
Health Technology Assessment (HTA)
Determination of utilities for the QLQ-C30
Georg Kemmler, Eva Gamper, Bernhard Holzner
Department for Psychiatry and Psychotherapy Innsbruck Medical University
Austria
Introduction
• Increasing importance of health economics and HTA in cancer research ( cost-utility analyses)
• Special “utility based“ QOL instruments are required for performing such analyses (like EQ-5D, SF-6D)
• Development of utility-based versions of the QLQ-C30 has been intiated, but so far restricted to English language versions (AUS, UK) ( next page)
• Versions for various European countries with national utility weights are required to make the QLQ-C30 a competitive utility instrument

Utilities for the EORTC QLQ-C30 The larger framework
• Study 1 (D Rowen, J Brazier et al.*): Utilities for the QLQ-C30 in multiple myeloma patients based on 8 of the 30 EORTC QLQ-C30 items (EORTC-8D, finished)
• Study 2 (M King et al.**): Utilities for the QLQ-C30 in a general population sample Stage 1: Determination of the number of domains (finished, 10 domains/items ) Stage 2: Determination of utilites by Discrete Choice Experiments (feasibility testing just started)
• Study 2a (EORTC QLG, in cooperation with M. King et al.):
Country-specific utilities for the QLQ-C30 (planning phase)
* Rowen D, Brazier JE, Young TA, Gaugrist S, Craig BM, King MT, Velikova G. Value Health 2011
** Consortium on Multi-Attribute Utility in Cancer MAUCa (M King, …, N Aaronson, G Velikova et al.)
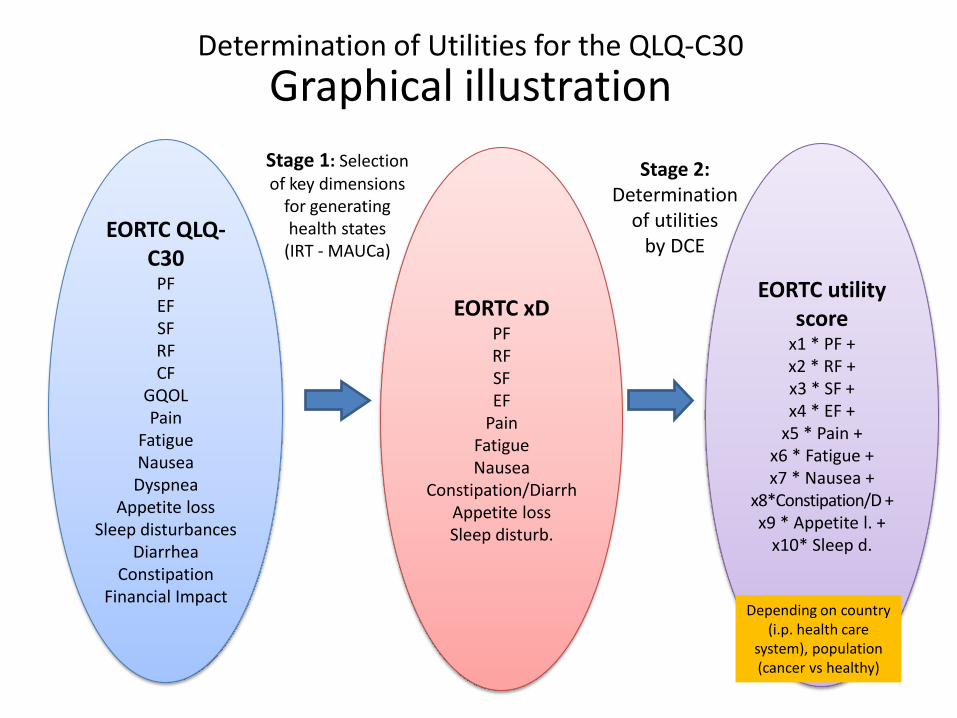
Determination of Utilities for the QLQ-C30
Graphical illustration
EORTC QLQ-C30
PF EF SF RF CF
GQOL Pain
Fatigue Nausea Dyspnea
Appetite loss Sleep disturbances
Diarrhea Constipation
Financial Impact
Stage 1: Selection of key dimensions
for generating health states
(IRT - MAUCa)
EORTC utility score
x1 * PF + x2 * RF + x3 * SF + x4 * EF +
x5 * Pain + x6 * Fatigue + x7 * Nausea +
x8*Constipation/D + x9 * Appetite l. +
x10* Sleep d.
Stage 2: Determination
of utilities by DCE
EORTC xD PF RF SF EF
Pain Fatigue Nausea
Constipation/Diarrh Appetite loss Sleep disturb.
Depending on country (i.p. health care
system), population (cancer vs healthy)
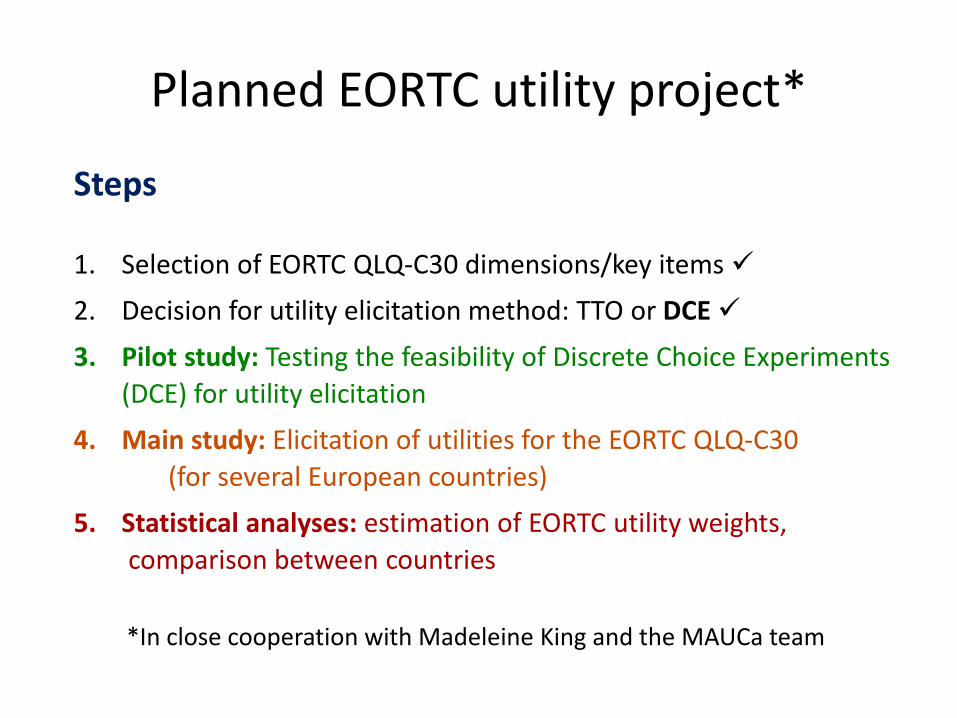
Planned EORTC utility project*
Steps
1. Selection of EORTC QLQ-C30 dimensions/key items
2. Decision for utility elicitation method: TTO or DCE
3. Pilot study: Testing the feasibility of Discrete Choice Experiments
(DCE) for utility elicitation
4. Main study: Elicitation of utilities for the EORTC QLQ-C30
(for several European countries)
5. Statistical analyses: estimation of EORTC utility weights,
comparison between countries
*In close cooperation with Madeleine King and the MAUCa team
Testing the feasibility of Discrete Choice Experiments (DCE) for utility elicitation:
First results of the Austrian pilot study
• Small sample of healthy controls (N=47), patients planned
• Each participant had to complete 12 individual DCEs (comparisons “Life A“ vs. “Life B“)
• Two different designs tested: black and white vs color ( )
• Test acceptability and feasibility
• Test for an effect of the design/layout
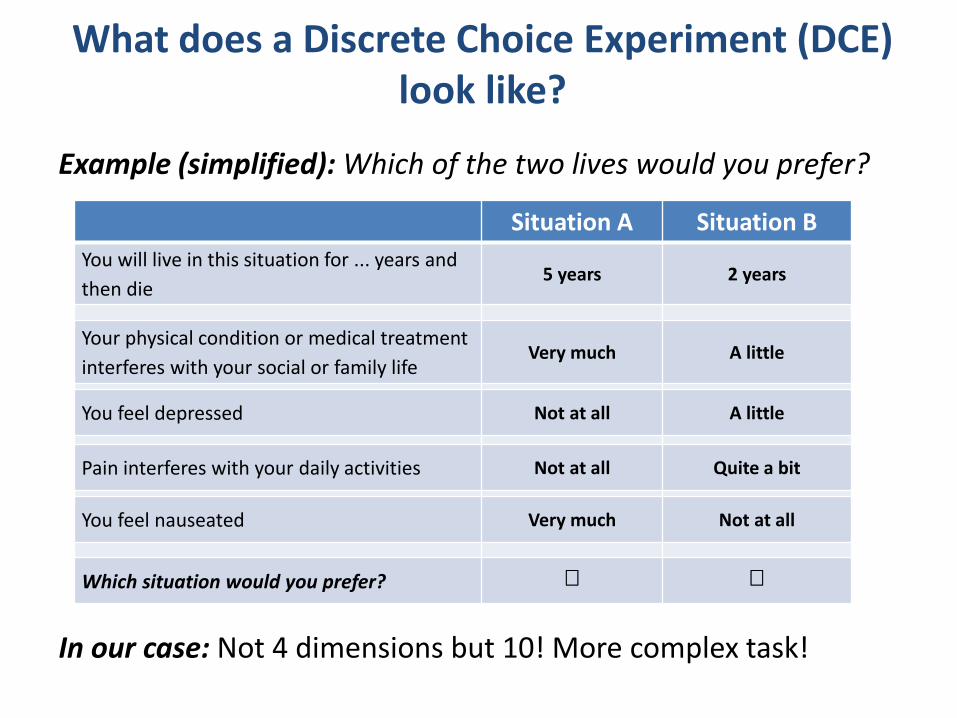
What does a Discrete Choice Experiment (DCE) look like?
Example (simplified): Which of the two lives would you prefer?
In our case: Not 4 dimensions but 10! More complex task!
Situation A Situation B
You will live in this situation for ... years and
then die 5 years 2 years
Your physical condition or medical treatment
interferes with your social or family life Very much A little
You feel depressed Not at all A little
Pain interferes with your daily activities Not at all Quite a bit
You feel nauseated Very much Not at all
Which situation would you prefer?
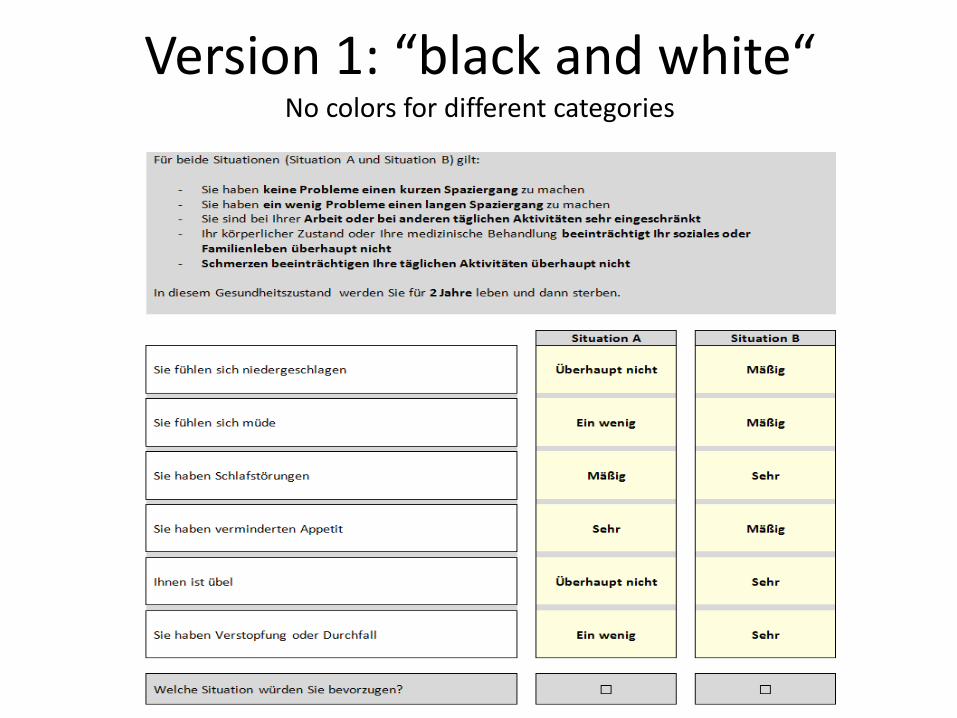
Version 1: “black and white“ No colors for different categories

Version 2: “color“ green (not at all) – yellow (a little) - orange (quite a bit) - red (very much)
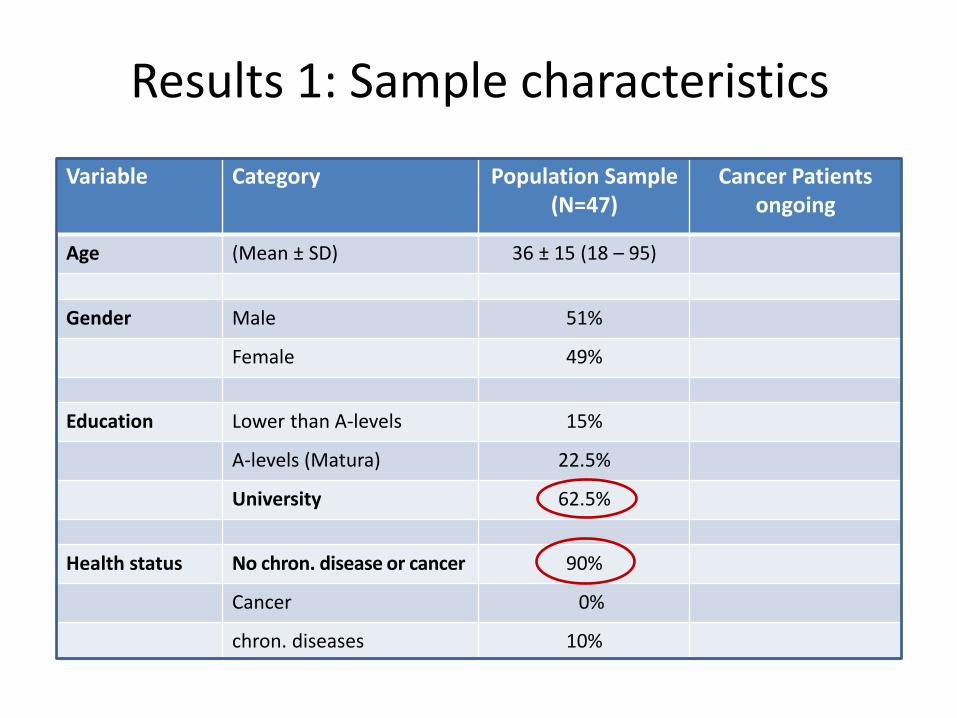
Results 1: Sample characteristics
Variable Category Population Sample (N=47)
Cancer Patients ongoing
Age (Mean ± SD) 36 ± 15 (18 – 95)
Gender Male 51%
Female 49%
Education Lower than A-levels 15%
A-levels (Matura) 22.5%
University 62.5%
Health status No chron. disease or cancer 90%
Cancer 0%
chron. diseases 10%
Results 2: Acceptability & Feasibility
Acceptability • All persons approached were willing to participate
• No complaints about annoying or intrusive questions
• However: possible selection bias (fairly high level of education!)
Feasibility • Every respondent was able to understand the task
• Clear explanations were essential (set of dimensions, severity levels)
• Problems were mentioned by a considerable proportion of persons (e.g. difficulties to imagine certain health states/ combinations)

Results 3: First statistical analyses
• In 7 of the 12 individual DCEs: clear preference for one to the two situations (>80% for one option, <20% for the other)
• In 5 of the 12 DCEs: opinions were more split
• Most influential dimensions: Nausea and Fatigue
• Color vs. black & white: Majority preferred color (73%), so far no significant differences between color and b & w
Limitations
• Utilities for individual health states can not yet be determined – too few cases, too few distinct DCEs
Summary: Aims of the planned EORTC QLG project
• General aim: Determination of country-specific utilities for the EORTC QLQ-C30
- many countries
- population sample and possibly cancer patients
• Phase I: Country-specific utilities for a few European countries (general population sample)

Many thanks for your attention!







