
4/3/2018
1
New Compounding Ideas and Marketing Innovation
Ranel A. Larsen, Pharm D, RPh
Erin Michael, MBA, CPhT
Objectives1. Explain common dental conditions encountered by
compounding pharmacists and technicians.2. Discuss the latest compounded treatment options
being prescribed for specific dental conditions.3. Describe formula examples and clinical applications
utilizing various compounded formulations.4. Understand the mechanism of microneedling and the
conditions it can be used for.5. Describe the procedure when using a microneedling
device.6. Explain the different active ingredients used along
with microneedling.
Target Markets
• Dentists
• Dermatologists and Cosmetic Patients

4/3/2018
2
Compounding for Dental Aliments
Common Dental Conditions
• Oral Mucositis
• Dry Mouth
• Lichen Planus
• TMJ
Mucositis
Inflammation of the mucosal membranes which can cause extreme pain, redness, ulcers and infections.
Most commonly a complication of chemotherapy and/or radiation treatment.

4/3/2018
3
Mucositis can significantly impact nutritional intake, mouth care and quality of life. Severe cases require a reduction in the chemotherapy dose or a break in the radiation treatment which
can negatively influence prognosis.
Treating Mucositis
• Multinational Association of Supportive Care in Cancer (MASCC) Pain Control Recommendations
– 2% Morphine Mouthwash
– 0.5% Doxepin Mouthwash
– Transdermal Fentanyl
”For compounded preparations such as mouthwashes, there are various formulations that
pharmacists can use based on the experience and needs of the individual physician and patient,
respectively.”
4/3/2018
4
“Magic Mouthwash”
Common APIs
Anesthetics
Diphen-hydramine
Anti-bacterials
Anti-fungalsSteroids
Misoprostol
Soothing Agents
(Maalox®)
Compounding Pearl - Nystatin

4/3/2018
5
Commercial Nystatin contains sugar
Sugar Feeds Yeast
Don’t use commercial product – use the raw powder
Compounding Pearl - Nystatin
Compounding Pearl - Ethanol
• The metabolism of ethanol (EtOH) by mucosal and/or bacterial alcohol dehydrogenase generates toxic metabolites such as acetaldehyde and free radicals. – Acetaldehyde accumulation
can damage the oral tissues. It interferes at many sites with DNA synthesis and repair
Make sure your vehicle
doesn’t contain EtOH
Mucositis - Formulas• Stanford Mouthwash
– Tetracycline 12.5mg/ml– Nystatin 12,000 U/ml– Hydrocortisone 0.46mg/ml– Diphenhydramine 1.25mg/ml
• Nystatin 12,500 U/ml / Hydrocortisone 0.25 mg/ml /Diphenhydramine HCl 2.5 mg/ml Mouthwash
• Misoprostol 0.0024%/Diphenhydramine HCl 0.1%/Lidocaine HCl 1% Oral Rinse
• Morphine Sulfate 2% Oral Rinse
• Morphine Sulfate 1mg/ml Oral Suspension
• Doxepin HCl 0.5% Mouthwash

4/3/2018
6
Dry Mouth (Xerostomia)
Decreased salivary secretions can cause altered taste, difficulty talking and swallowing, and can
lead to dental carries.
Causes of Xerostomia
• Increased Age
• Sjogren’s Syndrome
• Diabetes
• Thyroid Dysfunction
• Dehydration
• Medications
• Chemotherapy/Radiation
Treatment: Pilocarpine
• Cholinergic Agonist– Stimulates secretions of the exocrine glands
• When used orally can have systemic effects– Hyperhidrosis
– Nausea
– Increased urination

4/3/2018
7
Pilocarpine Formulas
• Pilocarpine HCl 2 mg Troche
• Pilocarpine HCl 10 mg/mL Oral Spray
• Pilocarpine HCl 10 mg/mL Oral Drops
• Pilocarpine HCl 5 mg Lollipop
”provided a significant subjective improvement in speech, swallowing, and decreased
subjective xerostomia as compared to the control”PMID: 26225058
Treatment: Xylitol, Betaine, Olive Oil
Treatment: Xylitol, Betaine, Olive Oil
• Xylitol 7%/Betaine 4%/Olive Oil 2% Oral Rinse– Xylitol: Salivary stimulant
– Betaine: Decreases the loss of water from the mucous component of saliva
– Olive Oil: Lubricant, anti-inflammatory
– Suggested Use: Swish x 1 min and swallow 3-4 x/day

4/3/2018
8
Treatment: Malic Acid
“The results of our randomized clinical trial clearly show a significant increase of salivary flow rates,
both unstimulated and stimulated, after the treatment with 1% malic acid”
PMID: 22926481
Treatment: Malic Acid
• The dissociation of malic acid generates a stimulation of salivary secretion to dilute the concentration of acids in the oral cavity.
• Malic Acid 1% Oral Spray– Suggested use: 3-4 times a day as needed
Treatment: Electrolytes
• Electrolyte troche or oral saliva gel• Sodium Chloride
• Potassium Chloride
• Calcium Lactate or Calcium Chloride
• Magnesium Sulfate
• Sodium Bicarbonate
• Sodium Phosphate
• Suggested Use: Q 4-6 hours prn

4/3/2018
9
Treatment: Saliva Substitute• Calcium Phosphate Oral Rinse
– Part A: Calcium Chloride Buffered Solution– Part B: Phosphate Buffer Solution
• Recommended directions for use:– Mix 15 ml of part A and 15 ml of part B together at time
of dose (30 ml total). – Swish the mouth thoroughly for 1 min with 1/2 the soln
and spit out. Repeat with the remaining 1/2 of the solnand spit out.
– Use BID up to 10 times a day as needed– Avoid eating or drinking x 30 min after dose
Oral Lichen Planus
Oral Lichen Planus
• Chronic inflammatory disorder of unknown cause– Appears to be cell-mediated immune
response– Presents with white lines or striae on lateral
borders of tongue, buccal mucosa and gingiva– Atrophic or ulcerative form painful and may
need long term pharmacologic therapy

4/3/2018
10
Oral Lichen Planus
Common APIs
Steroids
Tretinoin
TacrolimusAnesthetics
Hyaluronic Acid
Treatment: Steroids
• Triamcinolone 0.1% Oral Rinse or Adhesive Paste– Apply up to QID
• Clobetasol 0.05% Oral Rinse– Apply BID for up to 2 weeks
Treatment: Tretinoin
PMID: 20948096
PMID: 453874
Topical Tretinoin 0.05% or 0.1% - Apply BID

4/3/2018
11
Treatment: Tacrolimus
“It appears that topical tacrolimus is an effective alternative to topical clobetasol and may be
considered as a first-line therapy in the management of Oral Lichen Planus.”
PMID: 26204904
Treatment: Tacrolimus
• Tacrolimus 0.03% Oral Rinse– Suggested Use:
Swish and expectorate ½ tsp BID
– May add steroid or anesthetic if needed
Treatment: Hyaluronic Acid
“Statistically significant improvements were observed in the objective criteria which involved the degree of erythema and
the mean area of the lesions with 0.2% hyaluronic acid application than compared to the control group on placebo.”
PMID: 26894175

4/3/2018
12
Treatment: Hyaluronic Acid
• Hyaluronic Acid Oral Rinse– Apply TID, avoid eating or drinking for 30 min
after applicationShetty RR, Burde KN, Guttal KS. The Efficacy of Topical Hyaluronic Acid 0.2% in the Management of Symptomatic Oral Lichen
Planus. J Clin Diagn Res. 2016 Jan;10(1):ZC46-50
Treatment: Combination Formulas
• Tretinoin 0.1%/Clobetasol Propionate 0.05%– Oral Rinse
– Oral Paste
• Clobetasol Propionate 0.05%/Lidocaine Hydrochloride 1% Oral Gel
Temporomandibular Disorders(TMJ)
Pain and compromised movement of the jaw joint and the surrounding muscles.

4/3/2018
13
Treatment: Potassium Complex
“ the authors have found that the gel routinely and predictably provides rapid pain relief and patient
comfort and speeds restoration of the jaw's functional abilities, usually within 5 minutes after it is applied.”
PMID: 18240797
• Potassium Chloride 6%/Potassium Citrate 6%/Potassium Nitrate 6% Topical Gel– Apply to painful areas BID
Treatment: Potassium Complex
TMJ Transdermal Treatment
• Ketoprofen 5%/Cyclobenzaprine HCl 0.5% /Lidocaine HCl 5%/Bupivacaine HCl 1% Topical Cream
• Ketoprofen 10%/Cyclobenzaprine HCl 2% Topical Cream
• Suggested Use: Apply BID-TID
4/3/2018
14
Marketing Minute
Microneedling
Microneedling is a procedure that uses small, fine needles to create microinjuries in the skin while leaving the epidermis intact
AKA: Percutaneous Collagen Induction or Collagen Induction Therapy

4/3/2018
15
How does it work?
• Needles break old collagen bundles that tether scars or wrinkles
• This controlled skin injury stimulates the healing cascade and the production of collagen and elastin under the epidermis
Inflammation Proliferation Remodeling
Microneedling increases collagen formation
Control biopsy Biopsy from needled skin 6 weeks post-op; collagen
stained purple
Liebl H, Kloth L. Skin cell proliferation stimulated by microneedles. J Am Coll Clin Wound Spec.2012 Dec 25;4(1):2-6.
Microneedling significantly increases epidermal thickness
Enhanced epidermal thickness after one month and three months of microneedling treatments compared
to baselineEl-Domyati M, Barakat M, Medhat W, et al. Microneedling therapy for atrophic acne scars: an objective evaluation. J Clin Aesthet
Dermatol. 2015 Jul;8(7):36-42.

4/3/2018
16
Microneedling is used for many cosmetic conditions
Micro-needling
Wrinkles
Scars
Stretch Marks
Large Pores
Skin Rejuv.
Alopecia
Devices UsedRoller Pen
Needle Length • Length of needle selected depends on the
indication of the treatment– 0.2 mm – 0.5 mm: Alopecia and at home skin care
– 0.5 mm – 1 mm: Wrinkles/skin rejuvenation
– 1.5 mm – 2 mm: Scars

4/3/2018
17
Pain increases as the length/depth of the needle increases
Pre-Procedure Treatment
• Use a topical with:– Vitamin A (retinol)– Vitamin C – Palmitoyl pentapeptide or other peptides
• All of these ensure that collagen production will be maximized and that the skin will heal rapidly
• Use a minimum of 3 weeks before but preferably 3 months before microneedling
Pre-Procedure Formulations
• Retinol Molecular 2%/Ascorbic Acid 5% Topical Serum
• Retinol Molecular 2%/Ascorbic Acid 5% Topical Peptide Cream
4/3/2018
18
Procedure
1. Clean the skin2. Application of topical anesthetic (Not
necessary for at-home device usage) – Can be applied 2 different ways:
1. Apply 30-60 minutes prior to the start of procedure
OR2. Apply after a light “rolling” with the microneedling
device
Topical Anesthetic Application
• A study demonstrated that after microneedling with 0.5 mm depth and THEN applying Lido 2.5%/Prilo 2.5% pts had better pain control v. topical anesthesia alone when microneedling at a 2.5mm depth was performed.
– El-Fakahany H, Medhat W, Abdallah F, et al. Fractional microneedling: a novel method for enhancement of topical anesthesia before skin aesthetic procedures. Dermatol Surg. 2016 Jan;42(1):50-5.
Formulas:• Benzocaine 20%/Lidocaine 6%/Tetracaine 4% Topical Cream
• Benzocaine 10%/Lidocaine 5%/Tetracaine 2% Topical Cream
Procedure – Cont.
3. Skin is stretched with one hand and rolling is done in multiple directions (horizontal, vertical, and diagonal)
– endpoint is identified as uniform pinpoint bleeding
Singh A, Yadav S. Microneedling: Advances and widening horizons. Indian Dermatol Online J 2016;7:244-54

4/3/2018
19
Post-Procedure
• Clean face
• Apply serum/topical cream– Optimal time of skin
penetration when using topical products is at 5 minutes as the tissue starts to close considerable after 30 min
– Topical Vitamin A, vitamin C, peptides, hyaluronic acid, etc.
Post Procedure APIsAPI ↓
RednessMoisturizer Anti-
InflammatoryAids in healing
Anti-Wrinkle
Simulates collagen
production
Anti-Oxidant
Beta-glucan(Up to 2%)
X X X
Hyaluronic Acid(0.5-2%)
X X X
Niacinamide(Up to 6%)
X X X
Vitamin A(Retinol)(Up to 5%)
X X
Vitamin C(up to 15%)
X X
Post Procedure FormulationsGels: • Sodium Hyaluronate 1% Gel• Sodium Hyaluronate 2% Gel• Retinol Molecular 1%/Hyaluronic Acid Topical Gel
Serums: • Niacinamide 5%/Ascorbic Acid 2.5% Topical Serum• Ascorbic Acid 5%/Sodium Hyaluronate Topical
Serum• Ascorbic Acid 10%/Sodium Hyaluronate Topical
Serum

4/3/2018
20
Post Procedure Formulations
Creams:• Ascorbic Acid 5%/Beta Glucan/Hyaluronic Acid
Topical Peptide Cream
• Niacinamide 5%/Hyaluronic Acid/Beta GlucanTopical Peptide Cream
• Niacinamide 5%/Retinol Molecular 1%/Hyaluronic Acid/Beta Glucan Topical Peptide Cream
Recovery
• Quick recovery due to epidermis remaining intact
• Minimal side effects– Mild redness– Irritation– Inflammation
• Side effects typically dissipate over 24-48 hours
Counseling Points
• Counsel patient to avoid sun exposure and use sunscreen
• Apply serum/cream daily
• Repeat treatment usually at one month intervals x 4-6 treatments
• Takes approximately 3-6 months for final results.
4/3/2018
21
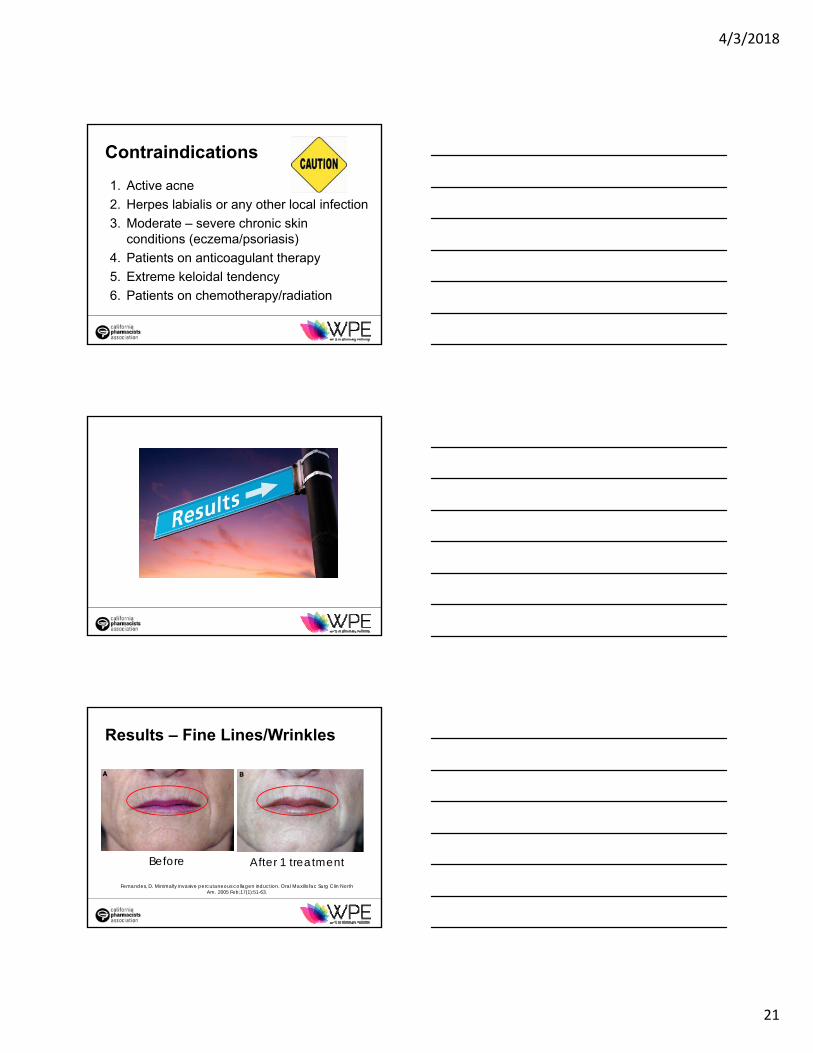
Contraindications
1. Active acne
2. Herpes labialis or any other local infection
3. Moderate – severe chronic skin conditions (eczema/psoriasis)
4. Patients on anticoagulant therapy
5. Extreme keloidal tendency
6. Patients on chemotherapy/radiation
Results – Fine Lines/Wrinkles
Before After 1 treatment
Fernandes, D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005 Feb;17(1):51-63.

4/3/2018
22
Results – Acne Scars/Hyperpigmentation
Before After 3 treatmentsLiebl H, Kloth L. Skin cell proliferation stimulated by microneedles. J Am Coll Clin Wound
Spec.2012 Dec 25;4(1):2-6.
Results – Androgenic Alopecia
Pre treatment -Baseline
Post treatment 12 weeks Weekly microneedling +
1ml 5% minoxidil BID
Dhurat R, Sukesh MS, Avhad G, et al. A randomized evaluator blinded study of effect of microneedling in androgenetic alopecia: a pilot study. Int J Trichology. 2013 Jan-Mar, 5(1): 6-11.
Androgenic Alopecia Formulations
• Minoxidil 5% / Azelaic Acid 5% Topical Foam
• Minoxidil 10% / Finasteride 0.1%Topical Gel

4/3/2018
23
How can microneedling help my practice?• At home microneedling devices can help increase
effectiveness of your formulations
• Dispense with cosmetics/anti-aging/firming formulation
• Many BHRT patients are interested in anti-aging
Are you ready to get started?
Marketing Minute

4/3/2018
24
References• Sroussi HY, Epstein JB, Bensadoun RJ, saunders DP, et al. Common oral
complications of head and neck cancer radiation therapy: mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease, and osteoradionecrosis. Cancer Med. 2017 Dec;6(12):2918-31.
• Lalla RV, Sonis ST, Peterson DE. Management of oral mucositis in patients with cancer. Dent Clin North Am. 2008 Jan;52(1):61-77, viii.
• Lalla RV, Bowen J, Barasch A, Elting L, et al. MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer. 2014 May 15;120(10):1453-61.
• Cerchietti LC, Navigante AH, Bonomi MR, Zaderajko MA, et al. Effect of topical morphine for mucositis-associated pain following concomitant chemoradiotherapy for head and neck carcinoma. Cancer. 2002 Nov 15;95(10):2230-6
• Pöschl, G., Seitz, H.K., 2004. Alcohol and cancer. Alcohol Alcohol. 39, 155–165, OxfOxfs.
• Kuntz R, Allen M, Osburn J. Xerostomia. Int J Pharm Compd. 2000 May-Jun;4(3):176-7.
• Gil-Montoya JA, Silvestre FJ, Barrios R, Silbestre-Rangil J. Treatment of xerostomia and hyposalivation in the elderly: A systematic review. Med Oral Patol Oral Cir Bucal. 2016 May 1;21(3):e355-66.
References• Chiang YZ, Al-Niaimi F, Madan V. Comparative efficacy and patient preference
of topical anesthetics in dermatological laser treatments and skin microneedling. J Cutan Aesthet Surg. 2015 Jul-Sep;8(3):143-6.
• Cohen BE, Elbuluk N. Microneedling in skin of color: a review of uses and efficacy. J Am Acad Dermatol. 2016 Feb;74(2):348-55.
• Singh A, Yadav S. Microneedling: Advances and widening horizons. Indian Dermatol Online J 2016;7:244-54
• El-Domyati M, Barakat M, Medhat W, et al. Microneedling therapy for atrophic acne scars: an objective evaluation. J Clin Aesthet Dermatol. 2015 Jul;8(7):36-42.
• Camirand A, Doucet J. Needle dermabrasion. Aesthetic Plast Surg. 1997 Jan-Feb;21(1):48-51.
• Few J, Semersky A. Commentary on: micro-needling depth penetration, presence of pigment particles, and fluorescein-stained platelets: clinical usage for aesthetic concerns. Aesthet Surg J. 2016 Aug 16.
• Fernandes, D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005 Feb;17(1):51-63.
References• Liebl H, Kloth L. Skin cell proliferation stimulated by microneedles. J
Am Coll Clin Wound Spec. 2012 Dec 25;4(1):2-6. • Dhurat R, Sukesh MS, Avhad G, et al. A randomized evaluator
blinded study of effect of microneedling in androgenetic alopecia: a pilot study. Int J Trichology. 2013 Jan-Mar, 5(1): 6-11.
• Chawla S. Split face comparative study of microneedling with PRP versus microneedling with vitamin C in treating atrophic post acne scars. J Cutan Aesthet Surg. 2014 Oct-Dec; 7(4): 209-212.
• Doddaballapur S. Microneedling with dermaroller. J Cutan Aesthet Surg. 2009; 2: 110-111.
• Gehring W. Nicotinic acid/niacinamide and the skin. Cosmet Dermatol. 2004 Apr;3(2):88-93.

4/3/2018
25
Thank you!







