarter seeing themselves as Asian British and almost all were British citizens who had been living in Newham for more than 11 years. There was a mixture of religions that were cited in the questionnaires, the majority; nearly half were Hindu, followed closely by Muslims and then Sikhs. Faith/Spirituality was seen by many people as very important part, and was seen as an integral part of their everyday life, which was not just about timings and prayer. Many found solace in their faith as many felt isolated.
In relation to language 99% of the group felt more comfortable in speaking an Asian language and
these ranged from Bengali, Gujarati, Punjabi and Urdu. Hindi/Urdu was seen as a universal
“language” which was seen as more beneficial in understanding than English, only 21% spoke any
English. Many respondents were multi lingual. Hence, the right communication was seen as an
integral part of accessing information.
Many people felt that they were not well informed in relation to what were perceived as Mental
Health issues, as well as how to access services.
The fact that many people did not want to talk about Mental Health in some part relates to the lack
of awareness mentioned above as well as the stigma attached to mental health and the impact
this illness can have on Asian communities.
Three fifths of those involved had a disability which impacted on their lives in relation to isolation
and their lack of confidence.
Another issue that raised a lot of discussion was the “sexuality” question 23 in the questionnaire.
There were respondents who refused to answer the question at all, whereas others were very
uncomfortable with the question, and this created. Interviewers gave examples, but as the words
were not easily transferrable, the situation was tense.
Depression, stress related issues and memory loss were known as issues for those who were
interviewed. However, over half had no idea of what services were available to them. A small
number had used individual counselling or support groups. For those who had used a service in
relation to a GP, Hospital, over three quarters said that an Advocate or Interpreter had not been
provided to them, which meant they found it very difficult to understand what was being said to
them.
In relation to therapies, reading religious texts was seen as very therapeutic with over half of
participants using this, with smaller numbers using Reiki, Faith healing and Head massage, with
over half of those involved
There were some elders who had no friends or visitors outside of social or health care services;
others had family who visited them. However, there was a high proportion who felt lonely, some
who were extremely lonely and were worried and upset because of their isolation.
Almost half of the respondents were Asian elders who lived alone. Many had expectations that
they would be living in an extended family network in the same accommodation. The impact on
wellbeing, their dreams and hopes of being looked after as they grew older was very difficult to
come to terms with.

13
Recommendations
1. To combat the lack of awareness of the range of Mental Health services available in Newham by reviewing how work is currently undertaken To develop an outreach programme that reaches out into the community and enable discussions of Mental Health and its impact on Asian communities
2. To develop a partnership programme with local community groups, voluntary organisations and faith groups (Places of Worship) to highlight issues of Mental Health
3. To recruit staff who speak a range of Asian community languages and dialect, both in frontline and Advocacy roles
4. To lobby for the development of Community Development Workers for Older People
5. To review and develop existing services run by the East London NHS Foundation Trust and other Mental Health providers such as the Adult Services, The Newham Primary Care Trusts etc., in the community and in institutions to ensure that they meet the needs of Asian elders referred there taking into consideration gender, diet, language and dialect, interests, religion etc.
6. To ensure access to universal services to ensure social inclusion of Asian elders and their family carers
7. To develop Mental Health information that is targeted at the Asian Community
8. To develop support groups for Asian elders who have mental health issues to reduce isolation and loneliness
9. To monitor progress on implementation of the above needs and report back to appropriate Boards, e.g. East London NHS Foundation Trust, Newham PCT, Older peoples Partnership Board, Overview and Scrutiny Board etc.
10. To establish an Implementation Group to monitor progress of actions identified

14
Introduction
The Centre for Ethnicity and Health’s Model of Community Engagement
Background to the Community Engagement Model
We often hear the following words or phrases:
• Community consultation • Community representation • Community involvement/participation • Community empowerment • Community development • Community engagement
Sometimes these terms are used inter-changeably; sometimes one term is used by different
people to mean different things. The Centre for Ethnicity and Health has a very specific notion of
community engagement. The Centre’s model of community engagement evolved over several
years as a result of its involvement in a number of projects. Perhaps the most important milestone
however came in November 2000, when the Department of Health (DH) awarded a contract to
what was then the Ethnicity and Health Unit at the University of Central Lancashire (UCLan) to
administer and support a new grants initiative. The initiative aimed to get local Black and minority
ethnic community groups across England to conduct their own needs assessments, in relation to
drugs education, prevention, and treatment services.
The DH had two key things in mind when it commissioned the work; first, the DH wanted a number
of reports to be produced that would highlight the drug-related needs of a range of Black and
minority ethnic communities. Second, and to an extent even more important, was the process by
which this was to be done.
If all the DH had wanted was a needs assessment and a ‘glossy report’, they could have
commissioned researchers and produced yet another set of reports that may have had little long
term impact. However this scheme was to be different. The DH was clear that it did not want
researchers to go into the community, to do the work, and then to go away. It wanted local Black
and minority ethnic communities to undertake the work themselves. These groups may not have
known anything about drugs, or anything about undertaking a needs assessment at the start of the
project; however they would have proven access to the communities they were working with, the
potential to be supported and trained, and the infrastructure to conduct such a piece of work.
They would be able to use the nine-month process to learn about drug related issues, and how to
undertake a needs assessment. They would be able to benefit and learn from the training and
support that the Ethnicity and Health Unit would provide, and they would learn from actually
managing and undertaking the work. In this way, at the end of the process, there would be a
number of individuals left behind in the community who would have gained from undertaking this
work. They would have learned about drugs, and learned about the needs of their communities,
and they would be able to continue to articulate those needs to their local service providers, and
their local Drug Action Teams (DATs). It was out of this project that the Centre for Ethnicity and
Health’s model of community engagement was born.

15
The model has since been developed and refined, and has been applied to a number of areas of
work. These include:
• Substance misuse • Criminal justice system • Policing • Sexual health • Mental health • Regeneration • Higher education • Asylum seekers and refugees
New communities have also been brought into the programme: although Black and minority ethnic
communities remain a focus to the work, the Centre has also worked with:
• Young people • People with disabilities • Service user groups • Victims of domestic violence • Gay, lesbian and bi-sexual and trans-gender people • Women • White deprived communities • Rural communities
In addition to the DH, key partners have included the Home Office, the National Treatment Agency
for Substance Misuse, the Healthcare Commission, the National Institute for Mental Health in
England, the Greater London Authority, New Scotland Yard, Aim higher and the Welsh Assembly.
1.1 The Key Ingredients of the Model
There are four essential ingredients or building blocks to the UCLAN Community Engagement
model.
1. An issue about which communities and other key stakeholders such as commissioners
and policy makers share some concern
The issue can be almost anything, but frequently involves a concern about inequitable access to,
experience of or outcome from services. The community and other stakeholders may not agree
about the causes of inequity or what to do about it – the key however is that they share a concern.
Usually the concern will be framed within some kind of local, regional or national policy context
(e.g. teenage pregnancy reduction).
2. The Community
According to the Centre for Ethnicity and Health model, a community engagement project must
have the community at its very heart. In order to achieve this, it is essential to work through a host
community organisation. This may be an existing community group, but it might also be
necessary to set up a group for this specific purpose of conducting the community engagement
research.
16
The key thing is that this host community organisation should have good links to the defined target
community1, such that it is able to recruit a number of people from the target community to take
part in the project and to do the work (see section on task below).
It is important that the host community organisation is able to co-ordinate the work, and provides
an infra-structure (e.g. somewhere to meet; access to phones and computers; financial systems)
for the day-to-day activities of the project. One of the first tasks that this host community
organisation undertakes is to recruit a number of people from the target community to work on the
project.
3. The Task or Tasks
The third key ingredient is the task or tasks that the community undertakes. According to the
Centre for Ethnicity and Health model, this must be action oriented. It should be something that is
meaningful, time limited and manageable. Nearly all of the community engagement projects have
involved communities in undertaking a piece of research or a consultation exercise within their
own communities. In some cases there has been an initial resistance to doing ‘yet another piece
of research’, but this misses the point. As in the initial programme run on behalf of the DH, the
process and its outcomes have equal importance. The task or activity is something around which
lots of other things will happen over the lifetime of the project. Individuals will learn; awareness
will be raised; stigma will be reduced; people will opportunities to volunteer and gain qualifications;
new partnerships will be formed; and new workers will enter the workforce. Besides, it is important
not to lose sight of the fact that it will be the first time that these individuals have undertaken a
research project.
4. Support and Guidance
The final ingredient, according to the Centre for Ethnicity and Health’s model, is the provision of
appropriate support and guidance. It is not expected that community groups offer their time and
input for free. Typically a payment in the region of £15-20,000 will be made available to the host
organisation. It is expected that the bulk of this money will be used to pay people from the target
community as community researchers2. A named member of staff from the community
engagement team is allocated as a project support worker. This person will visit the project for at
least half a day once a fortnight. It is their role to support and guide the host organisation and the
researchers throughout the project. The University also provides a package of training, typically in
the form of a series of accredited workshops.
1 The target community may be defined in a number of ways – in many of the community engagement projects it has
been defined by ethnicity. We have also worked with projects where it has been defined by some other criteria, such as age (e.g. young people); gender (e.g. women); sexuality (e.g. gay men); service users (e.g. users of drug services or mental health service users); geography (e.g. within a particular ward or estate) or by some other label that people can identify with (e.g. victims of domestic violence, sex workers). 2 This is not always possible, for example, where potential participants are in receipt of state benefits and where to
receive payment would leave the participant worse off.

17
The accredited workshops give participants in the project a chance to gain a University
qualification whilst they undertake the work. The support workers will also assist the group to form
an appropriate steering group to support the project3.
The steering group is an essential element of the project: it helps the community researchers to
identify the community they are engaging with, and can also facilitate the long term sustainability
of the projects recommendations and outcomes. The community researchers undertake a needs
assessment or a consultation exercise. However the steering group will ensure that the work that
the group undertakes sits with local priorities and strategies; also that there is a mechanism for
picking up the findings and recommendations identified by the research. The steering group can
also support individuals’ career development as they progress through the project.
1.2 The UCLAN Community Engagement Team
The Centre for Ethnicity and Health has a large and experienced community engagement team to
support the work. The team comprises of two programme directors, senior support workers,
support workers, teaching and learning staff, an administration team and a communications
officer. They work across a range of community engagement areas of specialisation, within a tight
regional framework.
National Programme Directors
Northern
Team
Midlands
Team
Southern Team
Senior Support Worker Senior Support
Worker
Senior
Programme
Advisors
Drug
Interventions
Programme
Support
Workers
Support
Workers
Support
Workers
Citizen Shaped
Policing
Teaching And Learning Team
Administration Team
Communications Officer
3 Very often we will have helped groups to do this very early on in the process at the point at which they are applying
to take part in the project.

18
1.3 Programme Outcomes
Each group involved in the Community Engagement Programmes is required to submit a report
detailing the needs, issues or concerns of the community. The qualitative themes that emerge
from the reports are often very powerful. Such information is key to commissioning and planning
services for diverse and ‘hard to reach’ communities. Often new partnerships between statutory
sector and hard to reach communities are formed as a direct result of community engagement
projects.
In 2005/-6 the Substance Misuse Community Engagement Programme was externally
evaluated. This concluded that:
• The Community Engagement Programme had made very significant contributions to increasing awareness of substance misuse and understanding of the substance misuse needs of the participating communities. It also raised awareness of the corresponding specialist services available and of the wider policy and strategy context.
• The Community Engagement Programme had enabled many new networks and professional relationships to be formed and that DATs appreciated the links they had made as a result of the programme (and the improvements in existing contacts) and stated their intentions to maintain those links.
• Most commissioners reported that they had gained useful information, awareness and evidence about the nature and substance misuse service needs of the participating organisations.
• All DATs reported positive change in their relationship with the community organisations. They stated that the Community Engagement Programme reports would inform their plans for the development of appropriate services in the future.
• A significant number of the links established between DATs and community organisations as part of the Community Engagement Programme were made for the first time.
• The majority of community organisations reported their influence over commissioners had improved.
• Training and access to education was successful and widely appreciated. 379 people went through an accredited University education programme.
• A third of community organisations in the first tranche reported that new services had been developed as a result of the Community Engagement Programme.
• The vast majority of participants and stakeholders expressed high levels of satisfaction with the project.
The capacity building of the individuals and groups involved in the programme is often one of the
key outcomes. Over 20% of those who are formally trained go on to find work in a related field.
The views expressed in the report are those of the group that undertook the work, and are not necessarily those of the Centre for Ethnicity and Health at the University of Central Lancashire.

19
1.4 Background Information about Newham
Newham is based in the East of London with an older adult population of 28,000. The borough is
the 6th most deprived in the country with high levels social and economic deprivation and poor
health outcomes in all major areas such as heart disease, stroke and mental health.
The borough is the most ethnically mixed in the country with high levels of immigration. More than
30 community languages are recognised by local agencies however minority ethnic groups are
proportionately under-represented in mental health services.
The communities in the borough that are most strongly represented within the services network
are predominately Asian, African and Caribbean. Other groups such as Irish elders are known to
experience social isolation and associated mental health problems.
Table 1.
NEWHAM 2011 POPULATION PROJECTIONS
Source: GLA 2003 Round Population Projections -
M M M M
50-54 55-59 60-64 65-69
7,002 5,515 4,455 3,038
F F F F
50-54 55-59 60-64 65-69
7,559 5,807 4,658 3,269
TOTAL 14,562
11,32
2 9,114 6,308
Smiling More Often Report, S. Griffiths, 2006
In common with London-wide trends, over half of Newham’s older population is within the age
range 65-74. Only a small proportion, just over one-tenth, are 85 years or older. Similarly,
Newham’s older population is characterised by more females (57%) than males (43%). Females
increasingly predominate in each successive age group, whilst males have a younger age profile.
Older people in Newham are likely to be homeowners or council renters and affected by higher
rates of low income, poor housing, ill-health and disability. They share common aspirations,
uppermost to lead independent active lives with a lifestyle they choose.
20
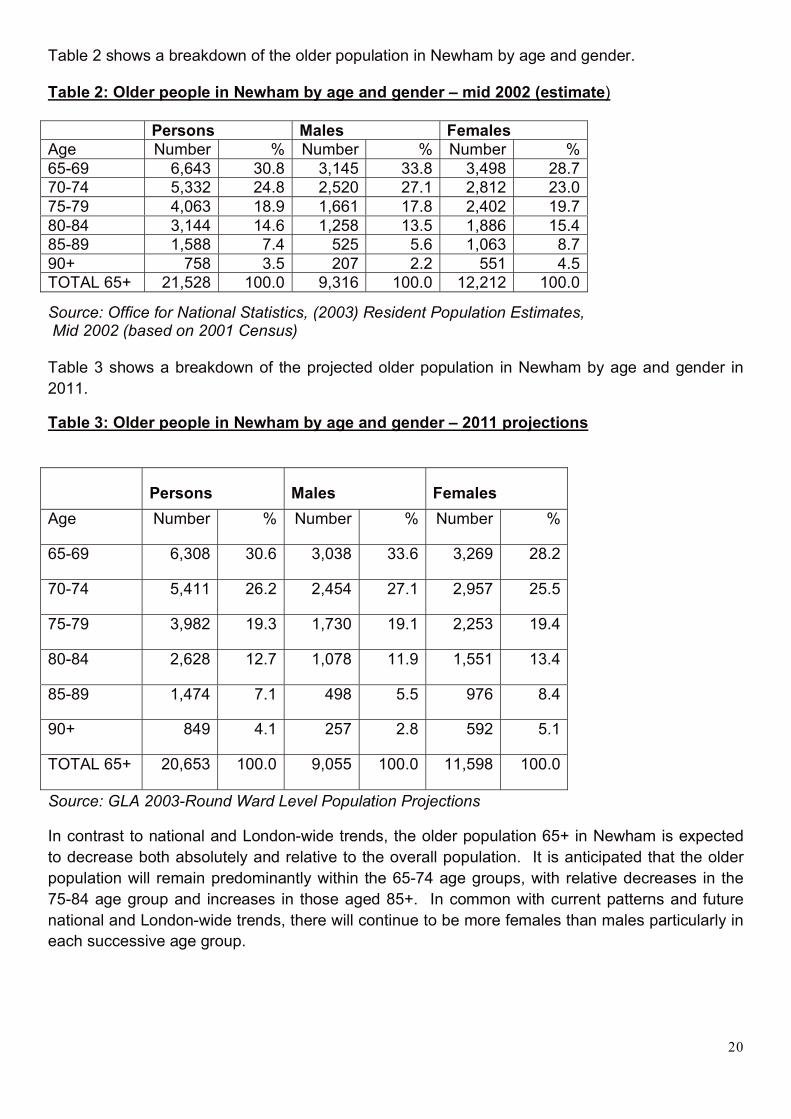
Table 2 shows a breakdown of the older population in Newham by age and gender.
Table 2: Older people in Newham by age and gender – mid 2002 (estimate)
Source: Office for National Statistics, (2003) Resident Population Estimates, Mid 2002 (based on 2001 Census)
Table 3 shows a breakdown of the projected older population in Newham by age and gender in
2011.
Table 3: Older people in Newham by age and gender – 2011 projections
Source: GLA 2003-Round Ward Level Population Projections
In contrast to national and London-wide trends, the older population 65+ in Newham is expected
to decrease both absolutely and relative to the overall population. It is anticipated that the older
population will remain predominantly within the 65-74 age groups, with relative decreases in the
75-84 age group and increases in those aged 85+. In common with current patterns and future
national and London-wide trends, there will continue to be more females than males particularly in
each successive age group.
Persons Males Females
Age Number % Number % Number %
65-69 6,643 30.8 3,145 33.8 3,498 28.7
70-74 5,332 24.8 2,520 27.1 2,812 23.0
75-79 4,063 18.9 1,661 17.8 2,402 19.7
80-84 3,144 14.6 1,258 13.5 1,886 15.4
85-89 1,588 7.4 525 5.6 1,063 8.7
90+ 758 3.5 207 2.2 551 4.5
TOTAL 65+ 21,528 100.0 9,316 100.0 12,212 100.0
Persons Males Females
Age Number % Number % Number %
65-69 6,308 30.6 3,038 33.6 3,269 28.2
70-74 5,411 26.2 2,454 27.1 2,957 25.5
75-79 3,982 19.3 1,730 19.1 2,253 19.4
80-84 2,628 12.7 1,078 11.9 1,551 13.4
85-89 1,474 7.1 498 5.5 976 8.4
90+ 849 4.1 257 2.8 592 5.1
TOTAL 65+ 20,653 100.0 9,055 100.0 11,598 100.0

21
Ethnicity
Newham’s population is characterised by its ethnic diversity, with the highest percentage of
residents from non-white groups in the country at 61.0% compared with 28.8% in London and
9.1% in England. Over the next decade, there will be greater diversity as the number of older
people from black and minority ethnic groups is expected to rise both absolutely and relatively.
This contrasts with anticipated reductions in the overall number and proportion from White groups.
This requires planning for needs for both dedicated and integrated provision, taking into account
the earlier onset of some illnesses usually associated with old age.
Table 4 gives a breakdown of the older population in Newham by age and ethnicity.
Table 4: Older people in Newham by age and ethnic origin – 2001
Source: Office for National Statistics, 2001, 2001 Census Standard Tables
In common with national and London-wide trends, Newham’s older population is predominantly
comprised of White ethnic groups, reflecting the younger age structure of black and minority ethnic
communities. One-quarter of Newham’s older population is from a black and minority ethnic
4 Includes “White: British”, “White: Irish” and “White: Other”
5 Includes “Mixed: White and Black Caribbean” and “Black or Black British: Black Caribbean”
6 Includes “Mixed: White and Black African” and “Black or Black British: Black African”
7 Includes “Mixed: White and Asian” and “Asian or Asian British: Other Asian”
8 Includes “Mixed: Other Mixed” and “Chinese or Other Ethnic Group: Other Ethnic Group”
Ethnic Origin 65-69 70-74 75-79 80-84 85-89 90+ Total
65+
% of
65+
pop
White4 4,137 3,894 3,553 2,649 1,481 665 16,379 75.1
Black
Caribbean5
784 414 232 94 42 29 1,595 7.3
Black African6 205 99 40 31 9 13 397 1.8
Black Other 20 9 8 3 3 0 43 0.2
Indian 704 504 285 198 39 23 1,753 8.0
Pakistani 278 161 58 31 14 13 555 2.5
Bangladeshi 273 154 45 35 0 9 516 2.4
Chinese 38 37 15 14 6 6 116 0.5
Other Asian7 130 81 55 22 7 3 298 1.4
Other8 83 33 31 20 3 3 173 0.8
Total 6,652 5,386 4,322 3,097 1,604 764 21,825 100

22
group, compared with 13% for London. The largest black and minority ethnic groups within
Newham’s older population are Indian (8%) and Black Caribbean (7%).
Similarly, Newham’s population of older people from black and minority ethnic groups is
predominantly within the age group 65-74. With the exception of Chinese groups, there is very
small representation within the 85+ age group. Older people from Bangladeshi, Pakistani, Black
African and Black Caribbean groups are particularly young, with over 75% aged 65-74. These
patterns contrast markedly with White groups who are characterised by a much older age profile,
with 51% aged 75+ and the highest proportion at 13% of those aged 85+.
Over the next decade, as the age structure of black and minority ethnic groups becomes closer to
the average, there will be shifts in the ethnic composition of the older population both nationally
and locally, Office for National Statistics, 2001.
It is anticipated that older people in Newham will continue to consist predominantly of White
groups who will represent two-thirds of the overall older population by 2011. However, there will
be greater diversity as the number of older people from black and minority ethnic groups is
expected to rise both absolutely and relatively. This will be particularly for Black African, Other
Asian, Black Other and Pakistani groups. This contrasts with anticipated reductions in the overall
number and proportion from White groups.
Older people from black and minority ethnic groups will continue to be characterised by a younger
age profile, but there will be increasing representation within the 75+ age groups particularly for
Black Caribbean, Bangladeshi, Indian and Chinese groups. The age structure for White groups
will remain fairly the same.

23
1. The Focus of this Report
Since 2000 over 250 community groups have taken part in one or other of the Centre for Ethnicity
and Health’s Community Engagement Programmes.
National Institute for Mental Health in England Community Engagement
Programme:
The community engagement research project at SubCo Trust targeted 100
Asian elders and their family carers in the London Borough of Newham. This
work was both qualitative and quantitative and we aimed the project at:
The Community engagement project was established to ascertain the
experiences of Asian elders and their family carers when trying to access
Mental Health Services, and/ or their experiences when they have been given
a service.
• We were particularly interested in how loneliness and isolation affected Asian elders and family carers
• We set out to find what type of services (if any) had been accessed and whether they had helped in any way
• We also wanted suggestions for future improvements so that we could feed them back to the Commissioners and Providers of services in Newham
Our aim was to gather information from questionnaires: in order to build a
picture of:
1. How current services are provided 2. What are the current gaps and barriers to accessing services 3. How current barriers can be removed in order to improve services
The focus of our work was the needs of:
a) Asian Elders – over the age of 55yrs living in the community
b) Asian Family Carers – ages varied – living in the community
The project seeks to identify and engage local hard to reach groups that are
under-represented in mental health services. The project ultimately aims to:
• Enhance social inclusion for these individuals • Encourage the development of social capital projects through
engagement with communities • Assist local agencies to identify the extent of mental health need
amongst excluded groups.

24
2.1 SubCo Trust and Who We Are
SubCo Trust (formerly known as SubCo Elders Day Centre) was formed in 1993, and is a
Company Limited by Guarantee, registration no: 3031652 and a Registered Charity, no:
1045237. SubCo is well known for its expertise in the provision of culturally appropriate services
to Asian elders and their carers.
The aim of SubCo is to provide day care provisions to frail Asian elders of the sub-continent
over the age of 55 years, with a particular focus on those who are frail, isolated and house
bound. SubCo is a product of a community led initiative.
Over the years we have pioneered a number of innovative services as a result of our continual
review of our services, and the cataloguing of unmet needs within the London Borough of
Newham. We see approximately 250 users per week. We specifically work for Asian elders. We
have strong partnerships within Asian communities, the independent and statutory sectors.
The projects and initiatives developed within SubCo have led to recognition of the improvement in
the quality of life for frail Asian elders. This can be seen at an individual level as well as at a macro
level in terms of influencing developments in appropriate services from frail Asian elders in
Newham by the statutory and voluntary sectors. SubCo has also been assisting other
organisations to develop services for elders and carers,
SubCo works towards the empowerment of elders, assisting them in accessing services they are
entitled to whilst campaigning for services they need that are culturally, religiously and linguistically
appropriate. SubCo has provided a range of services and activities from:
• Advice Surgeries (housing, welfare rights) • Mental Health Advocacy and support • Befriending • Health Advocacy • Bilingual Counselling sessions • Range of health promotion activities (surgeries, advice, physical exercise, workshops) • Home visits and support for carers • A programme of social and cultural activities such as arts and crafts, ESOL, games, outings
and groups • Drop in activities including book and video loans • Asian Meals Service (luncheon club and a meals on wheels delivery service) • Cantonese Meals Service • Shopping Service • Volunteers Programme • Intergenerational work • Establishing the Healthy Green Street Project • Development Work • Training & support Programmes

25
There is a body of evidence Felton, S, (1987), Social Service Inspectorate (1998), Norman, A, (1985) to indicate that the mental health needs of some older adults from ethnic minorities, and other hard to reach groups, are not being identified because of difficulties individuals from these communities have in accessing services, One of the principal difficulties such groups have is accessing clinically skilled and appropriate interpreting and translation services which explain mental health services in a way that is culturally sensitive and appropriate. This is pertinent to direct work with individuals, their carers and local community organisations.
SubCo has over the years built an excellent reputation in working with and networking with other organisations, particularly those working with older people. For example, Healthywise formerly known as Newham Healthy Living Network for Elders and Carers and has been instrumental in developing partnerships amongst the 17 strong membership of both voluntary and statutory organisations. the Older Peoples Reference Group that is based in Newham, As well as the Renewal programme which runs a number of projects ranging from carers, to refugees, to homeless people and hostels for young people.
We also have strong links with a number of faith based organisations in Newham who are not involved in “traditional networks.”
SubCo has also been a partner in a programme supporting older people who have survived a stroke, working with both Asian and Afro Caribbean communities to provide support for people post stroke. The Healthy Living Network partnership, referred to earlier, has included older people’s voluntary sector organisations working with BME communities on preventive programmes and improving service access.
The East London Foundation Trust, (formerly known as the East London and City Mental Health Trust) is the local statutory mental health provider and seeks to deliver culturally sensitive older adult mental health services. However it is felt that secondary care mental health services are predominantly Euro-centric and do not meet the needs of minority groups.
There is an established tradition of joint working across local organisations with links to the Newham Older People’s Partnership Board, and an agreed partnership strategy for older people’s services.
2.2 Methods
Methodology
SubCo aimed to gather information from questionnaires: in order to build a picture
of :
• How current services are provided • What are the current gaps and barriers to accessing services • How current barriers can be removed in order to improve services
Some of the respondents were known and were held on SubCo’s database and they were
contacted via a letter, leaflet and personal contact was made. We also contacted other
organisations, for example, Katherine Road Community Centre, LHA-ASRA Housing Association,
and Newham Carers Network, inviting them to participate. Potential respondents were invited to
participate in the project, and were offered the choice of one to one interviews or a focus group.

26
Prior to the actual gathering of data, 5 sessions were held to introduce the project and engage in
discussions around “Mental Health and Mental Wellbeing.” This was particularly important in
setting the scene for participation by exploring concepts and understanding of Mental Health in the
Asian Community and particular amongst elders and their family carers. These sessions were held
in discussion for a in the relevant community languages.
These sessions also encouraged people to come forward and participate in the community
engagement research project with SubCo.
If we had not undertaken this particular work then participation would have been very low.
Participants were invited by letter and in person via telephone conversations with a tear off slip
confirming attendance and the session they wanted to attend (See appendix?). Eight sessions
were available where individuals could choose which session they wanted to attend and bore in
mind linguistic and cultural preferences, for example:
• Language Specific
• Gender
• Female y Male Elders Only
• Male only Female Elders Only
• Mixed (male and female) Asian Elders
• Male Family Carer Specific
• Female Family Carer Specific
• Mixed (male and female) Family Carers
Participants also had the choice of whether they wanted to be interviewed on a one to one basis or
be part of a focus group.
Timings for each session were allocated accordingly for:
• One to one questionnaires
• Focus Groups
• Complementary therapies
• Refreshments
• Assistance with travel
• Personal Care support
The research tools that were used include: one to one questionnaires undertaken in structured
interviews and focus groups.
2.3 The Questionnaire
A questionnaire was developed and piloted with a small sample of Asian elders to ensure that the
questions were relevant and comprehensive. As the questionnaires were written in English, it was
imperative that certain concepts and phrases were applicable when translated and not “lost in
translation.”
The one to one interviews were conducted at SubCo and privacy was ensured so that the
interview could not be overheard by anyone apart from the interviewer and interviewee.

27
The interviews were conducted in the language of the interviewee’s choice to enable appropriate
dialogue. Interviewers were trained to undertake the interviews in the appropriate language.
Interviewees were also be offered the choice of a male or female interviewer and this enabled the
interviewee to feel more comfortable in answering questions around personal lifestyles,
experiences and issues triggering mental health in relation to isolation, loneliness cognitive or
functional illness.
Although the questionnaire was to be conducted in a structured interview, interviewers were
provided with at least 2 training sessions to enable them to engage with the interviewee and to
make them feel as comfortable as possible when answering questions. For example, using role
plays where interviewers had a turn in being an interviewer and a interviewee.
50 Asian elders were interviewed and answers were noted on the questionnaire.
2.4 The Focus Groups
A focus group was also piloted with a group of 6 Asian elders to gather their views on the themes
that were going to be introduced for discussion. As a result of the discussion an extra theme was
included around “Whether faith played a part in their life in dealing with Mental Health wellbeing.
Four focus groups were held and the makeup of these groups varied as we were able to offer a choice of:
• Asian Family Carer Women only group • Asian Family Carer Men only group
• Asian elders Men only
• Asian elders Women only
The focus groups lasted approximately 1 hr, and each group had the same themes running throughout including:
• Isolation and loneliness • Experiences of services • Suggestions of how services can be improved • Access or lack of access to services • Barriers encountered • How services could be improved • Discussions about specific illnesses • Language specific issues (if any)
A facilitator and a co facilitator led each of the groups, plus volunteers were on hand to provide
additional support where appropriate, both in terms of the discussion and personal care support.
2.5 Steering Group
The work was monitored by a Steering Group which met regularly on a 4 week basis. The Steering
Group was composed of: Ian Kennedy – Group Manager: Older People & General Services,
Michael McGhee –General Manager: Older persons Services Jane Tilston – Integrated
Commissioning Manager Older People (until November 2007), Sylvia West, Commissioning
Consultant (from November 2007), Taskin Saleem – Chief Executive, SubCo Trust and

28
coordinator of the Community engagement Research Project, Tim Bishop, FIS, Denise Bobb,
Race Equality Lead, Ghulam Hussain - Service User, The Safir Ahmed, Community Engagement
Research Worker, Shabana Asif, Community Engagement Research Worker, Thakorbhai Patel,
Community Engagement Research Worker.
2.6 The Community Engagement Research Team
The Team comprised of 3 Community Engagement Research workers and a coordinator, and
there were also 10 volunteers. Other members of the SubCo Trust Team were also available when
appropriate.
The community engagement research project was undertaken by bilingual and tri lingual
Community Engagement workers and volunteers who were able to communicate in a range of
languages including: Bengali, English, Guajarati, Hindi, Mauritian, Punjabi, Pashtu, Swahili and
Urdu. The Community Engagement Team comprised of both men and women.
The team members had a range of community development and community engagement
experience. All had experience of working with vulnerable adults and/or family carers.
The core team of 3 had to attend 5 workshops in relation to Mental Health, research techniques
and collation of information which was run by the University of Central Lancashire, plus a Support
Worker was allocated to the Project as a whole.
The information gained from the workshops coupled with SubCo’s expertise around working with
Asian elders and family carers enabled us to provide an induction programme and 3 training
sessions with the full team.
The focus at these sessions looked at:
• Aim of the Project • What we hope to achieve • Risk management
• “Coping strategies”
• Conducting and ending an interview
• Conducting and ending a focus group
• Role plays where staff and volunteers reacted various scenarios
• Importance of maintaining confidentiality
• What to do if a disclosure is made which may put the individual or others at risk
• What to do if an elder gets distressed during the interview or focus group
• Health & and Safety • Dynamics of Group work • Working with vulnerable adults • How to deal with conflict
The Steering group meets on a 4 weekly basis. For those who are on e mail, there are “round
robin” discussions as and when needed. For those who are not, e.g. the service user, they are
briefed and their feedback taken as and when appropriate.

29
2.7 Ethics
The University of Central Lancashire have a very rigorous Ethics Procedure. As part of this
procedure we were asked to clearly identify issues around ethics and how we were going to
implement these in practice see (section 9.6), this was the first time SubCo had completed an
Ethics form.
3 Quantitative Questionnaire Results
Gender/Age
Of our research sample group 30% were male and 70% were female. (See Fig.1). We interviewed people between the ages of 50 -90 years the majority of the group were aged between 61-70 years. (See Fig.2).
Ethnicity/Religion
Our project focus was on elders from Asian origins, we found that 57% of the elders we
interviewed were of Indian ethnicity, 22% were of Pakistani ethnicity, 4% were of Bangladeshi
ethnicity, 2% Tamil and a remaining 15% were Asian/ Asian British. (See Fig.3)
We found that all of the elders interviewed were born outside of the UK. (See Fig.4) 98% of them
have been living in the UK for more than 11 years (See Fig.5) and 93% are all UK citizens. (See
Fig.6). Of the people interviewed 33% were Muslim, 49% were Hindu, 16% were Sikh and 2%
were Zoroastrian (See Fig.39).
Language
The majority spoke Gujarati (41%), Panjabi (32%), Urdu (11%) and Bengali (6%) as a first
language (See Fig.7) and were able to write in Gujarati (46%), Panjabi (13%), Urdu (19%) and
Bengali (8%). (See Fig.8) We found that only 21% spoke English as a second language whereas
70% spoke other second languages and the remaining 9% did not speak any second language
(See Fig.47).
Accommodation
48% of them had their own homes (See Fig.13) and 46% were living alone (See Fig.12) the
remaining 54% were living with either a partner, children or both (See Fig.12). Out of the 46% that
were living with a partner, children or both 92% said that they were able to speak to the people
living with them on a regular basis (See Fig.16). 38% of the people said their conversations would
last between 0-30 minutes and 54% of them said their conversations would be between 30-60+
Minutes (See Fig.17).
Feeling alone
We found that 20% of the people interviewed had no visitors that visited them at home (See
Fig.19). The 60% that did have visitors visiting them at home were mainly Family 50% and Friends
40% (See Fig56). They were being visited on average of once a week 20%, 3 times a week 27%
and once a month 20% (See Fig.57). 37% of the people interviewed said that they go out 1-2
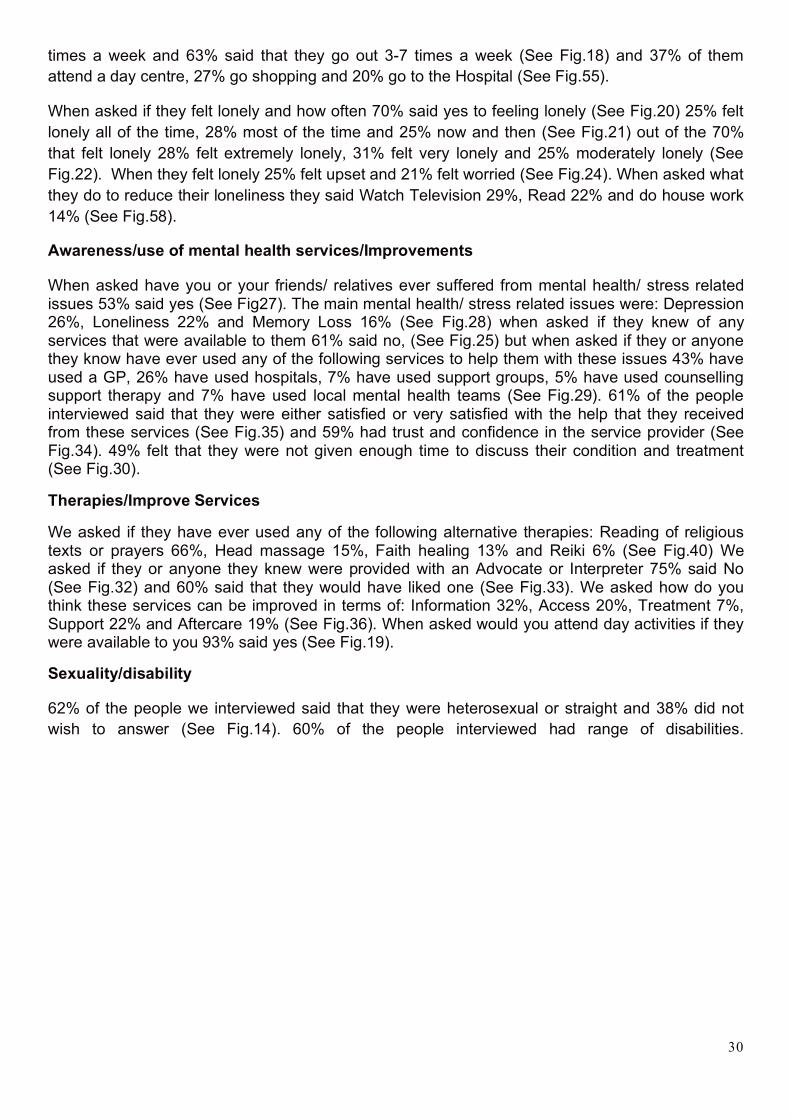
30
times a week and 63% said that they go out 3-7 times a week (See Fig.18) and 37% of them
attend a day centre, 27% go shopping and 20% go to the Hospital (See Fig.55).
When asked if they felt lonely and how often 70% said yes to feeling lonely (See Fig.20) 25% felt
lonely all of the time, 28% most of the time and 25% now and then (See Fig.21) out of the 70%
that felt lonely 28% felt extremely lonely, 31% felt very lonely and 25% moderately lonely (See
Fig.22). When they felt lonely 25% felt upset and 21% felt worried (See Fig.24). When asked what
they do to reduce their loneliness they said Watch Television 29%, Read 22% and do house work
14% (See Fig.58).
Awareness/use of mental health services/Improvements
When asked have you or your friends/ relatives ever suffered from mental health/ stress related issues 53% said yes (See Fig27). The main mental health/ stress related issues were: Depression 26%, Loneliness 22% and Memory Loss 16% (See Fig.28) when asked if they knew of any services that were available to them 61% said no, (See Fig.25) but when asked if they or anyone they know have ever used any of the following services to help them with these issues 43% have used a GP, 26% have used hospitals, 7% have used support groups, 5% have used counselling support therapy and 7% have used local mental health teams (See Fig.29). 61% of the people interviewed said that they were either satisfied or very satisfied with the help that they received from these services (See Fig.35) and 59% had trust and confidence in the service provider (See Fig.34). 49% felt that they were not given enough time to discuss their condition and treatment (See Fig.30).
Therapies/Improve Services
We asked if they have ever used any of the following alternative therapies: Reading of religious texts or prayers 66%, Head massage 15%, Faith healing 13% and Reiki 6% (See Fig.40) We asked if they or anyone they knew were provided with an Advocate or Interpreter 75% said No (See Fig.32) and 60% said that they would have liked one (See Fig.33). We asked how do you think these services can be improved in terms of: Information 32%, Access 20%, Treatment 7%, Support 22% and Aftercare 19% (See Fig.36). When asked would you attend day activities if they were available to you 93% said yes (See Fig.19).
Sexuality/disability
62% of the people we interviewed said that they were heterosexual or straight and 38% did not
wish to answer (See Fig.14). 60% of the people interviewed had range of disabilities.

31

32
33.2 Quantitative Data Graphs

33

34

35

36

37
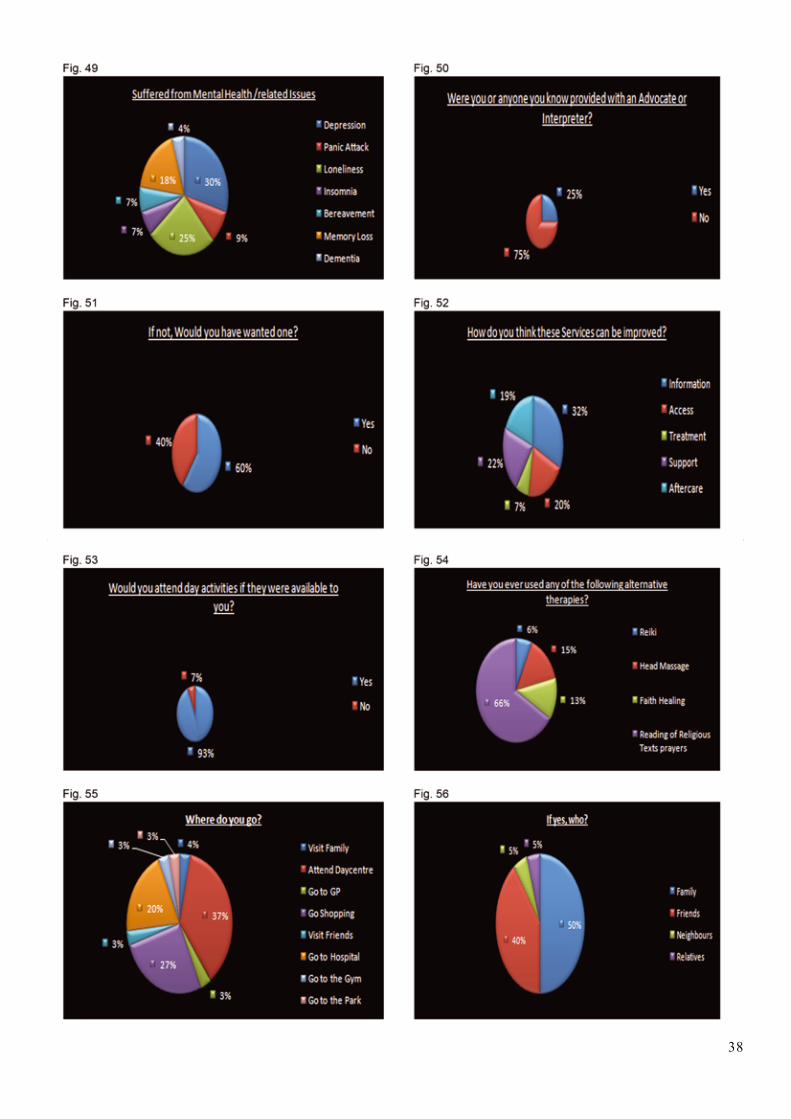
38

39
3.3 Quantitative Data Open Questions
50 people were asked about the kind of help they needed, their answers showed that they wanted
someone to visit them on regular basis since they did not have any family or friends.
35 respondents also wanted services where they could report minor repairs in their house and get
someone to repair them. Their answers also showed that they wanted a befriending service.
12 members of the Carers group requested more support groups sessions where they could meet people in
similar situations.
The reason for not accessing services was due to the fact that respondents “Had problems accessing
appropriate agencies”. Some of them said that they “Had to go through various channels before they got
through to the right person.” Therefore, they wanted easier access to services.
Respondents also felt that professionals did not have a good “understanding of service users’
problems/issues/difficulties”.
When asked if they knew of any Mental Health services only two services were mentioned. These services
were MIND, and the local Mental Health team. Respondents felt that their cultural and religious needs were
not understood well.
Language was also seen as an issue as information leaflets displayed were in English. Respondents made
a requested that provision were made where “Facilities, information centres, and people at these centres
for people who did not speak English.”
Respondents also said very, strongly, that they needed more Advocates, and a culturally appropriate
counselling service.
Fig.57 Fig.58

40
4 Qualitative Data
4.1 Focus Groups
For the community engagement research project, four focus groups were held and the makeup of these groups varied as we were able to offer a choice of:
• Asian Family Carer Women only group • Asian Family Carer Men only group
• Asian elders Men only
• Asian elders Women only
• Asian elders mixed group
The focus groups lasted approximately 1 hr, and each group had the same themes running throughout including:
• Isolation and loneliness • Experiences of services • Suggestions of how services can be improved • Access or lack of access to services • Barriers encountered • How services could be improved • Discussions about specific illnesses • Language specific issues (if any)
The same six specific questions were used in all the focus groups and the findings are listed
below.
4.2 Punjabi Women’s Group Focus Group
Ages ranged from 42 To 68 Years
Ethnic breakdown: Indian
This group was a Women’s only group and consisted of 13 women, who met together once a
week on Tuesday at SubCo in Plashet Road. The women gathered regularly for exercise and
health checks. They were all originally from India, and had lived here between 25 and 30 years.
Many only spoke Punjabi, and a handful spoke English and Urdu or Hindi as well.
This group is also involved in other activities, trips and visits arranged by SubCo.
A female facilitator, and a female scribe facilitated the group and both spoke in Punjabi for the
focus group session.
1. What is your understanding of Mental Health?
The respondents in the focus group’s understanding of mental health related to: “someone who
talks to themselves,” another went on to say that “people not remembering things or events,”
another understood mental health to be

41
“Someone who wants to remain alone” and another characterised mental health as “someone who
has low self esteem.”
Another member described it as “People staying quiet.”
Three other members described the symptoms of “someone who becomes paranoid, and is
suspicious of everyone.”
Whereas another member felt that mental health “also affects the body” where there was “physical
pain or neglect.”
Yet another member felt that mental health “was about being lonely and that they should talk to
the individual.”
It is interesting that members of this women only focus group saw mental health as individual
personal characteristics, where when negative contributed to the signs of mental health.
2. Amongst Asian communities mental health is an issue which is often frowned upon and hardly spoken about, what do you think are the possible reasons for that?
The respondents in the focus group as a grouping agreed that mental health was an area that
people did not talk about because they said: “That people will not talk about mental health as it will
affect the marriage prospects of members of the immediate family and people will not want to
know them.”
A number of members repeated this viewpoint, and another member went on to say that “this in
turn will reflect negatively on their family,” and another went on to emphasise that “people may not
take you seriously” in matters of marriage arrangements, advice or work.”
In Asian communities, marriage is still seen as an institution that is not just about the individual but
is also about their immediate family, and extended family networks. Therefore, it is not surprising
that this focus group saw mental health as being a subject that “was not to be spoken about” as it
would lead to a number of serious ramifications from their point of view.
3. What are the causes of isolation on one’s health?
The respondents in the focus group said isolation for them had the following features, particularly,
where it “can end up (making a person) feeling very angry and become aggressive.”
Another member went on to say that “depression” was a symptom. Another member said that it
left a person “feeling scared and paranoid” or “feel like nobody likes them.”
Yet another member described it as a symptom “where someone was very withdrawn from social
life.”
Two other members described isolation where “physical appearance gets neglected” and there is
a “loss of appetite and sleep.”

42
The above characteristics described by members of the Punjabi women focus group on isolation
on the one hand as being an individual characteristic and on the other hand a manifestation of
physical deterioration affecting the body.
4. If you have accessed any Mental Health services how was your experience, and what suggestions can you offer for future improvements to make these services more accessible to Asian elders?
All the respondents in the focus group said that they knew very little about mental health services
and that “an Information centre should be available where they can go to get information about
this.”
Four members said that they thought a “befriending service” should be available “where someone
could go and not feel lonely.”
The focus group had little more to say on the subject as they were unaware of what was available.
5. What therapy would you use or recommend to someone who is going through isolation?
The respondents in the focus group said to reduce isolation that they individuals should be helped
to get out of the home and one member felt “they could be taken on an outing.”
Another member said that they “could be taken out for shopping.”
Three other members felt that it was important to “find out their interests” and another said that
they “should take on a hobby.”
From this discussion the members of the focus group felt that it was important to take the person
out of their home environment in order to reduce their isolation.
6. Has your faith in anyway helped you overcome loneliness or depression? If so how?
The respondents in the focus group said faith played an important role, one member said that “It
diverts your mind.”
Another member said that “faith gives you inner peace.”
Another member went on to say that “reading religious books passes the time, it becomes a hobby
for some.”
Two members felt that “at least God loves us” and “there is nobody who cares except God.”
One member took a different view where she said faith helps you to “look upon people who are in
worse conditions.”
From the above we can see that faith is an important factor in assisting some individuals to
overcome loneliness or depression.

43
4.3 Asian Carers’ Focus Group
There were 12 members in focus group, all of who were carers of Asian elders.
Ages ranged from 35 To 72 Years.
2 were men, 10 were women
Ethnic Breakdown: Indian, Pakistani and Bangladeshi
1. What is your understanding of Mental Health
The members in the focus group said:
Mental Health was when the “brain keeps diverting,” another said that it was the result of “stress.”
Another member said that it rose as a result of “staying alone,” and another member said that it
was due to “depression and tension.”
Another member said that it came from “family problems and life style pressures.” Another
member also agreed that it was due to “family conflict.”
Three members attributed mental health due to an “illness,” due to a “disability” and another as “a
loss of ability to cope.”
2. Amongst Asian communities mental health is an issue which is often frowned upon and hardly spoken about, what do you think are the possible reasons for that?
The members in the focus group said mental health was not discussed because they “Do not want
anyone to find out,” another went on to say that “family issues must remain within the family.”
Another member could not understand “the point of talking about mental health,” and another felt
that “people are not interested in each others’ issues.”
3. What are the causes of isolation on one’s health?
The members in the focus group said:
Isolation would make them "become depressed, and start to get other related illnesses“, another
went on to talk about “self neglect and losing the will to do things if they weren’t going out
anywhere.”
Another member went on to emphasise that people would “lose social skills, and spend a lot of
time alone.”

44
4. If you have accessed any Mental Health services how was your experience, and what suggestions can you offer for future improvements to make these services more accessible to Asian elders?
The Members in the focus group said:
“People only take interest or pay any attention when they become too extreme,” another member
said that “they were given depression tablets.”
One member said that “staff had a lack of experience of people who can only speak in Asian
languages.” Another said that if “information (was) to be translated in other languages” this would
help. Another member said that a “Seminar should be held to educate us.”
5. What therapy would you use or recommend to someone who is going through isolation?
The members in the focus group said:
They “would talk to the person, introduce them to other services,” another said that “they would
find out what their interest was.” Another member said they “would encourage them to come to a
Support Group.”
6. Has your faith in anyway helped you overcome loneliness or depression? If so how?
The members in the focus group said:
That “Visiting a Gurdwara (Sikh Temple) motivates me to live.” Another member said that “I read
from the Quran when I feel low and pray,” another member said that “I sing Bajans (Hindi
Hymns).”
4.4 Asian Elders Focus Group
Ages ranged from 65 To 85 Years
3 were men, 8 were women
Ethnic breakdown: Indian and Pakistani
Tej Bhavan is a sheltered housing scheme run by LHA-ASRA Housing, for Asian elders in
Newham. Some live alone or with their husband or wife in a 1 bedroom flat. It is staffed by a
Scheme Manager, and tenants are linked to a community alarm system. There are also a range of
communal facilities available on site. 11 Asian elders took part in the Focus Group.
45
1. What is your understanding of Mental Health?
The respondents in the focus group understanding of mental health responded and one member
responded by saying that “it is when someone’s mind is not working properly,” another associated
it with the fact that “if children do not listen to you, you get stressed and start getting involved in
their decisions” demonstrating that it was about being disengaged from the decision making
process.
Another member said it was when others “they (family) start to think you’re going crazy or losing
it’.”
2. Amongst Asian communities mental health is an issue which is often frowned upon and hardly spoken about, what do you think are the possible reasons for that?
The members in the focus group response to this question varied and included responses such as
“people are scared of been hospitalised.” Another member went on to say that “if someone finds
out you will be stigmatised,” or the issues are not discussed because “people feel embarrassed
and insulted that you want to discuss family issues.”
A different member of the group said that “people feel it is an “insult” to tell if you are having a
mental problem.”
Another member went on to say that people do not speak about mental health because they “do
not know where to get support.”
3. What are the causes of isolation on one’s health?
The members in the focus group said that the affect isolation had was that there was more time
that led them to “thinking too much about problems“ or
“Worrying about things which you can’t do anything about.” Another member felt that it was the
result of “someone dying” and then being “left alone.”
4. If you have accessed any Mental Health services how was your experience, and what suggestions can you offer for future improvements to make these services more accessible to Asian elders?
Only one member of the focus group had had experience of mental health services and they said:
“I was referred to the psychiatric unit, and was advised not to be alone, should go out and visit
place or family.”
5. What therapy would you use or recommend to someone who is going through isolation?
The members in the focus group said:

46
“One member said that they would advise them to go out,” another one said they would encourage
the person to “make friends,” and another said that they should “go on holiday.”
6. Has your faith in anyway helped you overcome loneliness or depression? If so how?
The members in the focus group said:
That “yes going to my Mandhir (Hindu Temple) makes me feel light hearted,” another said they
“were able to meet other people there who have achieved some tranquillity in their life by coming
there.”
Another member said that by “going to the mosque gives me hope, and diverts my mind way from
been negative about life.”
4.5 Katherine Road Men’s 50+ Focus Group
Ages ranged from 40 To 72 Years
Ethnic breakdown: Pakistani
Lived alone: 4
Lived with partner: 7
Lived with family/other: 7
This group was a men’s only group and consisted of 18 men. The group was made up of men
from Pakistan who spoke both Urdu and Punjabi. The group meetings were held on a weekly
basis on Tuesdays and Thursdays and approximately 20 men attended. The focus group
consisted of 18 men, 2 facilitators and a scribe. The meeting was conducted in a mixture of Urdu
and Punjabi languages. The composition of the group was a mixture of men who were married or
separated from their families. All had been living in England for over 20 years. 8 were retired, and
6 were long term unemployed, 4 were currently working part time.
All members saw the group as a support group, and 6 spoke English as well.
The aim of the focus group was to ascertain individuals understanding of mental health, issues
associated with mental health, awareness of local mental health services and their experiences.
1. What is your understanding of Mental Health?
It was interesting to note that 7 members of the group found it easier to relate to the concept of
mental health as a condition where the person “malfunctions” and has to be “fixed” as the mind is
not functioning properly, for example,
One member said the: “Mind is like a computer sometimes it gets a virus which could be due to
anxiety or worry or an accident”

47
Another as a circuit: “where the brain is greatly connected with the body, if the brain has stress or
pressure the whole body gets affected.”
Again another member described it in terms of where “the body can forget to look after itself when
the mind is under pressure.”
Outside of these mechanical or engineering perspectives, members of the group found it difficult to
describe mental illness.
2. Amongst Asian communities mental health is an issue which is often frowned upon and hardly spoken about, what do you think are the possible reasons for that?
The members found this question difficult to answer or comment on, despite it being paraphrased
twice. However, they were able to agree that the reason mental health was not openly discussed
was due to the fact that:
“People try to sort it out themselves.”
That it was seen as a behavioural response which when “someone has mental illness when
you take them out, their behaviour may embarrass us e.g. they might swear or be rude”
And as a result “People may laugh at them.” Therefore to avoid embarrassment it was better to
keep the person isolated or “hidden” at home, and therefore not talk about it in public.
5 members of the group felt that there were other issues involved and described it as: “Our people
think it’s not mental health but rather its black magic. They do not understand that they are ill.”
3. What are the causes of isolation on one’s health?
In answer to this question, members of the focus group were able to attribute a number of factors
that led to isolation. One member explained isolation as “depression, living alone can make you
depressed” another went on to say that “Isolation can cause various illnesses.”
Yet another member, and this was shared by many in the group had a different perspective where
he said that “You are never alone if you read “Namaz” (Muslim Prayers) five times a day as Allah
is with you five times a day.” Therefore expressing that one is never alone if they have a spiritual
belief/faith.
Other members however, acknowledged that a physical disability can affect their situation, for
instance, “If someone is ill, had a stroke or something like that, there is no one there to help them
and so they stay at home on their own.”
4. If you have accessed any Mental Health services how was your experience, and what suggestions can you offer for future improvements to make these services more accessible to Asian elders?

48
Many members of the group found it difficult to answer this question as they said “We have no
idea about what services are available.”
They went on to say that “there should be leaflets to inform people of services available”, and
these should be made available “in mosques and other places of gathering.”
Two members who were on the Management Committee went on to say that
“We have no idea what to do if someone is suffering from any mental health issues” and that
“there should be training for committee members so we are aware and can pass on the
information to our members.”
5. What therapy would you use or recommend to someone who is going through isolation?
In response to this question, the group felt that it was a responsibility and a duty of all of them that
if they came across a person that was isolated then we should “Motivate them and as neighbours
keep an eye on elders who live alone” and “tell them about other groups in the area to join” and
“take them out for a walk.”
It is interesting to note that the group felt the importance of peer support as a major factor in
reducing isolation. This, in all probability, reflects many of the group members’ own reasons for
attending the Over 55s Group at Katherine Road.
6. Has your faith in anyway helped you overcome loneliness or depression? If so how?
All members of this focus group were Muslim, some of who practiced more devoutly then others.
Therefore, one member said that “reading Namaz (Muslim Prayer) gives (him) peace” and “zikr”
(remembrance of Allah {god}), which to him was “also a form to communication.”
Another member said that “if you go to pray in a Mosque five times a day, this is good exercise,
you meet other people,” and if “people who are having any difficulty may one day come to the
mosque and find themselves been helped by someone, especially if they are alone.”
Yet another member went on to explain that “my religion gives me “zehni sakoon” (peace of
mind).”
49
5 Themes Arising from Discussions at the Focus Groups
The main themes arising out of the Focus Groups can be listed as:
What is your understanding of Mental Health?
All the participants demonstrated that: • There was a lack of awareness of Mental health Services in Newham • They found it difficult to describe Mental Health • They did not know how to deal with Mental Health issues • They did not know where to go for assistance, advice etc
7. Amongst Asian communities mental health is an issue which is often frowned upon and hardly spoken about, what do you think are the possible reasons for that?
All the participants were unanimous in their views that Mental Health issues were not spoken about in Asian communities, as they felt it would have a detrimental effect on family members, prospects of marriage for their children, grandchildren and extended family networks etc:
• Mental Health was seen as an embarrassment • Mental Health was seen as a “stigma” • Mental Health was seen as a contagious disease • Where Mental Health had been identified then it had to be coped with internally, in the family, and kept hidden • Many felt that abnormal behaviour was seen as a deviation from the norm and
therefore the person was “mad”
8. What are the causes of isolation on one’s health?
Many of the participants found it difficult to link isolation to health. However they were able to say
that the following had an impact:
Isolation led to “loneliness”, which then resulted in “depression,” which in turn led to a loss of
confidence.
Another strong theme was the factor of withdrawing from daily activities outside of the home by
“shutting themselves away” so as not to cause embarrassment to the family, or where the family
did not let them interact with the world outside.
9. If you have accessed any Mental Health services how was your experience, and what suggestions can you offer for future improvements to make these services more accessible to Asian elders?
There were very few participants who had experience of mental health services, or a family, friend
etc, who they had known. However, where one participant had experience they talked about being

50
given “pills,” but no one really explaining to them what the cause of their illness was, only that they
“would feel better if they took the “pills.”
In discussions around improvements that could be made to services and access easier, many of
the respondents said that:
Staff who spoke appropriate languages would be very helpful. Also staff that had experience of
working with people who did not have English as their first language and therefore their
understanding of what was being said to them could be misinterpreted.
Another theme was around information, where information needed to be made widely available in
places where people would normally go, e.g. places of worship, support groups, GP Practices,
Health Centres, and Community Centres etc. However, it was imperative that the people who ran
groups were aware of what services were available so that they could pass the information on
when approached by a member.
There was also a discussion around the importance of Mental Health Services undertaking
outreach work at Community Centres and places of Worship to raise awareness around services
available, types of support that could be provided and how to refer people to the right services.
The magnitude of enabling Asian communities to discuss Mental Health per se was seen as
imperative in dispelling myths and tackling taboos around Mental Health in Asian communities was
seen as a key piece of work that needed to be undertaken.
10. What therapy would you use or recommend to someone who is going through isolation?
In relation to therapies, many of the respondents felt Befriending and Support Groups were
important for people who had mental health problems to enable them to talk about their issues,
gain support from others who had experiences that were similar to theirs.
The importance of such support was seen as crucial in assisting people to maintain social
relations and community cohesion
11. Has your faith in anyway helped you overcome loneliness or depression? If so how?
A prevalent theme to reducing isolation and depression was the role that faith played at an
individual and group level. Many sought solace in their religion through, prayer.
This was undertaken both at home on an individual level, and/or as a group activity.
The following are examples of how this was followed: • Prayer • Singing Bhajans (Hindu Hymns) • Visiting a Gurdwara (Sikh Temple) • Mandhir (Hindu Temple) • Mosque (Muslim Place of worship) five times a day • Singing Naats (Islamic Hymns) • Namaz (Prayer) • Reciting the Quran (Muslim Holy Book)

51
5.1 Discussion
During the course of the project a number of discussions have been stimulated in relation to the future work that needs to be undertaken. We have undergone a very steep learning curve and at the same time we have consolidated our current good practice in the way we have been able to access and have dialogues with so called “hard to reach communities.”
In relation to gender over 70% of the respondents were women. It is an interesting indicator that less men were willing to participate then women, whether this is due to the fact the more men know about Mental Health then women, or whether this was due to the fact that they did not want to discuss the issues needs further exploration.
In relation to ethnicity and religion we had a very mixed grouping, with participants from Bangladesh, East Africa, India, and Pakistan, with over a quarter seeing themselves as Asian British and almost all were British citizens who had been living in Newham for more than 11 years.
There was a mixture of religions that were cited in the questionnaires, the majority; nearly half
were Hindu, followed closely by Muslims and then Sikhs. Faith/Spirituality was seen by many
people as very important part, and was seen as an integral part of their everyday life, which was
not just about timings and prayer. Many found solace in their faith as many felt isolated.
In relation to languages 99% of the group felt more comfortable in speaking an Asian language
and these ranged from Bengali, Gujarati, Punjabi and Urdu. Hindi/Urdu was seen as a universal
“language” which was seen as more beneficial in understanding than English, only 21% spoke any
English. Many respondents were multi lingual. Hence, the right communication was seen as an
integral part of accessing information
Many people felt that they were not well informed in relation to what were perceived as Mental
Health issues, as well as how to access services.
The fact that many people did not want to talk about Mental Health in some part relates to the lack
of awareness mentioned above as well as the stigma attached to mental health and the impact
this illness can have on Asian communities.
Three fifths of those involved had a disability which impacted on their lives in relation to isolation
and their lack of confidence.
Another issue that raised a lot of discussion was the “sexuality” question 23 in the questionnaire.
There were respondents who refused to answer the question at all, whereas others were very
uncomfortable with the question, and this created. Interviewers gave examples, but as the words
were not easily transferrable, the situation was tense.
Depression, stress related issues and memory loss were known as issues for those who were
interviewed. However, over half had no idea of what services were available to them. A small
number had used individual counselling or support groups. For those who had used a service in
relation to a GP, Hospital, over three quarters said that an Advocate or Interpreter had not been
provided to them, which meant they found it very difficult to understand what was being said to
them.
In relation to therapies, reading religious texts was seen as very therapeutic with over half of
participants using this, with smaller numbers using Reiki, Faith healing and Head massage, with
over half of those involved

52
There were some elders who had no friends or visitors outside of social or health care services;
others had family who visited them. However, there was a high proportion who felt lonely, some
who were extremely lonely and were worried and upset because of their isolation.
Almost half of the respondents were Asian elders who lived alone. Many had expectations that
they would be living in an extended family network in the same accommodation. The impact on
wellbeing, their dreams and hopes of being looked after as they grew older was very difficult to
come to terms with.
5.2 Impact and Sustainability
Some of the most interesting discussions have been held which have led to identifying work that
needs to be undertaken with Asian elders and their carers in the community and on hospital wards
and residential and nursing homes relating to:
• Case work • Befriending • Advocacy
Alongside this work we will be exploring how we can work with staff who are currently working with
Asian elders and their carers:
• Compiling information for staff institutions • Identifying resources available • Activities • Outreach and development work with voluntary and faith organisations
There is a need to investigate concepts of sexuality further and look at how work can be
undertaken so that the concepts and terms are not seen in a derogatory or offensive manner.
To further investigate the above, SubCo is currently researching and compiling a range of funding
streams that we may be able to access from Charitable Trusts as well as Statutory funders.
Running parallel to this, at SubCo, we will be reviewing some of our priorities over the next 3 years
in relation to mental health and dementia, impact on staff development, organisational
development and service user engagement.
The impact of the findings of our Community Engagement Project has an impact on how services
are currently provided in Newham in identifying how we can move forward together to demystify
services.
The fact that there is a lack of awareness of concepts around Mental Health raises a number of
further questions:
How to relay information and have discussion that is meaningful to Asian elders, family carers?
How to engage with the local community, voluntary and faith organisations etc?

53
What services are provided, and whether they meet cultural, linguistic and religious lifestyles are
important factors that need to be reviewed and Action Plans instigated?
Our findings show that in relation to the DRE findings on the building blocks around access,
community engagement and the provision of information highlights that there is still a long way to
go.
This project has raised begun the awareness raising process with individuals and groups, for
example, of Asian elders, carers, staff and volunteers from SubCo, as well as professionals from
the statutory sector.
In relation to our priorities at SubCo, we have identified the area of Mental Health as a priority over
the next 3 years. This has led us to look at developing a Business Case around unmet needs in
relation to Mental Health services and Asian elders.
We are also developing funding proposals to take this work forward and we are in the process of
identifying potential funders, for work that needs to be carried out locally an area that needs to be
prioritised and developed in the future.
6. Reflection
Over all attending the workshop, not only helped us gain the qualification, it also prepared us for
each step of our research. For example, how to conduct the questionnaire, and how to divide
different type of data, also what approached to use when analysing collected data. This
qualification has equipped us with the essential tools for carrying out any community research. We
not only completed our research, we also got the change to put the learnt material in to practices,
as both things were been done simultaneously. We have learnt a lot from the research and
qualifications, and both have given us great confidence for when doing similar work in future.
We had to attend 5 workshops of which 2 were for mental health policies and three were based on
community research. Three members of the research team attended the workshop for the
Qualifications. Two members gained the qualification for Community Research and Mental health,
and two members successfully achieved the certificate in Community research.

54
7 Recommendations
1 To combat the lack of awareness of the range of Mental Health services available in Newham by reviewing how work is currently undertaken To develop an outreach programme that reaches out into the community and enable discussions of Mental Health and its impact on Asian communities
2 To develop a partnership programme with local community groups, voluntary organisations and faith groups (Places of Worship) to highlight issues of Mental Health
3 To recruit staff who speak a range of Asian community languages and dialect, both in frontline and Advocacy roles
4 To lobby for the development of Community Development Workers for Older People
5 To review and develop existing services run by the East London NHS Foundation Trust and other Mental Health providers such as the Adult Services, The Newham Primary Care Trusts etc., in the community and in institutions to ensure that they meet the needs of Asian elders referred there taking into consideration gender, diet, language and dialect, interests, religion etc.
6 To ensure access to universal services to ensure social inclusion of Asian elders and their family carers
7 To develop Mental Health information that is targeted at the Asian Community
8 To develop support groups for Asian elders who have mental health issues to reduce isolation and loneliness
9 To monitor progress on implementation of the above needs and report back to appropriate Boards, e.g. East London NHS Foundation Trust, Newham PCT, Older peoples Partnership Board, Overview and Scrutiny Board etc.
10 To establish an Implementation Group to monitor progress of actions identified

55
8 References
Department of Health Social Services Inspectorate (March 2003) Inspection of Social Care
Services for Older People: London Borough of Newham
Felton, S. (1987) Ageing Minorities: Black People as they Grow Old in Britain, Commission for
Racial Equality, London
Griffiths S. (2006) Smiling More Often Report, Healthy Wise London
Norman, A, (1985) Triple Jeopardy: Growing Old in a Second Homeland, CPA
GLA (2003) Round Ward Level Population Projections
Office for National Statistics, 2001, 2001 Census Standard Tables
Office for National Statistics, (2003) Resident Population Estimates

56
9.1
Souc
hein
Pos
ter a
nd B
ooki
ng L
ette
r

57
9.2
Souc
hein
Que
stio
nnai
re

58

59

60

61
9.3 Questions for Souchein Focus Groups.
1) What is your understanding of Mental Health?
2) Amongst Asian communities Mental Health is an issue which is often frowned upon and hardly spoken about, what do you think are the possible reasons for that?
3) What are the causes of isolation on one’s health?
4) If you have accessed any Mental Health services how was your experience, and what suggestions can you offer for future improvements to make these services more accessible to Asian elders?
5) What therapy would you use or recommend to someone is going through isolation?
6) Has your faith in anyway helped you overcome loneliness or depression? If so how?

62
9.4
Souh
ein
Cons
ent
Form
- D
eliv
erin
g Ra
ce E
qual
ity
Men
tal H
ealth
Com
mun
ity E
ngag
emen
t Pro
ject
1:1
Inte
rvie
ws
Con
sent
:
The
abov
e ha
s be
en e
xpla
ined
to m
e.
I ag
ree/
do n
ot a
gree
* to
part
icip
ate
in a
1:1
inte
rvie
w
Yes
[ ]
N
o [
]
Plea
se ti
ck a
ppro
pria
te b
ox
I giv
e/do
not
giv
e* c
onse
nt fo
r the
info
rmat
ion
I hav
e di
sclo
sed
to b
e us
ed fo
r thi
s pr
ojec
t
Yes
[ ]
N
o [
] Pl
ease
tick
app
ropr
iate
box
*Del
ete
appr
opria
tely
We
wou
ld li
ke to
than
k yo
u in
adv
ance
for y
our c
oope
ratio
n!
Souh
ein
Cons
ent
Form
- D
eliv
erin
g Ra
ce E
qual
ity
Men
tal H
ealth
Com
mun
ity E
ngag
emen
t Pro
ject
Focu
s G
roup
s
Con
sent
:
The
abov
e ha
s be
en e
xpla
ined
to m
e.
I ag
ree/
do n
ot a
gree
* to
part
icip
ate
in a
1:1
inte
rvie
w
Yes
[ ]
N
o [
]
Plea
se ti
ck a
ppro
pria
te b
ox
I giv
e/do
not
giv
e* c
onse
nt fo
r the
info
rmat
ion
I hav
e di
sclo
sed
to b
e us
ed fo
r thi
s pr
ojec
t
Yes
[ ]
N
o [
] Pl
ease
tick
app
ropr
iate
box
*Del
ete
appr
opria
tely
We
wou
ld li
ke to
than
k yo
u in
adv
ance
for y
our c
oope
ratio
n

63
9.5 Guidelines for One to One Interviews
Introduction
This guideline will assist you to prepare you and prompt you to conduct yourself in an appropriate
manner with the participant you are interviewing. So please familiarise yourself before each
interview. You will have acquired these skills previously through training and support as volunteers
and workers as part of this project. Your multi lingual skills will be an asset to delivering this work,
as well as your working with elders and vulnerable adults. It is important that you remember to pay
particular attention to the following:
1. Ensure that the room has been booked and the seating arrangements are appropriate. 2. Ensure that your “escape” route has been planned in case the participant becomes angry,
violent etc and you have to leave immediately. 3. Greet the participant and make sure they are comfortable and address them appropriately
by name or term, e.g. “Mr,” “Mrs” “Aunty,” “Uncle” etc. 4. Ensure that seating is comfortable, if the person is a wheelchair user that the wheelchair is
positioned appropriately so that they can see you. Sit opposite the participant so that they can see you at all times.
5. If you know the participant, ask them if they would prefer to have another interviewer so that they can feel comfortable in answering some of the questions.
6. If they ask for another interviewer, then it is important that you end the interview immediately, but on a positive note. Explain that you will need to find another interviewer, and if this is not possible immediately, then you will need to arrange another time/day for the interview.
7. Engage with them in a friendly and professional manner and explain to them what you intend to do, i.e. ask them questions regarding their views on Mental Health issues and/or services.
8. Explain to them that if they do not wish to answer a question they do not have to. 9. If they want to end the interview they can do so at any time. 10. It is important that you explain that information from the questionnaire will be used for
purposes of a report and that confidentiality will be maintained in relation to their identity. 11. However, confidentiality will be broken if it appears, that they are likely to harm themselves
or someone else, then it will be necessary to report this to the appropriate authorities. 12. Please ensure that you ask them to complete and sign the Consent form. You may offer
them assistance where appropriate. 13. Ensure that your body language is positive, and that you maintain eye to eye contact where
possible, in between completing the questionnaire. 14. If the participant becomes upset, allow them time to recover and console them. 15. Ensure that you pace yourself, however, you should explain that the interview is to last
approximately 1 hour. 16. If the participant does not understand the question, paraphrase it, if there is still a difficulty
then give them a couple of examples that you are familiar with from the training sessions 17. If a conflict situation arises, explain that you will have to end the interview and call for
assistance from another colleague. 18. If issues are raised, that you have concerns about in relation to the service user, or if they
ask for assistance around a service etc., then it is important that you discuss this with a senior person after the interview, so that an appropriate referral can be made to an appropriate service(s).
19. When you have finished asking the questions, thank the participant for their time and show them to another room for a therapy session, lunch etc.
20. Please ensure that all completed questionnaires are returned to the project leaders

64
9.6 Application for ethical approval
Centre for Ethnicity and Health – Application for Ethical Approval
Name of Group SubCo Trust
Address 49 Plashet Road, Upton park, London E13 0QA
Name of Support Worker Imran Mirza
Date: 24th August 2007. Revised 22nd October 2007.
Section 2:
What kind of work does
the group intend to do as
part of this project?
SubCo will undertake community research work
with approximately 100 Asian elders and their
carers in the London Borough of Newham.
This work will be both qualitative and quantitative
and we will be aiming at:
a) Asian Elders – over the age of 55yrs based in
the community
b) Asian Carers – ages will vary – based in the
community
The project will be undertaken by bilingual and tri
lingual Community Engagement workers and
volunteers who will between them be able o
communicate in: Bengali, English, Hindi,
Guajarati, Punjabi, Swahili, and Urdu.
Issues around gender preferences due to cultural
reasons will also be respected.
SubCo aims to gather information from
questionnaires, focus groups and discussions
with the 2 key professionals Ian Kennedy –
Group Manager: Older People & General
Services, Michael McGhee –General Manager:
in order to build a picture of :
1 How current services are provided 2 What are the current gaps and barriers to
accessing services 3 How current barriers can be removed in
order to improve services
The information gathered will be analysed and a
final report will be produced with

65
recommendations for current commissioners and
providers of services n the London Borough of
Newham.
The report will highlight the results of the
research undertaken. In turn this will enable
commissioners and providers of services to:
o Look at how they commission services o How services can be made more culturally
and linguistically appropriate o Removing unnecessary barriers to enable
access to services o To review how services are currently
provided and refocus on areas such as training, core competencies required, make up of staff to reflect the community
The report will be launched at a public meeting
where invitees will range from professionals,
Asian elders, Asian carers, the Steering Group,
relevant community and faith groups, the local
press and other interested parties.
The report will be formatted with a range of
photographs and graphics used from other
generic services provided by SubCo. An
executive summary will also be available in a
range of relevant languages.
The report will also be presented to formal routes
within the Local Authority, the Primary Care Trust
and the East London Community Mental Health
Trust through the relevant Partnership Boards
and Scrutiny Groups.
The report will also be available on our website.
How do they intend to do
this?
The research tools that will be used include: one
to one questionnaires which will be undertaken in
structured interviews and focus groups.
The team consists of 3 Community Engagement
workers, 10 volunteers, a steering group and the
coordinator of the project (who is the Chief
Executive of SubCo Trust).
A questionnaire has been developed which will
be piloted in the first instance to ensure that the
questions are relevant and comprehensive. As
the questionnaires will be written in English, it will
be imperative that certain concepts and phrases

66
are relevant when translated into the various
languages.
The interviews will be undertaken at our Centre
as one to one interviews, and we will ensure that
there is privacy by ensuring that the interview
cannot be overhear by any one apart from the
interviewer and interviewee.
The interview will be conducted in the language
of the interviewee’s choice to enable appropriate
dialogue. Interviewers will be trained to undertake
the interviews in the appropriate language.
Interviewees will also be offered the choice of a
male or female interviewer and this will enable
the interviewee to feel more comfortable in
answering questions around personal lifestyles,
experiences and issues triggering mental health
in relation to isolation, loneliness cognitive or
functional illness.
Although there questionnaire is to be conducted
in a structured interview, interviewers will be
provided with at least 2 training sessions to
enable them to engage with the interviewee and
to make them feel as comfortable as possible
when answering questions. For example, using
positive body language, appropriate tone and
manner. If additional support is needed this will
be provided during the community engagement
work.
We will also look at sharing techniques with
interviewers in relation to ending interviews if an
interviewee finds the questions or their answers
overwhelming and does not want to continue.
Training will be provided by some of the
members of the Steering Group as well as the
UCLAN Support worker.
Approximately 50 Asian elders will be
participating in one to one interviews.
Answers will be noted on the questionnaire by
the interviewer.
We intend to hold 4 focus groups. The make up
of these groups will vary and we will be able to
offer:
67
Asian Carer Women only group
Asian Carer Men only group
Asian elders Men only
Asian elders Women only
The focus groups will last for approximately 1 hr
and 15 minutes, and each group will have the
same themes running throughout relating to
issues around:
o Isolation and loneliness o Experiences of services o Suggestions of how services can be
improved o Access or lack of access to services o Barriers encountered o How services could be improved o Discussions about specific illnesses o Language specific
There will be a facilitator and a co facilitator who
will be leading the group
2 training sessions developed which will be
around:
o Aim of the focus group o What we hope to achieve o Dynamics of Group work o Working with vulnerable adults o How to deal with conflict
Who will the respondents
be?
The respondents will be Asian elders from the
age of 55yrs, and carers of Asian older people
(no age restriction) living in Newham who have
had experiences in relation to Mental Health.
Some of the respondents will be known and are
held on SubCo’s database will be contacted via a
letter, leaflet and personal contact.
We will also write to other organisations, for
example, Age Concern Newham, Newham
Carers Network, and Sheltered Housing
Schemes.
Potential respondents will be invited to participate
in the project, and offering the choice of one to
one interviews and/or a focus group.
We aim to have 50 Asian elders for the one to

68
one questionnaires.
W aim to have 50 Asian elders and carers in the
5 distinctive focus groups.
Total 100
Who will they get to do the
work?
The Team will comprise of 3 Community
Engagement Workers, and there will also be
approx 10 volunteers. Other members of the
SubCo Trust Team will also be available where
appropriate.
The Community Engagement Team comprises of
both men and women who speak a range of
Asian languages and Swahili amongst them.
The volunteers will be made up of service users,
volunteers from the community with a range of
community development and community
engagement experience. All will have had
experience of working with vulnerable adults
and/or carers.
Where they will undertake
the work?
In the London Borough of Newham at our centre
and the Older Peoples Resource Centre in
Newham.
Confidential space will be provided for one to one
interviews.
For the focus groups we will ensure that the
rooms booked are of adequate size and are
accessible to Asian elders who are wheelchair
users, use mobility aids or have other specific
requirements.
How will those who are
doing the work be
supported and
supervised?
The workers and volunteers will be supported by
a coordinator in the first instance.
There will be monthly supervision meetings held
for workers and volunteers, as well as regular
weekly group meetings during the interviews and
focus group stage.
The work will be monitored by a Steering Group
which will also meet regularly on a 4 week basis.
The Steering Group is made of: Ian Kennedy –
Group Manager: Older People & General
Services, Michael McGhee –General Manager:
Older persons Services Jane Tilston –Integrated
Commissioning Manger, Older People Taskin

69
Saleem – Chief Executive, SubCo Trust, Tim
Bishop, FIS, Denise Bobb, REL, Ghulam Hussain
- Service User, The 3 main Community
Engagement Workers as and when appropriate.
How they will ensure that
participants in the project
have given consent? You
should have an
information sheet about
the project which is read
out and given to potential
participants which
explains to them (a) what
the project is about.(b)
that participation is
voluntary (c) what will
happen to the information
that they provide (d) that
they can stop the
interview at any time and
(e) that they do not have
to answer any questions
that they do not want to.
We will ensure that attached to the questionnaire
is a separate sheet that explains what the
participants are giving consent to. There will a
tick box.
Please see attached sheet.
Please enclose the
information sheet and
confirm that it addresses
issues (a), (b), (c), (d) and
(e) above
Information sheet enclosed ( x ) tick to confirm
Issue (a) covered ( x ) tick to confirm
Issue (b) covered ( x ) tick to confirm
Issue (c) covered ( x ) tick to confirm
Issue (d) covered ( x ) tick to confirm
Issue (e) covered ( x ) tick to confirm
How they will the project
ensure confidentiality?
Note: you will not usually
need to know (or collect)
the names or addresses
of respondents.
If you know them already,
or if you are going to ask
people their names as a
matter of courtesy, these
We will ensure confidentiality by ensuring:
o That staff have signed up to a confidentiality clause as part of their contract of employment which stresses the importance of maintaining confidentiality
o That volunteers have signed up to a confidentiality clause as part of their volunteer contract – as above.
o That if in a one to one interview, it is found that the individual knows the Community

70
should not be recorded on
the questionnaires or the
notes that relate to the
interview.
Note: you cannot
guarantee confidentiality
to anyone taking part in a
focus group. You can
request that people keep
things within the group,
but you cannot guarantee
that the will. This must be
made clear to people who
agree to participate in
focus groups.
Engagement Worker, the participant can ask for another interviewer. If they want to continue with the same interviewer than they will be reassured that the information will remain confidential and their anonymity is preserved.
o That in a focus group that the ground rulesensure that participants and facilitators agree to maintain confidentiality. However,we will make it clear that maintaining confidentiality is dependent on the individuals and not the Project.
o There will be limits to confidentiality, and therefore we cannot guarantee total confidentiality. The information that we receive as a research team will be treated as confidential, and we will not pass this on to anyone else in a way in which it can be attributed back to any individual unless we are given information which leads us tobelieve that someone is at risk of serious harm, including child abuse. In this event, we will need to pass the informationon to other relevant bodies (such as a GP, the police, or a social worker) in order to try to prevent or stop the harm.
How will data generated
by the project be handled
and stored?
The data generated by the project will be subject
to the Data Protection Act. We will also ensure
that all information is stored in secure and locked
filing cabinets.
Questionnaires will not have names on them,
only a reference number which will identify
information if it needs to be cross referenced.
Where information is stored on the computer we
will ensure that the data is protected via
passwords.
What risks are there?
How will risks be identified
and managed?
Note you need to think
about risks to researcher
and volunteers and risks
to participants. For some
people, simply taking part
We will undertake a risk assessment and this will
identify:
Risks to the Community Engagement Workers &
Volunteers. There may be risks in relation to the
issues brought up by respondents that may affect
the emotional and well being of the team. For
example, issues relating to Adult Protection,
bereavement, or poor service delivery, conflict,
breakdown of extended families networks etc.

71
in the research may be a
risk (e.g. if the parent of a
young Muslim woman
finds out that she has
been talking to someone
about drugs). For others,
particular situations may
be risky (e.g. if you are
using ex-drug users to
work on the project, are
you putting them at risk of
relapse by asking them to
go back into situations
where drugs are being
sold or used? If
something gets stolen
from an office, will they
get blamed for it
[regardless of whether or
not they did it] because
everyone knows they are
a drug user?). Are the
interviewees particularly
vulnerable or frail? Are
interviewers likely to be
vulnerable to allegations
of misconduct?
Are the risks of carrying
out or participating in
individual interviews
different from those of
taking part or running a
focus group? They
probably are, and you
need to show that you
have thought about and
addressed this.
THIS IS ONE OF THE
MOST IMPORTANT
SECTIONS OF THE
FORM. YOU MUST
THINK CAREFULLY
As part of the induction programme the team will
have briefing sessions that focus on managing
risk during the life of the project. Particular
attention will be given to one to ones and focus
groups.
We also provide a time to be able to discuss
“coping strategies” at team meetings, in
supervision and support sessions as agenda
items.
SubCo’s Human Resources network will provide
access to emotional support via where
counselling can be made available for the team
to talk through these issues either on a one to
one basis or as a group.
We will not be undertaking any home visits so
risk here will be minimal. However, as team
members will be undertaking one to one
interviews in a private office, meeting room etc
we will ensure that precautions are taken in
relation to seating arrangements, access to panic
alarm, etc.
Similarly, in a focus group the above precautions
will be taken. As well as looking at risks to
confidentiality.
The risks in relation to confidentiality will be
highlighted at group sessions. We will try to
minimise risk by stating at the beginning of the
session when ground rules are discussed that
participants sign up to ensuring information
remains confidential. However, participants will
be briefed that it is important that they do not
discuss particular issues if they feel
uncomfortable.
As we are working with vulnerable elders, it is
possible that an elder may get distressed, have a
panic attack or fall ill. We will ensure that there
are First Aiders on hand. Where appropriate we
will contact the emergency Ambulance Services
as well.
Therefore as well as a facilitator and co facilitator
being available to run the group, we will ensure

72
ABOUT WHAT THE
POSSIBLE RISKS ARE
AND ABOUT WHAT
STEPS CAN BE TAKEN
TO REDUCE AND
MANAGE THEM. THE
ETHICS COMMITTEE
UNDERSTANDS THAT
IT IS USUALLY
IMPOSSIBLE TO
ERADICATE EVERY
RISK, BUT THE ETHICS
COMMITTEE MUST BE
SATISFIED THAT ANY
RISKS ARE
REASONABLE, AND
THAT STEPS HAVE
BEEN TAKEN TO
MINIMISE THEM
that there are volunteers on hand who can assist
in managing the situation and provide
reassurance to other participants of the Focus
Group.
We will also ensure that access to premises meet
Health and Safety Guidelines in relation to
minimizing hazards in the environment, COSH,
as trailing leads, appropriate lighting, seating etc.
Again team members will available to assist
where necessary.
CRB checks will be undertaken.
Please confirm the make
up of the steering group
The Steering Group is made of: Ian Kennedy –
Group Manager: Older People & General
Services, Michael McGhee –General Manager:
Older persons Services Jane Tilston –Integrated
Commissioning Manger, Older People Taskin
Saleem – Chief Executive, SubCo Trust, Tim
Bishop, FIS, Denise Bobb, REL, Ghulam Hussain
- Service User, Imran Mirza, UCLAN Support
Worker, the Community Engagement Workers
and volunteers as and when appropriate.
How often does the
Steering Group meet. It
needs to meet often
enough to both guide the
research and keep it on
track, and to pick up on
any ethical issues that
may arise.
The Steering group meets on a 4 weekly basis.
For those who are on e mail, there are “round
robin” discussions as and when needed. For
those who are not, e.g. the service user, they are
briefed and their feedback taken as and when
appropriate.
Is the Steering Group
clear that is has a
responsibility for helping
to manage the ethical
issues that may arise as a
result of running this
project?
Yes, the Steering Group is aware of these
responsibilities and will also be sent a copy of
this form.

73
Section 3: To Be Completed By UCLan internal ethics committee
Date received:
Reviewed by: Kate Davies, Jez Buffin, Christine Brown
Decision: We don’t mean to be pedantic, but pleased make
sure that you read your work through carefully
before you submit it or send it out. There are
several issues above which are unclear, simply
because of poor or incomplete wording. A
simple read through by the group and the
support worker should have picked these up.
Please clarify the issues raised as possible
typing errors on pages 1, 3, 4 and 5.
Otherwise this is pretty good, with only a few of
points to address
1. Please rectify your confidentiality statements so that you are clear that you will not be guaranteeing confidentiality to anyone in the event that they disclose information that suggests that they or someone else is at risk of serious harm.
2. Think through the issue about using photographs in the final report as discussed above
3. Review your steering group membership to ensure links to the REL and FIS
4. You need to amend your consent forms as indicated. We have developed new forms for you – one for 1:1 interviews and one for focus group (see below)

74
9.7 Steering Group Terms of Reference
1. The role of the Steering Group is to oversee the project
2. The Steering Group to meet every 6 weeks
3. Membership of the Steering Group will consist of a range of partners: Service Manger for Mental Health, Service Manager for Social Work Safeguarding Adults, the Integrated Commissioning Manager for Older Peoples Services from different sectors, and at least 1 Service User, the Chief Executive of SubCo, the Support Worker from UCLAN
4. To assist with research tools, interviews, draft questionnaires, outcomes etc
5. To look at preliminary findings
6. To link to the DRE Building Blocks
7. To monitor the Action Plan and agree milestones
8. To identify future training needs, opportunities in relation to the commissioning and provision of services in Newham


75
SubCo Trust Ltd. 49 Plashet Road, Upton Park. London E13 0QA
T: 020 8548 0070 F: 020 8472 2696 Website: www.subco.org.uk
Company Limited by Guarantee Number: 3031652
Registered Charity Number: 1045237







